










Services on Demand

article
 English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
Indicators
Share

 Permalink
PermalinkAvaliação Psicológica
Print version ISSN 1677-0471On-line version ISSN 2175-3431
Aval. psicol. vol.16 no.1 Itatiba Jan./Mar. 2017
https://doi.org/10.15689/ap.2017.1601.02
ARTICLE
DOI: 10.15689/ap.2017.1601.02
Normative data of the Brazilian elderly in Logical Memory subtest of WMS-R*
Dados normativos de idosos brasileiros no subteste Memória Lógica da WMS-R
Datos normativos de los adultos mayores brasileños en sub-test de Memoria Lógica de WMS-R
Camila Rosa de Oliveira1,I; Margarida Maria Baptista Mendes Pedroso de Lima2,II; Cristiane Silva Esteves3,III; Valéria Gonzatti4,III; Susy Ane Ribeiro Viana5,III; Tatiana Quarti Irigaray6,III; Irani Iracema de Lima Argimon7,III
IFaculdade Meridional – IMED, Passo Fundo -RS, Brasil
IIUniversidade de Coimbra, Coimbra, Portugal
IIIPontifícia Universidade Católica do Rio Grande do Sul, Porto Alegre-RS, Brasil
ABSTRACT
The aim of this study was to establish normative data for the Brazilian elderly population in the Logical Memory (LM) subtest of the Wechsler Memory Scale, revised version (WMS-R) and investigate the ability of scores in this subtest (immediate and delayed recall) to discriminate the elderly with and without depressive symptoms. The sample consisted of 334 elderly participants. Participants answered a sociodemographic and health questionnaire, the MMSE, the GDS-15, and the LM subtest. Data were analyzed by descriptive statistics, Student's t test, multiple linear regression, univariate analysis, and discriminant analysis. Age, education, and depressive symptoms significantly influenced all the scores of LM. Normative data were available according to three age groups, three levels of education, sex, and presence or absence of depressive symptoms. Results are in agreement with the literature, demonstrating the importance of establishing reference standards in accordance with sociodemographic and cultural characteristics.
Keywords: aging; verbal memory; memory; cognition.
RESUMO
O presente estudo teve por objetivo estabelecer dados normativos a idosos brasileiros no subteste Memória Lógica (ML) da WMS-R e investigar a capacidade dos escores desse subteste (recordação imediata e tardia) para discriminar idosos com e sem sintomas depressivos. A amostra foi composta por 334 idosos. Os idosos responderam a um questionário sociodemográfico, ao MEEM, à GDS-15 e ao subteste ML. Os dados foram analisados por estatística descritiva, teste t de Student, regressão linear múltipla, análise univariada e análise discriminante. A idade, escolaridade e sintomas depressivos influenciaram significativamente todas as pontuações da ML. Os dados normativos foram disponibilizados de acordo com três grupos etários, três níveis de escolaridade, sexo e presença ou ausência de sintomas depressivos. Os resultados estão de acordo com a literatura, demonstrando a importância de estabelecer padrões de referência de acordo com características demográficas e socioculturais.
Palavras-chave: envelhecimento; memória verbal; memória; cognição.
RESUMEN
Este estudio tuve como objetivo establecer los datos normativos para mayores brasileños en la sub-prueba de la Memoria Lógica (ML) de la Escala de Memoria de Wechsler, versión revisada (WMS-R), e investigar la capacidad de las puntuaciones de la sub-prueba (memoria inmediata y retardada) para discriminar mayores con y sin los síntomas depresivos. La muestra se compuso de 334 personas mayores. Los participantes respondieron a un cuestionario sociodemográfico y de la salud, lo MEEM, la GDS-15 y la sub-prueba de ML. Los datos fueron analizados utilizándose la estadística descriptiva, la prueba t de Student, la regresión lineal múltiple, el análisis univariado y el análisis discriminante. La edad, la educación y los síntomas depresivos influenciaron significativamente todas las puntuaciones de la ML. Los datos normativos incluyen tres grupos de edad, tres niveles de educación, el género y la presencia o ausencia de los síntomas depresivos. Los resultados son consistentes con la literatura, lo que demuestra la importancia de establecer puntos de referencia de acuerdo a las características sociodemográficas y culturales.
Palabras clave: envejecimiento; memoria verbal; memoria; cognición.
Difficulties in recalling recent events are generally associated with mild cognitive impairment and degenerative neurological disorders such as Alzheimer's Disease (AD) (Salthouse, 2014). However, impairment in verbal episodic memory (VEM) could also be observed in the normal aging process (Celsis, 2000), indicating a possible development of dementia (Chapman et al., 2011a). Several studies have suggested the influence of age on VEM, comparing the performance of young adults, adults, and the elderly in recalling wordlist tests or retelling stories (Correia & Osorio, 2013; Silver, Goodman, & Bilker, 2012; Vlahou et al., 2013).
Although there are relevant gaps between different age groups, education has proven to be the factor of higher impact on VEM performance, as well as on other cognitive skills (Stern, 2012). Angel, Fay, Bouazzaoui, Baudouin, and Isingrini (2010) refer to the interaction between age and education in performing a wordlist recalling task, in which adults with lower levels of education performed poorly when compared with those with higher levels of formal education. Although it is expected that some cognitive skills decline with age, some changes are clearly associated with education (Beydoun et al., 2014). Foss, Formigheri and Speciali (2009), for example, find significant positive correlations between level of education and performance in VEM tests in the elderly.
Among other sociodemographic characteristics, gender has been studied with the aim of explaining changes in cognitive performance. However, especially in assessing mnemonic deficits, studies show contradictory results comparing men and women (Chapman et al., 2011b). There is evidence that depressive symptoms also influence VEM performance. In a longitudinal study, Koening et al. (2014) realized that elderly with a history of depression showed a decline in several cognitive skills, among them VEM. Also Pantzar et al. (2014), in a sample of elderly subjects, identified that serious depressive symptoms were associated with lower performance in attention tasks, executive functions, and VEM.
VEM could be assessed through learning/recalling wordlists or through retelling stories (Beck, GagneuxZurbriggen, Berres, Taylor, & Monsch, 2012; Lezak, Howieson, Bigler, & Tranel, 2012). In both tests, codification, storage, and recall processes are observed. Examples of wordlist tests are the Rey Auditory Verbal Learning Test and the California Verbal Learning Test (Lezak et al., 2012). These tests have the advantage of checking association strategies used to recall data — for example, sorting out words according to clues as to their semantic or phonological categories, as well as effects of primacy and recency (Sunderaraman, Blumen, DeMatteo, Apa, & Cosentino, 2013). Furthermore, performance in various trials allows the development of learning curves.
In recalling stories tests, the examiner reads a short story and then asks the participant to retell it. These tasks have a higher level of difficulty as they require new cognitive skills such as inferential processing (moral of the story) and work memory (Welland, Lubinski, & Higginbotham, 2002). In addition, they have higher ecological validity when compared to other VEM tests (Higginson, Arnett, & Voss, 2000), demonstrating a strong association with subjective cognitive complaints in the healthy elderly (Merema, Speelman, Kaczmarek, & Foster, 2012).
The LM subtest of WMS-R (Wechsler, 1987) is widely used in VEM impairments and has proven to be a major clinical and scientific task in assessing the elderly with and without cognitive disorders, other than AD (Laske et al., 2015). Other clinical pathologies such as depressive symptomatology may also influence the test results (Maeshima et al., 2013). However, there is no research offering normative performance data for the Brazilian elderly in this subtest. Accordingly, this study had three main goals:
- to provide reference normative data for the elderly Brazilian population in the LM subtest;
- to check the impact of age, education, gender, and depressive symptoms on the LM subtest performance; and
- to verify the LM capacity to discriminate the elderly with and without depressive symptoms.
Method
Participants
The sample comprised elderly subjects over 60 years of age, according to the World Health Organization for developing countries (WHO, 2002), and with different cultural and educational backgrounds. The participants were selected from the Family Health Strategy Program, EMISUS-FHSP (Gomes et al., 2013) in Porto Alegre, Brazil. The elderly from FHSP were randomly selected from two neighborhoods in Porto Alegre and they were assessed by neurologists, psychiatrics, psychologists, and nutritionists. Initially, 460 elders were included in the study, and the exclusion criteria were:
- scores suggestive of cognitive decline in the Mini Mental State Examination (adapted by Bertolucci, Brucki, Campacci, & Juliano, 1994), according to the cutoff points suggested by Kochhann, Varela, Lisboa, and Chaves (2010) that are suitable for the elderly population in south Brazil (21 points for illiterate, 22 for 1-5 years in formal education, 23 for 6-11, and 24 for 12 or more years);
- not completing the evaluation battery; and
- self-reported psychiatric or neurologic diagnosis.
Therefore, the final sample included 334 elderly participants between the ages of 60 and 95 years old (M=67.82; SD=6.41), between 0 and 15 years of formal education (M=5.02; SD=3.04): 213 (64%) were women and 121 (36%) were men. As for their civil status, 121 (36%) participants were married, 92 (28%) widowers, 52 (16%) single, 64 (18%) divorced, and 5 (2%) not answered. In the subjective health evaluation, 120 (36%) participants rated excellent/good, 164 (49%) regular, 26 (8%) bad/awful, and 24 (7%) did not answer. Furthermore, 207 (62%) participants were retired and 77 (23%) earned up to one minimum salary, 148 (44%) up to three, 28 (8%) up to six, 5 (3%) up to 10, 1 (1%) more than 10, and 75 (21%) did not answer. In relation to depressive symptoms, 73 (22%) participants had a score =6 on the Geriatric Depression Scale, short form — GDS-15.
Procedures and instruments
Participants were assessed in a session of approximately 90 minutes, and tests was administered according to the following sequence:
1. consent form;
2. sociodemographic and health questionnaire (to investigate age, education, gender, retirement, subjective perception of health, income, marital status, and history of clinical diagnosis);
3. MMSE: a screening test that provides temporo-spatial orientation, registration, attention/calculation, recall, and language measures, whose total score ranges between 0 and 30 points. The cutoff points suggested by Kochhann et al. (2010) are suitable for the elderly in southern Brazil and present sensitivity between 81% and 93% and specificity between 82% and 87%;
4. LM subtest (immediate recall) of WMS-R (Wechsler, 1987);
5. a visual distractor task;
6. LM subtest (delayed recall); and
7. GDS-15 (adapted by Almeida & Almeida, 1999): a scale composed of 15 dichotomous questions ("yes" and "no") concerning the occurrence of depressive symptoms. There are several cutoff points suggested in the literature for the short version, but the adopted values for case/non-case (6/5) present considerable degree of sensitivity (between 80% and 85%) and specificity (between 71% and 78%) for the Brazilian elderly (Pinho, Custódio, Makdisse, & Carvalho, 2010).
The LM subtest consists of two short stories that are read to the participants. In immediate recall, the elderly have to recall details of stories after having listened to them; in the 30-minute delayed recall, once again the elderly have to recall details of the stories. The score comprises the sum of correct information recalled (immediate and delayed), adding up to a score of 25 in both trials. In its original version, the LM subtest has a high level of internal consistency, adequate test-retest reliability coefficients, and evidence of construct, criterion, and discriminant validity (Strauss, Sherman, & Spreen, 2006).
This study was approved by the Research Ethics Committee of PUCRS (protocol no. 10/04967).
Statistical analysis
All data analyses were carried out using the software Statistical Package for the Social Sciences version 22 for Windows. Descriptive analysis comprised means, standard deviations, and absolute and relative frequency. Normality of data distribution was investigated with the Kolmogorov-Smirnov test. Effects of the variables, age, education, gender, and depressive symptoms, on the LM test performance were verified by multiple linear regression analysis (stepwise method). Analysis of error independence was investigated with the Durbin-Watson statistics. Participants without significant depressive symptoms were distributed into groups according to age (60-69 years old, 70-79, and 80+), education (illiterate – with zero years of study, 1-4, 5-8, and 9+), and gender. Student's t test was used for independent samples and analysis of variance (ANOVA) with post hoc Bonferroni (to provide greater control against type I error) to identify differences in the LM subtest performance in groups. Normative data for each group were reported through the means and standard deviations values, and scores related to cutoff point of 1.5 standard deviation below the average {z-score=[(participant score control group average)/control group standard deviation]}. Finally, a stepwise discriminant analysis was carried out following Wilks's method to check the capacity of the LM subtest scores to estimate to which group the participant belongs (presence or absence of depressive symptoms). Normality assumptions and homogeneity of the variances–covariances of each group were tested, respectively, with the Shapiro–Wilk and the M of Box tests. Results were considered statically significant at p ≤.05.
Results
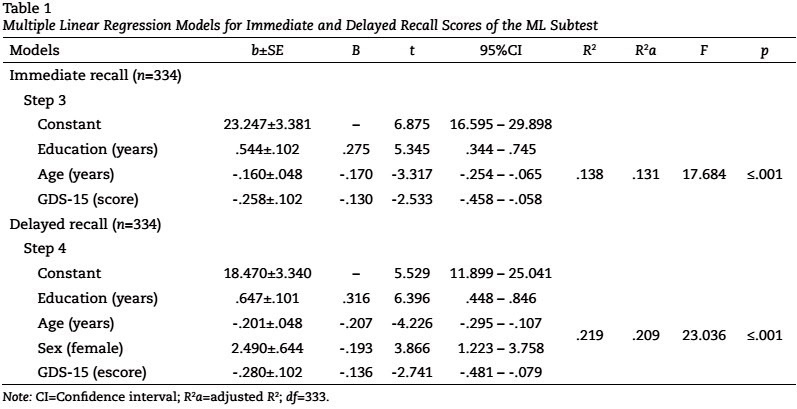
Table 1 presents the results for the explanatory models of multiple linear regression for immediate and delayed recall of the LM subtest. Predictive variables were education, age, gender, and depressive symptoms.
In immediate recall, correlation between significant variables to the model (education, age, and depressive symptoms) was moderate (multiple R=.372). These variables were responsible for 13.80% of the variance of verbal information immediate recall. Results showed that years of formal education were positively related to the immediate recall performance, while age and depressive symptoms correlated negatively. Patterned coefficients of regression showed that education has a higher impact than any other variable on that model (p≤001), followed by age (p≤001) and depressive symptoms (p=.012).
In what concerns delayed recall, all variables had a significant impact on the model, showing a moderate correlation (multiple R=.468), which accounts for 21.90% of the variance in performance. Age and depressive symptoms showed negative correlations, whereas education and female gender showed positive correlations. According to patterned coefficients of regression, it was clear that the variable with the highest impact on delayed recall was education (p≤.001), followed by age (p≤.001), gender (p≤.001), and depressive symptoms (p=.006).
According to the analysis of influence of education, age, gender, and depressive symptoms on the LM test performance, participants were distributed in different normative groups. Table 2 presents the means and standard deviations in immediate recall from three age groups (60-69 years old, 70-79, and 80+), four education groups (illiterate, 1-4 years of education, 5-8, and 9+), gender, and depressive symptoms. It should be highlighted that, as depressive symptoms have an impact on two of the three LM test scores, participants with six points or more on the GDS-15 were not included in groups by age, education, and gender. Normative data for all groups are presented according to average, standard deviation, and z-score.
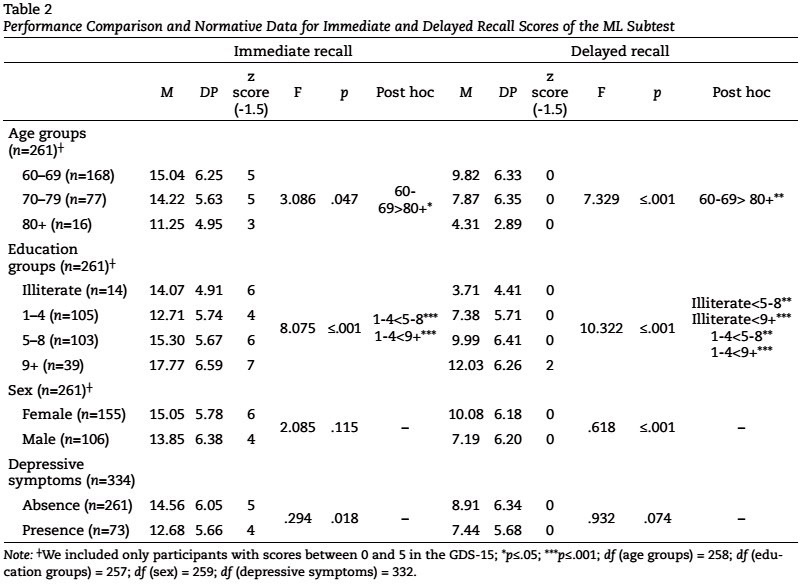
ANOVA demonstrated the impact of age, education, and depressive symptoms on immediate recall scores. The post hoc analysis showed that the age group 60- 69 years obtained significantly higher scores than the 80+ years group in immediate recall, i.e., the younger elderly recalled more details than the older elderly. However, no other significant differences were identified between the remaining age groups. In what concerns education, performance of the 1-4 years of education group was significantly lower than the 5-8 and 9+ groups. This group demonstrated worse scores than the more educated groups, and its results were similar to the illiterate group. Furthermore, participants with depressive symptoms demonstrated worst performance than participants without depressive symptoms. No differences were found between men and women in immediate recall scores.
According to the ANOVA of the delayed recall score (Table 2), post hoc results among age groups showed, once again, that the younger elderly (60–69 years) scored higher than the older elderly (80+ years). There were no other significant differences among the remaining age groups. Conforming to the post hoc for education levels, illiterate and 1-4 years of education groups scored significantly lower than the 5-8 and 9+ groups. Comparisons according to gender showed that women scored higher in delayed recall than men. There were no significant performance differences between groups with and without depressive symptoms. Discriminant analysis with the stepwise method extracted a discriminant function, keeping as statistically significant immediate recall score explaining 100% of the variability between the with and without depressive symptoms groups (Λ=.983; χ2=5.606; p=.041). The percentile of correctly classified participants was 56%.
Discussion
The current study had three main goals. The first one was to provide normative reference data to the Brazilian elderly in the LM subtest of the WMS-R. The second goal was to identify the effects of age, education, gender, and depressive symptoms on the LM subtest performance. Finally, the third goal was to identify immediate and delayed recall scores capacity to identify the elderly with and without depressive symptoms.
Several studies have tried to provide normative data for the elderly in LM subtest throughout different countries (Chapman et al., 2011b; Kawano, Awata, Ijuin, Iwamoto, & Ozaki, 2013); however, there were no normative data performance for the Brazilian elderly. According to studies (Chapman et al., 2011b; Silver et al., 2012), the main variables that have an impact on LM subtest are age, education, and gender.
According to the regression models for immediate and delayed recall scores, results demonstrated that age and education were negatively and positively correlated, respectively, which are according to the literature (Shi et al., 2014). Gender also proved to have an effect on two LM scores, as women scored higher than men. Depressive symptoms correlated negatively with immediate and delayed recall performance. Our results suggested that the older elderly scored significantly lower when compared to the younger age group. According to Cansino (2009), episodic memory is particularly vulnerable to aging, once contextual information or details of the moment/episode are susceptible to be forgotten than the event itself. In the aging process, changes occur both in memory acquisition and in recalling new information (Quevedo, Martins, & Izquierdo, 2006).
The effect of age on the performance of VEM may be associated with the recruitment of several brain regions and neural networks as a result of the aging process, such as the HAROLD (Cabeza, 2002) and PASA models (Davis, Dennis, Daselaar, Fleck, & Cabeza, 2008). While the information processing in young adults shows higher asymmetry between hemispheres, older adults tend to present lower lateralization. Besides, the elderly demonstrate higher activation in the anterior regions of the cerebral cortex when performing cognitive activities, suggesting a functional compensation.
In what concerns VEM, there is a higher involvement of the frontal cortex in recalling information processes. Based on techniques of neuroimaging, performance in immediate and delayed recall in VEM tasks was associated with volume of the right hippocampus and the left dorsolateral prefrontal cortex (Cox et al., 2015). Consequently, the elderly recruit different cerebral areas to efficiently perform memorization steps, showing a compensation effect. The hippocampus can also be activated when correlating recently learnt associations (Shing et al., 2010).
Corroborating these results, Kinugawa et al. (2013), while comparing three different age groups, observed that the decline in VEM increased with age. In assessments with LM, Kawano et al. (2013) identified a negative correlation with age, but not with education or gender. In another example, Silver et al. (2012) observed that the elderly scored low when compared with young in LM. Furthermore, the authors identified a moderate correlation between work memory and verbal memory. Similarly, our results show that the younger elderly achieved better performance in all modalities of the LM subtest compared with the older group (80 years or more).
This study demonstrated that the elderly with lower levels of education (illiterate and 1-4) scored poorly in the LM subtest compared with the higher educational groups. These results are consistent with those of Nitrini (2008), and other studies also showed positive correlations between education and VEM tasks (Gabriel & Conboy, 2010; Messinis et al., 2016). In the study of Angel et al. (2010) four groups were assessed according to age (young and elderly) and education (low and high) in a VEM test. Information recall score was lower in the elderly group, and older participants with lower levels of education obtained the worst accuracy. Furthermore, education acted as a protective factor, preventing decline of mnemonic abilities associated with aging.
Another possible explanation for the poorer performance of less-educated adults in the LM subtest could be the cognitive reserve (Stern, 2012), since the activities performed throughout the life span can contribute to strengthening and establishing new information networks, mainly to solve complex tasks. The level of education seems to increase information association networks in the cerebral cortex, which have an effect on processing speed and effective information acquisition, storage, and recall. The elderly with higher levels of education show a better learning than the less-educated ones and therefore perform better at storing and recalling information (Angel et al., 2010).
The results related to the influence of gender on the LM subtest seem to be contradictory. Chapman, Mapstone, Gardner, et al. (2011) compared the LM performance of male and female elderly with AD and healthy male and female elderly. The authors concluded that female elderly with AD scored lower than male elderly with AD in both immediate and delayed recall. However, the opposite pattern was observed in the healthy group, in which the female elderly scored higher than the male. A discriminant analysis was carried out by the authors, which showed that LM scores best identified AD in women than in men.
It is possible that the different findings related to gender in VEM performance are based on the individual and cultural differences of the samples studied. Once again the cognitive reserve can be a distracting variable when analyzing the role of gender in cognition. In studies focused on the rural population, for example, a higher effect of correlation between gender and education can be identified (Yang et al., 2012). Besides professional activities, medication, sociocultural background, alcohol, and tobacco addictions are not studied. These characteristics, which were not considered in this study, could explain the differences between genders in LM scores.
Depressive symptoms impacted the performance on the LM subtest in both immediate and delayed recall. Furthermore, immediate recall score classified correctly 56% of the participants according to the absence or presence of depressive symptoms. Some studies highlight the effect of depressive symptoms in cognition (Graziane, Beer, Snitz, Chang, & Ganguli, 2016). Depressive symptoms may be correlated to a lower attention level, which directly impacts acquisition and storage of verbal information, and attention level. Qualitative analyses of wordlist tasks showed a difference in performance between subjects with dementia and depressive symptoms, as they showed a higher usage of contextual clues (Strauss et al., 2006).
It is important to highlight that comparison of results of the present study with the results of other studies is a delicate task, as the samples differ according to cultural backgrounds. It is necessary to set normative performance patterns, irrespective of the cognitive construct, consistent with sociocultural reality of the respective country. For example, the distribution of normative groups into age and education levels reflects an adjustment according to sociodemographic characteristics, whereas depression is a confounding factor in the diagnosis of neurodegenerative diseases.
Our main results showed that the LM subtest correlates to age, education, depressive symptoms, and gender. However, subjects with cognitive decline or dementia were not included in this study, and it is necessary to investigate these clinical populations in future research. Another serious limitation was the number of participants in each normative group and, more specifically, the number of participants in some age and education groups was not homogeneous.
Dementia and neurodegenerative diseases are common among older people and represent a problem of public health. Consequently, valid and reliable neuropsychological assessment tasks are required for more accurate diagnoses. Hence, the results of this study are important as they provide normative data for a task that assesses VEM, which is widely used for the cognitive assessment of the elderly in clinical practice and research.
References
Almeida, O. P., & Almeida, S. A. (1999). Confiabilidade da versão brasileira da Escala de Depressão em Geriatria (GDS) versão reduzida. Arquivos de Neuropsiquiatria, 57(2-B), 421-426. doi: 10.1590/S0004-282X1999000300013 [ Links ]
Angel, L., Fay, S., Bouazzaoui, B., Baudouin, A., & Isingrini, M. (2010). Protective role of educational level on episodic memory aging: An event-related potential study. Brain and Cognition, 74(3), 312-323. doi: 10.1016/j.bandc.2010.08.012 [ Links ]
Beck, I. R., Gagneux-Zurbriggen, A., Berres, M., Taylor, K. I., & Monsch, A. U. (2012). Comparison of verbal episodic memory measures: Consortium to Establish a Registry for Alzheimer's Disease Neuropsychological Assessment Battery (CERAD-NAB) versus California Verbal Learning Test (CVLT). Archives of Clinical Neuropsychology, 27(5), 510-519. doi: 10.1093/arclin/acs056 [ Links ]
Bertolucci, P. H. F., Brucki, S. M. D., Campacci, S. R., & Juliano, Y. (1994). O Mini-Exame do Estado Mental em uma população geral: impacto da escolaridade. Arquivos de Neuropsiquiatria, 52(1), 1-7. [ Links ]
Beydoun, M. A., Beydoun, H. A., Gamaldo, A. A., Teel, A., Zonderman, A. B., & Wang, Y. (2014). Epidemiologic studies of modifiable factors associated with cognition and dementia: Systematic review and meta-analysis. BMC Public Health, 14, 643. doi: 10.1186/1471-2458-14-643 [ Links ]
Cabeza, R. (2002). Hemispheric asymmetry reduction in older adults: The HAROLD model. Psychology and Aging, 17(1), 85-100. doi: 10.1037/0882-7974.17.1.85 [ Links ]
Cansino, S. (2009). Episodic memory decay along the adult lifespan: A review of behavioral and neurophysiological evidence. International Journal of Psychophysiological, 71(1), 64-69. doi: 10.1016/j.ijpsycho.2008.07.005 [ Links ]
Celsis, P. (2000). Age-related cognitive decline, mild cognitive impairment or preclinical Alzheimer's disease? Annals of Medicine, 32(1), 6-14. doi: 10.3109/07853890008995904 [ Links ]
Chapman, R. M., Mapstone, M., Gardner, M. N., Sandoval, T. C., McCrary, J. W., Guillily, M. D., et al. (2011b). Women have farther to fall: Gender differences between normal elderly and Alzheimer's disease in verbal memory engender better detection of Alzheimer's disease in women. Journal of International Neuropsychological Society, 17(4), 654-662. doi: 10.1017/S1355617711000452 [ Links ]
Chapman, R. M., Mapstone, M., McCrary, J. W., Gardner, M. N., Porsteinsson, A., Sandoval, T. C., et al. (2011a). Predicting conversion from mild cognitive impairment to Alzheimer's disease using neuropsychological tests and multivariate methods. Journal of Clinical and Experimental Neuropsychology, 33(2), 187-199. doi: 10.1080/13803395.2010.499356 [ Links ]
Correia, F. A., & Osorio, I. C. (2013). The Rey Auditory Verbal Learning Test: Normative data developed for the Venezuelan population. Archives of Clinical Neuropsychology, 29(2), 206-215. doi: 10.1093/arclin/act070 [ Links ]
Cox, S. R., Bastin, M. E., Ferguson, K. J., Allerhand, M., Royle, N. A., Maniega, S. M., et al. (2015). Compensation or inhibitory failure? Testing hypotheses of age-related right frontal lobe involvement in verbal memory ability using structural and diffusion MRI. Cortex, 63C, 4-15. doi: 10.1016/j.cortex.2014.08.001 [ Links ]
Davis, S. W., Dennis, N. A., Daselaar, S. M., Fleck, M. S., & Cabeza, R. (2008). Que PASA? The posterior-anterior shift in aging. Cerebral Cortex, 18(5), 1201-1209. doi: 10.1093/cercor/bhm155 [ Links ]
Foss, M. P., Formigheri, P., & Speciali, J. G. (2009). Heterogeneity of cognitive aging in Brazilian normal elderls. Dementia & Neuropsychologia, 3(4), 344-351. [ Links ]
Gabriel, P., & Conboy, J. (2010). Atenção e memória visual na população idosa: uma associação entre habilidades literárias sob condições de interferência. Cuadernos de Neuropsicología, 4(2), 186-201. [ Links ]
Gomes, I., Nogueira, E. L., Engroff, P., Ely, L. S., Schwanke, C. H. A., De Carli, G. A., et al. (2013). The multidimensional study of the elderly in the family health strategy in Porto Alegre, Brazil (EMI-SUS). Pan American Journal of Aging Research, 1(1), 20-24. [ Links ]
Graziane, J. A., Beer, J. C., Snitz, B. E., Chang, C. C., & Ganguli, M. (2016). Dual trajectories of depression and cognition: A longitudinal population-based study. American Journal of Geriatric and Psychiatry, 24(5), 364-373. doi: 10.1016/j.jagp.2015.08.001 [ Links ]
Higginson, C. I., Arnett, P. A., & Voss, W. D. (2000). The ecological validity of clinical tests of memory and attention in multiple sclerosis. Archives of Clinical Neuropsychology, 15(3), 185-204. doi: 10.1093/arclin/15.3.185 [ Links ]
Kawano, N., Awata, S., Ijuin, M., Iwamoto, K., & Ozaki, N. (2013). Necessity of normative data on the Japanese version of the Wechsler Memory Scale-Revised Logical Memory subtest for old-old people. Geriatrics & Gerontology International, 13(3), 726-730. doi: 10.1111/ggi.12007 [ Links ]
Kinugawa, K., Schumm, S., Pollina, M., Depre, M., Jungbluth, C., Doulazmi, M., et al. (2013). Aging-related episodic memory decline: Are emotions the key? Frontiers in Behavioral Neuroscience, 7, 2. doi: 10.3389/fnbeh.2013.00002 [ Links ]
Kochhann, R., Varela, J. S., Lisboa, C. S. M., & Chaves, M. L. F. (2010). The Mini Mental State Examination: Review of cutoff points adjusted for schooling in a large Southern Brazilian sample. Dementia and Neuropsychologia, 4(1), 35-41. [ Links ]
Koenig, A. M., DeLozier, I. J., Zmuda, M. D., Marron, M. M., Begley, A. E., Anderson, S. J., et al. (2014). Neuropsychological functioning in the acute and remitted states of late-life depression. Journal of Alzheimers Disease, 45(1), 175-85. doi: 10.3233/JAD-148006 [ Links ]
Laske, C., Sohrabi, H. R., Jasielec, M. S., Müller, S., Koehler, N. K., Gräber, S. et al. Dominantly Inherited Alzheimer Network (DIAN) (2015). Diagnostic value of subjective memory complaints assessed with a single item in Dominantly Inherited Alzheimer's Disease: Results of the DIAN Study. BioMed Research International, 2015(4), 1-7. doi: 10.1155/2015/828120 [ Links ]
Lezak, M. D., Howieson, D. B., Bigler, E. D., & Tranel, D. (2012). Neuropsychological Assessment. New York, USA: OXFORD. [ Links ]
Maeshima, H., Baba, H., Nakano, Y., Satomura, E., Namekawa, Y., Takebayashi, N., et al. (2013). Time course for memory dysfunction in early-life and late-life major depression: A longitudinal study from the Juntendo University Mood Disorder Project. Journal of Affective Disorders, 151(1), 66-70. doi: 10.1016/j.jad.2013.05.050 [ Links ]
Merema, M. R., Speelman, C. P., Kaczmarek, E. A., & Foster, J. K. (2012). Age and premorbid intelligence suppress complaint-performance congruency in raw score measures of memory. International Psychogeriatrics, 24(3), 397-405. doi: 10.1017/S1041610211001918 [ Links ]
Messinis, L., Nasios, G., Mougias, A., Politis, A., Zampakis, P., Tsiamaki, E., et al. (2016). Age and education adjusted normative data and discriminative validity for Rey's Auditory Verbal Learning Test in the elderly Greek population. Journal of Clinical and Experimental Neuropsychology, 38(1), 23-39. doi: 10.1080/13803395.2015.1085496 [ Links ]
Nitrini, R. (2008). Immediate recall of short stories depends on educational level. Dementia & Neuropsychologia, 2(4), 310-314. [ Links ]
Pantzar, A., Laukka, E. J., Atti, A. R., Fastbom, J., Fratiglioni, L., & Bäckman, L. (2014). Cognitive deficits in unipolar old-age depression: A population-based study. Psychological Medicine, 44(5), 937-947. doi: 10.1017/S0033291713001736 [ Links ]
Pinho, M. X., Custódio, O., Makdisse, M., & Carvalho, A. C. C. (2010). Confiabilidade e validade da escala de depressão geriátrica em idosos com doença arterial coronariana. Arquivos Brasileiros de Cardiologia, 94(5), 570-579. doi: 10.1590/S0066-782X2010005000032 [ Links ]
Quevedo, J., Martins. M. R., & Izquierdo, I. (2006). Alterações cerebrais e memória. In C. M. C. Bottino, J. Laks, & S. L. Blay (Eds.), Demência e transtornos cognitivos em idosos (pp 3-12). Rio de Janeiro: Guanabara Koogan. [ Links ]
Salthouse, T. A. (2014). Correlates of cognitive change. Journal of Experimental Psychology – General, 143(3), 1026-1048. doi: 10.1037/a0034847 [ Links ]
Shi, J., Wei, M., Tian, J., Snowden, J., Zhang, X., Ni, J., et al. (2014). The Chinese version of story recall: A useful screening tool for mild cognitive impairment and Alzheimer's disease in the elderly. BMC Psychiatry, 14, 71. doi: 10.1186/1471-244X-14-71 [ Links ]
Shing, Y. L., Werkle-Bergner, M., Brehmer, Y., Müller, V., Li, S. C., & Lindenberger, U. (2010). Episodic memory across the lifespan: The contributions of associative and strategic components. Neuroscience and Biobehavioral Reviews, 34(7), 1080-1091. doi: 10.1016/j.neubiorev.2009.11.002 [ Links ]
Silver, H., Goodman, C., & Bilker, W. B. (2012). Impairment in associative memory in healthy aging is distinct from that in other types of episodic memory. Psychiatry Research, 197(1-2), 135-139. doi: 10.1016/j.psychres.2012.01.025 [ Links ]
Stern, Y. (2012). Cognitive reserve in ageing and Alzheimer's disease. Lancet Neurology, 11(11), 1006-1012. doi: 10.1016/S1474-4422(12)70191-6 [ Links ]
Strauss, E., Sherman, E., & Spreen O. (2006). A compendium of neuropsychological tests. New York: Oxford University Press. [ Links ]
Sunderaraman, P., Blumen, H. M., DeMatteo, D., Apa, Z. L., & Cosentino, S. (2013). Task demand influences relationships among sex, clustering strategy, and recall: 16-word versus 9-word list learning tests. Cognitive and Behavioral Neurology, 26(2), 78-84. doi: 10.1097/WNN.0b013e31829de450 [ Links ]
Vlahou, C. H., Kosmidis, M. H., Dardagani, A., Tsotsi, S., Giannakou, M., Giazkoulidou, A., et al. (2013). Development of the Greek Verbal Learning Test: Reliability, construct validity, and normative standards. Archives of Clinical Neuropsychology, 28(1), 52-64. doi: 10.1093/arclin/acs099 [ Links ]
Wechsler, D. (1987). Wechsler Memory Scale – Revised. San Antonio, Texas: Pearson. [ Links ]
Welland, R. J., Lubinski, R., & Higginbotham, D. J. (2002). Discourse comprehension test performance of elders with dementia of the Alzheimer type. Journal of Speech, Language and Hearing Research, 45, 1175-1187. doi: 10.1044/1092-4388(2002/095) [ Links ]
WHO – World Health Organization (2002). Active ageing: A police framework. A contribution of the World Health Organization to the second United Nations World Assembly on Aging. Madrid: WHO. [ Links ]
Yang, L., Unverzagt, F. W., Jin, Y., Hendrie, H. C., Liang, C., Hall, K. S., et al. (2012). Normative data for neuropsychological tests in a rural elderly Chinese cohort. Clinical Neuropsychology, 26(4), 641-653. doi: 10.1080/13854046.2012.666266 [ Links ]
 Correspondence address
Correspondence address
Camila Rosa de Oliveira
Rua Senador Pinheiro, 304, 99070-220
Passo Fundo, RS, Brasil.
E-mail: camila.oliveira@imed.edu.br
received on february, 2016
reviewed on june, 2016
approved on july, 2016
1 Camila Rosa de Oliveira is a Psychologist by Federal University of Rio Grande do Sul (UFRGS). PhD in Biomedical Gerontology by Pontifical Catholic University of Rio Grande do Sul (PUCRS). Master in Psychology (emphasis on human cognition) by PUCRS. Professor of the Postgraduate Program in Psychology at Faculdade Meridional IMED.
2 Margarida Maria Baptista Mendes Pedroso de Lima is a Psychologist by University of Coimbra. PhD in Psychology by University of Coimbra. Master of Science in Education by University of Coimbra.
3 Cristiane Silva Esteves is a Psychologist by PUCRS. PhD in Biomedical Gerontology by PUCRS. Master in Psychology (emphasis in clinical psychology) by PUCRS.
4 Valéria Gonzatti is a Psychologist by Lutheran University of Brazil (ULBRA). Master in Psychology (emphasis in clinical psychology) by PUCRS. Specialist in neuropsychology by UFRGS.
5 Susy Ane Ribeiro Viana is a Psychologist by Centro Universitário do Norte (UNINORTE). Master in Biomedical Gerontology by PUCRS.
6 Tatiana Quarti Irigaray is a Psychologist by UFRGS. Post-doctorate in Psychology by PUCRS. PhD and Master in Biomedical Gerontology by PUCRS. Professor of the Postgraduate Program in Psychology at PUCRS.
7 Irani Iracema de Lima Argimon is a Psychologist by PUCRS. PhD in Psychology by PUCRS. Master in Education by PUCRS. Professor of the Postgraduate Programs in Psychology at PUCRS and Biomedical Gerontology at PUCRS.

