










Services on Demand

article
 English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
Indicators
Share

 Permalink
PermalinkJournal of Human Growth and Development
Print version ISSN 0104-1282
Rev. bras. crescimento desenvolv. hum. vol.23 no.1 São Paulo 2013
ORIGINAL RESEARCH
Excessive daytime sleepnessand cardiometabolic risk factors in children and teenagers with overweight
Aline Silva Santos SenaI; Anajás da Silva CardosoI; Danielle Franklin de CarvalhoI; Jovany Luís MedeirosI; Giselda Félix CoutinhoII; Fernanda Cruz de Lira AlbuquerqueIII; Carla Campos Muniz MedeirosI,III
IMSs in Public Healthat the State Universityof Paraíba
IIDepartment of Physiotherapy, State Universityof Paraíba
IIICenter for Childhood Obesity - Elpídeode Almeida Health Institute -ISEA. R: Vila Nova da Rainha, 147. Centro. CEP: 58.400-220. Campina Grande/PB, Brasil. Tel. (83) 3310-6356
ABSTRACT
INTRODUCTION: Currently, an exacerbated trend for excessive daytime sleepiness in overweight children and adolescents has been observed. Obesity and sleep disorders have a combined effect on cardiovascular diseases and diabetes mellitus. The aim of the study was to evaluate the prevalence of excessive daytime sleepiness and its association with cardiometabolic risk factors.
METHOD: Cross-sectional study carried out in a public service, which is reference service for overweight children and adolescents in the period from June 2011 to March 2013 in Campina Grande / PB. The sample consisted of 140 children and adolescents aged from five to 18 years. Anthropometry and blood pressure measures were performed and a questionnaire on sleep habits and Epworth Sleepiness Scale were applied. Laboratory tests were also conducted (lipid profile, blood glucose levels, insulin, HOMA-IR, glycated hemoglobin, ultrasensitive C-reactive protein and leptin). Data were analyzed using SPSS software (v.17), through the chi-square test, ANOVA and Pearson's correlation, with significance level of 5%.
RESULTS: the prevalence of excessive daytime sleepiness was 19.3% and it was higher among girls. In those with excessive daytime sleepiness was observed the highest percentage change in LDL levels, HbA1c and CRP-u, but without statistical significance.
CONCLUSIONS: the presence of sleepiness were prevalent in this sample, and those with this condition showed less favorable metabolic results.
Key words: sleep, child, adolescent, obesity, sleep disorders due to excessive sleepiness.
INTRODUCTION
Currently, childhood obesity reaches epidemic proportions worldwide and is cited as the most important metabolic disorder in developed and developing countries, and its prevalence has increased in recent decades1. Cardiometabolic risk is defined as a set of modifiable risk factors and associated with Cardiovascular Diseases (CVD) and type 2 Diabetes Mellitus (T2DM)2, and overweight in childhood and adolescence is one of these factors 3, besides having a strong correlation with Sleep Disorders (SD).
When associated with excessive daytime sleepiness (EDS) and exercise intolerance, SD results in higher adiposity4. EDS, increased propensity to sleep at inappropriate times or involuntary naps5 can happen due to the short duration of sleep, being quite common in school environments by causing attention deficit, decreased yield and social interaction impairment6. The gold standard for SD diagnosis is polysomnography; however, since it is costly and time consuming, questionnaires and scales have been used.
The Epworth Sleepiness Scale (ESS) is an instrument for evaluating subjective and indirect EDS. It is fast, costless and simple to apply7. In overweight individuals, EDS is very common and despite being a symptom rarely mentioned by children and adolescents8, its prevalence ranges from 7.8% in children9 to 55.8% in adolescents10, variation attributed to different methods used11.
The increased propensity to EDS in childhood and adolescence is due to biological, environmental and behavioral factors12. However, the biological mechanisms underlying the different susceptibilities to early EDS remain unclear and have been associated with increased levels of cytokines and pro-inflammatory mediators, such as C-Reactive Protein (CRP) and leptin, changes that point to an inflammatory state and of Insulin Resistance (IR)13 with significant improvement after SD treatment14.
The knowledge of predisposing factors for obesity is of paramount importance for the elaboration of public policies, especially when it comes to sleep habits, a modifiable risk factor. In the last decade, a large number of studies on EDS with representative samples of children and adolescents have been published, although a lack of data still can be verified. Identifying the cardiometabolic risk factors in childhood is critical due to the importance of initiating prevention strategies and early treatment. Therefore, the objective of this study is to evaluate the prevalence of Excessive Daytime Sleepiness and its association with cardiometabolic risk factors in overweight children and adolescents.
METHODS
Cross-sectional study carried out from June 2011 to March 2012 at the Center for Childhood Obesity (COI), located at the Elpídeo de Almeida Health Institute - ISEA, Campina Grande / PB. The COI is a public reference service for multidisciplinary treatment of overweight children and adolescentse, with 390 currently enrolled children and adolescents.
The sample consisted of all overweight children and adolescents aged from five to 18 years, who attended the routine medical appointment on Fridays during the study period. Patients with adenotonsillar hypertrophy, cardiopulmonary or neuromuscular disease, neoplastic and / or liver disease and under use of medication / drugs (benzodiazepines or antidepressants, bronchodilators, corticosteroids, in addiction or alcoholism) that would interfere with sleep duration and / or EDS were excluded.
During this period, 190 individuals were evaluated. Of these, 17 were excluded: 11 did not meet the age criterion, two for being eutrophic, two for asthma diagnosis, two for adenoid hypertrophy. A loss of 33 individuals for non attendance at blood collection was recorded, and the final sample was composed of 140 individuals.
Anthropometric parameters: weight, height and waist circumference (WC) were collected in duplicate, considering the average of the measures. For weight, a digital Welmy ® scale with capacity of 150 kg and accuracy of 0.1 kg was used and for height, a Tonelli ® stadiometer with accuracy of 0.1 cm was used. At the moment of collection, subjects were wearing light clothing and barefoot, following recommendations of the World Health Organization (WHO)15.
WC was measured with Cardiomed ® inelastic tape with accuracy of 0.1 cm at the midpoint between the upper border of the iliac crest and the last costal margin, with arms positioned along the body and at the expiratory phase of respiration. Values above percentile (P) 90 16 (IDF, 2006) were considered as increased, with maximum value the cutoff point adopted for adults of 88 cm and for girls and 102 cm for boys 17. The nutritional status classification was performed by Body Mass Index (BMI), calculated by dividing the weight in kilograms (kg) by the square of height in meters (m). Overweight or obese individuals were classified as with excess weight, according to the CDC criteria18.
Laboratory tests were performed after a 10-hour fasting period. Total cholesterol (TC), High Density Lipoprotein (HDL), triglycerides (TG) and fasting glucose were assessed by enzymatic colorimetric method in automatic equipment (Model BioSystems 310), and Low Density Lipoprotein (LDL) calculated by the Friedewald formula, except when TG > 400 mg / L.
Insulin was measured by the INSULIN-CT radioimmunoassay method from CIS Bio International®, using Abbott ® gamma counter (intraassay variation coefficient 2.6%). Glycated hemoglobin (HbA1c) was measured by high-performance liquid chromatography method - HPLC ("Gold Standard" Method) and high-sensitivity CRP (CRP - u) by chemoluminescence using automated equipment IMMULITE 1000 (Siemens ®), being excluded from the analysis when CRP-ultrasensitive (CRP-u) > 10 mg / L, since in these cases, it is recommended to repeat the exam19. To assess IR, the Homeostasis Model Assessment was used (HOMA-IR).
The following cardiometabolic risk factors were considered: WC above or equal to P90 for sex, age and race, with a maximum of 88 cm for girls and 102 cm for boys16,17; TG > 130 mg / dl, HDL < 45 mg / dl , fasting glucose > 100mg/dl; Systolic blood pressure (SBP) and / or diastolic blood pressure (DBP) equal to or above the P95 for sex, height and age2; HbA1c > 5.7%20; HOMA-IR > 2.5 and CRP-u > 3 mg/l21. To evaluate EDS, ESS score > 10 confirmed the presence of EDS22.
The population was described through socio-demographic, anthropometric and clinical characteristics (sex, age, maternal education, nutritional status, WC, SBP, DBP), through absolute and relative frequency, mean and standard deviation. Statistical analysis, categorizations by age (children and adolescents), nutritional status (overweight / obesity and severe obesity) and the presence or absence of EDS were performed.
To evaluate the association of EDS with cardiometabolic risk factors, the chi-square and variance tests were used. The relationship between cardiometabolic risk factors and the presence or absence of EDS was measured by the Pearson correlation. Data were analyzed using SPSS version 17, adopting a significance level of 5%. The study was approved by the Ethics Research Committee of the State University of Paraíba (CAEE No.: 0255.0.133.000-11).
RESULTS
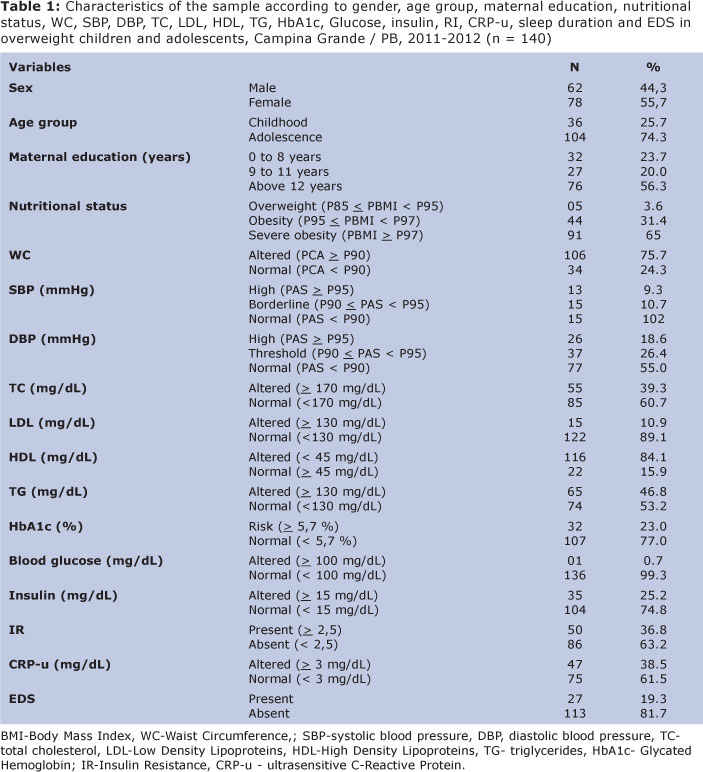
More than half of the sample was female and had severe obesity. Most were adolescents, with mean age of 12.6 years (± 3.4, 5.0 to 18.5). The increased WC was the most frequent cardiometabolic factor and altered glycemia was the less present factor. As for sleep, the EDS prevalence was 19.3% (Table 1).
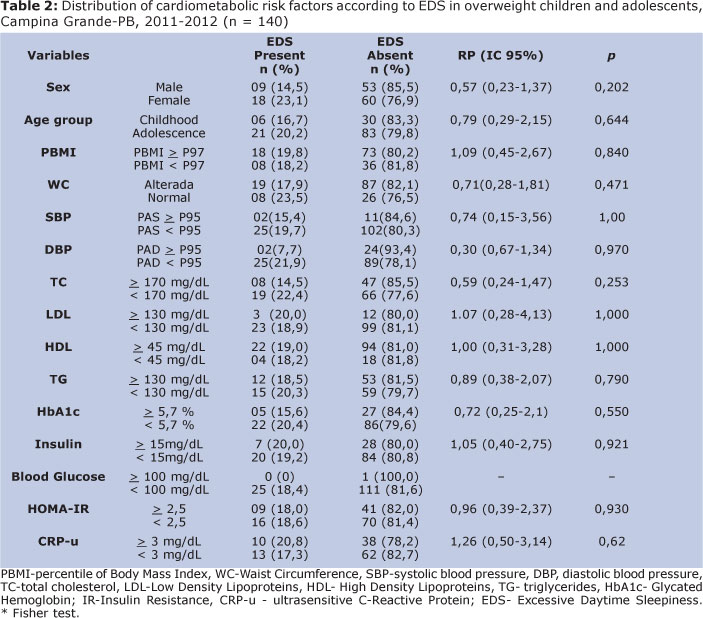
The EDS prevalence was higher in adolescents and girls, but no association with these variables was found. Individuals with EDS showed the highest changes in LDL, HbA1c and CRP-u levels; however, none of these associations were statistically significant. Therefore, there was no association between EDS and cardiometabolic risk factors (Table 2).
There was no significant difference between the mean values of cardiometabolic risk factors according to the presence or not of EDS (Table 3).
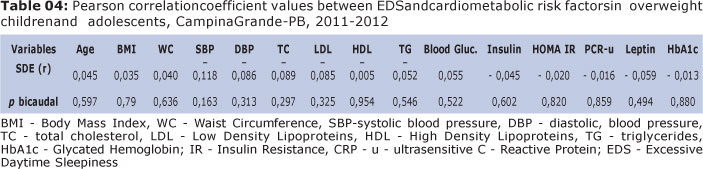
No correlation was observed between EDS and cardiometabolic risk factors (Table 4).
DISCUSSION
Excess weight in childhood is cited as a strong predictor of EDS and sleepiness can be one of the signs of this alteration23. In this study, sleepiness was present in almost ¼ of the population studied.
The prevalence found was lower than that reported by Souza et al.10 (55.8%) in pre-college preparatory course adolescents much higher than that verified by Petry et al9 (7.8%) in children and adolescents from public schools, both in Brazilian samples. These studies used the ESS for EDS diagnosis. The wide variation in prevalence rates may be justified by the subjectivity of this instrument, lack of standard evaluation techniques, different situations to which individuals were submitted as well as different nutritional status of the population evaluated13,23.
The high prevalence found in this study among adolescents may be due to the fact that EDS is relatively rarely diagnosed in children, since it depends on the perception of their caregivers, who rarely describe such symptoms spontaneously, and its prevalence ranges from 7 % to 49 %24. In adoles-cents, the EDS prevalence found by Pereira, Teixeira and Louzada25, after a systematic review of 23 cross-sectional studies ranged from 7.8% 9 to 55.8%10, both in Brazilian samples, and the ESS was the most used scale.
The cause of EDS in adolescents is multifactorial, but there may be a delay in the bedtime in the biological configuration, with a tendency to sleep late and wake up late, which cannot be accomplished within the academic calendar, resulting in a sleep debt accumulation26.
The average sleep duration was 8.54 hours (± 1.74; 5.0 to 11.5). Currently, studies have not allowed identifying a cutoff point for an ideal number of hours of sleep as a protective measure of EDS, and less than nine hours of sleep was a factor associated with high EDS levels27. Perez-Chada et al.28 assessed Argentinean adolescents aged 10 to 15 years and concluded that adolescents need more than eight hours of sleep per night, but due to life style adopted, they have shorter sleep than needed and are at high risk for Sleep Disordered Breathing (SDB) and EDS.
Girls had higher mean in ESS scores, having already shown this association with EDS in other studies25,29. In the absence of SD, obesity may be associated and contribute to the EDS screening, although it is unclear whether this alters the frequency of daytime symptoms23.
In the present study, overweight adolescents had no association of cardiometabolic risk factors with EDS; however, when sleepiness was present, higher mean blood glucose and HbA1c were identified. Redline et al.30 found that obese adolescents with SD were seven times more likely to have metabolic alterations and this varied with sleep efficiency and SD frequency. Da Cunha, Zanetti and Hass31 found that those with poor sleep quality had T2DM and HbA1c greater than 7%.
According to Nakra et al.32, DS treatment in children and adolescents have an impact on metabolic disorders, with an improvement in mean CRP, fasting glucose, insulin and insulin sensitivity, as well as a significant decrease in nighttime leptin.
In the presence of EDS, higher SBP and HOMA-IR were observed. Redline et al.30 in a sample aged eight to 16 years identified association between SD and SBP and DBP levels, and hypertension, arrhythmias and CVD were reported as the main consequences of SDB33. According to O'brien and Gozal34, increased blood pressure, and insulin resistance are due to sympathetic activation, activated by insulin and leptin.
In this sample, no correlation between EDS and of leptin and CRP levels, inflammatory mediators, was found, unlike other studies that found: increased leptin levels due to a resistance to this hormone35,36 in pre-pubescent obese children and adolescents and correlation of leptin levels with the SD levels37.
Obesity is currently described as a low level of systemic inflammatory disorder38 and the same concept applies to SDB and SDE that have been associated with increased levels of mediators inflamatórios39,40. Therefore, it is plausible that the coexistence of overweight and EDS amplify the inflammatory response associated with each of these conditions, resulting in the release of these mediators.
Unlike this study, Tauman et al.41 assessed children aged from 3 to 18 years and found a positive association of CRP with EDS and the SDB level, allowing the use of this biomarker in SD. The mechanism involved in the increased CRP is via episodic hypoxia and excitation after nocturnal awakenings may trigger endothelial dysfunction and systemic inflammation by mechanisms not yet defined 42.
A recent study 13 reported in children and adolescents, overweight is associated with EDS, regardless of the presence of SD, which is mediated by increased circulating levels of cytokines, resulting from obesity 38.
SD, besides compromising the sleep quality, has variable impact on the vigil quality. EDS is the main complaint of individuals with SD and the lack of prevalence data, incidences and associated factors were identified, especially in Brazilian populations. Epidemiological studies with instruments with greater reproducibility for measuring the problem are necessary to allow comparison between different results, which is a methodological limitation.
This study is a pioneer in Brazil, since it increases the SD approach and cardiometabolic risk factors resulting from excess weight; however, it does not allow identifying a causal relationship, due to its cross-sectional design. A longitudinal study dividing the population into obese and eutrophic individuals would allow the assessment of the effect of overweight on EDS.
The knowledge on sleep behavior and its influence on the development of cardiometabolic complications in the population of overweight children and adolescents can serve as a basis for the development of programs for behavior change, one of the focuses of public health policies. Public health has a broad focus and works to ensure the health and welfare of groups by improving the health and quality of life through the prevention and treatment of disease and by promoting healthy behaviors 43.
EDS had high prevalence and its presence should be monitored in overweight children and adolescents because groups with EDS showed less favorable results. Assessing EDS in overweight children and adolescents may be useful for the early SD diagnosis and predisposition for CVD and T2DM, justifying the need for screening this population for SD.
REFERENCES
1. World Health Organization. World Health Statistics. May 2013. Disponível em: http://www.who.int/gho/publications/world_health_statistics/2013/en/ Acesso em: 25/06/2013. [ Links ]
2. Sociedade Brasileira de Cardiologia (SBC). VI Diretrizes Brasileiras de Hipertensão Arterial. Arq Bras Cardiol. 2010 :13(1). [ Links ]
3. Hong, Y M. Atherosclerotic Cardiovascular Disease Beginning in Childhood. Korean Circ J. 2010;40:1-9. [ Links ]
4. Verhulst S L, Schrauwen N, Haentjens D, et al. Sleep-disordered breathing and the metabolic syndrome in overweight and obese children and adolescents. J Pediatr. 2007;150:608-12. [ Links ]
5. Bittencourt L R A, Silva R S, Santos R F, Pires M L N, Mello M T. Excessive daytime sleepiness. Rev Bras Psiq. 2005;27(1):16-21. [ Links ]
6. Teixeira L R, Lowden A, Lemos T S, et al. Sleep and sleepiness among working and non-working high school evening students. Chronobiol Int. 2007;24:99-113. [ Links ]
7. Boari L, Cavalcanti C M, Bannwart S R F D, Sofia O B, Dol J E L. Avaliação da escala de Epworth em pacientes com a Síndrome da apnéia e hipopnéia obstrutiva do sono. Rev Bras Otorrinolaringol. 2004;70(6):752-6. [ Links ]
8. Wolfson A R, Spaulding N L, Dandrow C, Baroni E M. Middle school start times: the importance of a good night's sleep for young adolescents. Behav Sleep Med. 2007;5:194-209. [ Links ]
9. Petry C, Pereira M U, Pitrez P M, Jones M H, Stein R T. The prevalence of symptoms of sleep-disordered breathing in Brazilian schoolchildren. J Pediatr (Rio J). 2008;84:123-9. [ Links ]
10. Souza J C, Souza N, Arashiro E S H, Schaedler R. Excessive daytime sleepiness in senior high school students. J Bras Psiquiatr. 2007; 56: 184-7. [ Links ]
11. Melendres M C, Lutz J M, Rubin E D, Marcus C L. Daytime sleepiness and hyperactivity in children with suspected sleep disordered breathing. Pediatrics. 2004;114:768-775. [ Links ]
12. Moore M, Meltzer L J. The sleepy adolescent: causes and consequences of sleepiness in teens. Paediatr Respir Rev. 2008;9:114-20. [ Links ]
13. Tsaoussoglou M, Bixler E O, Calhoun S, et al. Sleep-Disordered Breathing in Obese Children Is Associated with Prevalent Excessive Daytime Sleepiness, Inflammation, and Metabolic Abnormalities. J Clin Endocrinol Metab. 2010;95(1):143 - 150. [ Links ]
14. Barcelo A, de la Pena M, Barbe F, et al. Prostaglandin D synthase (trace) levels in sleep apnea patients with and without sleepiness. Sleep Med. 2007;8(5):509-511. [ Links ]
15. World Health Organization (WHO). Physical Status: the use and interpretation of anthropometry. Report of a WHO Expert Committee. Technical Report Series nº 854. Geneva; 1995. [ Links ]
16. IDF Clinical Guidelines Task Force. Global Guideline for Type 2 Diabetes: recommendations for standard, comprehensive, and minimal care. Diabet Med 2006;23(6):579-593. [ Links ]
17. Third Report of The National Cholesterol Education Program (NCEP). Expert panel on detection, evaluation, and treatment of high blood cholesterol in adults (Adult Treatment Panel III) final report. Circulation. 2002;106(25):3143-421. [ Links ]
18. CDC Table for calculated body mass index values for selected highs and weights for ages 2 to 20 years. [Acesso em 2011 jun 10]. Disponível em: htpp://www.cdc.gov/growthcharts. 2002 [ Links ]
19. Lande MB, Pearson TA, Vermilion RP et al. Elevated Blood Pressure, Race/Ethnicity, and C-Reactive Protein Levels in Children and Adolescents. Pediatrics 2008; 122(6):1252-1257. [ Links ]
20. American Diabetes Association (ADA). Standards of medical care in diabetes-2011. Diabetes Care 2011;34(1):S11-S61. [ Links ]
21. Giuliano I C B, Caramelli B, Pellanda L, Duncan B, Mattos S, Fonseca F A H. Sociedade Brasileira de Cardiologia. I Diretriz de prevenção da aterosclerose do Departamento de Aterosclerose da Sociedade Brasileira de Cardiologia. Arq Bras Cardiol. 2001;77(3): 1-48. [ Links ]
22. Tsara V, Serasli E, Amfilochiou A, Constantinidis T. Greek version of the Epworth Sleepiness Scale. Sleep and Breathing. 2004;8(2):91-95. [ Links ]
23. Gozal D, Kheirandish-Gozal L. Obesity and excessive daytime sleepiness in prepubertal children with obstructive sleep apnea. Pediatrics. 2009;123:13-18. [ Links ]
24. Chervin R D, Weatherly R A, Ruzicka DL, Burns JW, Giordani BJ, Dillon JE, et al. Subjective sleepiness and polysomnographic correlates in children scheduled for adenotonsillectomy vs. other surgical care. Sleep. 2006;29:495-503. [ Links ]
25. Pereira, E F, Teixeira, C S, Louzada, F M. Sonolência diurna excessiva em adolescentes: prevalência e fatores associados. Rev. paul. pediatr. 2010;28 (1):98-103. [ Links ]
26. Fuentes-Pradera M A, Sa´Nchez-Armengol A, Capote-Gil F, et al. Effects of sex on sleep-disordered breathing in adolescents. Eur Respir J. 2004;23:250-254. [ Links ]
27. Loessl B, Valerius G, Kopasz M, Hornyak M, Riemann D, et al. Are adolescents chronically sleep-deprived? An investigation of sleep habits of adolescents in the Southwest of Germany. Child Care Health Dev. 2008;34:549-56. [ Links ]
28. Perez-Chada D, Perez-Lloret S, Videla A J, et al. Sleep Disordered Breathing And Daytime Sleepiness Are Associated With Poor Academic Performance In Teenagers. A Study Using The Pediatric Daytime Sleepiness Scale (PDSS). Sleep. 2007;30(12):1698-1703. [ Links ]
29. Chung K F, Cheung M M. Sleep-wake patterns and sleep disturbance among Hong Kong Chinese adolescents. Sleep. 2008;31:185-94. [ Links ]
30. Redline S, Storfer-Isser A, Rosen C L, Johnson N L, Kirchner H L, Emancipator J, et al. Association between Metabolic Syndrome and Sleep-disordered Breathing in Adolescents. Am J Respir Crit Care Med. 2007;176:401-408. [ Links ]
31. Da Cunha M C B, Zanetti M L, Hass V J. Qualidade do sono em diabéticos do tipo 2. Rev Latino-am Enfermagem. 2008;16(5). [ Links ]
32. Nakra N, Bhargava S, Dzuira J, Caprio S, Bazzy-Asaad A. Sleep-Disordered Breathing in Children With Metabolic Syndrome: The Role of Leptin and Sympathetic Nervous System Activity and the Effect of Continuous Positive Airway Pressure. Pediatrics. 2008;122(3). [ Links ]
33. Cintra F D. Alterações cardiovasculares na síndrome da apnéia obstrutiva do sono. Arq. Bras. Cardiol. 2006;86(6). [ Links ]
34. O'Brien L M, Gozal D. Autonomic dysfunction in children with sleep-disordered breathing. Sleep. 2005;28:747-52. [ Links ]
35. Souza M S F, Cardoso A L, Yasbek J R P, Fainthch J. Aerobic endurance, energy expenditure, and serum leptin response in obese, sedentary, prepubertal children and adolescents participating in a short-term treadmill protocol. Nutrition. 2004;20:900-4. [ Links ]
36. Steinberg G R, Smith A C, Wormald S, Malenfant P, Collier C, Dyck D J. Endurance training partially reverses dietary-induced leptin resistance in rodent skeletal muscle. Am J Physiol Endocrinol Metab. 2004;286:E57-63. [ Links ]
37. Tauman R, Serpero L D, Capdevila O S et al. Adipokines in children with sleep disordered breathing. Sleep. 2007;30(4):443-449. [ Links ]
38. Vgontzas A N, Zoumakis E, Bixler E O, Linhm, Collins B, Basta M, et al. Selective effects of CPAP on sleep apnoea-associated manifestations. Eur J Clin Invest. 2008;38:585-595. [ Links ]
39. Kheirandish-Gozal L, Capdevila O S, Tauman R, Gozal D. Plasma C-reactive protein in nonobese children with obstructive sleep apnea before and after adenotonsillectomy. J Clin Sleep Med. 2006;2(3):301-304. [ Links ]
40. Gozal D, Serpero LD, Sans Capdevila O, Kheirandish-Gozal L. Systemic inflammation in non-obese children with obstructive sleep apnea. Sleep Med. 2008;9(3):254-259. [ Links ]
41. Tauman R, Ivanenko A, O'brien L M, Gozal D. Plasma C reactive protein levels among children with sleep-disordered breathing. Pediatrics. 2004;113:564-9. [ Links ]
42. Apostolidou MT, Alexopoulos EI, Chaidas K, Ntamagka G, Karathanasi A, Apostolidis TI, et al. Obesity and persisting sleep apnoea after adenotonsillectomy in Greek children. Chest 2008; 134 : 1149-55. [ Links ]
43. Atrash HK, Carpentier R. The evolving role of public health in the delivery of health care. J. Hum. Growth Dev.2013; 22(3):369-399. [ Links ]
 Correspondence to:
Correspondence to:
jajas-cardoso@hotmail.com
Manuscript submitted Oct 08 2012
Accepted for publication Dec 9 2012.

{kind=link}
{kind=link}
{kind=link}
{kind=link}