










Services on Demand

article
 English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
Indicators
Share

 Permalink
PermalinkPsicologia para América Latina
On-line version ISSN 1870-350X
Psicol. Am. Lat. no.32 México Nov. 2019
Behavioral intervention in women with Fibromyalgia: clinical significance and reliable change
Intervenção comportamental em mulheres com fibromialgia: Significância clínica e indice de mudança confiável
Intervención conductual en mujeres con fibromialgia: Significancia clinica y indice de cambio confiable
Luziane de Fátima KirchnerI; Maria de Jesus Dutra dos ReisII; Francine Náthalie Ferraresi Rodrigues QueluzIII
IDom Bosco Catholic University, Campo Grande - MS, Brazil
IIFederal University of São Carlos, São Carlos - SP, Brazil
IIISão Francisco University, Campinas – SP, Brazil
ABSTRACT
The aim of this study was to evaluate the effect of 20 sessions of intervention in analytic-behavioral on stress, anxiety, depression, social skills and disability of pain in women with fibromyalgia (n=4). The effects were measures by clinical significance and Reliable Change Index (JT Method, Jacobson & Truax). All participants answered self-report instruments to assess the variables and had the cortisol measured when awakening. After the intervention, we conclude that the sessions were effective, with positive changes in the scores of all instruments. However, no change in the cortisol response on awakening were found. Implications for future studies are discussed, for example, the importance in conducting evaluations using direct measures, beyond the self-report, to identification of clinical significance.
Keywords: clinical significance, chronic pain, behavioral intervention; fibromyalgia
RESUMO
O objetivo deste estudo foi avaliar o efeito de 20 sessões de intervenção analítico-comportamental sobre o estresse, a ansiedade, a depressão, as habilidades sociais e a incapacidade frente a dor em mulheres com fibromialgia (n=4). Os efeitos foram mensurados pela Significância Clínica e Índice de Mudança Confiável (Método JT, Jacobson & Truax). Todas as participantes responderam aos instrumentos de autorrelato para medir as variáveis, e o cortisol foi coletado ao despertar. Verificou-se que as sessões foram efetivas, com mudanças positivas nas pontuações de todos os instrumentos. No entanto, não foram encontradas mudanças na resposta do cortisol. Se discutem as implicações para os estudos futuros, assim como a importância de conduzir avaliações com o uso de medidas diretas, além do autorrelato, para a identificação da Significância Clínica.
Palavras-chave: significância clínica, dor crônica, intervenção comportamental, fibromialgia
RESUMEN
El propósito de este estudio fue evaluar el efecto de 20 sesiones de intervención analítica conductual sobre el estrés, la ansiedad, la depresión, las habilidades sociales y la discapacidad del dolor en mujeres con fibromialgia (n=4). Los efectos se midieron por la Significancia Clínica y el Indice de Cambio Confiable (Método JT, Jacobson & Truax). Todos los participantes responderán a los instrumentos de autoinforme para medir las variables y el cortisol que han evaluado al despertar. Después de la intervención, se verificó que las sesiones fueron efectivas, con cambios positivos en las puntuaciones de todos los instrumentos. Sin embargo, no se encontró ningún cambio en la respuesta del cortisol. Se discuten las implicaciones para los estudios futuros, así como la importancia de conducir evaluaciones con uso de medidas directas, además de lo autoinforme, para identificación de la Significancia Clínica.
Palabras clave: significancia clínica, dolor crónico, intervención conductual, fibromialgia
Introduction
The chronic pain is a complex phenomenon that involves the interaction between biological, neurochemical, emotional, cognitive, psychosocial and sociocultural elements. Among some pathologies characterized by the presence of chronic pain we known fibromyalgia, focus of this study. According to Skinner, although the socio-verbal community does not have access to variables that control pain behavior, these variables determines the topography of responses (e.g: complains, medication request and rest), that describe the sensations and organic states. In this way, reactions to painful processes are responses to private stimuli, but also the product of social contingencies (Skinner, 2003, 1979).
Fibromyalgia (FM) is a syndrome characterized by generalizedpaininthebody, whoseetiologyisnotknown (Heymann et al., 2010). There is an intense impairment in the individual's quality of life and functionality, and the main symptoms are related to anxiety, depression, difficult to sleep and stress (Reis & Rabelo, 2010; Riva, Mork, Westgaard, Rø & Lundberg, 2010; Wolfe et al., 2010). In addition, it was also found lower levels and lower variation of the cortisol awakening response (CAR) in women with FM compared to women without FM (healthy). This may indicate that women with FM have less resistance to respond appropriate to environmental stressors. Some authors postulate, however, that these psychoaffective and neuroendocrine damages (related to stress response) are, in part, resulted from a series of childhood traumatic experiences, coercive relationships and work overburden, which is regularly observed in this population (Crofford et al., 2004; Reis & Rabelo, 2010; Van Houdenhove, 2003). Such impairments interact with broad classes of mal-adaptive responses (example: complaining, asking for medication, etc.), which tend to remain by escape and avoidance leaving the person free from others stimuli that are more aversive (example: avoiding social interactions of risk, hostile work environment, etc.). This may happen with people that do not present a behavioral repertoire adequate to deal with everyday problems (Rachlin, 2010; Vandenberghe, 2005).
When adaptive behaviors are installed and under positive reinforcement control, maladaptive behaviors of pain and its correlates are reduced in frequency and may lead to the perception of improvement of symptoms (Kazdin, 1999). Behavioral treatments, in this perspective, consist of identify pain-contingent reinforcement, promoting differential reinforcement of alternative responses and teaching new responses, acquired throughout the therapeutic process (Main, Keefe, Jensen, Vlaeyen & Vowles, 2014; Vandenberghe, 2005). Considering interpersonal demand as a potential sustainer of chronic pain behaviors (Main et al., 2014), although new responses to specific health care need to be strengthened (e.g: better performance of work and health care), it is also important that the treatment allows the expansion of behaviors that contribute to better interpersonal relationship (Kirchner, Reis & Queluz, 2019; Penido & Rangé, 2007; Reis & Rabelo, 2010; Spicio et al., 2005).
Some studies in the literature have described the joint effect of both behavioral components (management of physical conditions with health care, and interpersonal relationships), as well as other intervention strategies (Nicassio et al., 1997; Thieme, Flor & Turk, 2006). These studies reported effects on intensity and disability related to pain and in depression, when performing group delineations, using inferential statistics. When studying small groups, statistical analyzes are not recommended. But despite this, other methods can be used to predict if the changes obtained with the treatment were significant in order to suggest that there was a positive impact on the individual's life. This method seems to have a more important clinical value than the inferential statistics (Kazdin, 2010). One of the methods available for this propose, was presented by Jacobson and Truax (1991). The method allows the research to determine if the changes occurred after the intervention, obtained by instrument scores, were clinically significant (CS) or if they constitute artifacts or measurement errors (analysis of the Reliable Change Index). Therefore, the present study aimed to evaluate the effect of the application of two intervention components presented sequentially (1-management of conditions of the physical environment, 2-management of the interpersonal relationships), on the variables stress, disability resulting from pain, anxiety, depression and social skills. The components aimed to manage conditions of the physical environment (component 1), and of the interpersonal relationships (component 2), based on intervention proposals discussed in the area (Main et al., 2014; Nicassio et al., 1997; Spicio et al., 2005; Thieme, Flor & Turk, 2006). This order of presentation of the components were chosen to answer the question of the study, suggesting that the component related to interpersonal demands would allow better results at the end of the study. In addition, the clinical significance and the reliability of the changes obtained (Reliable Change Index) were evaluated in order to identify the magnitude of the treatment effects.
Method
Participants
Four women aged 47-59 years (mean = 52.3; sd = ± 6.65), who presented a diagnosis of FM (Wolfe et al., 2010) and reported not participating in psychotherapy during the data collection period. Most of the participants (n = 3) stated that they had completed primary school, lived with their current partner, and were working. They had the FM diagnosis ranged from 8 to 25 years ago (mean= 14; sd = ± 7.61). All participants reported, in a initial interview, making regular use of anti-inflammatory or analgesic, and only one (S4) reported participating in activities for the benefit of health. Participants also presented different complaints, which they attributed to being related to the presence and intensity of the pain, such as: child labor or traumatic experiences in childhood (n = 4), stress in family conflicts (n = 3), and exhausting work activity (n= 3).
Materials and instruments
Initial interview: we prepared a script of initial interview to ascertain the participants' sociodemographic characteristics (age, marital status, educational level, diagnosis of FM, medications and others treatments) to describe the sample.
Fibromyalgia Impact Questionnaire, revised Brazilian version - FIQ-R (Paiva et al., 2013): It is consisted by 21 items on a Likert scale (0-10), with 10 being "the worst", and the patients were instructed to frame the questions in the context of the last 7 days. It was organized in three domains related to: 1) functionality (e.g.: How much your Fibromyalgia made it difficult walk continuously for 20 minutes; prepare a homemade meal); 2) global impact of FM (e.g.: Fibromyalgia prevented me from meet goals for the week on what); 3) intensity of symptoms (e.g.: in a numeric scales from 1 to 10, please rate the level of pain; please rate your level of stiffness). The sum of each domain is divided by 3, 2 and 1, respectively, and the sum of the sub scores is the final score. Internal consistency of the instrument α = .96.
Beck Anxiety Inventory - BAI (Cunha, 2001): It is consisted by a likert format scale of four points with a list of 21 physical and psychological symptoms that the participant may have experienced in the last week (e.g.: numbness or tingling; wobbliness in legs). The results indicate four levels of anxiety (Minimal < 9, Light 10-16, Moderate 17-19 and Severe > 30). Internal consistency of the instrument α = .92.
Beck Depression Inventory - BDI (Cunha, 2001): It is consisted by a likert format scale of four points with a list of 21 symptoms or attitudes that describe behavioral, affective, cognitive or somatic manifestations that may have occurred in the last week. It includes mood, pessimism, sense of failure, self-dissatisfaction, guilt, punishment, suicidal ideas, irritability, social with- drawal, fatigability, loss of appetite and others. The results may indicate four levels of depression (Minimal < 11, Light 12-19, Moderate 20-35 and Severe 36-63). Internal consistency of the instrument α = .82.
Social Skills Inventory - IHS (Del Prette & Del Prette, 2001): It is consisted by 38 items, in which the participants assess their reaction to interpersonal relationships, selecting the frequency of these reactions on a Likert 5-point scale (0 = never or rarely to 4 = always or almost always). The inventory evaluates five factors: 1) confrontation and self-assertion with risk (e.g: disagreeing with authority, disagreeing with the group, etc.); 2) self-affirmation in the expression of positive feeling (e.g: praising family members and others); 3) conversation and social entrepreneurship (e.g: end conversations, refusing abusive requests, etc.); 4) self-exposure to strangers and new situations (e.g: speaking in public, asking favors or talking to strangers); 5) self-control of aggressiveness (e.g: dealing with unfair criticism). The instrument classifies the repertoire of social skills in the scores: quite elaborate; good and above the medium; medium; good and below the medium; and with deficit. Internal consistency of the instrument α = .75.
Lipp Adult Stress Symptom Inventory – ISSL (Lipp, 2000): It is consisted by 37 somatic and 19 psychological items, usually present in stress. The occurrence of the symptoms indicate in the items should have happened in the last 24 hours, in the last week and in the last month. At the end, four different phases of stress could be identifi d: Alert, Resistance, Near Exhaustion and Exhaustion. Internal consistency of the instrument α = .91.
Polypropylene tubes (Eppendorf®, Hamburg, Germany) were used for the collection of saliva on awakening (Cortisol Awakening Response - CAR), which determined the free fraction of cortisol on the functioning of the hypothalamic-pituitary-adrenal (HPA) axis.
Data collection procedure
Data collection was performed in an individual service room of a psychology learning center of a public university in the interior of São Paulo, Brazil, and at the participant's home. This study was approved by the Ethics and Research Committee at Central Paulista University Center (Protocol Number 1.170.930).
Participants were recruited through an interview that identified the inclusion criteria established (diagnosis of FM and not participating in psychotherapy during the data collection period). Eleven women were initially selected, but four of them did not present the inclusion criteria for participating in the study, and other three gave up participating before the first intervention. So, data collection from this study was completed with four participants, who participated in all stages of the study. A digital recorder (Mp4) was used to record the sessions and subsequent judge's analysis.
The participants were sequentially conducted in the following stages: a) Initial Evaluation; b) Intervention Component 1 - Management of conditions of the physical environment; c) Intermediate Evaluation; d) Intervention Component 2 - Management of interpersonal relationships; e) Final Evaluation. Below is a detailed description of the evaluation and intervention procedures.
Evaluations: Self-report instruments (FIQ-R, BAI. BDI, IHS, ISSL) previously described were answered individually by the participants in a psychology learning center in all stages of the intervention (see Table 1). Two polypropylene tubes (Eppendorf®, Hamburg, Germany) were sequentially delivered to each participant for saliva collection to be performed the following morning (one upon awakening and another 30 minutes after) according to oral and written guidance. Since it was not possible to meet the collection requirements on the stipulated day, the participants were instructed to do it the next day. The samples were delivered to the researcher on the same day they were collected by the participants and stored in a freezer -20ºC until they were sent to a clinical laboratory for electrochemiluminescence assay in the Elecsys 2010 appliance (Roche®, São Paulo, SP, Brazil).
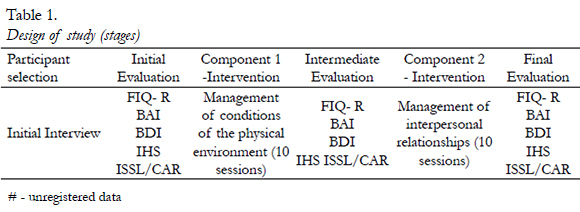
Interventions: We conducted 10 individual sessions with the component 1 and 10 individual sessions with the component 2. Both of them primarily aimed to expand the repertoire of health care and potentially reinforcing interaction skills in the participants' environment. Each session lasted 1 hour and 30 minutes, and was structured as follows: a) verification of changes in treatments (pharmacological / non-pharmacological) and activities performed during the week (30 minutes); b) presentation of the theme proposed for the session (40 minutes); and Progressive and Autogenic Muscle Relaxation training (20 minutes). The themes of Component 1 were: 1) FM, diagnosis and treatments; 2) Cost-benefit when take care their personal health and effects of relaxation training; 3) Identification of activities that increase pain; 4) Functional analysis of environmental variables (physical conditions) related to pain response; 5) Survey of positively reinforcing activities; 6) Functional analysis of variables that help in coping with pain; 7) Discussion about the pain maintenance cycle, 8-10) Identification of progress and gains related to physical environment. The themes of component 2 were: 1) Pain and interpersonal relationships; 2) Empathy; 3) Expression of positive feelings in interpersonal relationships; 4) Discrimination of feelings; 5) Patterns of passive, assertive and aggressive behavior; 6) Assertive communication (written activity); 7) Assertive communication (role-playing); 8-10) Identification of progress and gains related to socially skillful behaviors. Two judges analyzed the recordings of the sessions, identifying the reliability between two observers regarding the themes proposed for each session. The concordance index presented 56.6% of agreement for the sessions of component 1 and 71% for the sessions of component 2.
Data Analysis
The cortisol data were analyzed, obtaining the percentage of the difference between the values of collection 1 and collection 2, both performed on the same day, but the first on awakening and the second 30 minutes after. For the ISSL, the percentile and the stress phase that the participant was at each stage of evaluation was identified. In addition, the Reliable Change Index and clinical significance was measured for self-reported measures of stress, anxiety, depression and social skills, based on the scores of each participant in the initial and final evaluations. These analyzes were based on the JT method. The criterion A was used (when the instrument manual has normative data only for the dysfunctional population) to analyze the FIQ-R scores, the criterion B (when the data are only available for the functional population) was used to analyze the IHS, and the criterion C (when the manual provides normative data for both populations, functional and dysfunctional) was used to analyze the BAI and BDI instruments (Aguiar, Aguiar, & Del Prette, 2009).
Results
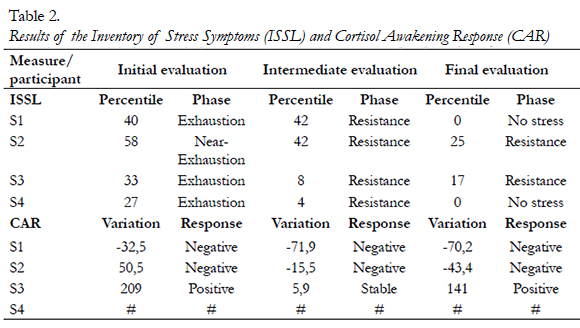
The presents the results for the self-report measure of stress, which indicates the percentile and the stage of the stress in which each participant were (alert, resistance, near exhaustion or exhaustion), and the direct measurement, variation of Cortisol Awakening Response (CAR), which indicates HPA axis resilience on stress response. Based on the fact that in healthy people occurs a cortisol peak about 30 minutes after awakening (Fries, Dettenborn & Kirschbaum, 2009), a "positive response" was considered in this study if the second collection (30 minutes after awakening) was 60% higher in relation to the first collection (on awakening). Percentages of change below 60% were considered 'stable response' and negative values were considered 'negative response'.
The data related to measure of self-report of stress (ISSL) indicated that, for all participants (n = 4), there was a reduction of stress symptoms (with phase change) after the application of intervention component 1 (Intermediate evaluation), and the decreasing in stress, percentile reduction or change in the stress phase for a better one was observed in the final evaluation. Two of the four participants reported, at the end of the study, no symptoms of stress. Regarding the response of the Cortisol Awakening Response-CAR, no positive effects were observed for the participants throughout the evaluation period. Only the participant 3 presented positive response of the cortisol variation when comparing the Initial and the Final evaluation.
In addition to the stress variable, the clinical significance and the Reliable Change Index, based on the JT Method (Jacobson & Truax, 1991) were assessed in the measures of Social Skills (IHS, General Score), Disability related to pain (FIQ-R), Anxiety (BAI) and Depression (BDI), in the Initial and Final evaluation. The data are presented in scatter plots, of which the Initial Evaluation scores are found on the X axis and the Final Evaluation scores on the Y axis. It is noted that the order of the scores on the axes of the first chart on the left is different because the instrument IHS has a positive indicator and the FIQ-R, BAI and BDI instruments have negative indicators. It is also possible to note that the scores presented in the Final Evaluation for FIQ-R, BAI and BDI are lower than the Initial Evaluation scores, and for IHS scores are higher. This indicates that positive changes occurred after the intervention, considering the scores of all these measures.
clinical significance is represented by horizontal lines, and the Reliable Change interval is represented by diagonal lines. Positive change in clinical status is attributed when values are in the upper left quadrant and positive change when values are above the diagonal line. Values observed on the lower left side and below the diagonal line indicate worsening of clinical status and reliable negative change, respectively. Finally, the values between the diagonal lines and between the horizontal lines indicate that it is not possible to affirm the existence of reliable changes related to the intervention (see Figure 1).
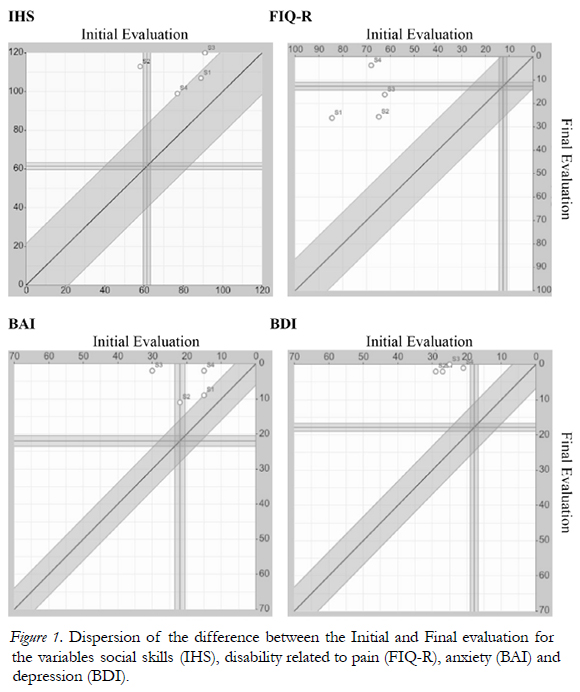
The change in clinical status, which displaced participants from the dysfunctional to functional population, was observed for all participants (S1, S2, S3 and S4) in relation to depression (BDI), for S2 in relation to social skills, for S3 in relation to anxiety (BAI), and for S4 in relation to disability related to pain. There was no change in clinical status for S1, S3 e S4 regarding social skills, and for S1 e S4 regarding anxiety, since those participants were already in the functional population at the beginning.
Reliable positive changes (BMI) were observed in relation to incapacities related to pain (FIQ-R) and in depression (BDI) in all participants (S1, S2, S3 and S4), and in relation to anxiety (BAI) and social skills (IHS) in three participants (S2, S3 and S4). Only for S1, regarding anxiety and social skills, it is not possible to state that the results obtained were because of the intervention, since the score of this participant is within the diagonal range (see Figure 1).
Discussion
The present study aimed to evaluate the effect of the application of component 1 - management of conditions of the physical environment, and the effect when including component 2 - management of the interpersonal relationships, on the variables stress, disability related to pain, anxiety, depression and social skills in women with Fibromyalgia. Although the intervention was not directly focused on the management of stress, changes in these indicators were observed after the application of the first component.
These results indicate that the discrimination and management of the physical environment and pain contingencies, combined with the availability of differential reinforcement of alternative responses by the therapist, may have enabled the reduction of the condition of uncontrollability in front of pain (Huzinker, 2010; Main et al., 2014). It is important to emphasize that since the beginning of the first component, the participants were instructed to perform the Progressive and Autogenous Muscle Relaxation Training at home, which was also conducted at the end of each session. This strategy has also been showed in the literature as effective in reducing pain and stress responses (Meeus et al., 2015).
Despite the changes observed in the reporting of stress symptoms (ISSL) for all participants, the variation of the cortisol response on awakening (direct measure of stress) was not observed. Some authors related that in healthy individuals a cortisol peak occurs about 30 minutes after awakening, and divergent responses suggest some type of deregulation on the HPA axis (Fries, Dettenborn & Kirschbaum, 2009). In the participants of this study, the increase in cortisol in the second collection was not observed, indicating that the HPA axis involvement was maintained. Only participant 3 presented a positive response on cortisol variation in the Initial and Final Evaluation. Changes in the routine, which could justify the results of this participant, were not noticed in the initial evaluation stage, but in the final evaluation the participant was away from work on previous days and on the day of saliva collection. It is suggested, therefore, that a short treatment period (10 and 20 sessions) and with a few hours duration, is still not enough to modify the directly measured physiological responses, but that intense changes in the routine (for example, the participant was absent from unpleasant and stressful labor activities for it) possibly have an impact on this variable.
The other study observed changes in the cortisol response in women with FM after participating in a multidisciplinary intervention (Bonifazi et al., 2006). However, this intervention involved different components (stretching, aerobic exercises, educational sessions, cognitive-behavioral therapy and relaxation training), and occurred in an intensive manner (seven hours a day for three weeks). The participants performed the collections in their residences at different times of the day (from 8am to 10pm), and as the participants of the present study, they could be subject to forget to take care of the procedure, or perform it at different times than previously stipulated, compromising the reliability of the result. These are some of the limitations in conducting saliva collections by at home participants, which could only be adequately managed if the participants were followed up at all collections or in controlled settings, such as in a hospital environment. In some samples of saliva (31%) it was not possible to evaluate the level of cortisol, since they were below the level of detection (below 0.054 mg / l). Some factors, such as the time interval between storage and the period of analysis, transport conditions of collection, use of tubes for collection of saliva other than those indicated in the analysis manual, may have debugged the material to be analyzed (Elecsys Cortisol®).
For the other instruments, FIQ-R, BAI and BDI and IHS, it was possible to note the positive changes in the scores after the intervention. The analyzes based on the JT Method (Jacobson & Truax, 1999) also showed, according to the scores of the Initial and Final Evaluation, that all participants moved from the dysfunctional population to the functional population in relation to the depression variable, and changes in scores of instruments was observed for variable anxiety, pain-related disability and social skills.
Regarding social skills participants had an initial below-medium repertoire, but nonetheless, they were still in the non-clinical range. In addition, positive changes (BMI) in the studied variables was observed for all participants and measures, except for S1 in social skills and anxiety. These results seem to establish a connection between treatment goals, changes in instrument scores and changes obtained by participants according to the reports in session (increasing reports on natural environment exposures and their consequences) indicating that, in fact, the intervention was effective, with the hypothesis that these results reflected improvements in participants' lives (Kazdin, 1999).
The significant change in scores for depression, which moved participants from a clinical to nonclinical condition, corroborate with statistically significant changes (p <0.05) obtained for these variables after a smaller number of sessions (Nicassio et al., 1997; Jensen et al., 2002). Additionally, Slater, Doctor, Pruitt, & Atkinson (1997) reported that 47% of patients with chronic low back pain who received behavioral treatment showed a reliable positive change and 41% left a clinical status to at least one of the variables measured (depression, pain or inability). This result is justified by the fact that the participants leave the condition of learned helplessness and uncontrollability in pain, giving rise to new, positively reinforced responses in the environment (Nicassio et al., 1997; Hunziker, 2010).
In the self-report measures used, we see as a limitation the fact that information may be subject to problems of memory, attention, side effects and iatrogenic medications, or even be under the control of a history of reinforcement that prioritizes socially desirable reports of the participants (Kohlsdorf & Costa Junior, 2009), regarding the efficacy of the treatment. No evaluations involving behavioral observation in structured situations or a natural environment were performed, they could be useful in identifying initial behavioral deficits and in the effectiveness of the intervention, and would reduce these self-report effects (Del Prette & Del Prette, 2009; Keefe, 1982).
It is known that the exclusive care in a therapeutic context, and yet, not involving family members, is insufficient to allow the generalization of responses to natural environment stimuli. This is a challenge in analytic-behavioral therapy (Lindsay & Stoffelmayr, 1982). and even more so in a chain of pain responses, possibly well established in the individuals' environment (Main et al., 2014).
Implications for practice
The application of an intervention should show evidence of validity, and individual analyzes, considering that the clinical differences of this population, tend to be valued (Morley, Linton & Vlaeyen, 2015). This study showed that a analytic-behavioral intervention, with 20 sessions distributed in two components (1 - management of the conditions of the physical environment, 2 - management of the conditions of the interpersonal relationship) was able to promote changes in health indicators of the participants, mainly in what refers to the symptoms of depression and anxiety. The JT method, developed by Jacobson and Truax (1991), is one of the ways to assess the impact of an intervention individually by participants, from the scores on pre and post test evaluations. The levels of clinical significance and reliable change, central concepts of this method, are calculated to ensure that the magnitude of the change exceeds the margin of measurement error. The method is, therefore, robust to support the analysis, but self-reported assessments may still experience biases of social desirability. The cortisol awakening response didn't change after the intervention and the data could not be detected for one of the participants (S4), but this should not discourage future researchers regarding the use of direct measures in this population.
Conclusions
This study showed that the change in the scores between pre and post-test evaluations were significative and it is possible of suggesting that they had an impact on participants' lives. However, the number of sessions was limited and had the participation of few subjects, who had the perception of symptom improvement evaluation as the main object of analysis. The application in a larger number of participants, with the use of direct measures, together with the measures of self-report, should be the target in the conduction of future studies.
References
Aguiar, A. A. R., Aguiar, R. G., & Del Prette, Z. A. P. (2009). Calculando a significância clínica e o índice de mudança confiável em pesquisa-intervenção. São Carlos, SP: EDUFSCar. [ Links ]
Bonifazi, M., Lisasuman, A., Cambiaggi, C., Felici, A., Grasso, G., Lodi, L., ... Carli, G. (2006). Changes in salivary cortisol and corticosteroid receptor-α mRNA expression following a 3-week multidisciplinary treatment program in patients with fibromyalgia. Psychoneuroendocrinology, 31(9), 1076–1086. doi: 10. [ Links ]1016/j.psyneuen.2006.06.008.
Crofford, L. J., Young, E. A., Engleberg, N. C., Korszun, A., Brucksch, C. B., McClure, L. A., ... Demitrack, M. A. (2004). Basal circadian and pulsatile ACTH and cortisol secretion in patients with fibromyalgia and/or chronic fatigue syndrome. Brain, Behavior, and Immunity, 18(4), 314–325. doi: 10. [ Links ]1016/j.bbi.2003.12.011
Cunha, J.A. (2001). Manual da versão em português das Escalas Beck. São Paulo, SP: Casa do Psicólogo. [ Links ]
Del Prette, Z.A.P., & Del Prette. A. (2001). Inventário de Habilidades Sociais (IHS). São Paulo, SP: Casa do Psicólogo. [ Links ]
Del Prette, Z.A.P., & Del Prette. A. (2009). Avaliação de habilidades sociais: bases conceituais, instrumentos e procedimentos. In A. Del Prette, Z. A. P. Del Prette (Eds.) Psicologia das habilidades sociais: diversidade teórica e suas implicações (pp.187-229). Petrópolis, RJ: Vozes. [ Links ]
Fries, E., Dettenborn, L., & Kirschbaum, C. (2009). The cortisol awakening response (CAR): Facts and future directions. International Journal of Psychophysiology, 72(1), 67–73. doi: 10. [ Links ]1016/j.ijpsycho.2008.03.014.
Heymann, R. E., Paiva, E. S., Helfenstein, J. M., Pollak, D. F., Martinez, J. E., Provenza, J. R., Fonseca, M. C. M. (2010). Consenso brasileiro do tratamento da fibromialgia. Revista Brasileira de Reumatologia, 50(1), 56-66. doi: 10. [ Links ]1590/S0482-50042010000100006.
Hunziker, M. H. L. (2010). Comportamento de dor: Análise funcional e alguns dados experimentais. Trends in Psychology, 18(2), 327-333. Recovered: <http://pepsic.bvsalud.org/scielo.php?script=sci_arttext&pid=S1413-389X2010000 200007&lng=pt&nrm=iso> [ Links ].
Jacobson, N. S., & Truax, P. (1991). Clinical significance: A statistical approach to defining meaningful change in psychotherapy research. Journal of Consulting and Clinical Psychology, 59(1), 12–19. doi: 10. [ Links ]1037/0022-006X.59.1.12.
Jensen, K. B., Kosek, E., Wicksell, R., Kemani, M., Olsson, G., Merle, J. V., Kadetoff, D., & Ingvar, M. (2012). Cognitive Behavioral Therapy increases pain-evoked activation of the prefrontal cortex in patients with fibromyalgia. Pain, 153(7), 1495-1503. doi: 10. [ Links ]1016/j.pain.2012.04.010.
Kazdin, A. E. (1999). The meanings and measurement of clinical significance. Journal of Consulting and Clinical Psychology, 67(3), 332–339. doi: 10. [ Links ]1037/0022-006x.67.3.332.
Kazdin, A. E. (1999). Os significados e medidas de significância clínica. Jornal de Consultoria e Psicologia Clínica, 67(3), 332-339. doi: 10. [ Links ]1037/0022-006x.67.3.332.
Keefe, F. J. (1982). Behavioral assessment and treatment of chronic pain: Current status and future directions. Journal of Consulting and Clinical Psychology, 50(6), 896–911. doi: 10. [ Links ]1037/0022-006X.50.6.896.
Kirchner, L. F., Reis, M. J. D., & Queluz, F. N. F. R. (2019). Intervenção comportamental para dor e sono em mulheres com fibromialgia. Acta Comportamentalia, 27(3), 371-388. [ Links ]
Kohlsdorf, M., & Costa Junior, A.L. (2009). O autorrelato na pesquisa em psicologia da saúde: desafios metodológicos. Psicologia Argumento, 27(57), 131-139. doi: 10. [ Links ]7213/rpa.v27i57.19763.
Lindsay, W. R., & Stoffelmayr, B. E. (1982). The Concept of Generalization in Behaviour Therapy. Behavioural Psychotherapy, 10(04), 346. doi: 10. [ Links ]1017/s0141347300008223.
Lipp, M. E. N. (2000). Inventário de sintomas do stress para adultos. São Paulo, SP: Casa do Psicólogo. [ Links ]
Main, C. J., Keefe, F. J., Jensen, M. P., Vlaeyen, J. W. S., & Vowles, K. E. (2014). Fordyce's behavioral methods for chronic pain and illness. Philadelphia: Lippincott Williams and Wilkins. [ Links ]
Meeus, M., Nijs, J., Vanderheiden, T., Baert, I., Descheemaeker, F., & Struyf, F. (2014). The effect of relaxation therapy on autonomic functioning, symptoms and daily functioning, in patients with chronic fatigue syndrome or fibromyalgia: a systematic review. Clinical Rehabilitation, 29(3), 221–233. doi: 10. [ Links ]1177/0269215514542635.
Morley, S., Linton, S.J., & Vlaeyen, J.W. (2015). Single case research methodology in clinical pain management – introduction and practical workshop. Conference at 9th Congress of the European Pain Federation, Vienna, Austria. [ Links ]
Nicassio, P. M., Radojevic, V., Weisman, M. H., Schuman, C., Kim, J., Schoenfeld-Smith, K., & Krall, T. A. (1997). Comparison of behavioral and educational interventions for fibromyalgia. Journal of Rheumatology, 24(10), 2000–2007. [ Links ]
Paiva, E. S., Heymann, R. E., Rezende, M. C., Helfenstein, M., Martinez, J. E., Provenza, J. R., Ranzolin, A., Assis, M. R., Pasqualin, V. D., & Bennett, R. M. (2013). A Brazilian Portuguese version of the Revised Fibromyalgia Impact Questionnaire (FIQR): a validation study. Clinical Rheumatology, 32(8), 1199-206. doi: 10.1007/s10067-013-2259-6. [ Links ]
Penido, M. A., & Rangé., B. (2007). Treinamento em Habilidades Sociais no Tratamento da Dor Crônica. In G. Angelotti (Ed.) Terapia Cognitivo Comportamental no tratamento da dor crônica (pp.107-120). São Paulo, SP: Casa do Psicólogo. [ Links ]
Rachlin, H. (2010). Pain and behavior after 25 years. Trends in Psychology, 18(2), 425-427. Recovered: http://pepsic.bvsalud.org/scielo.php?script=sci_arttext&pid=S1413-389X2010000200016&lng=pt&nrm=iso [ Links ]
Reis, M. J. D., & Rabelo, L. Z.(2010). Fibromialgiaeestresse: Explorando relações. Trends in Psychology, 18(2), 399-414. Recovered: <http://pepsic.bvsalud.org/scielo.php?script=sci_arttext&pid=S1413-389X2010000200014&lng=pt&nrm=iso> [ Links ]
Riva, R., Mork, P. J., Westgaard, R. H., Rø, M., & Lundberg, U. (2010). Fibromyalgia Syndrome is Associated with Hypocortisolism. International Journal of Behavioral Medicine, 17(3), 223–233. doi: 10. [ Links ]1007 / s12529-010-9097-6.
Scipio, C., Keefe, F., Anderson, T., Caldwell, L., Goldman, G., Caldwell, D., & Stainbrook, D. (2005). Links between social communication skills and physiological and psychosocial functioning in patients with RA. The Journal of Pain, 6(3), S24. doi: 10. [ Links ]1016/j.jpain.2005.01.093.
Skinner, B.F (2003) Ciência e comportamento humano. (J. C. Todorov, R. Azzi. Trans.) São Paulo, SP: Martins Fontes. [ Links ]
Slater, M. A., Doctor, J. N., Pruitt, S. D., & Atkinson, H. J. (1997). The clinical significance of behavioral treatment for chronic low back pain: an evaluation of effectiveness. Pain, 71(3), 257–263. doi: 10. [ Links ]1016/s0304-3959 (97) 03374-5.
Thieme K., Flor H., & Turk D.C. (2006). Psychological treatment in fibromyalgia syndrome: Efficacy of operant behavioural and cognitive behavioural treatments. Arthritis Research & Therapy, 8(4), R121. doi:10. [ Links ]1186/ar2010.
Van Houdenhove, B. (2003). Fibromyalgia: a challenge for modern medicine. Clinical Rheumatology, 22(1), 1–5. doi:10. [ Links ]1007/s10067-002-0672-3.
Vandenberghe. L. (2005). Abordagens comportamentais para a dor crônica. Psicologia Reflexão e Critica, 18(1), 47-54. doi:10. [ Links ]1590/S0102-79722005000100007.
Wolfe, F., Clauw, D. J., Fitzcharles, M.-A., Goldenberg, D. L., Katz, R. S., Mease, P., ... Yunus, M. B. (2010). The American College of Rheumatology Preliminary Diagnostic Criteria for Fibromyalgia and Measurement of Symptom Severity. Arthritis Care & Research, 62(5), 600–610. doi: 10. [ Links ]1002/acr.20140.
 Endereço para correspondência
Endereço para correspondência
Luziane de Fátima Kirchner
Graduate Program in Psychology
Dom Bosco Catholic University
6000 Almirante Tamandaré St
Campo Grande-MS, Brazil
CEP: 79117-010
+55 67 98190-2100
Recebido em: 09/2019
Reformulado em: 10/2019
Aceito em: 11/2019
Nota das autoras:
Financing: Coordenação de Aperfeiçoamento de Pessoal de Nível Superior (CAPES)
Sobre as autoras:
Luziane de Fátima Kirchner
PhD in Psychology from Federal Univerisity of São Carlos - UFSCar. She is currently Professor at Dom Bosco Catholic University - UCDB
E-mail: luzianefk@gmail.com
Orcid.org/0000-0002-3579-1768
Maria de Jesus Dutra dos Reis
PhD in Experimental Psychology from the University of São Paulo. She is Associate Professor at Federal University of São Carlos, UFSCar.
E-mail: jesus-reis@uol.com.br
Orcid.org/0000-0002-5128-2074
Francine Náthalie Ferraresi Rodrigues Queluz
PhD in Psychology from Federal University of São Carlos – UFSCar. She is currently a pos-doc researcher at São Francisco University.
E-mail: francine.queluz@gmail.com
Orcid.org/0000-0002-8869-6879

