










Services on Demand

article
 English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
 Curriculum ScienTI
Curriculum ScienTIIndicators
Share

 Permalink
PermalinkSMAD. Revista eletrônica saúde mental álcool e drogas
On-line version ISSN 1806-6976
SMAD, Rev. Eletrônica Saúde Mental Álcool Drog. (Ed. port.) vol.11 no.3 Ribeirão Preto Sept. 2015
https://doi.org/10.11606/issn.1806-6976.v11i3p136-144
ORIGINAL ARTICLE
DOI: 10.11606/issn.1806-6976.v11i3p136-144
Mortality caused by the consumption of alcoholic beverages
Anna Klara BohlandI; Arquimedes Ribeiro GonçalvesII
IPhD, Adjunct Professor, Universidade Federal de Sergipe, Aracaju, SE, Brazil
IIPhysician
ABSTRACT
The abusive consumption of alcohol expresses itself into a serious public health problem throughout the world. The objective of this study was to describe the deaths which are caused by alcohol in Sergipe between 1998 and 2010. Data have been collected using the Mortality Information System and were analyzed by the TabWin program. An increase has been observed in the number and the coefficients in the whole regional health, among men, at the age between 45 and 54 years, in a hospital environment and whose root cause was related to mental and behavioral disorders. In this way, by extending the approach of mortality, this study can help in future research, as well as contributing to health managers, especially regarding mental health.
Descriptors: Mortality; Alcohol-Induced Disorders; Alcoholic Beverages.
Introduction
Alcohol is considered a major contributor to the disease burden and premature deaths worldwide(1). Most hospital costs resulting from the use of psychoactive substances in Brazil is due to the misuse of alcohol (83.1%) against 16.9% regarding the expenses coming from the use of other psychoactive substances(2) .
The drugs, the alcohol and the lawful use, with great reach and social acceptance, however, their excessive consumption causes medical, psychological, professional and family problems, leading to high economic and social costs(3-4). This is a paradoxical fact, since this substance has its use accepted and even encouraged in various situations, such as religious rituals, family ceremonies, get-togethers with friends, celebratory events and popular festivals, among others(5).
The alcohol intake was evaluated in 193 countries, and it was found that worldwide about 2.5 million people die every year because of abusive consumption, resulting in approximately 4.0% of total deaths(4), which is a serious problem for public health(6).
Alcohol consumption is one of the main risk factors for premature mortality around the world, accompanied by smoking, obesity, physical inactivity and high blood pressure, being directly or indirectly connected to the development of numerous diseases, such as liver cirrhosis, arterial hypertension, cardiomyopathy, alcohol dependence, nutritional deficiencies, neurological disorders and numerous types of cancer(7-10), besides traumatic and violent situations such as accidents at work, traffic accidents, domestic violence and homicide(4). One of the ways to approach alcohol disorders(11) is through life cycles; each step involves a number of risks, and is concluded by the necessity of preventive efforts and treatment strategies. Certain social sectors or circumstances should be free of alcohol and in particular should not be consumed during childhood and adolescence(12). Other situations are when driving a vehicle or during pregnancy(1). Workplace, social, physical, legal, family and other related violence are also(5) singled out as problems related to alcohol use.
However, there are reports which state that moderate intake of alcohol has a protective effect regarding cardiovascular disease, which presents lower mortality rates compared to teetotalers and people who take part in exaggerated use(13).
To prevent deaths related to alcohol consumption(14), ways of prevention and health promotion are necessary, including those regarding the school population(15), aiming at the reduction of consumption and consequent reduction of the risk of disease and early death.
In the world, the population who is most affected by alcohol related deaths (4) are men from Europe (10.8%), from the USA (8.7%) and from Oceania (8.5%). Populations who suffer less consequences are from Eastern Mediterranean (0.9%), from Africa (3.4%) and from Southeast Asia (3.7%), especially regarding countries and regions with a Muslim culture, where this habit is forbidden because of religious and cultural reasons. Among women, there are more deaths in Europe and America (1.7% in both cases), followed by Oceania (1.5%), Africa (1.0%), Asia (0.4%) and the Eastern Mediterranean (0.2%).
Research regarding addiction in the European Union between 1980 and 2003, has shown that deaths related to alcohol accounted for over 10% of all mortality, and the authors highlighted the importance of national prevention strategies (16) .
In Brazil, the Ministry of health (MS) (17) revealed that there was an increase from 16.1% to 19.0% regarding Brazilians who have admitted the abuse of alcohol (consumption of five doses of alcohol in a single time for men and four for women) between 2006 and 2008. In the same period there was an increase in diseases and mortality coefficient attributable to the abusive consumption of this substance.
MS found that between 2000 and 2006 in Brazil 92,946 deaths have been registered, whose root cause was one of the diseases directly attributable to alcohol, and 146,349 had this group of diseases as root cause or associated cause(18). Another study(19) conducted in the country, between 2006 and 2010, showed deaths linked to mental and behavioral disorders due to use of alcohol by units of the Federation. The state of Minas Gerais presented the greatest mortality coefficient. Other places with relevant indices of mortality were the States of Ceará and Sergipe. Given this, the objective, in this work, is to describe the deaths attributable to alcohol in Sergipe, between 1998 and 2010.
Method
We conducted a study of mortality, showing as the cause of death of alcoholic beverage consumption. To this end, the data were collected by the Mortality information system (SIM)(20). The methodological procedure used was the descriptive epidemiology. We analyzed the categories and subcategories of the International statistical classification of diseases and Related Health Problems-10th revision (ICD 10)(21), containing, as root cause in the Declaration of death, diseases whose policies, by definition, are fully attributable to alcohol(22) .
Natural causes related to the exposure to alcohol
E244 - Pseudo-Cushing Syndrome induced by alcohol
F10 - Mental and behavioral disorders associated with the use and abuse of alcohol
G312 - Degeneration of the nervous system due to alcohol
G405 – Special Epileptic Syndromes
G621 - Alcoholic Polyneuropathy
G721 - Alcoholic Myopathy
I426 - Alcoholic Cardiomyopathy
K292 - Alcoholic Gastritis
K70 - Alcoholic liver disease
K852 - Acute pancreatitis induced by alcohol
K860 - Cryogenic designs-chronic pancreatitis induced by alcohol
O354 - Assistance to the mother regarding injuries caused to the fetus by maternal alcoholism
P043 - Fetus or newborn affected by the use of alcohol by mother
Q860 - Fetal alcohol Syndrome
R780 - Presence of alcohol in the blood
External causes related to the exposure to alcohol
T51 - toxic effects of ethanol
X45 - Accidental poisoning by alcohol exposure
X65 - Voluntary self-poisoning by alcohol
Y15 - Alcohol poisoning with undetermined intent
Y90 - Evidence of alcoholism detected by/alcohol rates
Y91 - Evidence of alcoholism determined by the level of intoxication.
Data were analyzed by the program TabWin(20). In addition to the number and percentage of deaths, it was calculated that the annual mortality is coefficient because of the consumption of alcohol in the State of Sergipe, whose population was also provided by the DATASUS(20). The calculations of coefficients for each of the seven regional health (Aracaju, Brazil, Nossa Senhora (NS) do Socorro, NS da Glória, Lagarto, Estância e Propriá). In addition to this, other variables were included: sex, age group and place of occurrence. Finally, it is noteworthy that this work was approved by the Research Ethics Committee of the Universidade Federal of Sergipe (CAEE: 12699213.5.0000.5546).
Results
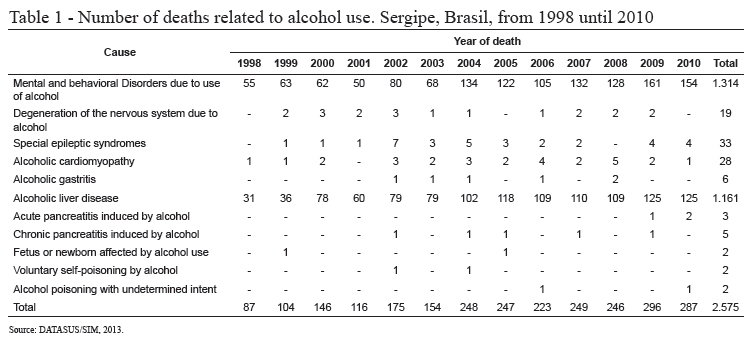
In Sergipe, in the period between 1998 and 2010, a total of 2,575 deaths, whose root cause was related to alcohol consumption we collected. These deaths (table 1) were distributed mainly in: mental and behavioral disorders related to alcohol (1,314) and alcoholic liver disease (1,161), and the other cases (100) in other categories.
Of these 2,575 cases, those with the dependency syndrome were the most frequent, with a total of 1,129 deaths (43.8%). In the category of alcoholic liver disease, the disease that predominated was alcoholic liver cirrhosis, with 674 deaths (26.2%), followed by alcoholic liver failure with 240 cases (9.3%).
According to table 2, during the examination period in the State of Sergipe, there has been increase by 1.7 times regarding the mortality coefficient because of the consumption of alcoholic beverages (from 5.1 deaths/100,000 inhabitants to 13.9 deaths/100,000 inhabitants.
2,306 male deaths were observed and 267 female deaths. Regarding males, the deaths were prevalent mental and behavioral disorders due to the use of alcohol, with 1,186 (51.4%) and 1,026 deaths from alcoholic liver disease (44.5%), while among women there was a predominance of deaths by alcoholic liver disease with 133 (49.8%) and 128 for mental and behavioral disorders due to alcohol use (47.9%).
In females, there was a growth from 0.9 deaths/100,000 women to 2.6 deaths/100,000 women (table 2). In males, an increase from 9.5 deaths/100,000 men to 25.8 deaths/100,000 men has been observed. The increase was an increase by 1.9 times in female mortality coefficient and regarding males there was an increase by 1.7 times. Also observed was the average coefficient of 19.1 deaths/100,000 men and 2.1 deaths/100,000 women in the period.
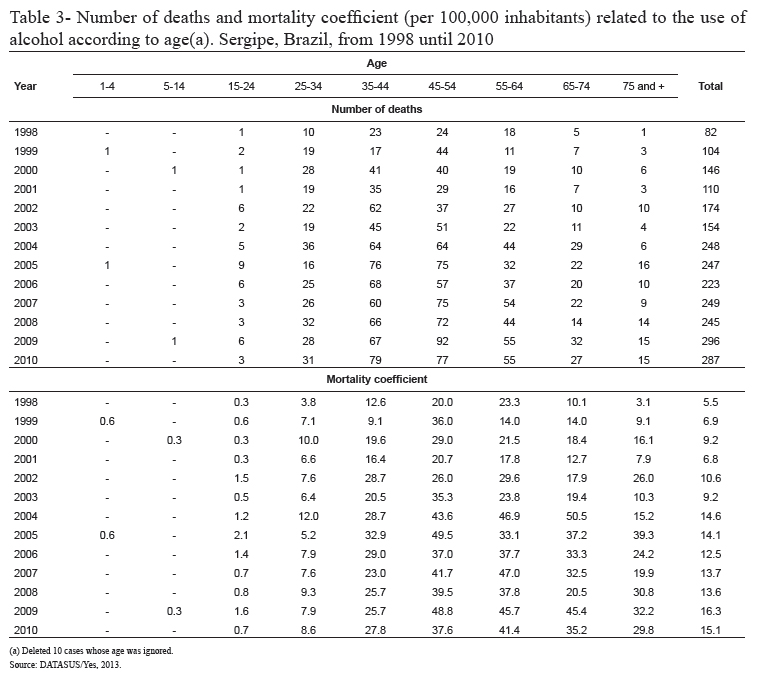
In relation to the age of death (table 3), a predominance of age between 45 and 54 years (28.9%) has been observed, followed by the 35 and 44 years (27.2%), with 1,412 deaths or 56.1% of the total. In the analyzed period, there was an increase in the number of deaths in all age groups from 25 years. The mortality of age less than 35 years were lower than the average coefficient (11.4/100,000 inhabitants), once again highlighting the mortality factors in the rage of 45-54, followed by the ranges 55-64 and 65-74.
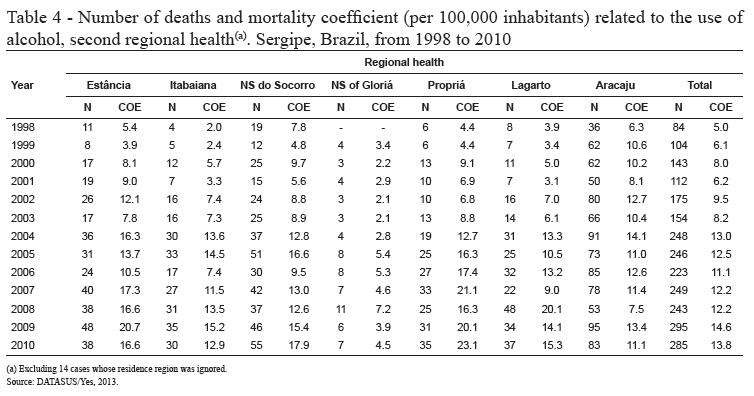
Table 4 shows the number of deaths and the coefficients for regional health. Aracaju is amongst the regions which shows the largest absolute number, with 914 cases (35.7%), followed by NS do Socorro with 418 (16.3%), Estância with 353 (13.8%), Lagarto with 292 (11.4%), Itabaiana with 263 (10.3%), Propriá with 253 (9.9%) and NS of Gloriá with 68 deaths (2.7%).
There was a predominance of cases of mental and behavioral disorders due to alcohol, in five of the State’s health regional, with exception of Lagarto and NS do Socorro, where the alcoholic liver disease deaths were the most frequent.
Among the health regions of the State regarding mortality coefficient, Aracaju was the region which showed greater stability, while the region of Propriá showed the largest growth during the study period. The regions of Propriá, Estância, NS do Socorro and Aracaju had the greatest coefficients. Besides NS Da Gloriá, only Lagarto and Itabaiana showed a lower mortality coefficient than the State of Sergipe.
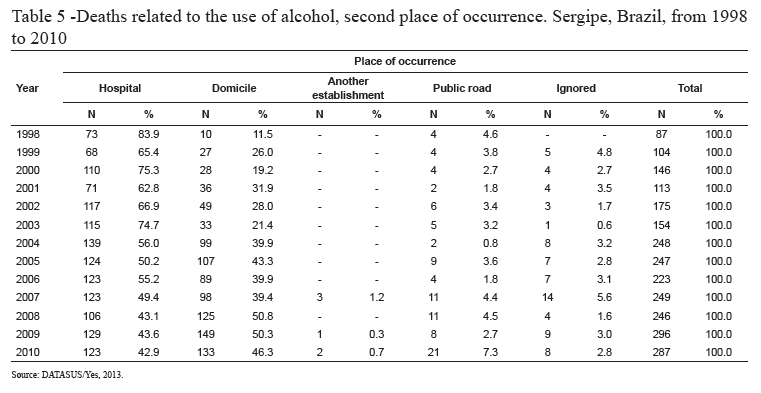
In relation to the place of the occurrence (table 5), a predominance of deaths in hospitals, with 1,421 cases (55.2%) have been observed. In that same time period, there were 983 domicile deaths (38.2%) and 91death (3.5%) on public roads. It is worth noting that over the period, the percentage of domicile deaths increased from 11.5% in 1998, to 46.3%, in 2010.
Discussion
In Sergipe a predominance of deaths regarding mental and behavioral disorders due to alcohol and related to the alcoholic liver disease have been observed. These results are consistent with those taken from the capitals of the North, Southeast and Midwest(15). According to the authors, in the Northeast and South, there were more deaths from alcoholic liver disease.
The data also showed an increase in mortality directly attributable to the consumption of alcohol in the State of Sergipe, between 1998 and 2010 regarding both sexes, which is likely due to the increasing beverage consumption pattern, both in men and in women(23). Similar results were obtained by MS(18), which also found that the consumption is more intense in the country.
The male deaths regarding mental and behavioral disorders due to alcohol (1,186), are different from the female deaths, which were for alcoholic liver disease (133). Men continue to be responsible for most cases(23). A 9/1 scale has been observed regarding male and female deaths, similar to the scale found for Brazil(15), between 1998 and 2002.
However, the rate of mortality among women has been growing with higher indexes than verified for males. Although this difference is not as articulate (1.9 times against 1.7 times), both men and women are dying more each time due to alcohol abuse. Such facts are confirmed by MS, who have observed an increase in excessive use of alcohol among women, from 8.1% in 2006, to 10.5% in 2008 (17) .
The present study showed that the abusive consumption of alcohol in the State of Sergipe was directly responsible for 2.0% of total deaths, being 3.2% of men and 0.5% of women. This rate is higher than found in Brazil between 1998 and 2002(15), which showed a 0.8% of male deaths and 0.1% of female death where alcohol was directly responsible for mental and behavioral disorders due to use of alcohol. These results demonstrate the importance of studying mortality and covering all the alcohol-related causes(22).
Male mortality coefficients obtained in the present, were larger than those observed in the series in Portugal (24) (in which there was an increase in mortality coefficient, from 19.7 in 2006 to 22.7 deaths per 100,000 inhabitants in 2009). Among women, the Portuguese study also showed lower numbers in relation to men, but also recorded an increase in the series (in 2006 from 3.1 to 3.7 fatalities in 2009 per 100,000 women younger than 65), therefore, higher than the one found in the present study.
The age group that presented the highest number of deaths in the State is the one that lies between 45 and 54 years, being similar to a recently held national survey (18). Data of the OMS(1) showed that alcohol was the main risk factor for death among men aged between 15 and 59 years.
As well as in Portugal, in the year 2010(24), there has been an increase in mortality directly attributable to alcohol, in all regions of the health state of Sergipe, which indicates that the consumption has increasingly intensified. The OMS also mentions increased mortality attributable to alcohol in the countries in economic growth , such as Brazil and China(1) .
Regarding the place of the occurred death, the majority have taken place in hospital environment. However, it has been observed that there was an increase of deaths at home, almost seven times bigger than the growth observed in hospitals. When analyzing the total deaths during the period, regardless of the cause, the percentage of calls was 33.2%, with a downward trend(20), but, in the present study, as mentioned above, the percentage of domicile deaths was 38.0%, in other words a sharply increasing trend.
The growing trend in the number of deaths in the home environment can be indicative that individuals or their families, by not being aware of their condition, are neglecting medical assistance being part of health services in order to combat stigma and prejudice(25).
Final considerations
It is worth noting that in this study only the deaths caused directly by the excessive consumption of alcohol were analyzed, being excluded are the cases where the substance is a factor associated with traffic accidents, domestic violence, homicide, heart disease or cancer.
It has been observed that the consumption of alcoholic beverages in Sergipe has been showing increasing levels of mortality in all health regions, in both sexes, being prevalent among men, however, has shown a more articulate increase in female mortality coefficient.
As in the present study we used the mortality attributable to alcohol, it can support future research and contribute to health managers, and in particular to mental health managers. The results indicate that the issue needs to be addressed and that, although there is no specific legislation concerning actions aimed at comprehensive care to people who consume alcohol, this still does not translate effectively in health actions.
At last, it is known that the fraction of risk attributable to alcohol consumption is higher than observed in this research. Because amongst the conditions of death or disease that are fully related to this cause, the conditions for which alcohol was only a component are also included. And therefore is much higher than concluded, revealing that today this is a topic worth considering as an important public health issue.
References
1. World Health Organization. Global status report on alcohol and health. Geneva; 2011. [ Links ]
2. Ministério da Saúde (BR). Secretaria de Atenção à Saúde. SVS/CN-DST/AIDS. A Política do Ministério da Saúde para atenção integral a usuários de álcool e outras droga. 2ed. Brasília: Ministério da Saúde; 2004. Série B. [ Links ] Textos Básicos de Saúde.
3. Almeida JC, Campos JADB. Desordens devido ao álcool em adolescentes: confiabilidade de um instrumento de medida. Alim Nutr. jun 2009;20(3):435-40. [ Links ]
4. World Health Organization. Sixtieth World Health Assembly A60/14 Add.1 Evidence-based strategies and interventions to reduce alcohol-related harm. Provisional agenda item 12.7. GENEVA; 14–23 May 2007. [ Links ]
5. Laranjeira R, Pinsky I, Zaleski M, Caetano R. I Levantamento Nacional sobre os padrões de consumo de álcool na população brasileira. Brasília: Secretaria Nacional Anti-Drogas; 2007. [ Links ]
6. Babor TF. La ciencia de la salud pública y la estrategia mundial sobre el alcohol. Bol OMS. 2010;88:643-3. [ Links ]
7. Organisation Mondiale de la Santé. Programme d’action combler les lacunes en santé mentale (mhGAP): élargir l’accès aux soins pour lutter contre les troubles mentaux, neurologiques et liés à l’utilisation de substances psychoactives. Genève; 2008.
8. Whunch V Filho. Consumo de bebidas alcoólicas e risco de câncer. Revista USP. dez 2013;96(1):39-44. [ Links ]
9. Baan R, Straif K, Grosse Y, Secretan B, Ghissassi FE, Bouvard V, et al. Carcinogenicity of alcoholic beverages. Lancet Oncol. 2007 Apr;8(4):292-3. [ Links ]
10. Boffetta P, Hashibe M, Vecchia CL, Zatonski W, Rehm J. The burden of cancer attributable to alcohol drinking. Int J Cancer. 2006 Aug;119(4):884–7. [ Links ]
11. Gunzerath L, Hewitt BG, Li TK, Warren KR. Alcohol research: past, present, and future. Ann N Y Acad Sci. 2011 Jan;1216(Addiction Reviews):1–23. [ Links ]
12. Lei nº 13.106, de 17 de março de 2015 (BR) [Internet]. [Acesso 18 abril 2015]; Disponível em: http://www.planalto.gov.br/CCIVIL_03/_Ato2015-2018/2015/Lei/L13106.htm [ Links ]
13. Moura JP. Álcool e o risco cardiovascular: a propósito de novas metanálises. Rev Fatores Risco. out 2011;23:(4)14-7. [ Links ]
14. Benedicto RP. Causas múltiplas de morte relacionadas ao consumo de álcool na microrregião de Ribeirão Preto–SP, 1996–2007. [Dissertação de mestrado em Enfermagem Psiquiátrica]. Ribeirão Preto: Escola de Enfermagem de Ribeirão Preto da universidade de São Paulo; 2011. 92 p. [ Links ]
15. Marín-Leon L, Oliveira HB, Botega NJ. Mortalidade por dependência de álcool no Brasil:1998 - 2002. PsicolEstudo. jan 2007;12(1):115-21. [ Links ]
16. Innamorati M, Pompili M, Martinotti G, Serafini G, Amore M, Lester D, et al. Trends in alcohol-related deaths in the EU countries in 1980-2003 Int J Soc Psychiatry. 2013 Apr;59(5):443-51. [ Links ]
17. Ministério da Saúde (BR). SUS. Cresce o consumo de álcool entre os brasileiros-VIGITEL 2008. [Internet]. [Acesso 13 jan 2014]; Disponível em: http://portalsaude.saude.gov.br/index.php/cidadao/principal/agencia-saude/noticias-anteriores-agencia-saude/3479-cresce-o-consumo-de-alccol-entre-os-brasileiros [ Links ]
18. Ministério da Saúde (BR). Secretaria de Vigilância em Saúde. Departamento de Análise de Situação em Saúde. Saúde Brasil 2007: uma análise da situação de saúde. Brasília: Ministério da Saúde; 2008. Série G. [ Links ] Estatística e Informação em Saúde.
19. Confederação Nacional dos Municípios. Mortes causadas pelo uso de substâncias psicotrópicas no Brasil [Internet]. Brasília; 2012. [Acesso 12 jan 2013]. Disponível em: http://www.clicrbs.com.br/pdf/12985756.pdf
20. Ministério da Saúde (BR). Informações de Saúde. [Internet]. Brasília, 2013. [Acesso 13 jan 2013]. Disponível em: http://www2.datasus.gov.br/DATASUS/index.php?area=0205
21. Organização Mundial da Saúde. Classificação internacional de doenças e problemas relacionados à saúde. Décima revisão. São Paulo: Centro Colaborador da OMS para a Classificação de Doenças em Português; 1993. [ Links ]
22. Rehm J. The risks associated with alcohol use and alcoholism. Alcohol Res Health. 2011 Mar;34(2):135-43. [ Links ]
23. Andrade AG, Silveira CM. Problemas comportamentais ligados ao uso de álcool. Revista USP. dez 2013;96(1):9-19. [ Links ]
24. Ministério da Saúde (PT). Plano Nacional de Saúde. Mortalidade por doenças atribuíveis ao álcool antes dos 65 anos [Internet]. [Acesso 30 jan 2013]; Disponível em: http://impns.dgs.pt/doencas-mentais/mortalidade-por-doencas-atribuiveis-ao-alcool-antes-dos-65-anos. [ Links ]
25. Ministério da Saúde (BR). Portaria GM/MS Nº 3.088, de 23 de dezembro de 2011. ]. [Acesso 30 jan 2013; Disponível em: http://www.brasilsus.com.br/legislacoes/gm/111276-3088.html [ Links ]
![]() Correspondence
Correspondence
Anna Klara Bohland
Universidade Federal de Sergipe. Departamento de Medicina
Rua Cláudio Batista, s/n
Bairro: Santo Antônio
CEP: 49060-100, Aracaju, SE, Brasil
E-mail: anna.bohland@uol.com.br
Received: July 1st 2014
Accepted: May 19th 2015

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}