










Services on Demand

article
 English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
Indicators
Share

 Permalink
PermalinkJournal of Human Growth and Development
Print version ISSN 0104-1282
Rev. bras. crescimento desenvolv. hum. vol.24 no.1 São Paulo 2014
ORIGINAL RESEARCH
Child Mortality in the Last Five-Year Periods in the City of Porto Velho, RO, Brazil
Kátia Fernanda Alves MoreiraI; Tathiane Souza de OliveiraII; Ticiana Albuquerque GonçalvesII; Cleson de Oliveira MouraIII; Sâmia Nagib MalufIV; Rosalina Semedo de Andrade TavaresIV; Carlos Mendes TavaresIV
IProfessora Associada. Universidade Federal de Rondônia. Rondônia, Brazil
IIDiscentes. Universidade Federal de Rondônia. Rondônia, Brazil
IIIProfessor Mestre em Ensino em Ciência em Saúde. Universidade Federal de Rondônia
IVUniversidade de Integração Internacional da Lusofonia Afro-Brasileira. Ceará, Brazil
ABSTRACT
OBJECTIVE: To analyze the evolution of child mortality.
METHODS: A descriptive ecological study was conducted. The database of deaths provided by the Mortality Information System between 2006 and 2010 was used. Only records in which the city of residence and occurrence of deaths corresponded to the city of Porto Velho and whose children were younger than 12 months at the time of death were included in this study. In addition, only deaths from preventable neonatal and post-neonatal causes were analyzed.
RESULTS: In the city of Porto Velho, during the period studied, there is a predominance of mothers aged between 20 and 34 years, whose percentages of child deaths varied between 26.0% in 2006 and 29.0% in 2010, with small variations in the remaining years. There was an increasing trend towards premature deaths, except in 2009, when the percentage was 45.0%. Between 2006 and 2007, this percentage remained at 50.0%, increasing to 53% in 2008 and subsequently to 54.0% of deaths among children younger than one year in 2010.
CONCLUSION: The estimate of incidence of child mortality in the period studied remained higher than the value expected by 2015 in Brazil.
Key words: evolution of child mortality, child health, public policies.
INTRODUCTION
Child mortality is understood as the number of deaths occurring between the time of birth and the first year of life, which is extremely influenced by socio-environmental, economic and health determinants. High child mortality rates reflect the living conditions of a certain population, in addition to being an efficient health indicator1 that can show the health status of this population, while the determinants refer to their risk of death2.
Deaths among children younger than one year are categorized into neonatal, which estimates the risk of death in the first 27 days of life, and post-neonatal, which estimates the risk of death between 28 days and the first year of life. The neonatal component, in its turn, is subdivided into early neonatal period, between zero and six days; and late neonatal period, between seven and 27 days3.
The child mortality rate (CMR) is assumed to be an excellent indicator of the quality of life of a population, capable of describing the health conditions of a society in terms of its level of development4. This rate is calculated by the ratio between the number of deaths among children younger than one year and the total number of live births (LB) in the same geographical location and period, multiplied by 1,0005.
The Child Mortality Coefficient (CMC) in Brazil is similar to those of developed countries in the 1960s, such as Canada and Japan, which currently have a CMC equal to 3/1,000 LB and 7/ 1,000 LB, respectively6. On the other hand, these rates are currently different from those of Angola and Afghanistan, whose CMC is approximately130/1,000 LB and 165/1,000 LB, respectively. These are developing countries with low economic power and, consequently, low social development6. Child mortality rates equal to or higher than 50 deaths/1,000 LB are considered to be high; between 20 and 49 deaths/1,000 LB, average; and lower than 20 deaths/1,000 LB, low7.
Several factors corroborate the reduction in child mortality in the country, among which are the improvements in basic sanitation, increase in the coverage of the Estratégia Saúde da Família (ESF - Family Health Strategy), especially for the maternal-child group, improvements in living and food conditions of the population, advances in health technologies, access to immunization, and mainly the promotion of exclusive maternal breast-feeding8.
One of the main Human Development Indicators (HDI) is the Child Mortality Coefficient (CMC) as it shows the socioeconomic level of a population, the quality of prenatal, childbirth, puerperal and infant care, apart from assessing other causes such as nutritional conditions, basic sanitation and immunization9.
Approximately 10 million children die annually worldwide10. However, the great majority of these deaths are preventable when there are improvements in the living conditions of the population, access to health services, and effectiveness of the actions provided to the population.
In the 1970s, Rutstein et al. (1976) presented their studies on the concept of preventable deaths or sentinel events were conducted11, showing that the majority of deaths among children younger than one year can be partly or completely prevented12 with the presence of effective health services13.
Preventable child deaths are associated with flaws in prenatal, childbirth and infant care, because they could be prevented through effective health services with preventive measures and treatment of the phenomenon or condition determining it. Access to health services and the quality of such services play an important role during prenatal care, in the perspective of following the entire gestational period and finding out the risk factors, aiming at an early intervention and the guarantee of the survival of newborns14.
Assuming that no information is unnecessary, the analysis of the evolution of child mortality from preventable causes is important due to its use as an indicator of quality of care for the population. Therefore, the study of the evolution of child mortality from preventable causes in the city of Porto Velho, RO, Northern Brazil, enables relevant resources the implementation of public policies that are egalitarian and suitable for cities, thus requiring research to understand this.
The present study analyzed the evolution of child mortality in the city of Porto Velho, focusing on preventable neonatal and post-neonatal causes between 2006 and 2010.
METHODS
A descriptive ecological study was conducted with data on live newborns and child deaths occurring between zero and 364 days of life, in the city of Porto Velho, RO, Northern Brazil, between 2006 and 2010. The study population is comprised of all deaths sent to and recorded in the Sistema de Informações sobre Mortalidade (SIM - Mortality Information System) database, found in the 0-to-6-day, 7-to-27-day, and 28-to-364-day age groups, living in Porto Velho, and of all Sistema de Informações sobre Nascidos Vivos (SINASC - Live Birth Information System) data on live newborns, both obtained from the Epidemiology Sector of the City of Porto Velho Department of Health. Data from this research project were approved by the Research Ethics Committee under CAAE 042/2010/CEP/NUSAU/UNIR.
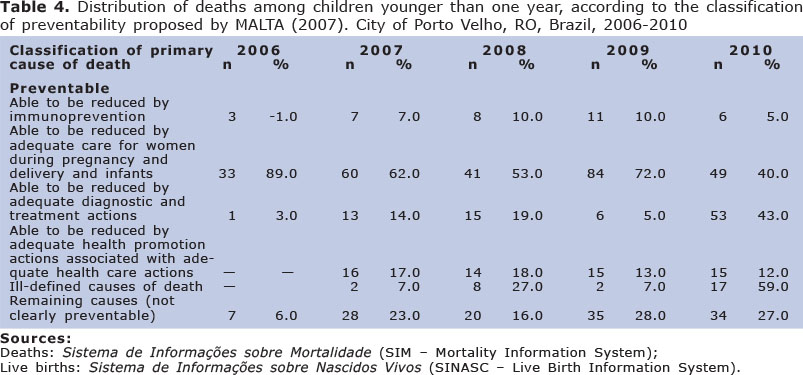
A database was constructed with the information about the total number of live newborns and child deaths by cause. All primary causes were coded according to the International Statistical Classification of Diseases and Related Health Problems - 10th Revision (ICD-10)15. Deaths were grouped by age (younger than 7 days; between 7 and 27 days; and between 28 and 364 days) and categorized into three groups: 1) preventable causes: 1.1) able to be reduced by immunopreventive actions; 1.2) able to be reduced by adequately caring for women during pregnancy and newborns; 1.3) able to be reduced by adequate diagnostic and treatment actions; 1.4) able to be reduced by adequate health promotion actions associated with adequate health care actions; 2) ill-defined causes of death: abnormal symptoms, signs and results of clinical and laboratory tests not classified elsewhere (from R00 to R99, except for R95); 3) remaining causes (not clearly preventable) described from the list of preventable causes of death through the Brazilian Sistema Único de Saúde (SUS - Unified Health System) actions between 2006 and 201016.
The 2006-2010 CMCs were calculated according to the data obtained, using the methodology proposed by the Rede Interagencial de Informações para a Saúde (RIPSA - Health Information Inter-Agency Network).
The descriptive data analysis was shown through frequency tables.
RESULTS
Among the five main primary causes of death among children younger than one year in the city of Porto Velho, the following stood out: septicemia, hypoxia and birth asphyxia (Table 5).
DISCUSSION
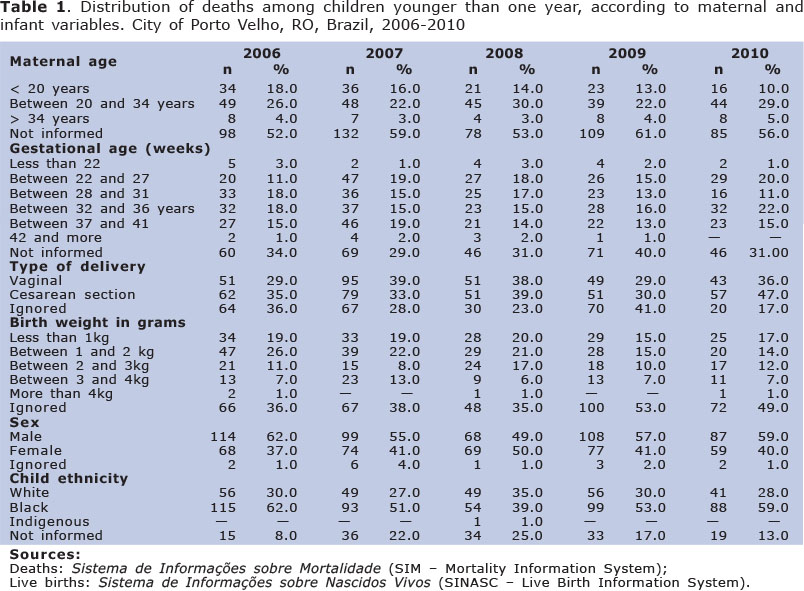
In the city of Porto Velho, during the period studied, there was a predominance of mothers aged between 20 and 34 years, whose percentages varied between 26.0% in 2006 and 29.0% in 2010, with small variations in the remaining years (Table 1).
Studies have reported that the maternal age when having a child is one of the factors positively associated with child mortality, especially when maternity occurs early or late throughout the female reproductive period, due to a series of behavioral, socioeconomic and biological factors17.
The present study revealed an increasing trend towards premature deaths, except in 2009, when the percentage was 45.0%. Between 2006 and 2007, this percentage remained at 50.0%, rising to 53% in 2008 and subsequently to 54.0% of deaths among children younger than one year in 2010, thus characterizing a high incidence of premature neonatal mortality.
Prematurity (gestational age lower than 37 weeks) is considered to be preventable by Decree 1,121/MS/200218, as the main causes of premature deliveries include genital infections, multiple deliveries, maternal hypertension, low pre-gestational body mass index (BMI), uterine dysfunctions and heavy maternal work19. Likewise, the increase in the rate of premature births may have resulted from induced Cesarean sections20.
The prevalence of Cesarean sections is considered to be high in the city of Porto Velho, during the period studied, varying between 35.0% and 47.0% of deliveries. Brazil has one of the highest percentages of Cesarean sections worldwide, totaling nearly 36.4% of all hospital deliveries21. In the international sphere, the accepted epidemiological standard for Cesarean deliveries is 15.0%22. Although there is little evidence that Cesarean sections increase the CMR, the high percentages indicate that many of these surgeries are voluntary.
Pregnant women have the right to adequate prenatal care and the right to receive guidance on warning signs during pregnancy and infant care. Thus, consultations during the puerperal period and family planning are important. Likewise, the population in general must be informed about the several technologies associated with pregnancy and childbirth, enabling women to choose the type of health care of their preference23.
In the present study, the majority of children who died had between 1 and 2 kg when they were born, with a significant decrease throughout this period (varying from 26.0% to 14% of deaths among children within this weight range). A study conducted in a different Brazilian city indicated that live newborns with a weight lower than 2.5 kg were at a higher risk of mortality when compared to those with a weight equal to or higher than 2.5 kg24. Therefore, low birth weight can be a predictive risk factor for child mortality and one of the most important indicators to evaluate the success of maternal health programs.
In the period studied, there was a higher incidence of deaths in male children than females, except for 2008 (Table 1). Being a male child is considered to be a risk factor for mortality in all stages of human life and the mortality coefficient of males is frequently higher than that of females in all ages25.
Likewise, there was a higher incidence of deaths in black children, especially in 2006 and 2010, when there were higher numbers of child deaths. This finding apparently indicates that being a black child is also a factor positively associated with child mortality.
The result of this finding about deaths among black children is similar to that of another study26, which showed a difference when black and white children were compared. In contrast, the later study showed higher values for causes considered to be preventable than the former one.
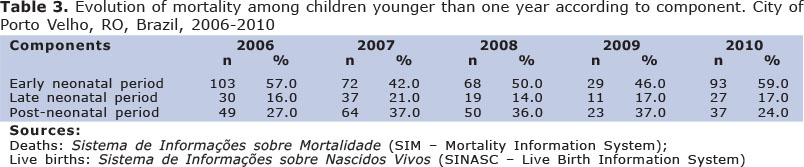
The present study revealed that, between 2006 and 2010, the city of Porto Velho had a child mortality rate that remained higher than the proposed goal for Brazil (15.7/1,000 LB until 2015). There was a predominance of early neonatal child mortality (< 7 days), when compared to the late neonatal or post-neonatal periods throughout the study period (Table 2).
The reduction in neonatal mortality must be viewed as a challenge, especially in the city of Porto Velho. This reduction is associated with the importance that city managers, services, the health system and society attribute to such high mortality rates, particularly on the first six days of life.
As early neonatal deaths occur in the 1st week of life, it is suggested that the "Rede Cegonha", a SUS-based initiative consisting of a health care network aimed at guaranteeing that women have the right to reproductive planning and humanized care during pregnancy, delivery and puerperium, and that children have the right to a safe birth and healthy growth and development, should be restructured, with investments in health care for pregnant women and newborns. The coverage of the maternal-child care network needs to be increased and the geographical and population criteria need to be redefined to facilitate access to this network by pregnant women, puerperae and newborns27.
High neonatal mortality rates are associated with unsatisfactory socioeconomic conditions, combined with the inadequate quality of health care provided to pregnant women and newborns. The public sector has encountered difficulties to reduce such high rates in the maternal-child component, as this would require more complex and higher-cost interventions28,29.
The reduction in neonatal mortality, which is divided into early neonatal period (0 to 6 days of life) and late neonatal period (7 to 27 days) is very slow, especially in the Northern region (Legal Amazon) and Northeastern region30. In the present study, the early neonatal component totaled 57.0% of deaths in 2006, decreasing to 42% in 2007 and thus showing a relative reduction in the total number of neonatal deaths in this period. In 2008, neonatal deaths totaled 50.0% of all deaths in this period, while this percentage was 46.0% and 59% in 2009 and 2010, respectively (Table 3).
With regard to the number of deaths among children aged between 28 days and one year, the results of this study indicated that the number of deaths in the post-neonatal period decreased throughout the years analyzed. In 2006, there were 27.0% of deaths, followed by 24.0% in 2010, the years when the lowest percentages of deaths occurred (Table 3).
Reduction in post-neonatal mortality in the city of Porto Velho follows the Brazilian standard. There has been a decreasing and stabilizing trend in mortality in several states in Brazil31. However, this situation should not be expected, in view of the socioeconomic development that this country has shown, the availability of knowledge and technologies32, and the universality of health care provided by the SUS. These deaths are considered to be a critical health problem, as they continue to be particularly associated with diarrhea and pneumonia and as they are potentially preventable33.
Results of this study show that there was a higher incidence of deaths from causes that can be prevented by adequate care for women during pregnancy and delivery and for newborns, when compared to other types of preventable deaths, reaching a peak in 2006. Likewise, they indicate a high incidence of deaths from preventable causes due to inadequate diagnostic and treatment actions (Table 4).
The identification of groups of causes of preventable deaths, both in the neonatal and postnatal periods, enables a more in-depth analysis of this situation, allowing comprehensive knowledge about the behavior of child mortality and resources for effective actions. However, there are few studies in the area of public health that categorize child deaths in terms of their preventability.
The results of the present study are in disagreement with those of other studies34,35 that show the main determining causes of child mortality, referring to perinatal diseases, newborns with low birth weight, congenital malformations, respiratory distress and bacterial septicemia. On the other hand, in Brazil, congenital malformations are pointed out as the second cause of child mortality, totaling 11.2% of deaths, whereas, in the United States, they are the main cause of death in the first year of life.
In a recent study about perinatal mortality and its associated components in an investigation about the history of gestations/deliveries37, the perinatal mortality coefficient was 12.7 per 1,000 births; 66.7% of the conceptuses were stillbirths and 33.3% were live births who died aged less than 7 days at the same hospital where they were born. Approximately 27% of the conceptuses were children of adolescent mothers and 44% of the mothers were primigravidae. Prenatal assistance was attended by 92% of the women; type of pregnancy showed 67.8% of preterm gestations with similar proportions for each one of the components. The coefficient for twin gestations was more than four times higher than the coefficient for mothers of singleton gestations. Regarding type of delivery, Cesarean sections corresponded to 31.1% of the total, and it is important to notice that there was a non-negligible amount of surgical deliveries in mothers whose product was a stillbirth. There was a relationship of the proportion of neonatal deaths in the first hours of life and the proportion of fetal deaths to the quality of the care offered in the women's pregnancy/puerperal cycle37.
In the present study, deaths from congenital malformations are not among the five main causes of death among children younger than one year during the study period. In contrast, there were high indices of preventable deaths that could be reduced through adequate care for women during pregnancy and childbirth and for newborns. The main cause of child mortality found in the present study was septicemia, which reached a peak (37.0%) in 2010, an alarming fact that indicates the need for urgent interventions. In view of these contexts of child mortality, especially with regard to the neonatal component (15.2%) in 2010, it is expected that the results of this study, combined with other inter-sectoral child care actions, contribute to decision-making, further reducing the number of neonatal deaths and child mortality in this city.
This commitment by the international leadership provides optimism that further progress towards achieving the MDG4 can be attained. With the share of under-five deaths during the neonatal period rising in every region and almost all countries, neonatal health will need to be addressed more effectively. Systematic action by governments and partner organizations is needed to reach women and babies with effective care. Highly cost-effective interventions are feasible even at the community level, and most can be linked with preventive and curative initiatives for mothers and babies36,37.
One of the limitations of this ecological study resulted from the presence of a significant number of variables with missing data, which reveals the underreporting of deaths that could affect data quality and, consequently, the interpretation of results. On the other hand, this study indicates the importance of implementing a service that constantly, systematically and fully records child death certificates and the strengthening of the city's child mortality committee, which could support the analysis of factors associated with child deaths and define their preventability.
REFERENCES
1. Jodas, D.A. Mortalidade evitável em menores de cinco anos: evento sentinela na qualidade dos serviços primários em Maringá-Paraná. 2010. 198 f. Dissertação (Mestrado em Enfermagem)- Escola de Enfermagem, Universidade Estadual de Maringá, Maringá, 2010. [ Links ]
2. Duarte, C. M. R. Qualidade de vida e indicadores de Saúde: Aspectos da mortalidade infantil no Estado do Rio de Janeiro e suas regiões. Cadernos de Saúde Pública, v. 8, p.414-427, 1992. [ Links ]
3. Caldeira, A.P.; França, E.; Perpétuo, I.H.O.; Goulart, E.M.A. Evolução da mortalidade infantil por causas evitáveis, Belo Horizonte, 1984-1998. Rev Saúde Pública. v.39, n. 1, p.67-74, 2005. [ Links ]
4. Fischer, T.K.; Lma, D.; Rosa, R.; Osório, D.; Boing, A.F. A mortalidade infantil no Brasil: série histórica entre 1994-2004 e associação com indicadores socioeconômicos em municípios de médio e grande porte. Medicina (RibeirãoPreto). 40 (4): 559-66, 2007. [ Links ]
5. Laurenti, R; Mello Jorge, M.H.P. de. Lebrão, M.L.; Gotlieb, S.L.D. Estatísticas de saúde. 2. ed. rev. e atual. São Paulo: EPU, 2005. [ Links ]
6. Organizações Mundial da Saúde (OMS). Estatísticas mundiais de saúde. 2010. Disponível em: http://www.who.int/whosis/whostat/EN_WHS10_Full.pdf. Acesso em: 21/jul/2012. [ Links ]
7. Pereira, M.G. Epidemiologia: teoria e prática. 6. Ed. Rio de Janeiro: Guanabara Koogan, 2002. 231p. [ Links ]
8. Lansky et al. Mortalidade infantil em Belo Horizonte: avanços e desafios. Revista da RMMG, Minas Gerais, v. 1, p. 1-10, 2007. [ Links ]
9. Fundo das Nações Unidas para a Infância (UNICEF). Situação da infância brasileira, 2006. Brasília: UNICEF, 2008a. [ Links ]
10. Fundo das Nações Unidas para a Infância (UNICEF). Situação da infância brasileira, 2006. Brasília: UNICEF, 2008b. [ Links ]
11. Rutstein, D.D.; Berenberg, W.; Chalmers, T.C.; Child, C.G.; Fishman, A.P.; Perrin, E.B. Measuring the quality of medical care: a clinical method. The New England Journal of Medicine. n. 294, p.582-8, 1976. [ Links ]
12. Alves, A. C. et al. Principais causas de óbitos infantis pós-neonatais em Belo Horizonte, Minas Gerais, Brasil, 1996 a 2004. Revista Brasileira de Saúde Materno Infantil, Recife, v. 8, n. 1, p. 27-33, 2008. [ Links ]
13. Malta, D.C.; Duarte, E.C.; Almeida, M.F.; Dias, M.A.S.; Morais NETO, O.L.; Moura, L. et al. Lista de causas de mortes evitáveis por intervenções do Sistema Único de Saúde do Brasil. EpidemiolServSaúde. 16(4): 233-44, 2007. [ Links ]
14. Malta, D.C.; Duarte ,EC..; Escalante ,J.J. C.; Almeida, M.F.A.; Sardinha, L. V.; Macário, E.M.; Monteiro, R.A.M.; Morães Neto, O.L.M. Brasil, 1997 a 2006: contribuições para a avaliação de desempenho do Sistema Único de Saúde. Cad. Saúde Pública, Rio de Janeiro, v.26, n.3, p.481-491, 2010. [ Links ]
15. Organizações Mundial da Saúde (OMS). Relatório Mundial da Saúde 2008. Cuidados de saúde primários: agora mais do que nunca. [online] Genebra: OMS; 2008. Disponível em: http://www.who.int/whr/2008/whr08_pr.pdf Acesso em 20 fev 2010. [ Links ]
16. Malta, D.C.; Duarte, E.C.; Almeida, M.F.; Dias, M.A.S.; Morais NETO, O.L.; Moura, L. et al. Lista de causas de mortes evitáveis por intervenções do Sistema Único de Saúde do Brasil. EpidemiolServSaúde. 16(4): 233-44, 2007. [ Links ]
17. Araújo, B.F. et al. Mortalidade neonatal precoce no município de Caxias do Sul: um estudo de coorte. Jornal de Pediatria, Rio de Janeiro, v. 76, n. 3, p. 200 - 206, 2000. [ Links ]
18. Brasil. Ministério da Saúde. Secretaria de Atenção à Saúde. Pacto nacional pela redução da mortalidade materna e neonatal. Brasília: Ministério da Saúde, 2004. [ Links ]
19. Rede Interagencial de Informações para a Saúde (Brasil). Indicadores e dados básicos para a saúde - IDB 2001. Brasília, DF: Ministério da Saúde, 2001. Disponível em: <http://www.opas.org.br/publicmo.cfm?>. Acesso em: 25 mai. 2010. [ Links ]
20. Barros, F. C. et al. The challenge of reducing neonatal mortality in middle-income countries: findings from three Brazilian birth cohorts in 1982, 1993 and 2004. Lancet, London, v. 365, n. 9462, p. 847-54, 2005. [ Links ]
21. Victora, C. G. Intervenções para reduzir a mortalidade infantil pré-escolar e materna no Brasil. Revista Brasileira de Epidemiologia, São Paulo, v. 4, n. 1, p. 3-69, 2001. [ Links ]
22. Fescina, R.H. A incidência de cesárea nas Américas. J Febrasgo, n. 1, p.7-8, 2000. [ Links ]
23. Fernandes, J.S. Mortalidade infantil por causas evitáveis na 18ª coordenadoria regional de saúde do rs - análise descritiva do ano de 2003. 2005. 61 f. Dissertação (Monografia)- Centro Universitário Feevale Instituto de Ciências da Saúde, Novo Hamburgo, 2005. [ Links ]
24. Silva, A. A. et al. Young maternal age and preterm birth. Paediatric and Perinatal Epidemiology, England, v. 17, n. 4, p. 332-339, Oct. 2003. [ Links ]
25. Pereira, M.G. Epidemiologia: teoria e prática. 6. Ed. Rio de Janeiro: Guanabara Koogan, 2002. 231p [ Links ]
26. Cunha, P.G.M. Estela. Mortalidade infantil por raça/cor, et al. I Seminário Saúde da População Negra, 2004. [ Links ]
27. Fréu et al. Determinantes da mortalidade neonatal de uma coorte de nascidos vivos em Passo Fundo - RS, 2003-2004. Revista da AMRIGS, Porto Alegre, v.52, n.2, p. 97-102, 2008. [ Links ]
28. Gastaud, A.L.; Honer, M.R.; Cunha, R.V. Mortalidade Infantil e evitabilidade em Mato Grosso do Sul, Brasil, 2000 a 2002. Rio de Janeiro, Cad Saúde Pública, v. 24, n.7, p.1631-1640, 2008. [ Links ]
29. Iams, J.D.; Romero, R.; Culhane, J.F.; Goldenerg, R.L. Primary, secondary, and tertiary interventions to reduce the morbidity and mortality of preterm birth. Lancet, n. 371, p.164-75, 2008. [ Links ]
30. Brasil. Ministério da Saúde. Indicadores e dados básicos - Brasil 2009. Brasília: Ministério da Saúde, 2009. [ Links ]
31. Caldeira, A. P.; Gonçalves, E. Avaliação de impacto da implantação da Iniciativa Hospital Amigo da Criança. Jornal de Pediatria, Rio de Janeiro, v. 83, n. 2, p. 127-132, 2007. [ Links ]
32. Brasil. Ministério da Saúde. Pacto pela redução da mortalidade infantil nordeste- Amazônia legal. [online] Brasília; 2009. [Disponível em: http://portal.saude.gov.br/portal/saude/profissional/area.cfm?id_area=1583. Acesso em 19 jun 2010. [ Links ]
33. Brasil. Ministério da Saúde . DataSUS. Informações de Saúde. Brasília: 2005. Disponível em: http//www.datasus.gov.br. Acesso em: 13 jul. 2009. [ Links ]
34. Amorim, M. M. R. de et al. Impacto das malformações congênitas na mortalidade perinatal e neonatal em uma maternidade-escola do Recife. Rev. Bras. Saúde Mater. Infantil. [online], n.6, p.19-25, 2006. [ Links ]
35. Soares, VMN; Schor, N; Tavares, CM. Vidas arriscadas: uma reflexão sobre a relação entre o número de gestações e mortalidade materna. Journal of Human Growth and Development, 2008: 18(3): 254-263. [ Links ]
36. Atrash HK. Childhood mortality: still a global priority. Journal of Human Growth and Development. 2013;23(3): 257-260. [ Links ]
37. Laurenti R, et al. Perinatal mortality in hospitals of the state of São Paulo: methodological aspects and some characteristics of mothers and conceptuses. Journal of Human Growth and Development. 2013, 23(3): 261-269. [ Links ]
Manuscript submitted Aug 01 2013
Accepted for publication Dec 28 2013
Corresponding author: katiaunir@gmail.com and tavares.is.c@gmail.com

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}