










Serviços Personalizados
Journal

artigo
 Inglês (pdf)
Inglês (pdf)
 Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
 Curriculum ScienTI
Curriculum ScienTIIndicadores
Compartilhar

 Permalink
PermalinkJournal of Human Growth and Development
versão impressa ISSN 0104-1282
Rev. bras. crescimento desenvolv. hum. vol.22 no.2 São Paulo 2012
ORIGINAL RESEARCH
Environmental pollutants and odds of hospitalization for asthma in children - São José dos Campos, Brazil, in the years 2004-2005
Camila Trolez Amancio; Luiz Fernando Costa Nascimento; Thiago Trolez Amancio
Departamento de Medicina da Universidade de Taubaté - UNITAU. Av. Tiradentes, 500 - CEP: 12030-180 - Taubaté, SP - Brasil. Fone: (55 12) 3625-4271
ABSTRACT
OBJECTIVE: to estimate the association between exposure to air pollutants and hospital admissions for asthma.
METHODS: this is an ecological study of time series, which included individuals from 0 to10 years living in Sao Jose dos Campos, for the period 2004 to 2005.Data of hospitalizations for asthma were obtained from DATASUS. The data of ambient levels of particulate matter, sulfur dioxideand ozone were obtained from the Company of Technology of Environmental Sanitation (CETESB) and temperature and humidity from the Foundation for Science, Technology and Space Applications (FUNCATE). Lag models have been made from 0 to 7 days and analyzed by binary logistic regression,yielding odds ratios and their confidence intervals of 95% by SPSS 15.0.
RESULTS: there were 809 admissions, ranging from 0 to 7. It was possible to identify an association of the particulate matterboth on the same day of exposure and the next third, fifth and sixth days with the admissions; sulfurdioxide was associated with hospitalizations in the first, second and third days after exposure andozone on the third day after exposure to gas. Thus, this study showed an association between airpollutants and asthma hospitalization in a medium-sized city.
Key words: asthma; air pollution; particulate matter; sulfur dioxide; ozone.
INTRODUCTION
Among the environmental factors related to the pathogenesis of respiratory diseases, we can highlight air pollution, a major public health problems today. Studies have found that air pollutants, even at exposure levels below acceptable standards, can cause deleterious effects to human health1. It is known that the lungs are the main target of attack of air pollutants, among which the primary are particulate matter (PM10), sulfur dioxide (SO2) and ozone (O3).
The particulate matter is a mixture of liquid and solid particles suspended in the air which can reach the lower airways. It presents an important characteristic of transporting gases adsorbed on its surface to the most distal portions of the airways. The sulfur dioxide resulting from combustion of fossil elements, can be transported to distant regions of the primary sources of emission, which increases its area. Moreover, the ozone formed from chemical reactions involving sunlight, has powerful oxidizing and cytotoxic effect2.
Among respiratory diseases, bronchial asthma, one of the most common chronic diseases of childhood, has been linked to exposure to environmental pollutants in many parts of the world3-6. In Brazil, the relationship between exposure to environmental pollutants and respiratory disease has been studied mainly in large urban centers and medium-size cities1,7-10.
Besides, being a disease of worldwide prevalence, asthma generates high costs, both socially and for the health system11. In 2007, the financial cost due to hospitalization for asthma in children and adolescents spun around R$ 6 million (1 US$ H" R$ 1.70) for the State of Sao Paulo and R$ 70,000 for the city of Sao Jose dos Campos, SP12.
Children and elderly people with diseases of cardio-pulmonary involvement prior are the most susceptible to the adverse effects of air pollution. For children, the fact is due to greater exposure to pollutants, increased ventilation per minute and higher levels of physical activity13.
It is believed that the manifestations of the biological effects of air pollution have a behavior gap in relation to the individual's exposure to these pollutants14. This means that the manifestation of symptoms of acute asthma in a certain individual may be due to pollution on the days preceding or concurrent with the outcome, which is called lag.
Thus, the objective of this study was to estimate the association between exposure to air pollutants and the chance of hospitalization for bronchial asthma in children and adolescents in Sao Jose dos Campos-SP.
METHODS
It is an ecological study of time series, which used data from hospitalizations in Sao Jose dos Campos, in the periods of 01/01/04 to 12/31/05, obtained from the Department of Information and Informatics of National Health System (DATASUS) 15. All hospitalizations in subjects aged between 0 and 10 years with International Classification of Diseases 10th revision (ICD-10) referred to asthma (J45) were selected. The present study refers to the municipality of Sao Jose dos Campos, a city in the state of Sao Paulo, which is 91 km away from São Paulo, in the Paraíba Valley, with approximate population of 600,000 inhabitants. It presents itself as a regional center for industry, shopping and services in the Vale do Paraíba and southern Minas Gerais State, serving a population of approximately 2 million in habitants16.
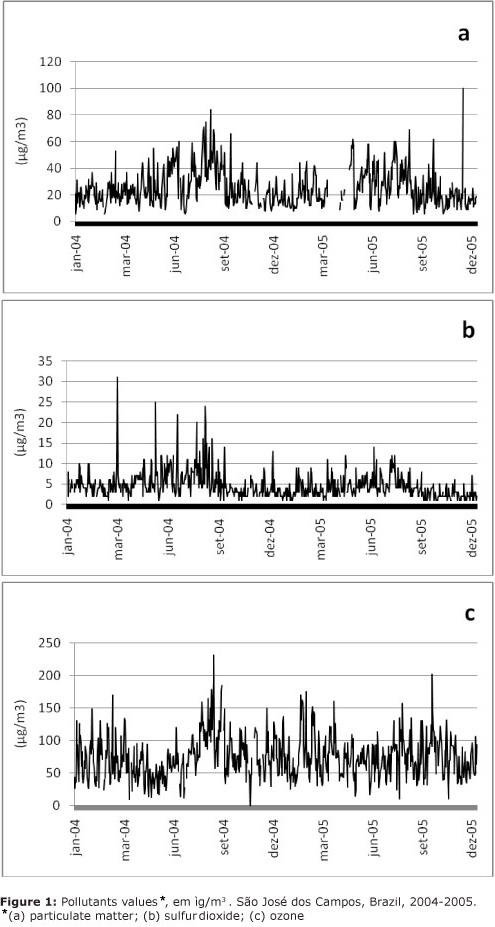
Information on the daily levels of pollutants particulate matter, sulfur dioxide and ozone were obtained from the Agency of Environmental Sanitation Technology (CETESB)17, which has a monitoring station in Sao Jose dos Campos, located in the central region. For all pollutants, data collection was started in the first hour of the day, for 24 hours and were quantified in mg/m3. We considered the daily averages of each pollutant. The technique to quantitate the PM10 was Beta monitor for the technique of coulometry SO2 and O3 chemiluminescence. The interpolation of missing data of pollutants was not performed because these data have no deterministic behavior, but chaotic.
Data on temperature and humidity were obtained from the Foundation for Science, Technology and Space Applications (FUNCATE)18. To estimate the relationship between exposure to environmental pollutants and hospital admissions for asthma, both on the same day as the previous days, we constructed models of lags distributed from zero to seven days prior to exposure (lag).
The asthma hospitalization variables were then recoded, with zero referring to absence of a hospital admission and 1 for one or more admissions daily. Then, we analyzed the relationship between exposure to pollutants, which were analyzed as continuous variable, in a unipollutant model adjusted for minimum temperature and humidity, and hospitalizations for asthma with lags from zero to seven days, making use of SPSS 15.0. To estimate this association, binary logistic regression was made and odds ratios obtained with their respective confidence intervals of 95%.
RESULTS
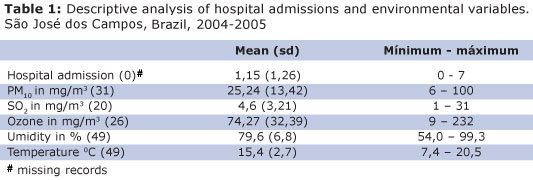
There were 809 hospitalizations of children aged between zero to 10 years for asthma in Sao Jose dos Campos during the study period. The mean was 1.11 hospitalizations (SD = 1.24), with daily ranges 0-7. April, May and June are the months with the highest numbers of admissions in both years of study.
Forty-nine data on humidity, maximum temperature, minimum temperature and average temperature were not obtained. This period of failure refers to the first day of January 2004 until the eighteenth day of February 2004.
There was no information regarding the 31 days of average daily particulate matter (4.2% missing data), 20 days of sulfur dioxide (2.7%) and 26 days ozone (3.6%), irregularly distributed in study period. The admission data were obtained on all days of the study period.
Mean values of hospital admissions, environmental pollutants concentrations, humidity and minimum temperature with respectives standard deviations and minimum and maximum values, as well as the number of days that did not have this information, are shown in Table 1.
The distribution of the daily levels of environmental pollutants are shown in Figure 1.
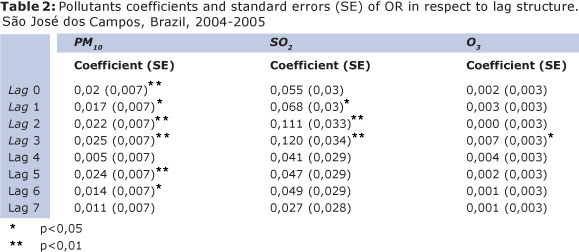
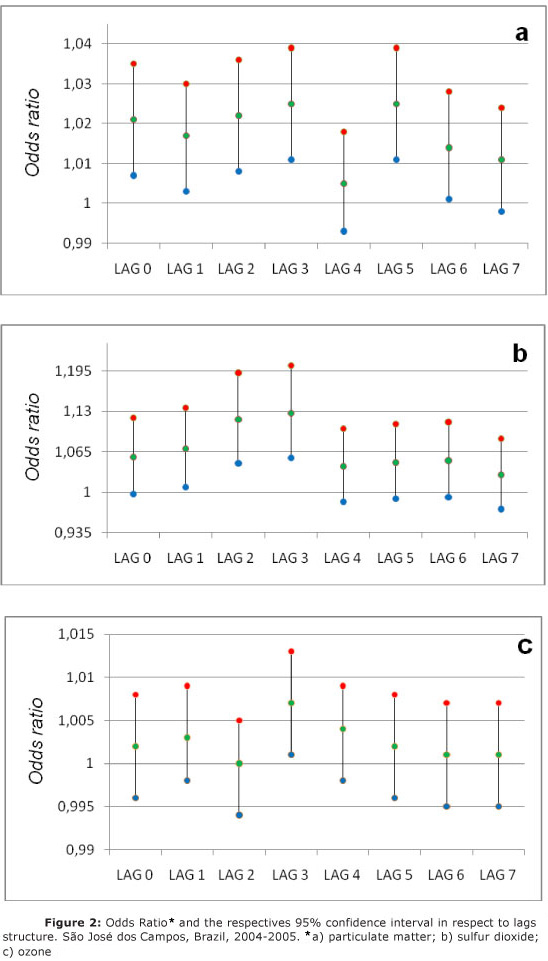
From the binary logistic regression, we obtained the coefficients of the odds ratios and standard errors for each pollutant in each lag structure, shown in table 2. Figure 2 shows the odds ratio obtained by relating the concentrations of air pollutants, adjusted for minimum temperature and humidity, and hospitalizations for asthma, with their respective 95% confidence intervals for lags from zero to seven days.
DISCUSSION
This is the first study to estimate the association between exposure to air pollutants (PM10, SO2 and O3) and hospitalizations for asthma in a medium-size city in Brazil, such as Sao Jose dos Campos. We chose to use logistic regression to estimate the odd of hospital admission unlike other studies in Brazil that used Poisson regression to estimate the increase in risk of hospitalization19,20.
The months with higher numbers of hospital admissions for asthma in this study were April, May and June in both years of study, and this is possibly due to the lower temperatures occurring in those months.
The PM10 exposure is significant in the same day, the three subsequent days, in the fifth and sixth days. It is known that one of the mechanisms involved in the onset of deleterious effects from exposure to PM10 is the pulmonary inflammation. This pollutant also presented a greater statistical significance in the research conducted by Nascimento et al, also in children in Sao Jose dos Campos, in relation to hospitalization for pneumonia10. On the other hand, in a study conducted in Mexico, there was no significant relationship between ambient levels of PM10 and emergency visits for respiratory causes21.
Possibly, this difference in statistical findings is due to disregard of individual exposure to the pollutant, to different sampling, having this focus on young people up to 17 years, the longer period of analysis (4 years) in relation to this study and the use of a different analysis model, the Poisson regression.
In the search of Gouveia et al, carried-out in São Paulo, Brazil, it was observed that an increase of 10ìg/m3 in the level of inhalable particulate matter is associated with an increase of 4.6% in hospital admissions for asthma in children8. In our study, for an increase of 10ìg/m3 of PM10, the odd of hospitalization increases from 5% to lag of 3 days, and 23% for 1-day lag.
The Air quality guideline (ACG) of the World Health Organization (WHO), published in 2005, accepted maximum daily exposure levels for the PM10 up to 50∝g/m3 and annual exposure to concentrations below 20 ∝g/m3, being acute exposures at levels greater than 150 ug/m3 associated with the increase of mortality by 5% due to cardiorespiratory changes caused by the pollutant.
The levels of annual average concentration of PM10 obtained in this study exceed acceptable levels by the WHO, and annual exposure levels above 70ug/m3 are associated with significant deleterious effects on health, leading to increased mortality by 15%13. This pollutant has as one of its main sources the vehicular fleet, directly interfering in their levels.
The sulfur dioxide, in turn, had a statistical significance in the second and third days of exposure, increasing the chance of at least one hospital admission between 17% and 36% for an increase of 10∝g/m3. This pollutant, in a study carried out in Sao Paulo by Braga et al, showed the largest contribution in hospital admissions for respiratory causes among children less than or equal to 2 years, decreasing with advancing age; when analyzed in a group of 0 to 19 years, was also found a significant increase in the hospital admissions7.
The maximum value of sulphur dioxide was 31ìg/m3 and its mean was 4.6 ∝g/m3. The maximum concentrations found in this study (31ìg/m3) are slightly above values recommended by the WHO, which accepts 20ug/m3 as maximum exposure level for 24 hours13.
Moreover, ozone was significant only in hospital admissions for asthma on the third day after exposure to the pollutant. This is according to a study by Bakonyi et al, which resulted in a statistically significant effect only in O3 for 3 days moving mean with respect to care for respiratory diseases .
In study carried out with students in Rio de Janeiro, there was a protective effect of ozone: the increase of 10∝g/m3 of O3 would be associated, one day after exposure, to an increase of 0.2 l/min in mean lung function and on the other hand, considering the indicator of three days of lag, there was a reduction in mean lung function, though no significant9. This situation is known as paradoxical ozone association.
For this pollutant, WHO guideline accepts maximum levels of exposure up to 100∝g/m3 eight hours a day. Levels above 240 ug/m3 are associated with significant effects on health such as decreased lung function, airway inflammation and respiratory hyperreactivity13. The mean of 24 hours was found to be 74.27∝g/m3 during the period of 2004 to 2005 years.
In addition to acute effects such as increased hospital admissions due to respiratory diseases, a study shows a strong relationship between chronic exposure to pollutants such as NO2 and PM10, and decreased lung development in children, resulting in adulthood by decreasing lung capacity and consequently with increased morbidity and mortality. It was not observed relationship of ozone exposure with decreasing pulmonary function in this cited study9. These data reinforce those found by Moura et al, in a study with one year time series including children up to 12 years about the role of PM10 exposure and visits in emergency rooms in a region of Rio de Janeiro22. Unlike Lin et al, it was not possible to identify the role of ozone on asthma hospitalization23.
It is noteworthy that, although the odds ratio values found were of small magnitude, the risk prevention can have a major economic and social impact on public health in Brazil, because of exposure to pollution is a frequent event and the high prevalence of symptoms related to asthma, has been estimated as of approximately 24% in Brazilian students (24).
Moreover, in our study, only the hospitalizations through the public health system were recorded, and may have been errors in coding of diagnoses and, also, double counting of the same patient; other situation is that only part of the survey cases that have resulted hospitalization for asthma, ignoring the crises and consultations that have not resulted in hospitalization. Individual exposures to the pollutants studied were not considered and a homogeneous atmosphere with the same level of exposure to all individuals was considered.
So, it was possible to identify an association between pollutants and hospital admissions for asthma, checking the increase of hospitalizations for asthma in according to particulate matter, sulfur dioxide and ozone exposure. This study may provide subsidies for the development of measures to reduce the health risks associated with pollution.
Camila Amancio thanks the São Paulo State Research Foundation (FAPESP) for the scholarship of scientific initiation (grant 2009/09487-4).
REFERENCES
1. Bakonyi SMC, Danni-Oliveira IM, Martins LC, Braga ALF. Air pollution and respiratory diseases among children in the city of Curitiba, Brazil. Rev Saúde Pública 2004;38(5):675-700 [ Links ]
2. Cançado JED, Braga A, Pereira LAA, Arbex MA, Saldiva PHN, Santos UP. Repercussões clínicas da exposição à poluição atmosférica. J Bras Pneumol 2006;32:S5-S11 [ Links ]
3. Tolbert PE, Mulholland JA, Maclntosh DL, Xu F, Daniels D, Devine OJ, et al. Air Quality and Pediatric Emergency Room Visits for Asthma in Atlanta, Georgia. Am J Epidemiol 2000;151:798-810 [ Links ]
4. J Castellsague, J Sunyer, M Sáez, J M Antó. Short-term association between air pollution and emergency room visits for asthma in Barcelona. Thorax 1995;50:1051-1056 [ Links ]
5. J Sunyer, C Spix, P Quénel, A Ponce-de-León, A Pönka, T Barumandzadeh, et al. Urban air pollution and emergency admissions for asthma in four European cities: the APHEA Project. Thorax 1997;52:760-765 [ Links ]
6. González Gómez JG, Barrera Gómez LE, Arévalo Orozco MA. Prevalencia del asma bronquial en la ciudad de Guadalajara, Jalisco, México. Alergia 1992;39:3-7 [ Links ]
7. Braga AL, Saldiva PH, Pereira LA, Menezes JJ, Conceição GM, Lin CA, et al. Health effects of air pollution exposure on children and Adolescents in São Paulo, Brazil. Pediatric Pulmonology 2001;31:106-113 [ Links ]
8. Gouveia N, Freitas CU, Martins LC, Marcílio IO. Hospitalizações por causas respiratórias e cardiovasculares associadas à contaminação atmosféricas no Município de São Paulo, Brasil. Cad. Saúde Pública 2006; 22(12): 2669-2677 [ Links ]
9. Castro HA, Cunha MF, Mendonça GAS, Junger WL, Cunha-Cruz J, Leon AP. Efeitos da poluição do ar na função respiratória de escolares, Rio de Janeiro, RJ. Rev Saúde Pública 2009; 43(1): 26-34 [ Links ]
10. Nascimento LFC, Pereira LAA, Braga ALF, Módolo MCC, Carvalho Jr JA. Efeitos da poluição atmosférica na saúde infantil em São José dos Campos, SP. Rev Saúde Pública 2006; 40(1) 77-82 [ Links ]
11. Ministério da Saúde [internet]. Brasil: Ministério da Saúde; 2010 [acesso em 29 jan 2010]. Disponível em: http://portal.saude.gov.br/saude/visualizar_texto.cfm?idtxt=23509 [ Links ]
12. DATASUS [internet]. Brasília: Ministério da Saúde. [acesso em 14 out 2009]. Departamento de Informações e Informática do Sistema Único de Saúde. Disponível em: http://tabnet.datasus.gov.br/cgi/tabcgi.exe?sih/cnv/mrsp.def [ Links ]
13. Organização Mundial da Saúde [internet]. Geneva: Organização Mundial da Saúde. [acesso em 24 set 2009]. Air Quality Guideline. Disponível em: http://www.who.int/phe/health_topics/outdoorair_acg/en [ Links ]
14. Braga ALF, Conceição GMS, Pereira LAA, Kishi HS, Pereira JCR, Andrade MF et al. Air pollution and pediatric respiratory hospital admissions in São Paulo, Brazil. J Environ Med 1999;1:95-102 [ Links ]
15. DATASUS [internet]. Brasília: Ministério da Saúde. [acesso 16 set 2009]. Departamento de Informações e Informática do Sistema Único de Saúde. Disponível em: http://w3.datasus.gov.br/datasus/index.php [ Links ]
16. Prefeitura Municipal de São José dos Campos [internet]. São José dos Campos: Prefeitura Municipal. [acesso em 4 fev 2010]. Disponível em: http://www.sjc.sp.gov.br/acidade/populacao.asp. [ Links ]
17. CETESB [internet]. São Paulo: CETESB [acesso 16 set 2009]. Companhia de Tecnologia de Saneamento Ambiental. Disponível em: http://www.cetesb.sp.gov.br [ Links ]
18. FUNCATE [internet]. São Paulo: FUNCATE [acesso 16 set 2009]. Fundação de Ciência, Aplicações e Tecnologia Espaciais. Disponível em: http://www.funcate.org.br [ Links ]
19. Bobak M. Outdoor air pollution, low birth weight, and prematurity. Environ Health Perspect 2000; 108:173-6 [ Links ]
20. Ritz B, Yu F, Fruin S, Chapa G, Shaw GM, Harris JA. Ambient air pollution and risk of birth defects in southern California. Am J Epidemiol 2002; 155: 17-25 [ Links ]
21. Hernández-Cadena L, Barraza-Villareal A, Ramírez-Aguilar M, Moreno-Macías H, Millar, Carbajal-Arroyo LA, et al. Morbilidad infantil por causas respiratórias y su relación con la contaminación atmosféricas en Ciudad Juárez, Chihuahua, México. Salud pública Mex 2007; 49:27-36) [ Links ]
22. Moura M, Junger WL, Mendonça GAS, Leon AP. Air quality and emergency pediatric care for symptoms of bronchial obstruction categorized by age bracket in Rio de Janeiro, Brazil. Cad. Saúde Pública 2009; 25(3): 635-644 [ Links ]
23. Lin S, Liu X, Lê LH, Hwang S-A. Chronic exposure to ambient ozone and asthma hospital admissions among children. Environ Health Perspect 2008; 116(12):1725-30 [ Links ]
24. Solé D, Wandalsen GF, CameloNunesIC, Naspitz CK, ISAAC Grupo Brasileiro. Prevalence of symptoms of asthma, rhinitis, and atopic eczema among Brazilian children and adolescents identified by the International Study of Asthma and allergies in Childhood (ISAAC) Phase 3. J Pediatr (Rio J). 2006-82: 3416. [ Links ]
 Corresponding author:
Corresponding author:
luiz.nascimento@unitau.br
Manuscript submitted Jun 25 2011
Accepted for publication Feb 10 2012

{kind=link}