










Servicios Personalizados
Revista

Articulo
 Inglés (pdf)
Inglés (pdf)
 Articulo en XML
Articulo en XML Referencias del artículo
Referencias del artículo
Indicadores
Compartir

 Permalink
PermalinkJournal of Human Growth and Development
versión impresa ISSN 0104-1282versión On-line ISSN 2175-3598
J. Hum. Growth Dev. vol.31 no.1 Marília ene./abr. 2021
https://doi.org/10.36311/jhgd.v31.11066
ORIGINAL ARTICLE
Mortality and hospitalization for liver disease in the Western Amazon from 2008 to 2017
Alex Nunes CalladoI; Italla Maria Pinheiro BezerraII; Luiz Vinícius de Alcantara SousaIII; Luiz Carlos de AbreuI
IPós-Graduação em Ciências da Saúde - Centro Universitário FMABC - São Paulo, Brasil
IIEscola Superior de Ciências da Santa Casa de Misericórdia de Vitória - EMESCAM
IIILaboratório de Delineamento de Estudos e Escrita Cientifica - Centro Universitário FMABC, Santo André, São Paulo - Brasil
ABSTRACT
INTRODUCTION: As liver diseases (LDs) occur as liver damage takes place, their causes are variable and mostly caused by viruses and alcohol intake. The cases of LDs have increased significantly; they are also charged with mortality rates and hospitalizations.
OBJECTIVE: to analyze mortality and hospitalizations due to LDs in the Western Amazon.
METHODS: Ecological study with time series design using secondary data related to deaths and hospital admissions for LDs in the Western Amazon.
RESULTS: The number of cases of mortality due to male diseases is higher in men, considering the period from 2008 to 2017. The study results also show that the affected patients are mostly over 50 and under 20 years old, who are the least likely to die. Regarding hospitalization rates, male patients have the highest number of hospitalizations and are not different from mortality; patients over the age of 50 also represent the largest hospitalization cases.
CONCLUSION: There is a tendency towards stability in cases of mortality and hospitalization due to liver diseases in the Western Amazonia.
Keywords: mortality, hospitalization, disease, incidence.
Authors summary
Why was this study done?
This study was carried out to identify the mortality and hospitalization due to liver diseases, discover its possible causes, and identify health actions that influence the conditions and the improvement of quality of life of individuals in the region studied.
What did the researchers do and find?
A search was performed on secondary databases, referring to the number of deaths and hospitalizations. The investigation revealed a higher incidence in the number of cases in male patients over the age of 50, with a hospitalization rate higher than the mortality rate; besides, the hospitalization and mortality rates showed stability among the years studied.
What do these findings mean?
Creating means and strategies aimed at health promotion and prevention can contribute to the awareness of professionals and the population and guarantee better results in the conditions of prognosis and treatment of patients affected by liver diseases, ensuring the quality of life and lower rates of morbidity and mortality.
INTRODUCTION
The second-largest organ in the human body is the liver, weighing an average of 1500g; this organ has a vital and very complex function for the essential functions. Liver disease (LD) occurs when damage to this organ happens, mostly caused by viruses or alcohol use; the degree of harm suffered significantly influences the affected patient's risk of life1.
The liver is responsible for innumerable biochemical pathways in the production, modification, and use of nutrients and other metabolically essential substances. Hence, LD can significantly impact the nutritional state, regardless of its leading cause; therefore, it is considered one of the diseases with more significant difficulties in treatment2.
Because some patients develop asymptomatic disease until liver compensation, understanding the real numbers of chronic liver disease (CLD) cases may not be reliable3.
Among the most common LDs cases are chronic hepatitis C, alcoholic LD, non-alcoholic steatohepatitis, hepatitis B, autoimmune disease, cholangitis sclerosing, primary biliary cirrhosis, hemochromatosis, and Wilson's disease. These diseases' activity is monitored based on their serum levels of aminotransferases, ensuring the classification of the severity of each4.
With the increase in the incidence of LD, it is estimated that the impacts caused by them will be increasingly more significant since LD directly impacts the quality of life of the population5,6.
Méndez-Sánches (2005)7 says that in 2050, approximately 2 million cases of chronic liver diseases (CLD) will be diagnosed, with alcohol still being the most frequent cause of these diseases, followed by non-alcoholic fatty liver diseases (NAFLD).
Behavioral issues can be great allies in the illness process, as alcohol abuse can lead to its progression. Concerning Alcoholic Liver Diseases (ALD), for example, individuals' alcohol intake is the main factor of its cause, in addition to other environmental and genetic factors, such as age, weight, use of illicit drugs, and other concomitant infections8.
One of the leading causes of LD mortality is NAFLD, becoming one of the primary chronic liver diseases. It happens because the number of obese and insulin-resistant patients has increased significantly, becoming a public health problem9.
Hospitalization rates for LD tend to increase; studies report that this increment will be three times higher in admissions to intensive care units (ICU) and hospitals, which suggests an increase in the incidence of the population10,11.
'The leading causes of hospital admissions are liver cirrhosis, alcoholic liver cirrhosis, and acute and subacute insufficiency, which are more frequent in patients between 40 and 59 years. The primary determinant for these diseases' occurrence is the exacerbated use of alcoholic beverages, most responsible for liver cirrhosis cases, being considered accountable for the increased use of public health services12.
The population's lifestyle can influence the onset of liver disease. Men are the most affected because they consume more alcohol and still have an aggravating factor; they do not usually seek health services frequently, leading to late diagnosis.
Thus, this study contributes to discovering the real reasons for LDs, identifying the mortality and hospitalization rates caused by them. It will also improve the evidence of LDs, providing knowledge for the prevention of new cases and better health conditions for patients.
Therefore, this study aims to assess mortality and hospitalization of liver disease in the Western Amazon from 2008 to 2017.
METHODS
It is an ecological study with a time series design using secondary data on deaths and hospitalizations due to LD in the Western Amazon13,14.
Data were collected by place of residence of deaths and hospitalizations. The unit of analysis selected for this study was the Western Amazon, which comprises the States of Acre, Amazonas, Rondônia, and Roraima, Brazil, with 6 million population15.
Death data correspond to the period from January 2008 to December 2017 (from 1996 onwards, death certificates started to be coded using ICD-10). Hospital admission data from January 1, 2008, to December 31, 2017 (as of 2008, a new table of procedures, medications, orthoses, and prostheses and select materials from the Unified Health System - SUS) was implemented.
All deaths and hospitalizations of public and private hospitals accredited by the Unified Health System during 2008-2017 were considered. According to the 10th Review of the International Classification of Diseases (ICD-10), Hepatic disease was defined using the code used in K70-K77.
Mortality and hospitalization rates were used to construct the results; the population was composed of the number of cases per year (numerators) and people (inhabitants). Rates were also calculated according to gender and age group.
Data collection
The data were extracted from the file transfer service provided by the Department of Informatics of the Unified Health System (DATASUS) (website: www.datasus.gov.br). It started with the systematic recording of mortality data (Vital Statistics - Mortality and Live Births).
With advances in the control of infectious diseases, the health situation analysis started to incorporate other dimensions of health status, including epidemiological information and morbidity. It is worth mentioning that these systems are used to support objective analyzes of the health situation, evidence-based decision-making, and public policies in the country.
Through this official public domain database of health information in the country, we collected data on deaths and hospitalizations due to LDs presented in this study.
Data were consulted through the TABNET, and TABWIN programs. These tabs were developed to perform quick tabs on DBF files. Two independent researchers collected data to identify possible discrepancies.
The Mortality Information System receives, processes, confers consistency, and validity on the primary cause of death recorded in the Death Certificate (DC) and provides information on more than 96% of deaths in Brazil17.
The Hospital Information System of the Unified Health System (SIH/SUS) registered more than 85% of people seeking public and private hospitals registered in the Unified Health System (SUS). It includes 92.3% of health units in Brazil17. We used information corresponding to the patient hospitalization date by place of residence, in this case, in the Western Amazon region.
The population count and demographic censuses carried out between the years 2008-2017, under the coordination of the Brazilian Institute of Geography and Statistics (IBGE), provided information on the number of residents of the Western Amazon, broken down by sex age group. For the inter-census years, estimates made by IBGE were used16.
Mortality and hospitalization rates for the entire Western Amazon region were presented and standardized by age group, using the World Health Organization's world standard population and stratified by age group (less than one year, were excluded), male and female (ignored were removed). For the LD subtypes, only the number of cases were evaluated18.
The mortality study represents a way of understanding the Epidemiology of LD. The data obtained from the Ministry of Health's information systems are reliable, especially in the Western Amazon, where the Information Systems are of good quality and completeness, enabling their use as a feasible tool to assess LD18.
Mortality studies have their limitations when secondary data are analyzed, especially about the validity of identifying the fundamental cause of death. However, it should be noted that the secondary data are official and come from the Ministry of Health. Even containing possible underreporting, they are the data available for elaborating public policies, and as such, they must be considered.
Data analysis
Mortality and hospitalization rates were calculated, stratified by age group, year by year (2008-2017), expressed by 100,000 inhabitants, in a gross and standardized manner.
The organization of the data was through Microsoft Excel 2016 spreadsheets. For trend analysis, methodologies based on the authors Antunes and Cardoso (2015) were used19.
To evaluate the trend of cases of mortality from LD in the period studied, linear and polynomial regression models were used, with the LD mortality rate (dependent variable - Y) and time as the dependent variable (independent variable - X) expressed in the years that make up the study period (2008 to 2017). Thus, the following values were estimated: slope (β) and respective probability (p); determination coefficient (r2). A polynomial regression model was used to analyze the variables of female gender and age group of 50 years or more. Therefore, the values of the slope were not determined. (β)15.
For the trend analysis of cases of hospitalization for LD, a polynomial model was used, with the hospitalization rate (dependent variable - Y) and time (independent variable - X) as a dependent variable. Thus, the following values were estimated: respective probability (p) and determination coefficient (r2).
The trend was also estimated with rates standardized by sex and age group (0 to 19 years, 20 to 49 years, and 50 years or more). Finally, Pearson's correlation was performed, with a 95% confidence level, and the statistical program used was Data Analysis and Statistical Software for Professionals (Stata) version 11.0®.
Ethical and legal aspects of research
The present study involves only the description and analysis of secondary data: population, obtained by the general population census, of deaths, collected from the Mortality Information System. All of these information sources are in the public domain. Additional information that is not freely accessible will not be collected. In particular, no personally identifiable information will be obtained for this study.
RESULTS
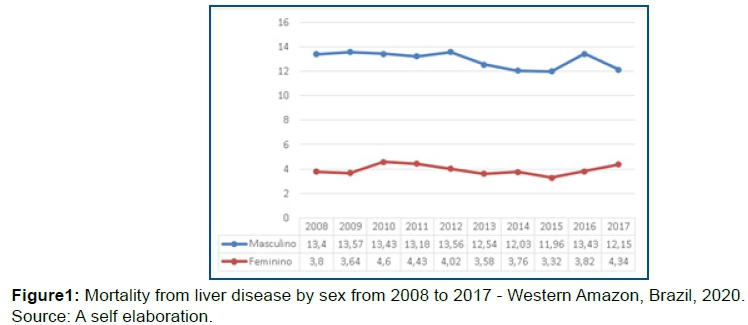
The number of mortality cases due to LDs was higher in males in the period 2008 to 2017 in Western Amazonia (figure 1).
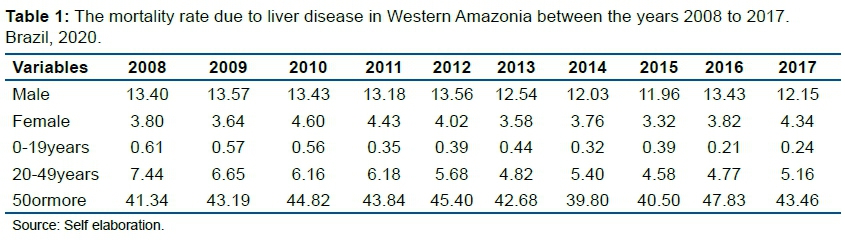
The results show that affected patients are mostly over 50 years, and those under 20 are the least likely to die. There is a stable rate between those years studied, as shown in table 1.
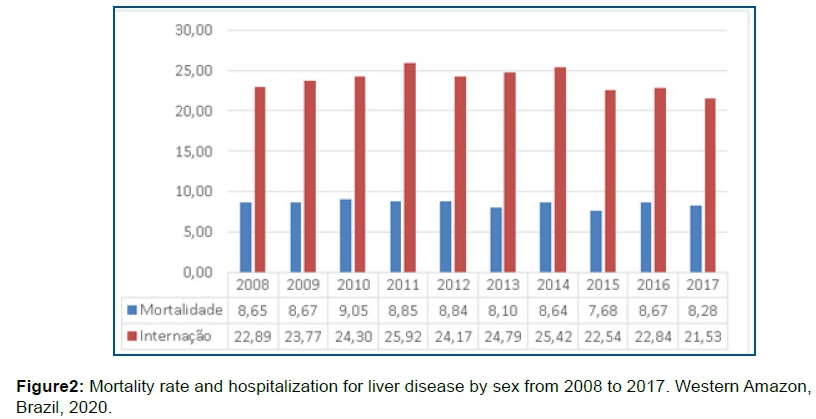
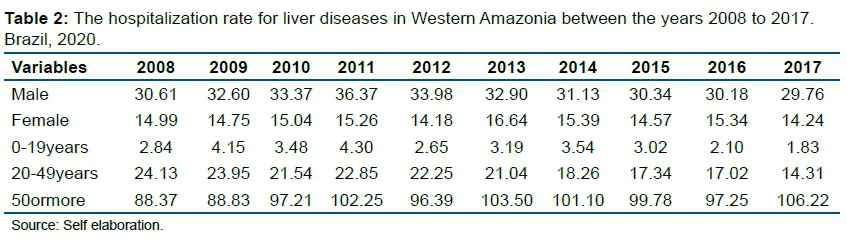
Regarding the hospitalization rate, male patients are responsible for the largest hospitalizations related to LDs. And not unlike mortality, patients older than 50 years also represent the largest hospitalization cases.
Studies have shown that the rate of hospitalization in the Western Amazon is much higher than the rate of mortality from LD, but during the study period it maintained a trend (figure 2).
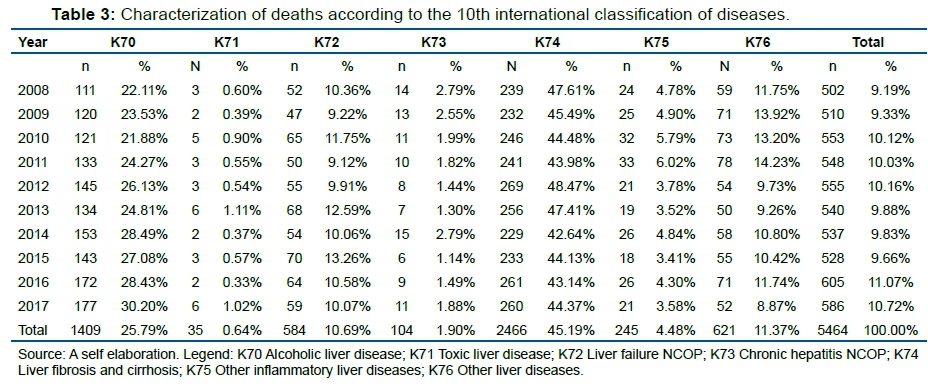
Regarding ICDs, the main cause of deaths was the ICD-K74 Liver fibrosis and cirrhosis, responsible for 2466 (45.19%) of the number of deaths, followed by the ICD-K70. Alcoholic liver disease with 1409 (25.79%). Toxic liver diseases represent the lowest number of cases in the period, with 35 (0.64%) deaths.
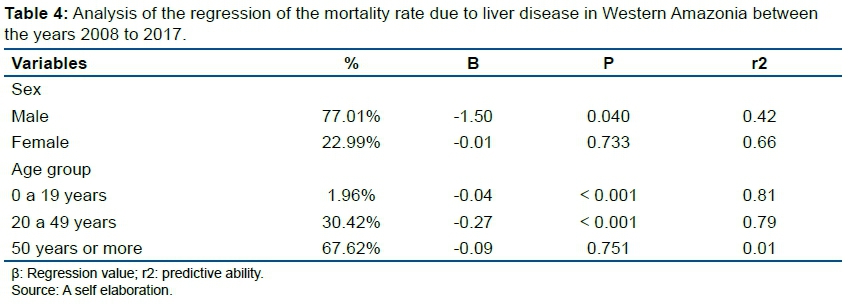
When analyzing the regression from 2008 to 2017, the cases remained stable, with deaths in males representing 77.01% of the cases, and individuals over 50 years of age 67.62%.
The regression analysis showed a trend towards stability in males (β = -1.50). When analyzing the correlation between sex and mortality, a statistical association was identified (p <0.05) (table 2).
The female gender showed an inverse correlation, indicating a reduction (p = 0.733/r = 0.66), in the age group 0 to 19 (p = <0.001/r = 0.81), from 20 to 49 (p = <0.001/r = 0.79) and 50 years or older (p = 0.751/r = 0.01). (table 4).
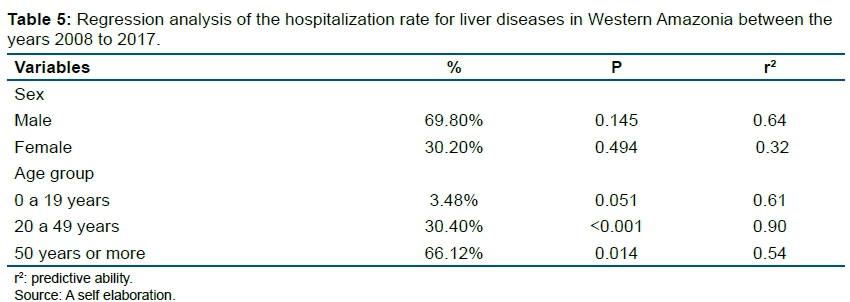
The cases were stable for the hospitalization analysis, with a more significant number of hospitalizations in males, with 69.80% of the cases. Individuals over the age of 50 are those who are most hospitalized.
For hospitalization, the female gender showed an inverse correlation, indicating a reduction (p = 0.145/r0.64), in the age group 0 to 19 years (p = 0.051/r0.61), from 20 to 49 (p = <0.001/r0.90) and for those aged 50 or over (p = 0.014/r0.54) (table 5).
DISCUSSION
The results indicate that between the years 2007 to 2018, the mortality data had a stable rate in the Western Amazon region, with the number of deaths due to LDs higher in the male population and who are older than 50 years.
Hospitalization cases were also higher in male patients over 50 years of age. Besides, it was noted that the numbers of hospitalizations for LDs are higher than the number of deaths, but that they also had a stable trend between the study period.
In both mortality and hospitalization cases, the most common ICDs were the ICD-K74 Liver fibrosis and cirrhosis and the ICD-K70 Alcoholic liver disease, with toxic liver diseases with the least number of patients.
Regarding sex, corroborating the findings, Laurenti, Jorge, and Gotlieb (2005)20, revealed in their study that male mortality is about 50% higher concerning women, reaching up to three times higher in men aged from 20 to 39 years.
A study carried out in São Paulo also showed that the male mortality rate is higher in different causes, whether due to illness or external reasons (violence and accident). In this study, in all major groups, the difference between male and female deaths was considerable, with the most massive difference between the coefficients due to external causes21.
The male mortality coefficient was 711.9 (deaths/100 thousand), while the female mortality coefficient was 526.6. It means that the number of more deaths in men than women is 31 thousand21.
For cirrhosis cases, liver cancer, and disorders due to alcohol use, men's mortality rate was 27.5/100 thousand inhabitants. In comparison, it was 5.4/100 thousand inhabitants; this shows a rate of 5.1 times higher in the male population, corroborating with the present study22.
Regarding diseases, Sala and Mendes (2010)21 pointed out similar results when presenting a big difference in the coefficient concerning mortality from diseases of the digestive system. In this study, the main conditions that caused deaths in the male population were alcoholic liver diseases, fibrosis, and liver cirrhosis, mainly over 30 years.
Corroborating the results, an epidemiological study conducted in Amazonas showed a prevalence of 54.8% of liver cirrhosis cases, occurring more frequently in men than in women, affecting the age group between 20 and 39 years23.
Other research has identified that alcoholic liver disease is responsible for 40% of liver cirrhosis mortality, being considered the leading cause of preventable morbidity and mortality. Furthermore, given the impacts of liver disease, liver cirrhosis is the preeminent cause of hospitalizations and mortality and alcoholic, the second3,24,25.
Melo, et al. (2017)22 had shown that in 2015 in Brazil, the total number of deaths due to cirrhosis, liver cancer, and disorders due to alcohol use was 28,337 deaths. Of these deaths, the highest concentration was in the age group of 50 to 59 years, corroborating with the present study.
Rocha, Marinho, Rodrigues, (2017)26, identified alcoholic LDs and unspecified liver cirrhosis as the main causes of death, being predominantly in male individuals when relating LDs to mortality. The 40 to 65 age group was the most affected by alcoholic LD.
LD is responsible for almost 2 million deaths per year worldwide, making it one of the leading causes of morbidity and mortality27. And although the results show a stable trend over the years in the Western Amazon region, health services must be prepared to act in these cases, especially with risk groups.
Therefore, even with the progress in diagnoses and treatments that has been happening, many people still suffer from liver problems, and many end up dying from complications of cirrhosis, hepatitis, and other liver diseases27,28. For example, liver cirrhosis, when it affects the individual, can have severe consequences, progressing to total liver dysfunction. Therefore it is considered a significant public health problem, as the only solution for these cases is liver transplantation9.
Concerning diseases involving alcohol, the World Health Organization (WHO) attributes a more significant proportion of alcohol-related diseases to men, with many deaths among them. In Brazil, the highest prevalence of excessive alcohol consumption is in the adult male population, almost three times higher than in the female population29.
In several aspects of health, it is clear that there is an elementary differential in terms of male and female mortality; in practically all age groups and causalities, men are still the ones who die the most. Most of these deaths occur due to the digestive system's diseases, one of the main ones being liver cirrhosis, which may or may not be associated with alcoholism20.
The Pan American Health Organization, in its manifestations, recognizes that alcohol is still a great villain for men's health, in addition to other psychoactive substances that help in the prognosis of certain diseases30. And the impact of these substances is being seen in the face of analyzes of mortality and hospital morbidity20.
The care system of the Unified Health System (SUS) follows guidelines for health promotion, prevention, and recovery, with a vast service network for the population. For patients who abuse alcohol, the SUS provides a Psychosocial Care Centers Network, with reception units, therapeutic residency services, and beds in general hospitals31.
This system can contribute to the study's findings because its number of deaths is less than the hospitalizations, indicating that the Western Amazon's health services are equipped to deal with these clinical conditions and put into practice SUS guidelines, ensuring the recovery of the affected population.
If professionals can create health promotion actions and develop new care practices, the results will be satisfactory, which will enable a higher quality of life for these patients. Therefore, it is essential to open the eyes to care practices, visualizing the individual beyond the disease32.
Thus, it is imperative to create means of prevention and health promotion, taking into account behavioral and social indicators and considering each individual's habits and styles, as many diseases will only be controlled when there is awareness about the dangers that some patterns can bring.
Thus, it is crucial to include men in health services, as some diseases are more prevalent in this public, so it is worth adding them to the control mechanisms and daily health practices.
Therefore, it is expected that the results can contribute to the development of services and health professionals, guaranteeing new means for prevention and improvements in patients' health conditions, enabling even better results from the indicators and more remarkable scientific progress on the subject.
Finally, studies on mortality have their limitations when secondary data are analyzed, especially about the validity of identifying the primary cause of death. However, it should be noted that the secondary data are official and come from the Ministry of Health (MS) and even containing possible underreporting, they are the data available for the elaboration of public policies. As such, they must be considered.
CONCLUSION
In the period from 2008 to 2017 in Western Amazonia, there was a tendency towards stability in the rate of mortality and hospitalization for liver diseases, being more frequent in males and the age group above 50 years old.
Acknowledgments
The financial viability of the article is due to the Acre - Health Project in the Western Amazon (multi-institutional agreement process no. 007/2015 SESACRE-UFAC-FMABC).
REFERENCES
1.Ferreira FC, Cunha CJ, Dullius MA, & Souza DN. Procedimentos de cintilografia hepática e aperfeiçoamento de profissionais utilizando objeto simulador antropomórfico de fígado em medicina nuclear. Sociedade Brasileira de ProtecaoRadiologica (SBPR), Recife, PE, 2011. [ Links ]
2.Maio R, Dichi JB, Burini RC. Conseqüências nutricionais das alterações metabólicas dos macronutrientes na doença hepática crônica. Arquivos de Gastroenterologia, 2000. 37(1): 52-57. https://doi.org/10.1590/S0004-28032000000100011 [ Links ]
3.Kim WR, Brown JRS., Terrault, N. A., & El-Serag, H. Burden of liver disease in the United States: summary of a workshop. Hepatology, 2002. 36(1), 227-242. https://doi.org/10.1053/jhep.2002.34734 [ Links ]
4.Mincis M, Mincis R. Enzimas hepáticas: aspectos de interesse prático. Revista Brasileira de Medicina, 2006. 56-60. [ Links ]
5.Lim YS, Kim WR. The global impact of hepatic fibrosis and end-stage liver disease. Clinics in liver disease, 2008. 12(4), 733-746. [ Links ]
6.Davis GL, Alter MJ, El-Serag H, Poynard T, Jennings LW. Aging of hepatitis C virus (HCV) -infected persons in the United States: a multiple cohort model of HCV prevalence and disease progression.Gastroenterology, 2010. 138(2), 513-521. [ Links ]
7.Méndez-Sánchez N, Villa AR, Chávez-Tapia NC, Ponciano-Rodriguez G, Almeda-Valdés P, González D, Uribe M. Trends in liver disease prevalence in Mexico from 2005 to 2050 through mortality data. Annals of Hepatology, 2005. 4(1), 52-55. [ Links ]
8.Mathurin P, Bataller R. Trends in the management and burden of alcoholic liver disease. Journal of hepatology, 2015. 62(1), S38-S46. [ Links ]
9.Veras RDSC, Lima MM, Gonçalves PD, Oliveira HA, Salgado P HC, Torres ALM. Perfil das doenças hepáticas crônicas no ambulatório do Unifeso. Cadernos da Medicina-UNIFESO, 2018. 1(1). [ Links ]
10.Liang W, Chikritzhs T, Pascal R, Binns CW. Mortality rate of alcoholic liver disease and risk of hospitalization for alcoholic liver cirrhosis, alcoholic hepatitis and alcoholic liver failure in Australia between 1993 and 2005. Internal medicine journal, 2011. 41(1a), 34-41. [ Links ]
11.Welch C, Harrison D, Short A, Rowan K. The increasing burden of alcoholic liver disease on United Kingdom critical care units: secondary analysis of a high quality clinical database. Journal of health services research & policy, 2008. 13. [ Links ]
12.Jepsen P, Vilstrup H, Sørensen HT. Alcoholic cirrhosis in Denmark-population-based incidence, prevalence, and hospitalization rates between 1988 and 2005: a descriptive cohort study. BMC gastroenterology,2008. 8(1), 1-7. [ Links ]
13.Silva JLD. Suicídios invisibilizados: investigação dos óbitos de adolescentes com intencionalidade indeterminada (Doctoral dissertation, Universidade de São Paulo). 2017. https://doi.org/10.11606/T.6.2017.tde-20042017-154508 [ Links ]
14.Sousa ALV, Silva Paiva L, Santos Figueiredo FW, do Carmo Almeida TC, Oliveira FR, Adami F. Trends in stroke-related mortality in the ABC region, Sao Paulo, Brazil: an ecological study between 1997 and 2012. The open cardiovascular medicine journal, 2017. 11, 111. [ Links ]
15.Instituto Brasileiro de Geografia e Estatística. Características gerais da população, religião e pessoas com deficiência. Rio de Janeiro, 2010. 1-215, 2010. [ Links ]
16.Zétola VHF, Nóvak EM, Camargo CHF, Carraro JH, Coral P, Muzzio JA, Werneck LC. Stroke in young adults: analysis of 164 patients. Arquivos de neuro-psiquiatria, 2001. 59(3B), 740-745. [ Links ]
17.Ministério da Saúde. Manual de Pericia Medica. II edição. 2004. [ Links ]
18.Ahmad OB, Boschi-Pinto C, Lopez AD, Murray CJ, Lozano R, Inoue M. Age standardization of rates: a new WHO standard. Geneva: World Health Organization, 2001. 9(10). [ Links ]
19.Antunes JLF, Cardoso MRA. Uso da análise de séries temporais em estudos epidemiológicos. Epidemiologia e Serviços de Saúde, 2015. 24, 565-576. [ Links ]
20.Laurenti R, Jorge MHPDM, Gotlieb SLD. Perfil epidemiológico da morbi-mortalidade masculina. Ciência & Saúde Coletiva, 2005. 10, 35-46. [ Links ]
21.Sala A, Mende JDV. Perfil da mortalidade masculina no Estado de São Paulo. BEPA. Boletim Epidemiológico Paulista (Online), 2010. 7(82), 15-25. [ Links ]
22.Melo APS, França EB, Malta DC, Garcia LP, Mooney M, Naghavi M. Mortalidade por cirrose, câncer hepático e transtornos devidos ao uso de álcool: Carga Global de Doenças no Brasil, 1990 e 2015. Revista Brasileira de Epidemiologia, 2017. 20, 61-74. [ Links ]
23.Araújo ARSD, Souza ARMD, Lira EDFD, Novais MAM. Análise quantitativa dos antígenos de superfície do vírus da hepatite B em portadores de hepatite B em associação com vírus da hepatite D no Amazonas. 2019. [ Links ]
24.Abenavoli L, Milic N, Rouabhia S, Addolorato G. Pharmacotherapy of acute alcoholic hepatitis in clinical practice. World Journal of Gastroenterology: WJG, 2014. 20(9), 2159. [ Links ]
25.Nader LA, Mattos AA, Bastos GA. Burden of liver disease in Brazil. Liver International, 2014. 34(6), 844-849. https://doi.org/10.1111/liv.12470 [ Links ]
26.Rocha MC, Marinho RT, Rodrigues T. Mortality associated with hepatobiliary disease in Portugal between 2006 and 2012. GE-Portuguese Journal of Gastroenterology,2018. 25(3), 123-131. [ Links ]
27.Mokdad AA, Lopez AD, Shahraz S, Lozano R, Mokdad AH, Stanaway J, Naghavi M. Liver cirrhosis mortality in 187 countries between 1980 and 2010: a systematic analysis. BMC medicine, 2014. 12(1), 1-24. [ Links ]
28.Blachier M, Leleu H, Peck-Radosavljevic M, Valla DC, Roudot-Thoraval F. The burden of liver disease in Europe: a review of available epidemiological data. Journal of hepatology, 2013. 58(3), 593-608. [ Links ]
29.Garcia LP, Freitas LRSD. Heavy drinking in Brazil: results from the 2013 National Health Survey. Epidemiologia e Serviços de Saúde, 2015. 24, 227-237. https://doi.org/10.5123/S1679-49742015000200005 [ Links ]
30.Las condiciones de saludenlas Américas. Washington, DC (OPS - Publicación Científica 524). 1990. [ Links ]
31.Ministério da Saúde. Saúde mental no SUS: os centros de atenção psicossocial / Ministério da Saúde, Secretaria de Atenção à Saúde, Departamento de Ações Programáticas Estratégicas. - Brasília: Ministério da Saúde, 2004. [ Links ]
32.Bezerra IMP, Sorpreso ICE. Conceitos de saúde e movimentos de promoção da saúde em busca da reorientação de práticas. J Hum Growth Dev, 2016. 26(1), 11-20. [ Links ]
 Correspondence:
Correspondence:
itallamaria@hotmail.com
Manuscript received: October 2020
Manuscript accepted: January 2021
Version of record online: March 2021


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}