










Services on Demand

article
 English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
Indicators
Share

 Permalink
PermalinkPsicologia: teoria e prática
Print version ISSN 1516-3687
Psicol. teor. prat. vol.21 no.1 São Paulo Jan./Apr. 2019
https://doi.org/10.5935/1980-6906/psicologia.v21n1p102-118
ARTICLES
PSYCHOLOGICAL EVALUATION
Effects of a behavioral intervention in a school setting on hyperactivity and inattention
Efectos de intervención conductual en ambiente escolar sobre desatención e hiperactividad
Alisson Rogério C. de SiqueiraI; Mayara M. M. SilvaII; Elifas T. de PaulaIII; Marcos Vinícius de AraújoIV; Maria Cristina T. V. TeixeiraV; Luiz Renato R. CarreiroVI
IDevelopment Disorders Post-Graduate Program, Mackenzie Presbyterian University (UPM)
IIDevelopment Disorders Post-Graduate Program, Mackenzie Presbyterian University (UPM)
IIIDevelopment Disorders Post-Graduate Program, Mackenzie Presbyterian University (UPM)
IVDevelopment Disorders Post-Graduate Program, Mackenzie Presbyterian University (UPM)
VDevelopment Disorders Post-Graduate Program, Mackenzie Presbyterian University (UPM)
VIDevelopment Disorders Post-Graduate Program, Mackenzie Presbyterian University (UPM)
ABSTRACT
The clinical characteristics of Attention Deficit Hyperactivity Disorder (ADHD) can be a model to identify and manage behaviors of inattention, hyperactivity, and impulsivity of students without the disorder in the classroom. The objectives of the study were to verify the effects of implementing behavioral management guidelines to reduce these behaviors in a mainstream class. A total of 29 second-year students aged between 6 and 8 years were enrolled in the Experimental Group (EG), in which the guide was used, and a Control Group that kept their usual activities. Behavioral profiles were assessed by parents (CBCL/6-18) and teachers (TRF/6-18) before and after the intervention, in addition to an observation protocol filled by teachers. The results, according to teachers' responses, showed reduction in the frequency of inattention and hyperactivity behaviors in the EG. It can be concluded that the guide was effective in the classroom, with the potential for use in school practice.
Keywords: ADHD; behavioural management; classroom; teacher; school.
RESUMEN
Las características clínicas del Trastorno del Déficit de Atención/Hiperactividad (TDAH) pueden ser modelo para identificar y manejar conductas de desatención, hiperactividad e impulsividad de alumnos sin lo trastorno en clases escolares. Los objetivos del estudio fueron verificar los efectos de la implementación de una guía de manejo para reducir estas conductas en una clase. Fueron acompañados 29 alumnos de 2º año, entre 6 y 8 años separados en Grupo Experimental (GE), en el cual se implementó la guía, y un Grupo de Control que continuó con actividades regulares. El perfil conductual fue evaluado por padres (CBCL/6-18) y profesores (TRF/6-18) antes y después de la intervención con protocolo de observación para el profesor. Por las respuestas de los profesores, verificamos reducción de frecuencia de conductas de desatención e hiperactividad en el GE. Se concluye que la utilización de la guía fue eficaz en la clase, indicando su uso potencial en la práctica escolar.
Palabras clave: TDAH; manejo conductual; aula; profesor; escuela.
1. Introduction
Studies on attention-deficit/hyperactivity disorder (ADHD) may be a model for understanding how behaviors of inattention, hyperactivity, and impulsiveness are expressed in the classroom context. The fifth edition of the Diagnostic and Statistical Manual of Mental Disorders of the American Psychiatric Association (DSM-5, American Psychiatric Association, 2014) classifies ADHD as a neurodevelopmental disorder characterized by impairments associated with inattention, disorganization and/or hyperactivity, and impulsivity. The prevalence rates of the disorder are 5% in children and 2.5% in adults (American Psychiatric Association, 2014; Polanczyk, Willcutt, Salum, Kieling, & Rohde, 2014). When interventions are inadequate, ADHD can cause substantial long-term impairment in several areas of social, academic, and occupational functioning as well as in socialization (DuPaul & Stoner, 2007; Sasser, Schoenfelder, & Stein, 2017).
In the case of ADHD in childhood, one of the main concerns of teachers is the stimulation of attentional skills and the reduction of hyperactive behavior patterns in students with the disorder. In the classroom, teachers also need to deal with students who present attentional skills at varying levels, even if they do not have the disorder, in addition to managing the difficulties of students with ADHD who may also be in their classrooms (Suades-González et al., 2017). Previous studies have shown that, during the first years of schooling, teachers report that students, in general, can present behaviors in the classroom such as finding it difficult to focus on their work, follow instructions, complete work, be organized, and may easily be distracted, leave their seat, or try to answer questions before they are complete (Moore, Russell, Arnell, & Ford, 2017). These manifestations may be due to behavioral deficits or excesses that are not compatible with learning situations, often because the child has not developed an adequate repertoire that allows them to concentrate on activities, inhibit distractors or select behaviors appropriate to the situation (Araújo, Carvalho, Teixeira, & Carreiro, 2015). These behaviors, even in children with development within expected milestones, may interfere with academic achievement, impair the quality of classes, and also intensify the frequency and severity of the signs and symptoms of those students in the same class who do have ADHD.
Previous studies have focused on assessing learning impairments associated with inattention and hyperactivity/impulsivity (Smith, Breaux, Green, & Langberg, 2018; Moore et al., 2017) as well as on the development of intervention strategies to minimize such losses (Araújo, 2012; Araújo et al., 2015; Pfiffner et al., 2018; DuPaul, 2018; Faraone et al., 2018). From the clinical point of view, ADHD can be used as a model to understand how the behaviors of inattention, hyperactivity, and impulsivity are expressed in the school environment. Araújo et al. (2015) developed a behavioral intervention program, based on the observation of children with ADHD, that allowed the teacher to act to reduce the frequency of typical behaviors of children with this diagnosis in a classroom context and thereby improve the learning conditions.
Procedures based on the behavioral management of students with ADHD in the school environment can also reduce inattention, hyperactivity, and impulsivity in children without the disorder (Veenman, Luman, & Oosterlaan, 2018; Siqueira, 2015; Barkley, 2002; Cordier, Vilaysack, Doma, Wilkes-Gillan, & Speyer, 2018; Veenman, Luman, & Oosterlaan, 2017). Among behavioral interventions, those based on applied behavioral analysis have shown evidence of efficacy (Barkley et al., 2008; DuPaul & Stoner, 2007), the classroom being a favourable environment for this type intervention. A previous study assessed the effectiveness of a behavioral intervention program conducted by teachers from ten primary schools (intervention group) compared to a control group (Latouche & Gascoigne, 2017). The study observed improved student behaviour as well as an increase in teachers' sense of self-efficacy.
Suades-González et al. (2017) conducted a longitudinal study to evaluate inattentive developmental patterns in children with and without signs of ADHD. From the teachers' reports, the authors observed that the group of children with signs of ADHD showed significant deficits in the areas of executive attention, reaction time, and variability compared to children without any signs of the condition. They also assessed the continuous development of some aspects of attention in primary school children, differentiating patterns by sex, and symptoms of ADHD. These results support the need for intervention programs in schools to facilitate student development, regardless of whether the child has an ADHD-compatible clinical presentation or not.
A study by Veenman et al. (2017) assessed whether the effectiveness of a behavioral management program conducted by teachers to reduce signs of ADHD could be confirmed by other instruments other than the teachers' own accounts. The results indicated that the greater the engagement of the teachers in the program, the greater were the changes reported by them, and did not necessarily match the changes in behavior assessed by other more objective measures. Thus, this study highlighted the importance of using different behavioral measures in the classroom to assess the true effectiveness of intervention programs applied by the teachers.
Signs of ADHD are associated with difficulties in dealing with social, behavioral, and academic elements of school. According to Moore et al. (2017), there is still a lack of studies that assess evidence related to interventions to support children with ADHD in schools. There are also few studies focused on the experiences and practices of educators with children who are inattentive, impulsive, or hyperactive (Tran et al., 2018, Moore et al., 2017). A study by Moore et al. (2017), suggested that factors such as attitudes toward ADHD, relationships experienced by students with ADHD, and other treatments being provided need to be carefully considered before strategies are put into practice in the classroom. The main objective of this study was, therefore, to assess the effects of a behavioral intervention program in the classroom on the frequency of inattention and hyperactivity in students, irrespective of a diagnosis of ADHD.
2. Method
2.1 Participants
The study sample comprised 60 participants (n = 29 students), aged 6 to 8 years and their respective carers (n = 29, 26 parents and three grandparents) and teachers (n = 2, who were the class teachers). The students were enrolled in the 2nd year of elementary school in a Center for Integral Education (CIE) in the city of Curitiba, PR. The participants were divided into an experimental group (EG, 16 students, 11 boys, mean age = 6.3, SD = 0.4) and a control group (CG, 13 students, 11 girls, mean age = 6.4, SD = 0.5). The teachers had more than 10 years' experience of teaching in early childhood education and often participated in continuing education programs provided by the government. The study was conducted during the school year. Data from school records were used to identify the presence of the exclusion criteria, which were any intellectual disability or other neurodevelopmental disorders, such as autism spectrum disorder. All the methodological procedures used were submitted and approved by the Human Subject Research Ethics Committee of the Mackenzie Presbyterian University (Process No. 1169/09/2009 and CAAE No. 0067.0.272.000-09).
2.2 Instruments
Child Behavior Checklist for Ages 6-18: the CBCL/6-18 is completed by parents/caregivers, who are referred to as the informants. The CBCL/6-18 comprises two parts. The first part has seven open questions related to illnesses; disabilities; social, school and practical skills; as well as the interests and the qualities or overall strengths of the child. The second part comprises 113 questions with a list of statements that describe patterns of emotional and behavioral functioning in children and adolescents. The informant has to indicate the frequency of these patterns in the previous six months. Behavior problems are grouped into externalizing and internalizing problems. The checklist allows the grouping of problems in scales, the main ones being: a) syndrome scales (anxious/depressed, withdrawn/depressed, somatic complaints, social problems, thought problems, attention problems, rule-breaking behavior, aggressive behavior); b) DSM-oriented scales (depressive problems, anxiety problems, somatic problems, attention deficit and hyperactivity problems, oppositional and defiant problems, and conduct problems); and c) internalizing, externalizing and total problem scales. The items of the behavior problem scale are scored as 0, when the item is not true; 1, when the item is somewhat or sometimes true; and 2, when the item is very true or often true (Bordin, Rocha, Teixeira, & Rescorla, 2013; Achenbach & Rescorla, 2010; 2001). The validity of the instrument has previously been demonstrated in a Brazilian sample (Rocha et al., 2013).
Child Behavior Checklist for Ages 6-18 (TRF/Teacher's Report Form for Ages 6-18): completed by the student's teacher, also referred to as the informants. The TRF comprises two parts. The first part contains open questions aimed at investigating competencies with a primary focus on the student's academic behaviors. Like the CBCL, the second part comprises statements that describe patterns of emotional and behavioral functioning in children and adolescents, and the teacher indicates the frequency of these patterns of behavior in the previous six months. The problem and behavior scales follow the same grouping as the CBCL (Bordin et al., 2013; Achenbach & Rescorla, 2010; 2001). The validity of the instrument has previously been demonstrated in a Brazilian sample (Rocha et al., 2013).
The Behavioral Management Guide for Children and Adolescents with signs of Inattention and Hyperactivity: the guide produced by Araújo (2012) and published as a book in 2015 (Araújo et al., 2015). The guide was designed with applied behavior analysis as its theoretical basis and employs stimulus control and reinforcement strategies. The guide sets out 16 actions grouped into three strategies: Stimulus Control (SC) - behavior control by antecedent stimulus; Reinforcement (Rf) - behavior control through the use of positive reinforcers for appropriate behaviors; and Reinforcement Stimulus Control (RfSC) - behavior control through antecedent management and positive reinforcement for appropriate behavior. The guide makes it possible to establish implementation rates for each strategy through a checklist and an observation protocol (OP) that must be completed by the teacher (Araújo et al., 2015). The OP comprised 16 items grouped into five behavioral categories: inattention, restlessness, movement, impulsivity, and being easily distracted.
2.3 Data collection procedures
The EG teacher was responsible for the implementation of the behavioral management guide developed by Araújo et al. (2015), the teacher of the CG did not receive any special training. The 2nd grade classes were chosen because they were not the students' entrance or final classes of EF I (elementary school). The CBCL/6-18 and the TRF/6-18 were applied by the first author at the beginning of the school year and reapplied after 28 weeks at the end of the intervention. In addition, the teacher completed the OP for each student at the beginning and end of the intervention and weekly checklists on the use of the tips of the guide. The teacher of the EG attended 12, 45-minute training sessions on the use of the guide and its suggested classroom methods, behavioral management strategies, and on how to complete the checklist and OP.
2.4 Data analysis
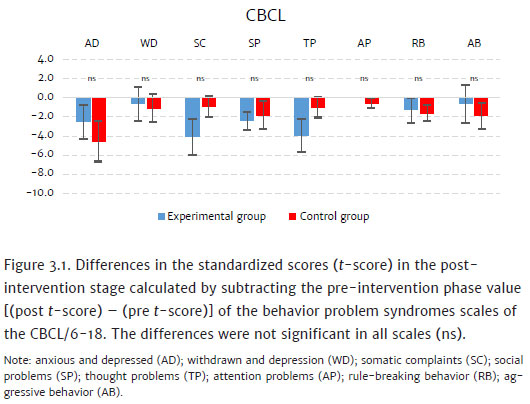
The CBCL and TRF checklists were analyzed using the computer program Assessment Data Manager 7.2 (ADM). The data generated behavioral profiles that could be compared with the scores of normative samples, according to age and sex (Achenbach & Rescorla, 2010; 2001). Data from the Group 3 normative sample (of which Brazil is part) were used in the processing of the study data with ADM (Rescorla et al., 2012). The data were analyzed comparing the differences between the standardized scores (t-score) before and after the intervention, i.e., taking the value of the post-intervention stage and subtracting the value of the pre-intervention stage [difference = (post t-score) - (pre t-score)]. Negative values represented a decrease in problem indicators and positive values an increase. Analyses of the CBCL and TRF syndromes scales and the TRF ADHD scale were conducted using one-way analysis of variance (Anova). All confidence intervals in the study were constructed with a 95% confidence interval. However, values of 0.05 < p < 0.1, because they were close to the acceptance limit, were considered to tend to be significant (up to five percentage points above the alpha value adopted), so they were also described in the results. Parametric statistical tests were used, since the data were quantitative and continuous, with a normal distribution. As for the observation protocol, the percentage of reduction of the behaviors in the post-intervention evaluation in relation to the pre-intervention values for each student was calculated, and the average reduction per group was calculated.
3. Results
The aim of this study was to assess the effects of a behavioral intervention on the frequency of students' inattention and hyperactivity behaviors. The students were divided into two groups, a control group (CG) and an experimental group (EG), and the results of the CBCL/6-18 and TRF/6-18 syndromes scales were analyzed. Regarding the CBCL/6-18, both the EG and CG presented a reduction in all scales, as can be observed by the negative difference values [(post t-score) - (pre t-score)]. In this case, there were no statistically significant differences between the CG and EG comparing the differences (post-intervention - pre-intervention) (Figure 3.1).
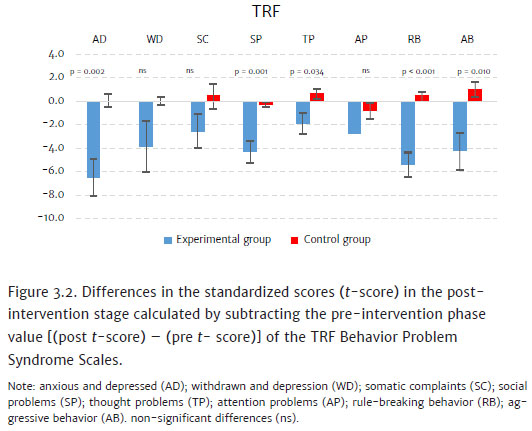
Regarding the TRF/6-18, the EG presented a reduction in all the scales that make up the syndrome scales, as shown in Figure 3.2 (blue bars). In contrast, the CG only showed a slight variation, with some positive values indicating an increase in problems post-intervention. Comparing the differences (post-intervention - pre-intervention) between the EG and the CG by means of one-way Anova, a statistically significant difference was observed between the groups in the following scales: anxious and depressed (AD) (F[1 , 28] = 12,068, p = .002 ); somatic complaints (SC) (F[ 1,28] = 12,615, P = .001); thought problems (TP) (F[1,28] = 5,007, P = .034); rule-breaking behavior (RB) (F[1, 28] = 21.521, P < .001), and aggressive behavior (AB) (F[1, 28] = 7,602, P = .010); in the other scales no significant differences were observed (Figure 3.2). The results indicated that there was a more significant reduction in behavioral problems in the EG compared to the CG, according to the teachers' reports.
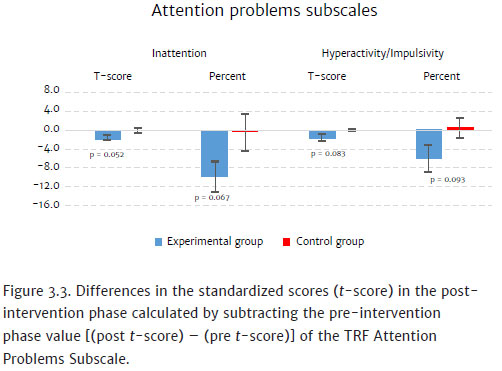
In respect of the DSM-oriented scale of attention deficit and hyperactivity disorders from the TRF, there was a greater reduction in both t-scores and percentile scores for the indicators of both inattention and hyperactivity/impulsivity in the EG compared to the CG (Figure 3.3). Anova revealed marginally significant effects, with values close to significance. This may suggest a greater tendency to reduce these indicators in the EG compared to the CG according to the teachers' reports.
At the beginning of the application of the guide, the teachers reported difficulties in handling some students in the classroom; however, over time, the guide was used more frequently. The checklist completed by the EG teacher during the 28 weeks of the intervention showed a 99% implementation rate and indicated that the teacher used the recommended strategies at least once a week. From the 18th week, a strategy to communicate with parents was used a few times, that is, the strategy was used only in some classes or days during the week.
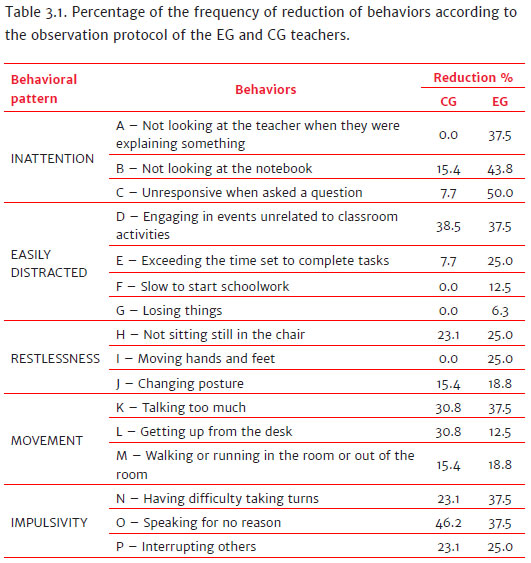
Regarding the percentage of reduction in the frequency of behaviors in relation to the observation protocol, it was observed that the EG obtained a reduction in all items. In the CG, this reduction did not occur in the following behaviors, as shown in Table 3.1: a) behavior A from inattention pattern; b) behaviors F and G from the easily distracted pattern; c) behavior I from the restlessness pattern. Comparing the reduction between the groups, there was a greater reduction in the EG in all behaviors, except for behavior D from the easily distracted pattern, behavior L from the movement pattern and behavior O from the impulsivity pattern (Table 3.1).
4. Discussion
The results, in general, showed a reduction in behaviors characteristic of inattention and hyperactivity in the EG, independently of whether or not the students had ADHD, although some reductions were also observed in the CG. The reduction of these behaviors was more strongly expressed in the data from the TRF checklist and the observation protocol. The main function of the CBCL/6-18 is to be a report from the informant in relation to the home environment, and it was used in this study to assess whether behavioral changes in school would extend into the home environment. Caregivers responding to the CBCL/6-18 after the intervention reported some reductions in behavioral problems, but they were not significantly different in relation to changes in the CG. A similar study of children diagnosed with ADHD (Araújo, 2012), using the same program reported that the effects of the intervention were also found in the family environment. Such variability reinforces the need to use multiple informants to assess behavioral modifications in different environments, as suggested by Veenman et al. (2017). In the present study, the lack of generalization of the findings in the classroom to the family environment may have occurred because of CBCL results showed relatively few indicators of behavioral problems.
The TRF showed a significant reduction in indicators of student behavioral problems in various scales of the instrument in the EG. These behavioral changes in the EG can probably be attributed to the effects of the application of the behavioral management guide. The reductions observed in the CG may have been due to the standard teaching strategies that the teacher used day-to-day in the classroom. In contrast, the EG teacher had been trained in the use of the behavioral management guide and its implementation contributed to a more significant reduction in inattention and hyperactivity/impulsivity in the students of the mainstream class. The teacher, using these procedures, effectively made it possible for the behavior of the students to change. This study had similar results to those of Latouche and Gascoigne (2017), which reported an increase in the knowledge and self-efficacy of teachers in respect of the management of signs of ADHD in students in elementary schools, as well as being a practical and cost-effective measure. The results of our study allow us to make a similar hypothesis; that the teacher also improved their understanding of inattentiveness and hyperactivity/impulsivity in the students, as the use of the intervention was able to reduce such behaviors in the EG.
The study showed that the behavioral management guide was effective in a school environment. Even though the intervention was based on the model of ADHD, that is to say was created for the management of children with the disorder, it was effective in a global way in reducing inattention and hyperactivity in children in a class, independent of a diagnosis of ADHD. These results show that the protocol has the potential for use in school practice. It was also shown that the teacher can be both the informant and the intervening agent responsible for changing classroom behaviors. However, it is important that teachers using the intervention are given precise guidelines and support to allow them to apply the strategies to change classroom behaviors, as well as in respect of the strategies required that allow them to evaluate these changes. Some limitations of the study should be highlighted. The first is in respect of the fact that there was only one teacher per group and the second that one of the instruments used (TRF/6-18) was applied by the same teacher who applied the intervention, which might have resulted in evaluation bias.
Although the study was conducted in a small convenience sample, the efficacy of the guide when applied in a mainstream classroom was tested. Future studies should use larger samples and also assess whether personal or training factors related to individual teachers influence behavioral improvement outcomes. It is also necessary to use other instruments that can assess the student's school performance to avoid any bias resulting from the teacher being the only informant.
References
Achenbach, T. M., & Rescorla, L. A. (2001). Manual for the ASEBA school-age forms & profile. Burlington, VT: University of Vermont, Department of Psychiatry. [ Links ]
Achenbach, T. M., & Rescorla, L. A. (2010). Mental health practitioners' guide the Achebach System of Empirically Based Assessment (ASEBA) (7th ed.). Burlington, VT: University of Vermont, Research Center for Children, Youth & Families. [ Links ]
American Psychiatric Association. (2014). Manual diagnóstico e estatístico de transtornos mentais: DSM- 5. (Trans. Maria Inês Corrêa Nascimento et al., American Psychiatric Association, Ed., 5th ed.). Porto Alegre: Artmed. [ Links ]
Araújo, M. V. (2012). Manejo comportamental pelo professor no contexto de sala de aula de alunos identificados com TDAH: Desenvolvimento, implementação e avaliação de guia de intervenção. (Tese de Doutorado não publicada). Universidade Presbiteriana Mackenzie, São Paulo, Brasil. [ Links ]
Araújo, M. V., Carvalho, A. M., Teixeira, M. C. T. V., & Carreiro, L. R. R. (2015). Orientações práticas para professores de alunos com comportamentos de desatenção e hiperatividade em sala de aula. São Paulo: Casa do Psicólogo. [ Links ]
Barkley, R. A. (2002). Transtorno de Déficit de Atenção/Hiperatividade: Guia completo para pais, professores e profissionais da saúde. Porto Alegre: Artmed. [ Links ]
Barkley, R. A., Anastopoulos, A. D., Robin, A. L., Lovett, B. J., Connor, D. F., Shapiro, C. J., ... Hathaway, W. L. (2008). Transtorno de Déficit de Atenção/Hiperatividade: Manual para diagnóstico e tratamento (3 ed.). Porto Alegre: Artmed. [ Links ]
Bordin, I. A., Rocha, M. M., Teixeira, M. C. T. V, & Rescorla, L. A. (2013). Child Behavior Checklist (CBCL), Youth Self- Report (YSR) and Teacher's Report Form (TRF): an overview of the development of the original and Brazilian versions Child Behavior Checklist (CBCL), Youth Self- Report (YSR) and Teacher's Report For. Cadernos de Saúde Pública, 29(1),13-28. doi: 10.1590/S0102-311X2013000100004 [ Links ]
Cordier, R., Vilaysack, B., Doma, K., Wilkes-Gillan, S., & Speyer, R. (2018). Peer inclusion in interventions for children with ADHD: A systematic review and meta-analysis. Biomed Research International, 2018,1-51. doi: 10.1155/2018/7693479 [ Links ]
DuPaul, G. J. (2018). Promoting success across school years for children with Attention-Deficit/HyperactivityDisorder: Collaborative school-home intervention. J Am Acad Child Adolesc Psychiatry, 57(4),231-232. doi: 10.1016/j.jaac.2018.02.001 [ Links ]
Dupaul, G. J., & Stoner, G. (2007). TDAH nas escolas: estratégias de avaliação e intervenção. São Paulo: M Books. [ Links ]
Faraone, S. V., Rostain, A. L., Blader, J., Busch, B., Childress, A. C., Connor, D. F., & Newcorn, J. H. (2018). Practitioner Review: Emotional dysregulation in attention-deficit/hyperactivity disorder - implications for clinical recognition and intervention. J Child Psychol Psychiatry, 5. doi: 10.1111/jcpp.12899 [ Links ]
Frizzo, G. B., Pedrini, J. R., Souza, D. S, Bandeira, D. R., & Borsa, J. C. (2015). Confiabilidad de la lista de chequeo de comportamiento infantil y la forma de reporte de profesores en una muestra de niños brasileros. Universitas Psychologica, 14(1),149-156. doi: 10.11144/Javeriana.upsy14-1.rcbc [ Links ]
Latouche, A. P., & Gascoigne, M. (2017). In-service training for increasing teachers' ADHD knowledge and self-efficacy. Journal of Attention Disorders, 23(3),270-281. doi: 10.1177/1087054717707045 [ Links ]
Moore, D. A., Russell, A. E., Arnell, S., & Ford, T. J. (2017). Educators' experiences of managing students with ADHD: A qualitative study. Child: Care, Health and Development, 43(4),489-498. doi: 10.1111/cch.12448 [ Links ]
Pfiffner, L. J., Rooney, M. E., Jiang, Y., Haack, L. M., Beaulieu, A., & McBurnett, K. (2018). Sustained effects of collaborative school-home intervention for Attention-Deficit/Hyperactivity Disorder symptoms and impairment. J Am Acad Child Adolesc Psychiatry, 57(4),245-251. doi: 10.1016/j.jaac.2018.01.016 [ Links ]
Polanczyk, G. V., Willcutt, E. G., Salum, G. A, Kieling, C., & Rohde, L. A. (2014). ADHD prevalence estimates across three decades: An updated systematic review and meta-regression analysis. International Journal of Epidemiology, 43(2),434-442. doi:10.1093/ije/dyt261 [ Links ]
Rescorla, L. A., Ivanova, M. Y., Achenbach, T. M., Begonav, I., Chahed, M., Drugli, M. V., ... Zhang, E. Y. (2012). International epidemiology of child and adolescent psychopathology: 2. Integration and applications of dimensional findings from 44 societies. Journal of the American Academy of Child and Adolescent Psychiatry, 51(12),1273-1283, doi: 10.1016/j.jaac.2012.09.012 [ Links ]
Rocha, M. M., Rescorla, L. A., Emerich, D. R., Silvares, E. F., Borsa, J. C., Araújo, L. G., & Assis, S. G. (2013). Behavioural/emotional problems in Brazilian children: findings from parents' reports on the Child Behavior Checklist. Epidemiol Psychiatr Sci, 22(4),329-338. doi: 10.1017/S2045796012000637 [ Links ]
Sasser, T., Schoenfelder, E. N., & Stein, M. A. (2017). Targeting functional impairments in the treatment of children and adolescents with ADHD. CNS Drugs, 31(2),97-107. doi: 10.1007/s40263-016-0400-1 [ Links ]
Smith, Z. R., Breaux, R. P., Green, C. D., & Langberg, J. M. (2018). Evaluation of the interplay between homework motivation and sluggish cognitive tempo in youth with ADHD: Associations with homework performance. J Atten Disord, 3. doi: 10.1177/1087054718763722 [ Links ]
Siqueira, A. R. C. (2015). Manejo comportamental em sala de aula para redução de comportamentos de desatenção e hiperatividade: Orientação ao professor e implementação de guia de intervenção. (Dissertação de Mestrado não publicada). Universidade Presbiteriana Mackenzie, São Paulo, Brasil. [ Links ]
Suades-González, E., Forns, J., García-Esteban, R., López-Vicente, M., Esnaola, M., Álvarez-Pedrerol, M., ... Sunyer, J. (2017). A longitudinal study on attention development in primary school children with and without teacher-reported symptoms of ADHD. Frontiers in Psychology, 8,655. doi: 10.3389/fpsyg.2017.00655 [ Links ]
Tran, J. L. A., Sheng, R., Beaulieu, A., Villodas, M., McBurnett, K., Pfiffner, L. J., & Wilson, L. (2018). Cost-effectiveness of a behavioral psychosocial treatment integrated across home and school for pediatric ADHD-Inattentive Type. Adm Policy Ment Health, 45(5),741-750. doi: 10.1007/s10488-018-0857-y [ Links ]
Veenman, B., Luman, M., & Oosterlaan, J. (2017). Further insight into the effectiveness of a behavioral teacher program targeting ADHD symptoms using actigraphy, classroom observations and peer ratings. Frontiers in Psychology, 8,1157. doi: 10.3389/fpsyg.2017.01157 [ Links ]
Veenman, B., Luman, M., & Oosterlaan, J. (2018). Moderators influencing the effectiveness of a behavioral teacher program. Frontiers in Psychology, 9,298. doi: 10.3389/fpsyg.2018.00298 [ Links ]
 Mailling address:
Mailling address:
Luiz Renato Rodrigues Carreiro
Rua da Consolação, 896, prédio 28, 1º andar, Consolação
São Paulo, SP, Brazil. CEP 01302-907
E-mail: renato.carreiro@gmail.com; luizrenato@mackenzie.br
Submission: 23/05/2018
Acceptance: 14/11/2018
Financial Support: The study was supported by the Coordenação de Aperfeiçoamento de Pessoal de Nível Superior (CAPES), Brasil - Financing code 001, CAPES PROEX (0653/2018), and the Fundo Mackenzie de Pesquisa (Mackpesquisa).

