










Servicios Personalizados
Revista

Articulo
 Inglés (pdf)
Inglés (pdf)
 Articulo en XML
Articulo en XML Referencias del artículo
Referencias del artículo
Indicadores
Compartir

 Permalink
PermalinkJournal of Human Growth and Development
versión impresa ISSN 0104-1282versión On-line ISSN 2175-3598
J. Hum. Growth Dev. vol.30 no.1 São Paulo enero/abr. 2020
https://doi.org/10.7322/jhgd.v30.9970
ORIGINAL ARTICLE
Body self-perception in age school children with Down Syndrome
Autopercepção corporal em crianças com Síndrome de Down (SD) em idade escolar
Dayse Karoline Santos da SilvaI; Larissy Alves CotonhotoII; Mariane Lima de SouzaIII
IMestre em Psicologia - Programa de Pós-Graduação em Psicologia da Universidade Federal do Espírito Santo
IIPós-doutoranda em Psicologia - *Programa de Pós-Graduação em Psicologia da Universidade Federal do Espírito Santo
IIIProfessora doutora em Psicologia -*Programa de Pós-Graduação em Psicologia da Universidade Federal do Espírito Santo
ABSTRACT
INTRODUCTION: The notion of body or body perception is of great importance in the development of motor skills and functionality. In atypical development situations, as in the case of Down syndrome (DS) there is a delay in the development and motor skills are compromised, which possibly is reflected in the quality of body self-perception in children with DS
OBJECTIVE: To assess the characteristics of body self-perception in school age children with DS
METHODS: This is an exploratory and descriptive study involving 10 children aged between seven and nine years. To assess body perception, it was used the Body Notion factor from the Psychomotor Battery (BPM). Data analysis was performed qualitatively and quantitatively according to the criteria established by the instruments and the researchers
RESULTS: The participants' performance regarding the notion of body was not related to their age. The right and left discrimination capability was the body notion sub-factor with the worst performance and the self-image was the sub-factor with the best performance. The drawings of the human figure were split into two categories: unidentifiable (Class A, n = 8) and recognizable (Class B, n = 2
CONCLUSION: It is suggested that the self-perception of children with Down Syndrome analyzed in this study has a strong relationship with the body and environmental stimuli together with psychomotor and cognitive development, which, however, does not coincide with their chronological age
Keywords: Down syndrome, Self-perceived body, child, draw.
Authors summary
Why was this study done?
This study was done to assess the aspects of the body self-perception in children with Down Syndrome.
What did the researchers do and find?
Researchers analyzed the body self- perception of 10 children aged between seven and nine years through the factor 'Body Notion' from the Psychomotor Battery (BPM). Findings indicated the participants' performance regarding the body notion is not related to their age. The right and left discrimination capability was the body notion sub-factor with the worst performance and the self-image was the sub-factor with the best performance, although only two participants have drawn recognizable human figures.
What do these findings mean?
These findings mean that self-perception of children with DS has a strong relationship with the body and environmental stimuli together with psychomotor and cognitive development. However, psychomotor and cognitive development does not seem to coincide with their chronological age.
INTRODUCTION
The movement of the body accompanies the human being since the prenatal period and for it to be perfected and specialized, a multifactorial system that encompasses bodily responses and the capacity for perception must be fully functioning. Despite being an inherent characteristic of human life, movement needs a base, which is the perception of the body itself, and the possibilities of movement based on the notion of the body.
Psychomotor development in childhood is characterized by the acquisition of motor, neurological and psychic skills to guarantee the child an ample self control of his body and diverse possibilities of movement and interaction with the environment. Basic skills such as walking, running and manipulating objects are necessary for directing daily routines, characteristics of the child's development and maturation1.
As a consequence of the integration and maturation of these skills, tonicity, balance, lateralization, spatio-temporal structuring, praxis and the notion of body occur. Psychomotricity develops over time, from the simplest to the most refined and specific motor skills. Delays or deficits can be observed when this integration is not done in the correct time or inappropriately2.
The notion of body perception is of great importance in the development of motor skills and functionality. Body perception is characterized by an engendering of sensory contents that begin to be associated in childhood. It could be defined as an awareness of the body from sensory multimodalities3. In this sense, sensory impressions, that is, the results of sensory stimuli, are important for the development of the child's awareness of his own body. If one of these experiences is impaired, it can negatively influence the full development of the body's consciousness. Motor disorders are attached to the characters of corporeality, so that the synchrony between motor development and the development of the schema and body awareness is crucial for typical development4.
It is known that in situations of atypical development the impairment of motricity and functionality is a constant. Worldwide, Down Syndrome (DS) is one of the most frequent cause of atypical development in children, among the cases of genetic malformations and it is the most common cause of intellectual disability5.
This syndrome is due to an error in chromosome pair 21 - in which there should normally be two pairs of cells, but there are three, is also called Trisomy 21 and is characterized by presenting generalized ligament laxity, hypotonia, atlanto-axial instability and joint hypermobility, small and round skull with flattened occipital region, short and wide neck (with excess nuchal skin), small and malformed ears, small mouth with a large and generally protruding tongue6 and deficits in cognitive functions such as attention, memory, language and abstract thinking7.
Children with DS have a delay in development and motor acquisitions are compromised and can be achieved in up to twice the time of a child with typical development. In addition to the delay, both the lack of physical experiences with the environment and the deficit of perceptual sensory integration of oneself can interfere in the cognitive development process and generate difficulty in carrying out activities of daily living8.
The motor skill of children with DS is characterized by un-coordination, slowness, variability and hesitation, in addition to the difficulty in responding to changes in the environment9. Through several methods and different approaches, studies show that children with Down Syndrome are at a disadvantage compared to typical children. In Greece, researchers assessed typical and children with DS for gross motor skills and executive function and observed that, in both aspects, children with DS scored significantly less than typical children10. In another study that evaluated motor acquisitions in infants with DS and typical children, there was a difference in age of acquisition of motor skills in all tasks between the typical group and the group with DS11.
Despite these studies on motor skills, the notion of body perception in children with DS is still poorly studied. Existing publications focus on self-concept and self-perception related to motor skills: in the first case, a study using self-reports suggests that, in the perception of children with DS, they have a full and happy life12; in the second research topic, two independent studies indicate that there is a delay in this coupling of the perception of action in children with DS13,14.
Regarding the assessment of body perception, the available tests are usually part of a complex battery, developed for the observation of psychomotricity factors in general. In such batteries, body perception is assessed through body design15,16. From the point of view of developmental psychology, the child's drawing expresses his mental evolution and, consequently, the process of becoming aware of himself and the world, that is, a process of knowledge represented graphically. Children's graphics are the result of memories about an object, which may be the body itself, and are accurate due to motor skills and cognition17.
This study is based on the understanding that the difference between the typical motor development and the motor development of a child with DS is related to body experience and, for it to be performed with mastery, the body self- perception and exploring its capacity are essential processes.
Thus, the objective of this study is to analyze body self-perception in school age children with Down Syndrome.
METHODS
Study design
This is an exploratory and descriptive study, with quantitative and qualitative data analysis18. The research project was approved by the Ethics Committee on Research with Human Beings at UFES - Campus Goiabeiras, State of Espírito Santo, Brazil, with registration and accepted under No. 1,629,376.
Participants
Ten children with Down Syndrome, aged between seven and nine years, of both sexes, who attended specialized educational institutions in Grande Vitória, Espírito Santo, Brazil composed the study sample. The following inclusion criteria were adopted: being able to communicate, being a regular student at the institutions. The immobility of one or more limbs was considered an exclusion criterion. In order to preserve the children's identity, the real names were changed to fictitious names.
Instruments
The assessment of body perception, it was used a quantitative instrument, the Body Notion of the Psychomotor Battery (BPM), by Vitor da Fonseca19. BPM is an instrument based on a set of tasks that allows the detection of functional deficits in psychomotor terms, covering the sensory and perceptual integration that is related to the child's learning potential.
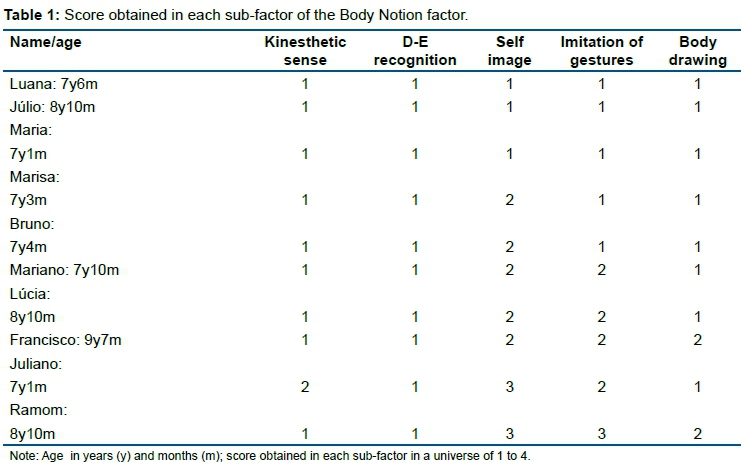
We used the Body Notion Factor, which contains five sub-factors, characterized by the following tasks: (1) Kinesthetic factor: the child must name 16 body areas pointed by the evaluator; (2) Right and Left Differentiation (R-L): the child must perform eight tasks with the body differentiating R and L, such as crossing the right leg over the left knee; (3) Self-image: the child should put his finger on his nose four times, twice in each hand; (4) Imitation of gestures: the child must imitate the gestures made by the evaluator with his finger in the air; (5) Drawing the body: the child must draw himself, the best he knows. Each subfactor has a maximum score of four (4) and a minimum of one (1). The higher the score obtained, the better the tasks performance. The minimum score obtained on the factor is five (5) points and the maximum twenty (20) points.
For the qualitative assessment of the child's knowledge about his own body, the designs obtained in the BPM body drawing sub-factor were evaluated according to parameters related to the level of anatomical details, established by the authors.
Data collection and analysis procedures
First, the research objective and its procedures were explained and clarified to representatives of the educational institutions. After having the permission from the institutions and the authorization of children guardians, the children were included according to the inclusion criteria. The selected children were evaluated within their institution, in a private room. Before the evaluations, it was carried out a process of setting up and linking the child to the researcher, playing with modeling clay. Each evaluation lasted an average of 20 minutes.
After collection, the data provided by the instrument and the drawing done by the children were tabulated and evaluated. The application of the Notion of Body factor was performed by a trained researcher and the total score obtained on the factor was calculated by adding the values obtained in the sub-factors. Then, the average score on the body notion factor was calculated for the sample.
The drawings were classified according to the contour, line and presence of delimited body parts. In the drawings in which the human figure is recognized, these characters were observed: 1. Presence of head: size (large, small, suitable for the rest of the body), shape (square, round, misshapen), contour (regular or irregular) and trace (continuous or interrupted); 1.1 Presence of the face: eyes (size, symmetry, contour and line), nose (size, symmetry, contour and line), mouth (size, symmetry, contour and line) and their distribution on the face; 2. Presence of legs (joined to the trunk, to the head), joined symmetrically on both sides (right-left), contour line (regular or irregular); 2.1 Presence of hands: contour, shape, line and symmetry and presence of defined fingers; 3. Presence of arms (joined to the trunk, to the head), joined symmetrically on both sides (right-left), contour line (regular or irregular); 3.1 Presence of feet: contour, shape, line and symmetry and presence of defined toes; 4. Trunk: size (large, small, suitable for the rest of the body) and shape (square, round, triangular) contour (regular or irregular), line (continuous or interrupted); 5. Presence of neck: size (large, small, suitable for the rest of the body), contour (regular or irregular), line (continuous or interrupted); 6. Hair: size and shape.
RESULTS
Of the total children evaluated, six were boys and four girls, aged between seven years and one month and nine years and seven months. The results of the evaluations indicated a moderately better performance in the self-image subfactor and in the imitation of gestures. The worst performance occurred in the R-L recognition subfactor (Table 1).
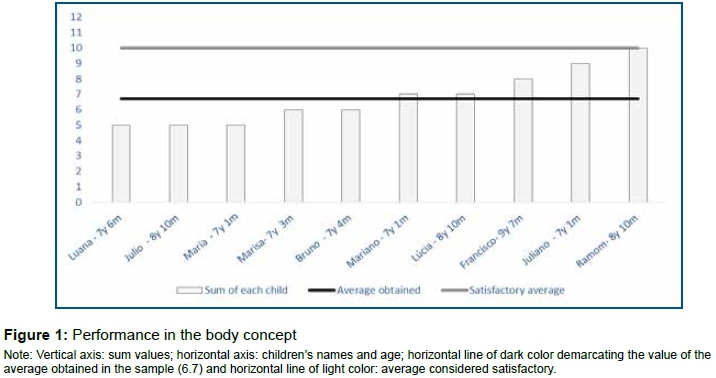
The results of the sum of the Notion of Body factor varied regardless of age. Children of the same age (Júlio and Ramom) had the lowest and highest scores, respectively (Figure 1). The average of the sample sums was 6.7 and is below the expected average in a child with typical development of the same age. In the BPM body concept factor, 10 is the score considered satisfactory, when the child performs the tasks, but with difficulty; 15 is the score considered good and the child performs the tasks properly; and 20 characterizes an excellent score, when the child performs the tasks with mastery, without any difficulty.
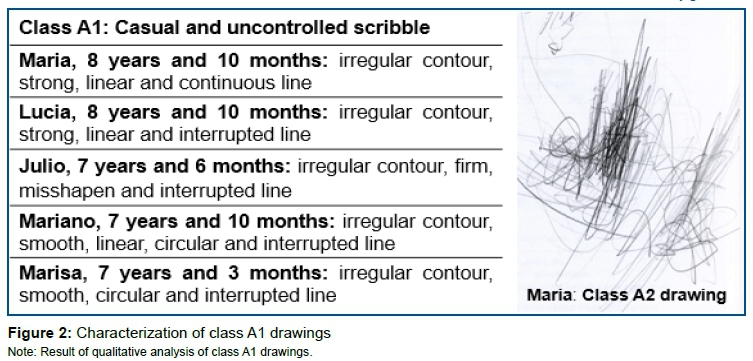
The results of the analysis of the drawings indicated two classes (A and B), respectively, unrecognizable human figure and recognizable human figure. Class A is subdivided into class A1, which contains only casual and uncontrolled squiggles (Figure 2) and class A2 contains drawings with poorly controlled lines, which look like rough geometric lines or refer to geometric shapes (Figure 3). Class B represents the drawings in which the human figure was recognized (Figure 4).
The average age of children with class A drawings was 7.5 years. And, in these children's drawings, it was not possible to recognize the human figure. In class B, the mean age was 9.25 years and, in the drawings of children included in that class, it was possible to recognize the human figure.
The Class B drawings were made by the children who obtained the highest scores for the Notion of Body factor. In those the body is presented in more detail, with greater discrimination of anatomical characteristics such as the presence of head and limbs, however not all older children showed greater detail in their drawings. In drawings done by children below 8 years, it was not possible to identify a human figure.
DISCUSSION
Our results suggest that the body perception of children with DS is altered, with special relevance in decreasing the kinesthetic sense and in the deficit in R-L recognition. It is possible that these changes occur due to factors that imply the delayed psychomotor and cognitive development of children with the syndrome. Motor development delay in children with DS has been well documented in the scientific literature, and among the main factors that cause this delay is hypotonia, lack of balance and cognitive deficit20,21.
From the psychomotor point of view, there is a relationship between the development of the body's perception and the stimulus given to the child. The development process is closely linked to the process of experiencing body sensations.
For a person to have a satisfactory development of his body image, he has to experiment with his movements in order to direct his actions in the world and be aware of his body limitations and possibilities. This process can be facilitated or hindered by several factors, such as age, trauma, physical or cognitive disabilities, environmental and biological factors, and pedagogical and therapeutic interventions22. In fact, the development of an individual with DS is equivalent to that of typical children, thus resulting from cultural, social, environmental and genetic influences23.
The common and low result for the task of discrimination of right and left is a response consistent with the literature, since it is necessary to have awareness of own body, so that it can be differentiated on the right and left by the individual.
Laterality is the result of experiences of the body segments of the two halves of the body throughout life, that is, it requires a certain degree of body awareness for it to develop24. The awareness that there is a right and left side is also essential for the child to perceive its movement in time and space25. In a study that aimed to detect foot preference in children with Down syndrome, the researchers concluded that the difficulty in perceiving additional weight by the receptors present in the muscle spindles and tendons influences the formation of the body scheme and laterality26. The study compared a group with DS and another without DS in performing a task: moving a mobile with their feet, initially without a load and then with a load of one third of the weight of the legs. In children with DS, additional weight did not influence foot preference.
The highest score on the self-image subfactor may have occurred because the instructions for carrying out the task were also performed by the examiner, so that the participant could see what should be done. Thus, it is possible that, by having the possibility of imitating the action, the participant had a better chance of doing well in the task. That is, the task performed by the examiner may have served as visual feedback. The data found point to the importance of imitation for child development.
In fact, the importance of imitation in the development of mental representations has been indicated in more than one theoretical model of cognitive development that follows two main perspectives: the classic approach of Piaget's theory and the approach resulting from the most current empirical research. For the first, imitation precedes mental representations; it undergoes a transformation process over six stages of the sensorimotor period, ranging from reflex exercises to representative imitation and deferred imitation27. For the second, a little more recent in developmental psychology28,29, this acquisition occurs in reverse order, that is, the capacity for representation is a necessary condition for imitation. Thus, the imitation process becomes essential in the representation process; in this case, representation of the body itself30. In this sense, it is feasible to assume that imitation and representation of the body itself in children with DS are lagging, as these acquisitions in typical children generally occur between the first six years of life.
Regarding the body self-perception of the children evaluated, there was no variation in age, that is, children of different ages had similar performance, obtaining the same score. This result can be explained by the individuality of each child, that is, by the capacity of reaction and subjectivity inherent to each one and by the level of stimulation and opportunities offered.
This result indicates that more accurate motor skills acquisition and greater perception of the body itself in a mental representation (complex behavior that precedes language) depend not only on chronological age and that, in children with DS, development does not seem to follow the fixed chronological order of the acquisitions expected in the typical development. In other words, body self-perception seems to depend much more on the development of psychomotor skills than on the passage of time8.
Our findings of qualitative assessments of drawings done by children with DS can be explained based on the literature on the graphics development. In the class A drawings, the figures represented with doodles and grotesque geometric shapes show the stage of development of the graphics called doodles, characterized by random doodles and made by children aged between two and four years, with typical development31. In children with DS, the acquisition of motor skills occurs with delay and, therefore, even at seven and nine years of age, it is not entirely strange that their drawings are graphically similar to those of children aged four or younger.
Class B drawings represent the human figure at different stages. In these cases, there is the intention of the drawing, but the graphic representation does not always correspond to the real one. This ability, determined by motor coordination and limited by manual graphic movements, is improved since the child's practice and maturity32. Thus, it is understandable that children with DS in this sample, aged between seven years and one month (7y1m) and nine years and seven months (9y7m), demonstrate fine motor skills and motor skills in the process of improvement.
Regarding the results for the body concept factor, it was possible to observe some behaviors that presuppose the symbolic function, among which are deferred imitation, mental image, in addition to the ability to dissociate the body from the external object - perception of the body itself, a characteristic that begins at the sensory motor stage and expands throughout development.
According to Piaget, the child develops the symbolic function from behaviors that appear almost simultaneously, but that overlap in complexity. At an increasing level of complexity, they include deferred imitation, symbolic play, drawing, mental image and language. This function arises from the sensorimotor stage (0 to 2 years) and develops in the next stage, called preoperative (2 to 6-7 years).
Thus, it can be suggested that the children in this study, aged between seven and nine years old, present characteristics of the sensorimotor and preoperative stages. It seems to be that children with DS in this sample intend to draw themselves, designing what they know before expressing, in their pictures , what they see27. For Luquet, quoted in Piaget27, the child's drawing up to the age of 8-9 years is essentially realistic in intention, but initially the child draws what he knows about a character or object, and only later graphically expresses what he/she sees in it.
The drawings by Juliano, Francisco and Ramom illustrate very adequately the three important phases of realism in the drawing: the "fortuitous realism", in which the doodle drawings can be allocated, is well characterized in the drawing by Juliano; the "failed realism", in which the elements are juxtaposed and can be represented by the "badamecos", is very well characterized by Francisco's drawing; and the phase of "intellectual realism" (graphic evolution of the previous phase), which essentially presents the conceptual attributes of the model, without concern for visual perspectives, well characterized by Ramom's design.
It is important to note that the evolution of the design happens concomitantly with the structuring of the space, according to the different stages of development. Thus, it is possible to infer from the drawings presented that the collaboration of cognitive, motor and perceptual aspects is necessary for the mental image of the body itself to be displayed graphically31.
This study used part of the instrument Psychomotor Battery Body Notion factor to measure body self-perception, which can be understood as a methodological limitation. However, the combination of quantitative data with a descriptive and qualitative analysis of the drawings expanded the discussion on this characteristic. In addition, as it is an exploratory study, the results suggest interesting hypotheses to be tested in future studies. For example, our findings about decreased body self-perception suggest a trend that the ability to perceive may need more time to develop in this population. Therefore, it is emphasized the body self-perception as an important attribute to be considered in stimulating the development of children with DS.
In the context of health and rehabilitation, inserting body self-perception as a variable when assessing development in children with DS can bring important benefits to the users of these services. In view of the possible relationship between self-perception and basic motor and cognitive functions, the assessment of body self-perception maximizes the possibilities of therapeutic approaches, which can determine a significant improvement in the care of children with DS by different health professionals.
In conclusion, the body self-perception of children with Down Syndrome is related to body and environmental stimuli together with psychomotor and cognitive development, which, however, does not coincide with the development that occurs chronologically..
Acknowledgments
We are grateful for the support and encouragement from the Espírito Santo Research and Innovation Support Foundation - FAPES (process: 70224617) and to Professor Claudia Broetto Rossetti, for the help given to this research.
Francisco, 9 years and 7 months: presence of a single element that represents the head, neck and trunk without distinction from them, with a regular and circular shape, continuous and firm line; in this element are represented the eyes, which are characterized by a uniform line, size proportional to the shape that is inserted, arranged somewhat asymmetrically and superiorly, presenting a little detailed mouth representation with a linear and horizontal line proportional to the way it is inserted, arranged inferiorly. Presence of upper limbs with different sizes with a firm, linear outline, and there is no representation of hands or fingers. Presence of lower limbs inserted with the same size, with a firm and linear line, and there is no representation of feet.
Ramom, 8 years and 10 months: presence of medium-sized head in relation to the rest of the body, with a rounded shape, with a firm and continuous line. On the head there is representation of the eyes, which are characterized by a rounded shape, slightly irregular contour, different sizes, arranged superiorly and inserted asymmetrically; in one eye, there is a point located inside it, in eye D; nose characterized by its rounded shape, irregular outline, centrally arranged, inserted just below the midline; mouth proportional to the rest of the body. The legs are connected to the trunk inferiorly and asymmetrically, with relatively equal sizes, regular contour line; feet with different sizes, slightly asymmetrical, contour line regular and continuous. The arms are connected to the trunk in its upper portion, asymmetrical, with equal sizes, regular contour line, presence of hands, with different sizes, slightly asymmetrical, regular and continuous contour line; and there are suggestive images of irregular and asymmetrical fingers, presence of hair, short and irregularly shaped, and clothing.
Note: Result of qualitative analysis of class B drawings.
REFERENCES
1.Toledo DR, Barela JA. Sensory and motor differences between young and older adults: somatosensory contribution to postural control. Rev Bras Fisioter. 2010;14(3):267-75. DOI: https://doi.org/10.1590/S1413-35552010000300004 [ Links ]
2.Brêtas JRS, Pereira SR, Cintra CC, Amirati KM. Avaliação de funções psicomotoras de crianças entre 6 e 10 anos de idade. Acta Paul Enferm. 2005;18(4):403-12. DOI: http://doi.org/10.1590/S0103-21002005000400009 [ Links ]
3.Leal IA. Poder de projetar-se do ser no mundo em Merleau-Ponty. Princípios Rev Filosof. 2012;19(32):393-417. [ Links ]
4.Simons J, Leitschuh C, Raymaekers A, Vandenbussche I. Body awareness in preschool children with psychiatric disorder. Res Dev Disabil. 2011;32(5): 1623-30. DOI: http://dx.doi.org/10.1016/j.ridd.2011.02.011 [ Links ]
5.Arya R, Kabra M, Gulati S. Epilepsy in children with Down syndrome. Epileptic Disord. 2011;13(1):1-7. DOI: http://dx.doi.org/10.1684/epd.2011.0415 [ Links ]
6.Coelho C. A síndrome de Down. [cited 2019 Apr 01] Available from: https://www.psicologia.pt/artigos/textos/A0963.pdf [ Links ]
7.Silva MNS, Santos KMB, Andrade LM, Zanona AF. Avaliação funcional do desenvolvimento psicomotor e ambiente familiar de crianças com síndrome de down. Rev Interinst Bras Ter Ocup. 2017;1(2):186-201. [ Links ]
8.Bonomo LMM, Rossetti CB. Aspectos percepto-motores e cognitivos do desenvolvimento de crianças com Síndrome de Down. Rev Bras Cresc Desenv Hum. 2010;20(3):723-34. DOI: https://doi.org/10.7322/jhgd.19980 [ Links ]
9.Campos AC, Savelsbergh GJ, Rocha NA. What do we know about the atypical development of exploratory actions during infancy? Res Dev Disabil. 2012;33(6):2228-35. DOI: http://doi.org/10.1016/j.ridd.2012.06.016 [ Links ]
10.Wang HI, Long IM, Liu MF. Relationship between motor skill competency and executive function in children with Down's syndrome. Res Dev Disabil. 2012;33(6):1792-8. DOI: http://doi.org/10.1016/j.ridd.2012.05.002 [ Links ]
11.Pereira K, Basso RP, Lindquist, ARR, Silva LGP, Tudella E. Infants with Down syndrome: percentage and age for acquisition of gross motor skills. Res Dev Disabil. 2013;34(3):894-901. DOI: http://doi.org/10.1016/j.ridd.2012.11.021 [ Links ]
12.Skotko BG, Levine SP, Goldstein R. Self-perceptions from people with Down Syndrome. Am J Med Genet Part A. 2011;155A(10):2360-9 DOI: http://doi.org/10.1002/ajmg.a.34235 [ Links ]
13.Brunamonti E, Pani P, Papazachariadis O, Onorati P, Albertini G, Ferraina S. Cognitive control of movement in down syndrome. Res Dev Disabil. 2011;32(5):1792-7. DOI: https://doi.org/10.1016/j.ridd.2011.03.008 [ Links ]
14.Polastri PF, Barela JA. Perception-action coupling in infants with Down syndrome: effects of experience and practice. Adapt Phys Act Q. 2005;22(1): 39-56. DOI: https://doi.org/10.1123/apaq.22.1.39 [ Links ]
15.Camargos ACR, Fontes PLB, Araújo APS, Silva FC, Pereira, LP, Souza SMF. Desenvolvimento motor de crianças pré- termo moderada aos sete e oito anos de idade. Fisioter Pesqui. 2011;18(2):182-7. DOI: https://doi.org/10.1590/S1809-29502011000200014 [ Links ]
16.Askevold F. Measuring body image. Preliminary reporto on a new method. Psycother Psychosom 1975;26(2):71-7. DOI: http://dx.doi.org/10.1159/000286913 [ Links ]
17.Souza SHV. A Criança e a Expressão do Pensamento através do Grafismo. Rev Thema. 2012;9(2):1-23 [ Links ]
18.Dal-Farra RA, Lopes PTC. Métodos mistos de pesquisa em educação: pressupostos teóricos. Nuances: Estud Educ. 2013:24(3):67-80. DOI: http://dx.doi.org/10.14572/nuances.v24i3.2698 [ Links ]
19.Pereira K, Tudella E. Perfil psicomotor de escolares: quanto ao gênero, à idade gestacional e ao aspecto físico. Fisioter Mov. 2008;21(1) 47-55. [ Links ]
20.Felício SR, Gava NM, Zanella RC, Pereira K. Marcha de crianças e jovens com síndrome de Down. ConScientiae Saúde. 2008;7(3):349-56. DOI: https://doi.org/10.5585/conssaude.v7i3.1326 [ Links ]
21.Meneghetti CHZ, Blascovi-Assis SM, Deloroso FT, Rodrigues GM. Avaliação do equilíbrio estático em crianças e adolescentes com Síndrome de Down. Rev Bras Fisioter. 2009;13(3):230-5. DOI: http://dx.doi.org/10.1590/S1413-35552009005000029 [ Links ]
22.Eiras LFG, Amorim BB, Carmo NM, Russo MM. Construção da imagem corporal em deficientes visuais. Rev Arq Mov. 2012;8(2):94-110. [ Links ]
23.Bissoto ML. O desenvolvimento cognitivo e o processo de aprendizagem do portador da Síndrome de Down: revendo concepções e perspectivas educacionais. Rev Ciêncs Cog. 2005;4:80-8. [ Links ]
24.Souza RM, Teixeira LA. Sobre a relação entre filogenia e ontogenia no desenvolvimento da lateralidade na infância. Psicol Reflex Crit. 2011;24(1):62-70. DOI: http://dx.doi.org/10.1590/S0102-79722011000100008 [ Links ]
25.Serafim G, Peres LS, Corseuil HX. Lateralidade: conhecimentos básicos e fatores de dominância em escolares de 7 a 10 anos. Cad Ed Fís. 2000;2(1):11-30. [ Links ]
26.Santos GL, Bueno TB, Tudella T, Dionísio J. Preferência podal em lactentes com síndrome de Down: fatores extrínsecos e intrínsecos. Fisioter Pesq. 2012; 19(2):171-7. DOI: http://dx.doi.org/10.1590/S1809-29502012000200014 [ Links ]
27.Piaget J, Inhelder B. A psicologia da criança. 7 ed. São Paulo: Difel, 1982. [ Links ]
28.Meltzoff AN, Moore MK. Imitation in Newborn Infants: Exploring the Range of Gestures Imitated and the Underlying Mechanisms. Develop Psych. 1989; 25(6):954-62. DOI: http://dx.doi.org/10.1037/0012-1649.25.6.954 [ Links ]
29.Jones SS. The development of imitation in infancy. Philos Trans R Soc Lond B Biol Sci. 2009; 364(1528):2325-35. DOI: http://doi.org/10.1098/rstb.2009.0045 [ Links ]
30.Barbosa RG, e Batista IL. Vygotsky: Um Referencial para Analisar a Aprendizagem e a Criatividade no Ensino da Física. Rev Bras Pesq Educ Ciênc. 2018;1:49-67. [ Links ]
31.Rodrigues MH. Análise do desenho infantil segundo as ideias de Luquet. Rev Unifebe. 2010;1(8):19-34. [ Links ]
32.Luquet GH. O desenho infantil. Lisboa: Companhia Editora do Minho, 1989 [ Links ]
 Correspondence:
Correspondence:
daysekaroline@hotmail.com
Manuscript received: August 2019
Manuscript accepted: October 2019
Version of record online:March 2020


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}