










Services on Demand

article
 English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
Indicators
Share

 Permalink
PermalinkPsicologia: teoria e prática
Print version ISSN 1516-3687
Psicol. teor. prat. vol.20 no.2 São Paulo May/Aug. 2018
https://doi.org/10.5935/1980-6906/psicologia.v20n2p309-324
ARTICLES
CLINICAL PSYCHOLOGY
Beliefs about childhood cancer: perceptions of survivors and mothers
Creencias sobre el cáncer en niños: percepción de sobrevivientes y madres
Elisa Kern de CastroI; Franciele Cristiane PelosoII; Luisa VitalIII; Maria Júlia ArmiliatoIV
IUniversidade do Vale do Rio dos Sinos, Unisinos, RS, Brasil
IIUniversidade do Vale do Rio dos Sinos, Unisinos, RS, Brasil
IIIUniversidade do Vale do Rio dos Sinos, Unisinos, RS, Brasil
IVUniversidade do Vale do Rio dos Sinos, Unisinos, RS, Brasil
ABSTRACT
Beliefs regarding a disease refer to mental schemes people construct based on their direct or indirect experiences and that are related to their health behavior and self-regulation. Such beliefs help childhood cancer survivors understand their behavior in their follow-up treatment. This study's purpose was to examine the beliefs concerning childhood cancer among 27 survivors and 49 mothers, who completed sociodemographic surveys and questionnaires addressing disease perceptions via an online platform. Results reveal that mothers, more frequently than survivors, perceived childhood cancer as a chronic disease with cyclical symptoms, with more negative consequences and emotional representations. The mothers also reported having greater understanding regarding the disease and more strongly believed in personal and treatment control in comparison to survivors. The conclusion is that the fact that survivors more positively perceived childhood cancer may indicate they re-signified their experiences in an adaptive manner.
Keywords: cancer; childhood cancer; health beliefs; self-regulation; illness perception.
RESUMEN
Las creencias sobre la enfermedad se refieren a esquemas mentales que las personas construyen a partir de su experiencia directa o indirecta y que se relacionan con su conducta en salud y autorregulación. En sobrevivientes de cáncer en la niñez, sus creencias ayudan a comprender sus conductas en el periodo post-tratamiento. El objetivo fue examinar las creencias sobre el cáncer en la niñez en 27 sobrevivientes adultos jóvenes y 49 madres que contestaron a cuestionarios sociodemográfico y de percepción de la enfermedad en un sitio web. Los resultados mostraron que las madres percibieron el cáncer en la niñez como una enfermedad crónica, con síntomas cíclicos, con consecuencias y representación emocional más negativa que los sobrevivientes. Además, las madres refirieron comprender la enfermedad y creer en el control personal y del tratamiento a un nivel más alto que los sobrevivientes. Se concluye que el hecho de que los sobrevivientes perciban el cáncer en la niñez de manera más positiva pueda indicar una nueva significación de la experiencia de manera positiva.
Palabras clave: cáncer; cáncer en niños; creencias en salud; autorregulación; percepción de la enfermedad.
Introduction
Childhood cancer represents a set of diseases that have in common the uncontrolled proliferation of abnormal cells anywhere in the body. The disease represents the most common cause of death by natural causes (7%) among 1- to 19-year-old individuals; 12,600 new cases are expected in Brazil in 2018. The most frequent types of tumors during childhood include lymphoma, neoplasia in the central nervous system, and leukemia. Cure is possible for 70% of patients worldwide; however, survival rates in Brazil are lower than expected because of regional differences in the supply of specialized services. Treatments include chemotherapy, radiotherapy, surgery, and bone marrow transplantation (INCA, 2018).
One way to understand the potential effects of childhood cancer would be to investigate the beliefs of individuals. The Common Sense Model of Self-Regulation (CSMR) (Leventhal, Nerenz, & Steele, 1984) is used to understand how individual beliefs or subjective perceptions that people hold regarding a given disease interfere in individuals' health. According to this model, people organize their thoughts concerning a given disease or the threat it represents through mental schemes that are constructed over the course of life. In the face of a threat to one's health, people refer to their schemes to identify and assess their possibilities for cure of and/or recovery from their health condition, as well as what behaviors they are supposed to adopt to cope with it (Leventhal et al., 1984; Leventhal, Leventhal, & Breland, 2011). The CSMR is structured according to nine dimensions: 1) identity (symptoms); 2) cyclical timeline; 3) acute/chronic timeline; 4) causes (what individuals believe caused the disease); 5) consequences (real or imaginary); 6) personal control (what an individual believes s/ he can do to manage the disease and/or aid its cure); 7) treatment control (how much an individual believes in the treatment); 8) illness coherence (how much an individual understands the disease); and 9) emotional representation (emotional impact caused by the disease) (Moss-Morris et al., 2002; Phillips, Leventhal, & Leventhal, 2012).
Prior representations originating from an individual's culture regarding cancer, added to his/her experiences, play an essential role in the way the individual perceives and copes with a disease (Phillips et al., 2012). In the case of childhood cancer, the disease strongly affects the child's family and especially the mother, who is an important source of care during treatment and whose mental health may be affected (Bemis et al., 2015; Lawrenz, Peuker, & Castro, 2016). It is common, after the treatment is finished, for the survivor and family members to experience ambivalent feelings. On the one hand, there is joy for the child having overcome the disease but there is also fear of relapse (Hosoda, 2014).
Beliefs concerning childhood cancer after treatment and repercussions for the lives of both survivors and their families are seldom explored. One study (Wenninger et al., 2013) assessed the perception of illness of 167 survivors of childhood cancer concerning how they understand their coping process and psychological health. The results show that survivors are not very optimistic about their future, which consequently leads to a negative emotional representation of the disease. The highest levels of distress were found among female survivors, who did not have stable affective relationships and experienced treatment side effects. Another study addressing 16 mothers of childhood cancer survivors identified correlations between some dimensions of illness perception and symptoms of post-traumatic stress disorder (PTSD). A negative emotional representation of childhood cancer was the dimension most frequently related to PTSD, especially flashbacks and avoidance. Greater personal control was associated with fewer avoidance symptoms (Lawrenz et al., 2016). So far, only one study related the perception of illness of caregivers and children (Juth, Silver, & Sender, 2015), however, the children were adolescents still in the treatment phase. The results indicate that a subjective perception of the severity of the disease was associated with objective indicators. The adolescents' subjective perception of the severity of the disease was associated with their mental health and also that of their caregivers.
Therefore, considering that the experience of childhood cancer reflects on the lives of those involved at the medium and long terms, this study's objective was to examine the beliefs of childhood cancer among survivors and mothers.
Method
Design: This is an Ex Post Facto study.
Participants
A total of 27 survivors of childhood cancer (average age = 23.1 years old; SD = 4.61) and 49 mothers of childhood cancer survivors (average age = 43.8 years old; SD = 9.7) linked to the Childhood Cancer Institute of Rio Grande do Sul (ICI-RS) took part in this study. Inclusion criteria were having experienced childhood cancer, being in remission for at least one year, and being older than 18 years of age at the time of data collection. The mothers should have experienced childhood cancer with one of their children and have been one of their child's caregivers during the treatment. Patients still in the active phase of treatment for childhood cancer at the time of data collection were not included.
The participants were contacted through the dissemination of the study in the social network of the Childhood Cancer Instituted of the Rio Grande do Sul (ICI-RS) and that of the University and also via telephone using a list the institution provided. Participation was through an online platform. Because the participants remained anonymous, we could not identify how many mother-child pairs were in the sample.
Instruments
• Form addressing sociodemographic and clinical data - childhood cancer survival version: questions related to sociodemographic data (sex, age, marital status, education, etc.) and information regarding the disease and its treatment (data about the diagnosis, treatment and remission).
• Revised Illness Perception Questionnaire - IPQ-R (Moss-Morris et al., 2002): assesses the beliefs or perceptions an individual holds or has held regarding a disease. The instrument is divided into three sections: (a) Diseases identity: a list of symptoms where the individuals are supposed to indicate whether the symptoms are related to the disease or not; (b) cyclical timeline, acute/chronic timeline, Consequences, Personal Control, Treatment Control, Illness Coherence; and Emotional Representation: answers are presented in a five-point Likert scale where the individual indicates how much s/he agrees with the statement; (c) Causes of the disease: answers are provided on a five-point Likert scale where individuals check their level of agreement. The higher the score, the more negative are one's beliefs or illness perception. At the end of the instrument, the participant is supposed to list the three main causes s/he believes contributed to disease onset. The instrument was originally written in English but the version translated into Portuguese, used in another Brazilian study, was adopted here (Castro, Aretz, Lawrenz, Romeiro, & Haas, 2015).
• Revised Illness Perception Questionnaire for Healthy People - IPQ-RH (Figueiras & Alves, 2007): is the instrument that corresponds to the IPQ-R to assess illness perceptions among healthy individuals. The sessions and scales are the same as those contained in the IPQ-R. The original version is written in Portuguese as used in Portugal, and the version adapted to Brazil had already been used in other studies (Castro, Peuker, Lawrenz, & Figueiras, 2015; Lawrenz et al., 2016).
Procedures
Data Collection
Data were collected using a self-report form and the search for participants was both active and reactive. The reactive search occurred by disseminating the survey online platform on the web pages of the ICI-RS and of the Brazilian Society of Pediatric Oncology and also through folders available at the ICI-RS's reception. An active search was implemented using a list provided by the ICI-RS containing the files of families that had asked for some type of assistance at the institution. These families were called via telephone and invited to complete the survey, the link for which was later sent by email. A total of 95 families out of the 130 listed was contacted between 2015 and 2016; however we cannot determine how many of these families completed the instrument in response to the telephone call or how many completed the survey in response to any of the other strategies used to disseminate it, because the respondents remained anonymous. A free and informed consent form was completed as soon as the participants accessed the website. Only after they provided their consent were they able to access the online form. Data collection was automatically interrupted when participants did not provide their consent.
Data analysis
Data were analyzed using the SPSS 22.0. Descriptive analyzes (frequency, percentage, mean, standard deviation) were performed with the sociodemographic and clinical data of childhood cancer survivors and mothers. The frequency and percentage of symptoms assigned to childhood cancer by survivors and mothers were also verified. To analyze the causes of the disease spontaneously reported by the participants, we used the categorization developed by Peuker et al. (2016; 2015); the frequencies and percentages for answers were also verified by group. Inferential statistics was checked using z scores to standardize the answers of the patients who completed the IPQ-R and IPQ-RH. The distribution of the sample was not normal for most variables (Shapiro-Wilk test), which led to using the Mann-Whitney U test to examine potential discrepancies in the beliefs of mothers and survivors. Additionally, the Chi-square test was performed to verify significant differences between causes and symptomatology between groups. The level of significance was established at p<0.05 and the size effect was also calculated (Cohen's d).
Ethical considerations
This study was approved by the Institutional Review Board at the Unisinos University, with the consent of ICI-RS, under CAE No. 13962113.8.1001.5344. Ethical procedures concerning research addressing human subjects were in compliance with resolution No. 466/12. The web pages that contained the information collected were protected with a password to ensure the confidentiality and safety of information.
Results
Sample characterization
Among the survivors, 59.3% (N = 16) were women and 40.7% (N = 11) were men, 48.1% (N = 13) were married or had a stable partner and were aged 23.1 years old at the time of data collection (SD = 4.61). In terms of education, 55.5% (N = 15) had attended higher education and the remaining 44.5% (N = 12) had attended high school. Diagnoses were obtained 14 years ago on average (SD = 7.04) and at the time of the diagnosis, the participants were nine years old on average (DP = 5.3). The treatment lasted an average of 2.46 years (SD = 2.33) and 55.6% (N = 15) did not attend school in part of this period. The participants were in clinical remission for at least 11.04 years (SD = 7.51), on average. In regard to the type of cancer of these survivors, 44.4% (N = 12) had been diagnosed with leukemia, 18.5% (N = 5) with lymphoma, 3.7% (N = 1) with CNS tumor, and 33.4% (N = 9) with other types of cancer. In regard to the treatment, all them (N = 27) underwent chemotherapy, 48.1% (N = 13) radiotherapy, 70.4% (N = 19) surgery, and 11.5% (N = 3) underwent bone marrow transplantation. 22.2% (N = 6) relapsed and 25.9% (N = 7) experienced physical sequelae due to the cancer or treatment.
The mothers were currently aged 43.8 years old (SD = 9.7) and 69.4% (N = 34) were married or had a stable partner. In terms of education, 34.7% (N = 17) attended primary school, 40.8% (N = 20) high school, and 24.5% (N = 12) had higher education. The mothers were 33.9 years old on average (SD = 9.24) at the time their children were diagnosed. The children were diagnosed with the disease 9.7 years ago on average (SD = 8.87) and treatment lasted 2.27 years on average (SD = 2.24). Their children were no longer in treatment for an average of 7.5 years (SD = 6.60). Among the 49 participating mothers, 47 (95.9%) were the primary caregivers. In regard to the type of cancer their children experienced, 34.7% (N = 17) reported leukemia, 18.4% (N = 9) lymphoma, 10.2% (N = 5) CNS tumor, and 36.7% (N = 36) reported other types of cancer. In regard to treatment, 91.8% (N = 45) underwent chemotherapy; 40.8% (N = 20) radiotherapy; 53.1% (N = 26) surgery; 18.4% (N = 9) bone marrow transplantation; and 4.1% (N = 2) reported other types of treatment. Among them, 20.4% (N = 10) reported their children's condition relapsed and 30.6% (N = 15) had physical sequelae accruing from the cancer or treatment.
Perception of illness
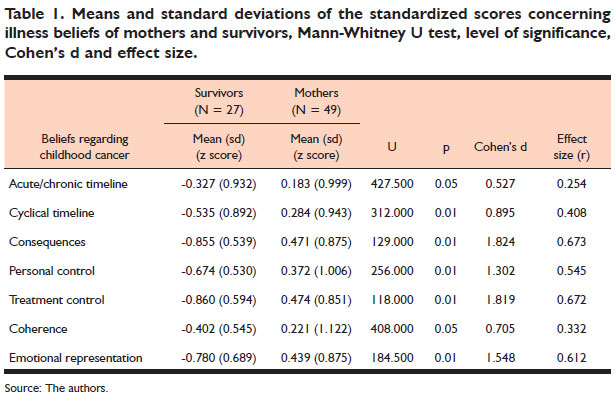
In regard to beliefs about illness, the Mann-Whitney U test revealed differences in the beliefs held by survivors and mothers in all subscales, while mothers scored higher than survivors in all of them, as shown in Table 1. The size effect for most variables was moderate, showing that mothers consider the disease to have more cyclical symptoms than survivors, with more negative consequences and emotional representations. However, compared to the survivors, mothers more frequently believe in personal control and treatment control and also believe they have greater understanding (coherence) of the disease, though the size effect concerning this result is low.
In regard to the symptomatology assigned to childhood cancer (Identity dimension), the main symptoms reported by both survivors and mothers were similar. The Chi-square test revealed significant differences between the groups in terms of the symptoms sore throat and headaches; mothers reported these symptoms more frequently than did the survivors. No significant differences were found in regard to the remaining symptoms. Fatigue, loss of energy, pain, and weight loss were the main symptoms assigned to childhood cancer, as presented in Table 2.
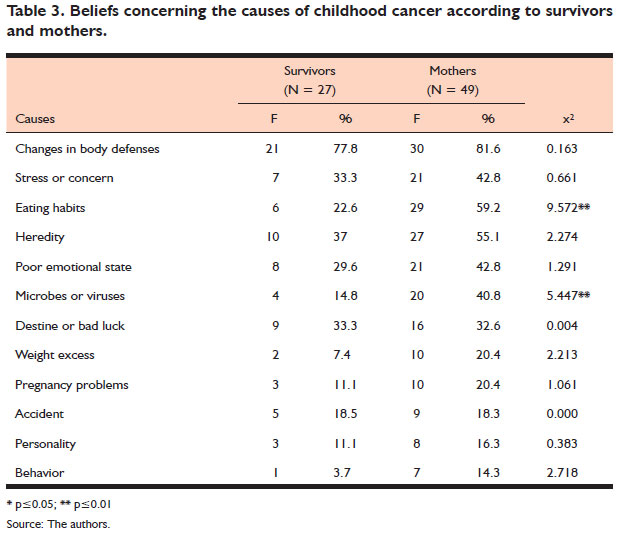
Finally, in regard to beliefs of what caused the disease, the Chi-square test revealed significant differences between the groups concerning the causes 'eating habits' and 'microbes or viruses'; mothers reported these causes of childhood cancer more frequently than the survivors. No significant differences were found in regard to the remaining causes. Additionally, causes that were more frequently assigned to childhood cancer were changes in the body's defenses, heredity, destiny or bad luck. The mothers more frequently assigned the causes to body's defenses, eating habits and heredity, as shown in Table 3.
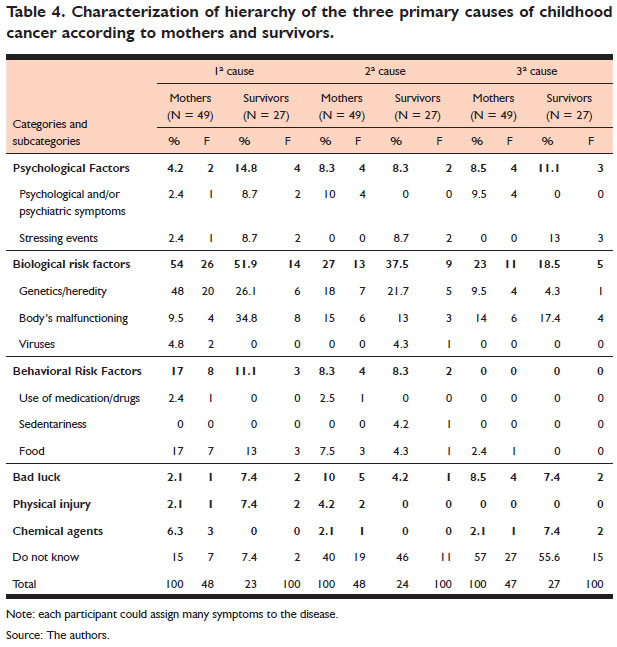
In the instrument's section where individuals are asked to openly list the three main causes they believe had caused their cancer, most participants reported the etiology of the disease was linked to biological risks such as heredity or bodily malfunctioning, as shown in Table 4.
Discussion
This study's main result shows that beliefs about illness held by mothers and survivors present important discrepancies, considering that mothers more frequently present more negative beliefs compared to survivors. Even though the perceptions of symptoms and causes are similar between mothers and survivors, mothers believe childhood cancer has a more chronic nature with more cyclical symptoms, with more severe consequences and negative emotional representation, compared to survivors. On the other hand, mothers also believe they have greater understanding about the disease (coherence) and more frequently perceive greater personal control and believe that treatment controls the disease.
Experiences in the face of a situation of disease may vary considerably due to the individual characteristics and resources of those involved, the severity of the disease, and type of treatment, in addition to the characteristics of the environment (support received from family and health staff, educational level, etc.) (Bemis et al., 2015; Hosoda, 2014). The follow-up of childhood cancer is always surrounded by uncertainty and doubts regarding the future, while knowledge so far involves psychological symptoms and adjustment problems, rather than on variables that can enable one to understand how to adapt to this new phase post-treatment (Wakefield et al., 2010). It is known that mothers more frequently present psychological symptoms compared to childhood cancer survivors, including post-traumatic stress disorder (Castro, Armiliato, Vital, Peloso, & Souza, 2017; Pai et al., 2007). The reasons that lead to such conditions, however, need to be more deeply explored. There is evidence that the eminent risk of death of a child during childhood, in addition to the demands imposed by the disease and other factors, heavily tax these mothers, negatively affecting their mental health.
The survivors' perceptions concerning the chronic nature of child care, with less severe cyclical symptoms, and less negative emotional representations, in comparison to the mothers' perceptions, may be related to a repressive coping style (Myers, 2010). This author's review has shown that people affected by severe diseases, such as childhood cancer, dissociate their somatic responses of emotional distress, seldom express negative affections, and tend to avoid negative information about themselves when assessed through self-reported questionnaires (Myers, 2010). Their mechanisms need to be better understood, though there is evidence that childhood cancer survivors develop this coping style, which may be associated with resilience (Sharpe, Rowe, Russel, Long, & Phipps, 2015). That is, repressing emotional distress associated with the disease may lead to better apparent adaptation and resilience. Therefore, it is possible that, applied to the idea that beliefs about illness, survivors hold more positive illness beliefs than their mothers because they repress or minimize their experiences with the disease.
In regard to coherence perception (understanding) regarding childhood cancer, survivors claim to know less about the disease than the mothers claim to know. They experienced the disease when they were still children, thus, they may have re-signified their memories so that their memories and cognitions were modified (Clanton et al., 2011; Wengenroth et al., 2015). It is also possible that the survivors, while still children, were spared from learning certain information about the disease and the treatment, which would prevent them from having a full understanding of what actually happened. On the other hand, the mothers were among the main caregivers and needed to act actively; that is, they were responsible for seeking medical help, making appointments, seeking clarification and making decisions about the treatment, which lead them to believe they understood what happened.
In regard to the belief that the disease more negatively affected the mothers than the survivors, may be related not only to the distress caused by their children's disease but also to other issues related to financial hardship, the need to abandon their routine lives such as their jobs, family issues related both to their husbands as well as to the care they needed to provide to other children while the sick child was still undergoing treatment; all these situations have been reported in the literature (Pai et al., 2007). Thus, if childhood cancer can be considered a traumatic event (Castro et al., 2017), the difficulties that follow because of the situation are also important stressors that may lead mothers to have a more negative perception of illness in comparison to survivors.
In regard to beliefs about personal control and treatment control, the mothers, more frequently than survivors, hold these beliefs possibly because the result of the treatment was positive and their children are either in remission or are considered to be cured. The survivors, in turn, because they were sick during their childhood, may not have understood or lacked a notion of their role and responsibility for the treatment success. It is, however, assumed that the perceptions concerning these dimensions of the mothers who lost their children is diminished.
Emotional representation accruing from the disease was more negative among mothers than survivors, meaning that mothers consider themselves to be more strongly affected emotionally by cancer than their children. This result may be related to the repressive adaptive coping strategies adopted by some survivors, which were previously mentioned (Myers, 2010; Sharpe et al., 2015). The time elapsed since the diagnosis up to the time of this study (14 years on average) is a period sufficiently long in the life of a young adult. During this period, the survivors may have given a new meaning to their experiences during childhood, developing defense mechanisms and increasing their self-control of their awareness of the time when the stressing event took place as a way to adapt and move on with their lives (Myers, 2010). The mothers, on the other hand, were overwhelmed with responsibilities and the care they had to provide to their children, which, added to a feeling of guilt many of them experienced for having been unable to protect their children from the suffering caused by the disease (Pai et al., 2007), may help explain this result. The diagnosis of cancer imposes a real risk for the life of a child and the mothers, when they realize such a risk exists, may have a more negative emotional representation that, after the treatment, is in general associated with a fear of potential relapse.
The fact the mothers, more frequently than survivors, assign the causes of childhood cancer to eating habits or microbes/viruses shows that their beliefs regarding the disease are distanced from reality. According to the American Cancer Society (ACS, 2017a, 2017b), risk factors among children based on scientific evidence include exposure to radiation, indirect inhalation and smoking, and genetic mutations that occur in the beginning of life or during embryo development. Therefore, even though the mothers experience their children's diseases and received clarification from the health staff, they still hold misconceptions about the causes of childhood cancer. Additionally, both mothers and survivors reported that the main causes of childhood cancer are biological factors, such as changes in body defenses and heredity. Although, it is noteworthy that while psychological stress and poor emotional state were not considered to be the main causes, both survivors and mothers mentioned these factors. There is evidence that stress decreases one's immunity and/or leads to the development of unhealthy habits, such as poor eating habits and the use of alcohol and/or drugs, and that these factors are linked to oncological diseases (Ashford et al., 2015). This relationship with the etiology of childhood cancer, though, is not clearly established (INCA, 2017). The relationship of stress with the development of cancer is not discarded, as it is a relationship that is constantly investigated; however, such an association has not been specifically established with childhood cancer.
In regard to the symptomatology of childhood cancer, both mothers and survivors report that the main symptoms are fatigue, loss of strength, weight loss and pain. Significant differences were found between the two groups in terms of headaches and sore throat. The mothers, more frequently than survivors, believe these symptoms are related to childhood cancer. In fact, these symptoms are common in childhood cancer but their onset depends on the type of cancer and the child's general state (INCA, 2017). It is possible that the memories mothers have regarding the pain and malaise children experienced during the treatment are related to this symptomatology.
This study's results indicate that the beliefs survivors held regarding childhood cancer were more positive than those of their mothers. This result may be associated with their mental health because, as reported in the literature, the mothers of survivors present more psychological symptoms than their children (Castro et al., 2017). Additionally, this study addresses childhood cancer so that the memories of survivors regarding the event may have been affected by their growth process and maturation inherent to the cycle of life. These relationships, however, need to be better clarified in future studies, as well as the association between one's perception of childhood cancer and difficulties mothers and survivors faced during treatment, such as access to health services, family issues related to a husband and other children, to one's job, among others.
This study is the first to examine the beliefs of mothers and survivors regarding childhood cancer. In this sense, relevant contributions are presented here and indicate there is a need to understand what survivors and their mothers think about the disease in order to help them cope with situations in life and the fear of relapse, in addition to enabling them to acquire improved quality of life. This study's contribution also includes the fact it shows and reinforces the need for specialized psychological care to be provided by the pediatric oncological staff to help children and their families to deal with the disease and minimize distress.
This study's limitations include the small number of participants, the fact that data were collected online, and it was not possible to match the mothers with the children who participated in the study. The results, however, were very clarifying and suggest that future studies should more deeply investigate beliefs concerning mental health to implement interventions intended to help survivors and their mothers to acquire improved quality of life.
References
American Cancer Society (2017a). Do we know what causes childhood leucemia? Recuperado em 22 junho, 2017, de https://www.cancer.org/cancer/leukemiain-children/causes-risks-prevention/what-causes.html [ Links ]
American Cancer Society (2017b). Risk factors and causes of childhood cancer. Recuperado em 22, 2017, de https://www.cancer.org/cancer/cancer-in-children/risk-factors-and-causes.html [ Links ]
Ashford, N., Bauman, B., Brown, H., Clapp, R., Finkel, A., Gee, D., Hattis, D., Martuzzi, M., Sasco, A., & Sass, J. (2015). Cancer risk: role of environment. Science, 347(6223),727-732. [ Links ]
Bemis, H., Yarboi, J., Gerhardt, C. A., Vannatta, K., Desjardins, L., Murphy, L. K., & Compas, B. E. (2015). Childhood cancer in context: sociodemographic factors, stress, and psychological distress among mothers and children. Journal of Pediatric Psychology, 40(8),733-743. doi:10.1093/jpepsy/jsv024 [ Links ]
Castro, E. K. de, Aretz, M., Lawrenz, P., Romeiro, F. B., & Haas, S. A. (2015). Illness perceptions in Brazilian women with cervical cancer, women with precursory lesions and healthy women. Psicooncología, 10(2-3),417-423. doi:10.5209/rev [ Links ]
Castro, E. K. de, Armiliato, M. J., Vital, L., Peloso, F., & Souza, M. A. de (2017). Mental health and childhood cancer: the relationship between PTSD symptoms in survivors and mother. Revista Brasileira de Psicoterapia, 19(2),5-16. [ Links ]
Castro, E. K., Peuker, A. C., Lawrenz, P., & Figueiras, M. J. (2015). Illness perception, knowledge and self-care about cervical cancer. Psicologia: Reflexão e Crítica, 28(3),483-489. doi:10.1590/1678-7153.201528307 [ Links ]
Clanton, N. R., Klosky, J. L., Li, C., Jain, N., Srivastava, D. K., Mulrooney, D., ... Krull, K. R. (2011). Fatigue, vitality, sleep, and neurocognitive functioning in adult survivors of childhood cancer: a report from the Childhood Cancer Survivor Study. Cancer, 117(11),2559-2568. doi:10.1002/cncr.25797 [ Links ]
Figueiras, M. J., & Alves, N. C. (2007). Lay perceptions of serious illnesses: an adapted version of the Revised Illness Perception Questionnaire (IPQ-R) for healthy people. Psychology & Health, 22(2),143-158. doi:10.1080/14768320600774462 [ Links ]
Hosoda, T. (2014). The impact of childhood cancer on family functioning: a review. Graduate Student Journal of Psychology, 15,18-30. Recuperado em 15 setembro, 2017, de http://www.tc.columbia.edu/publications/gsjp/gsjp-volumes-archive/36303_2hosoda.pdf [ Links ]
Howard Sharp, K., Rowe, A., Russel, K., Long, A., & Phipps, S. (2015). Predictors of psychological functioning in children with cancer: disposition and cumulative life stressors. Psycho-Oncology, 24,779-786. doi:10.1002/pon.3643 [ Links ]
Instituto Nacional de Câncer José Alencar Gomes da Silva - INCA (2018). Câncer infantil. Recuperado em 5 junho, 2017, de http://www2.inca.gov.br/wps/wcm/connect/tiposdecancer/site/home/infantil [ Links ]
Juth, V., Silver, R. C., & Sender, L. (2015). The shared experience of adolescent and young adult cancer patients and their caregivers. Psycho-Oncology, 24(12),1746-1753. doi:10.1002/pon.3785 [ Links ]
Lawrenz, P., Peuker, A. C. W. B., & Castro, E. K. de (2016). Illness Perception and Indicators of PTSD in Mothers of Childhood Cancer Survivors. Trends in Psychology, 24(51),439-450. doi:10.9788/TP2016.2-03En [ Links ]
Leventhal, H., Leventhal, E. A., & Breland, J. Y. (2011). Cognitive science speaks to the "Common-Sense" of chronic illness management. Annals of Behavioral Medicine, 41(2),152-163. doi:10.1007/s12160-010-9246-9 [ Links ]
Leventhal, H., Nerenz, D. L., & Steele, D. J. (1984). Illness representation and coping with health threats. In A. Baum, S. E. Taylor, & J. E. Singer (Eds.), Handbook of psychology and health (pp. 219-252). [ Links ]
Moss-Morris, R., Weinman, J., Petrie, K., Horne, R., Cameron, L., & Buick, D. (2002). The Revised Illness Perception Questionnaire (IPQ-R). Psychology & Health, 17(1),1-16. doi:10.1080/08870440290001494 [ Links ]
Myers, L. B. (2010). The importance of repressive coping style: findings from 30 years of research. Anxiety, Stress & Coping, 23(1),3-1. doi:10.1080/10615800903 366945 [ Links ]
Pai, A. L. H., Greenley, R. N., Lewandowski, A., Drotar, D., Youngstrom, E., & Peterson, C. C. (2007). A meta-analytic review of the influence of pediatric cancer on parent and family functioning. Journal of Family Psychology, 21(3),407-415. doi:10.1037/0893-3200.21.3.407 [ Links ]
Peuker, A. C., Armiliato, M. J., Souza, L. V., & Castro, E. K. (2015). Causal attribution to cervical cancer. Psicooncología, 12(2-3),249-257. doi:10.5209/rev [ Links ]
Peuker, A. C., Armiliato, M. J., Vital de Souza, L., & Kern de Castro, E. (2016). Causal attribution to cervical cancer. Psicooncología, 12(2-3), 249-257. doi:10.5209/ rev_PSIC.2015.v12.n2-3.51007 [ Links ]
Phillips, L. A., Leventhal, H., & Leventhal, E. A. (2012). Physicians communication of the common-sense self-regulation model results in greater reported adherence than physicians' use of interpersonal skills. British Journal of Health Psychology, 17(2),244-257. doi:10.1111/j.2044-8287.2011.02035.x [ Links ]
Wakefield, C. E., McLoone, J., Goodenough, B., Lenthen, K., Cairns, D. R., & Cohn, R. J. (2010). The psychosocial impact of completing childhood cancer treatment: a systematic review of the literature. Journal of Pediatric Psychology, 35(3),262-274. doi:10.1093/jpepsy/jsp056 [ Links ]
Wengenroth, L., Rueegg, C. S., Michel, G., Gianinazzi, M. E., S, E., Von Der Weid, N. X., ... & Kuehni, C. E. (2015). Concentratio, working speed and memory: cognitive problems in young childhood cancer survivors and their siblings. Pediatric Blood Cancer, 62(5),875-882. doi:10.1002/pbc [ Links ]
Wenninger, K., Helmes, A., Bengel, J., Lauten, M., Völkel, S., & Niemeyer, C. M. (2013). Coping in long-term survivors of childhood cancer: relations to psychological distress. Psycho-Oncology, 22(4),854-861. doi:10.1002/pon.3073 [ Links ]
 Mailling address:
Mailling address:
Elisa Kern de Castro
Avenida Unisinos, 950, Cristo Rei
São Leopoldo, RS, Brazil. CEP 93022000
E-mail: elisakc@unisinos.br
Submission: 11.3.2017
Acceptance: 5.2.2018

{kind=link}
{kind=link}
{kind=link}
{kind=link}