










Servicios Personalizados
Revista

Articulo
 Inglés (pdf)
Inglés (pdf)
 Articulo en XML
Articulo en XML Referencias del artículo
Referencias del artículo
Indicadores
Compartir

 Permalink
PermalinkJournal of Human Growth and Development
versión impresa ISSN 0104-1282versión On-line ISSN 2175-3598
J. Hum. Growth Dev. vol.32 no.2 Santo André mayo/ago. 2022
https://doi.org/10.36311/jhgd.v32.13318
ARTIGO ORIGINAL
Vascular accesses for hemodialysis: current situation in the State of Ceará, Brazil
João Kennedy Teixeira LimaI; Sylvia Rannyelle Teixeira LimaII; Antonio Leonel de Lima JúniorIII; Ana Carolina Gonçalves de AbreuIV; João Antônio CorrêaV
IProfessora Maria Nilde Couto Bem Street, apartment 902, 63041-155, Juazeiro do Norte-CE, Brazil. ORCID: 0000-0003-4188-5880; aculdade de Medicina do ABC /Universidade Federal de Campina Grande
IIFaculdade de Medicina de Juazeiro do Norte. ORCID: 0000-0003-3179-3296
IIIFundação Instituto Oswaldo Cruz; ORCID: 0000-0003-1267-2181
IVFaculdade de Medicina do ABC. ORCID: 0000-0002-7618-2109
VFaculdade de Medicina do ABC; ORCID: 0000-0002-3192-3436
ABSTRACT
INTRODUCTION: the ideal access for hemodialysis is represented by arteriovenous fistulas both as initial access and in use and are determinants of health care parameters for chronic renal patients
OBJECTIVE: to evaluate vascular access for hemodialysis
METHODS: this is a cross-sectional study, with a sample of 2513 individuals on hemodialysis in Ceará. Data were collected on age, sex, time of treatment, underlying disease, initial access and access in use. The data were divided into two groups, the interior of the state and the Metropolitan Region of Fortaleza, in the State of Ceará, and compared using the Student's Test (p<0.05
RESULTS: the most common age group was between 19 and 64 years (73%). Men prevailed in both regions, 713 (63%) in the countryside and 792 (57%) in the metropolitan area. The most common cause of Chronic Kidney Disease was Hypertension 306 (27%), followed by Disease of undetermined cause 295 (26%) in the countryside; in the metropolitan region, Diabetes Mellitus 356 (26%) was the main cause, followed by Hypertension and Disease of undetermined cause, each with 344 (25%), p=0.001. In the countryside, 9% started treatment for fistula while in the metropolitan area 12%, p=0.011. 79% of patients in the countryside used fistulas and 81% in the metropolitan area, p=0.156
CONCLUSION: arteriovenous fistulas are more frequent as initial accesses in the metropolitan region than in the interior, but there is an equivalence of fistulas in use in both regions. Catheter is the main initial access route. The evaluation of vascular accesses in Ceará showed that hemodialysis services are able to maintain good parameters of care for patients with chronic kidney disease
Keywords: hemodialysis, double-lumen catheter, vascular access.
Authors summary
Why was this study done?
To understand and characterize the attention to the chronic renal patient in the hemodialysis program in Ceará, especially when relating the early referral and the care with the initial vascular accesses and in use, it is necessary to analyze the vascular accesses.
What did the researchers do and find?
Data was collected from hemodialysis clinics in Ceará by reviewing patients' medical records for their primary data (age, sex, underlying disease) and their vascular accesses (first access and the vascular access in use). We found that the percentage of initial accesses for hemodialysis is in disagreement with the objectives oriented by international normative institutions and that the number of accesses in use was in agreement with the same orientations. However, the results aligned with the world reality; where the patient does not have an early diagnosis of renal disease, nor an early referral to a hemodialysis service to have an arteriovenous fistula made, conditioning that the use of catheters as the first access is very prevalent to start the treatment. We compared two distinct regions, the metropolitan region of Fortaleza and the interior of Ceará. We observed that in the metropolitan region of Fortaleza there are more chances that the patients start dialysis treatment through fistulas compared to those from the interior; however, when the patient is inserted into the hemodialysis services when comparing the use of fistulas and catheters, this difference is no longer observed. This evidenced fact represents good attention and quality of the hemodialysis services in the state of Ceará.
What do these findings mean?
The significance of the potential understanding of the first vascular access for hemodialysis, represents the level of primary and secondary care to the chronic renal patient, the understanding of the disease, the diagnosis, and early referral, the health dynamics for this specific public; as for the evaluation of the accesses in use, it represents the resolution capacity of the specialized services in hemodialysis in the state of Ceará. When comparing the two regions, we identify the divergences between two regions, we identify the need for the implementation of effective public policies, especially in the interior, for patient access to specialized services in Nephrology.
INTRODUÇÃO
Chronic kidney disease (CKD) is an important global public health problem, a true epidemic that burdens society and the world economy1,2. The treatment of advanced CKD, referred to as end-stage chronic kidney disease (ESCKD) requires many financial resources both for both developed and developing countries3.
CKD consists of damage and progressive and irreversible loss of kidney function (glomerular, tubular and endocrine). The definition and classification of CKD has evolved over time, but current guidelines define this condition as impaired kidney function, demonstrated by a glomerular filtration rate less than 60 mL/min per 1.73m2, or markers of kidney damage, or both, of at least three months' duration, regardless of the underlying cause. In its most advanced stage, ESCKD, the kidneys are no longer able to maintain the normality of the patient's internal environment4.
The increase in the number of cases has been reported in the last decade in different sources5, and is related to the aging and demographic transition of the population, as a result of the improvement in life expectancy and the rapid process of urbanization. Diabetes (DM) and arterial hypertension are the main causes, while socioeconomic, racial and gender disparities are also determining factors6-8.
In developed countries, the prevalence is estimated between 10 and 13% in the adult population9. In developing countries, prevalence data are limited and heterogeneous9. In Brazil, estimates of the prevalence of this disease are uncertain, but it is estimated that 122,825 patients were undergoing dialysis in 201610.
The incidence and prevalence of CKD also vary within countries by ethnicity and by social determinants of health, possibly due to epigenetic influence. Many people are asymptomatic or have nonspecific symptoms, such as lethargy, itching, or anorexia. Diagnosis is commonly made after fortuitous findings from screening tests (urine summary and blood tests) or when symptoms become severe11.
The treatment of patients with ESCKD, Renal Replacement Therapy (RRT), is based on hemodialysis (HD), peritoneal dialysis and kidney transplantation programs10,12,13.
HD is the most far-reaching therapy and aims to replace part of the kidney functions, removing toxic substances, excess water and mineral salts from the body, thus establishing a new situation of balance through the blood14.
The main indications for HD are: pericarditis, fluid overload or pulmonary edema refractory to diuretics, malignant hypertension unresponsive to antihypertensive drugs, progressive uremic encephalopathy or neuropathy with confusion, asterixis, myoclonus, seizures, bleeding diathesis attributable to uremia, refractory hyperkalemia, overt uremia and refractory metabolic acidosis15,16.
A vascular access is necessary to perform HD, which can be an aretriovenous fistula (AVF) or a two-lumen central vein catheter (CVC). Accesses can be temporary or permanent. Temporary access can range from several hours (single dialysis) to a few months (while waiting for AVF maturation). Temporary access is established by percutaneous insertion of a double-lumen CVC into a large vein (internal jugular, femoral, or less desirable, subclavian). The construction of a permanent vascular access allows repeated accesses for months to years17.
The ideal access allows a safe approach, provides adequate flow to perform HD and has a low complication rate18. Vascular access for HD in chronic patients should generally be AVFs and CVCs should be avoided17.
Problems regarding treatment planning for patients with renal failure may already occur in the pre-dialysis phase19,20. AVFs should be made at least six months before starting RRT, in stage IV of CKD in which the patient had a creatinine clearance below 30mL/min/1.73m2, as there may be failures, the need for a new manufacturing procedure, as well as the need for time for the AVF maturation to occur, (it usually occurs in a variable period from 4 to 12 weeks)21-24.
Maturation is a series of modifications that allow repeated punctures and the use of compressive dressings after removal of the collecting needle, without, however, obstructing the vein. After making the AVF, anastomosis between the vein and the artery, several phenomena take place, such as the enlargement of the artery and the increase in arterial blood flow. On the venous side, there is also dilation, arterialization, and an overall increase in blood flow through the AVF. Venous arterialization consists of venous parietal thickening caused by the proliferation of smooth muscle cells in the vascular wall, making the vein less susceptible to extrinsic compression25.
The CVCs to HD should be used in emergency situations for a short time or when an AVF is not available. CVCs are associated with venous thrombosis, infection or other complications, make it difficult to obtain new accesses and can, over time, influence the exhaustion of conventional venous accesses, making the acquisition of a new access a technically challenging procedure and increasing morbidity and mortality. Of the patient and, therefore, should be avoided26-29.
The choice of access is so important that it was one of the main causes of hospitalization among patients with chronic kidney disease in the United States, reaching 25% of all hospitalizations in the first year and 11% after the second year of hemodialysis treatment, generating a cost of more than one billion dollars a year13.
The most important nephrology institution in America, called NKF The National Kidney Foundation, through the KDOQI - Kidney Disease Outcomes Quality Initiative, guides that 50% of patients start HD for AVF30-33 and that HD services preserve 65% of patients performing HD by native FAVs34-37.
It is evident that an epidemiological study on vascular access for the reality in Ceará-Brazil is of fundamental importance for surgeons, nephrologists and nurses involved with chronic renal patients.
The objective of this study was to evaluate the quality of care for patients with chronic renal failure through hemodialysis accesses in the state of Ceará, addressing characteristics of the initial vascular access, which is a data of access to health services, and vascular access in use, which is data related to specialized medical care. The results obtained will make it possible to analyze the pre-dialysis care strategy and the quality control of Renal Replacement Therapy services through vascular access and, mainly, to know the reality of the region.
METHODS
This is a cross-sectional study of primary data from patients in an HD program in the state of Ceará carried out between January 2015 and January 2016.
The population consisted of all patients in an HD program in the state of Ceará. Data were collected from 2513 patients, approximately 55.1 and 2% of the estimated patients on HD in the state of Ceará and Brazil, respectively, in 2016. All patients or their guardians who signed the Free and Informed Consent Form were included.
The study took place in 18 HD clinics, nine in the countryside and nine in the Metropolitan Region of Fortaleza (RMF), capital of the state. Another eight clinics were excluded from the study for various reasons. The patients were separated into two distinct groups, those undergoing treatment in the interior and in the RMF.
The variables of age, sex, duration of treatment, underlying disease, initial vascular access and vascular access in use were analyzed. Data collection took place by obtaining the variables from the patients' medical records by medical students and by experienced physicians.
The total number of vascular accesses was evaluated according to their type and location.
Statistics were used to describe and summarize the data set. Absolute and relative values were used. The "t test" was used to compare the main data that are: age group, treatment time interval, underlying disease, frequency of initial and current accesses of patients in HD program. A confidence level of 95% and sampling error of 5% was considered.
The study was approved by the Ethics Committee of Faculdade de Medicina do ABC (Protocol nº 12262613.6.0000.0082).
RESULTS
There were 2513 HD patients in the 18 clinics. Nine clinics were located in the countryside and nine in the RMF, 1128 patients located in the countryside and 1385 in the RMF. According to data from the Brazilian Society of Nephrology (SBN).
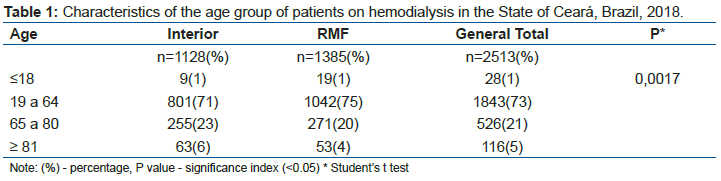
In all clinics, the most common age group was between 19 and 64 years old, productive age group - more than 73% of the sample.
The elderly public represented respectively 29% in the countryside and 24% in the RMF, 26% of the entire sample. There was a predominance of elderly people in the countryside.
And according to the distribution of patients in terms of age (table 1), the sample had a differentiated distribution, so much so that there was a significant difference in the samples between the groups studied (p=0.0017).
More male patients, 60% of the sample, were undergoing dialysis treatment, a fact evidenced in the different areas (table 2). There was a prevalence of men in the countryside, six percent more than in the RMF.
Most patients had less than three years on HD; 364 (32%) patients in the countryside and 441 (32%) patients in the RMF, a total of 805 (32%). All age groups were very homogeneous, with a similar distribution when compared to each other (table 3) (p=0.6275).
It was found that, in the countryside, the cause that most led the patient to HD was hypertension, 306 (27%), followed by Disease of undetermined cause 295 (26%). In the RMF, DM was the most common cause with 356 (26%), followed by Hypertension and Disease of undetermined cause, each with 344 (25%), equally (table 4). Data showed differences in causes between interior and RMF and were significant differences (p>0.001).
Nine percent of the patients in the countryside started dialysis treatment by AVF and approximately 12% by RMF. Low rates of AVFs are evidenced as the initial access in both regions (table 5), but it was also observed that it is more common for the FMR patient to initiate HD through AVF (p=0.011).
Eighty percent of patients were being treated for AVF; 79% in the countryside and 81% in the RMF (table 6). The small difference was not representative (p=0.156).
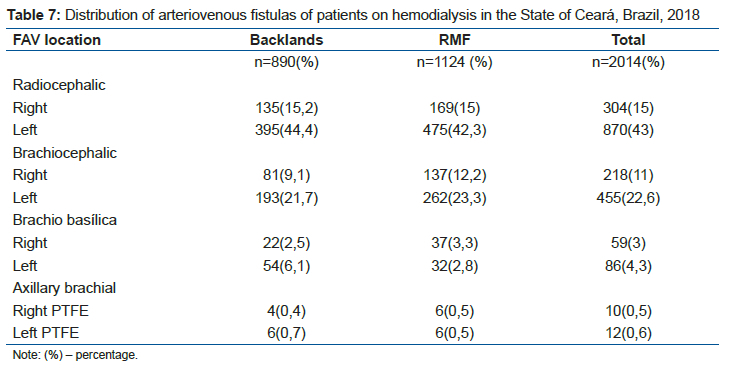
Distal AVFs represented 530 (59.6%) of accesses in the interior against 644 (57.3%) in the RMF. The AVFs with interposition of synthetic material (PTFE-Polytetrafluoroethylene) represented 10 (1.1%) in the interior and 12 (1%) in the RMF (table 7).
There was a predominance of the right jugular vein both in the interior and in the RMF when commenting on CVC accesses and it was greater than 50% in the interior and represented one third of the patients in the RMF. The number of short-term CVCs was more than three times higher than the long-term ones. A greater number of CVCs in subclavian veins was identified in the RMF in Ceará. The number of long-term CVCs was higher in the RMF and represented 27.2%, while in the countryside, 19.4% (table 8).
DISCUSSION
Assessing the quality of care for patients with CKD through vascular access and clinical data of patients on a chronic hemodialysis program in Ceará allows us to know the population undergoing this treatment and infer about some aspects of the reality of pre-dialysis care and assistance specialist doctor offered.
Of the patients who made up the study population, 1843 (73%) were adults (between 18 and 64 years old) and 642 (26%) were elderly (65 years of age or older). An epidemiological census carried out in Brazilian hemodialysis clinics by Sesso in 2016 showed that 65.7% were adults and 33% were elderly10. In this scenario, there were no differences in age when compared to the national scenario exposed by Sesso in which the most patients were formed by young people.
It was identified that there were differences regarding the age group between the interior and the metropolitan region. There was a significantly higher percentage of elderly people in the countryside than in the metropolitan region (p=0.0017). This fact drew attention in the sense that the elderly in the metropolitan region were less ill than those in the countryside, that is, they were better cared for because they lived in an area with likely more accessibility to health services than in the countryside.
The predominance of males in the population studied corroborates the results of other studies of patients with end-stage renal disease undergoing hemodialysis when comparing males and females10,38-40.
For Burelli et al.41, people residing in urban areas seek health services more to perform routine and preventive examinations, while in rural areas the main motivation for seeking care is diseases and in emergency regimes.
Burelli's study41 and the male predominance in dialysis patients may explain the higher percentage of male patients undergoing treatment in the countryside (63%) than in the RMF (57%) (p=0.002) and the national average (57%).
Comparative studies between genders show that men are more vulnerable to diseases, especially serious and chronic illnesses, and that they die earlier than women. In addition, authors point out that, unlike women, men do not seek primary care services and enter the health system at more complex levels of care41.
It is important to consider that, for every three deaths of adults, two are men. They generally live, on average, seven years shorter than women and have more heart disease, cancer, diabetes, higher cholesterol and blood pressure, all risk factors for chronic kidney disease. In this sense, it is essential that health professionals are aware of the general and specific problems that may affect this population and their care demands42-44.
The distribution regarding treatment time was uniform between the two regions in Ceará (p=0.627), the data was measured because with the extension of life expectancy given to these patients by the dialysis treatment itself, the depletion of the venous system of the upper limb could lead to the need to create exceptional vascular accesses and could influence the research results45.
In the context of the search and understanding of the main underlying causes of CKD, which is seen as part of the increase in the global burden of non-communicable diseases and their complications, hypertension (26%) is among the non-communicable diseases and is the most common and affected cause. 27% of interior residents. A similar situation is the understanding that diabetes mellitus was the main cause of renal failure in the metropolitan region of Ceará, also with 26%46,47.
Marinho et al.48, in a systematic review study, observed an advanced industrialization in regions with a higher prevalence of chronic kidney disease, accompanied by an increase in the prevalence of diabetes, hypertension as an underlying disease, a result similar to that observed in Ceará and Brazil by Sesso (2016)10.
Disease of undetermined origin (25%) was the second cause of renal failure in Ceará. There was a high prevalence of cases both in the interior (26%) and in the metropolitan region (25%). Oliveira et al (2011) suggested that most patients do not have access to nephrological monitoring during the early stages of CKD and the absence of renal biopsies may better define cases of diagnosis of undetermined disease39,49.
Rosa-Diez et al.49 attribute the lack of early diagnosis to little exploration of kidney disease data in Latin American countries.
Still taking the parameters of Sesso (2016)10, SAH affects 34% of patients with CKD undergoing dialysis and is the main cause of CKD in Brazil, followed by DM (30%) and of undetermined origin (11%)10. In Ceará, a lower prevalence of SAH (26%) and DM (22%) was found as a cause of ESRD (p<0.001).
The NKF/KDOQI recommends that 50% of patients start hemodialysis through fistulas30-33. In the data collected in Ceará, only 12% of the patients started hemodialysis due to fistulas, 10% in the countryside and 13% in the metropolitan region (p=0.011), far below the desirable.
Despite the two regions maintaining a low rate, it was still shown that patients in the metropolitan region obtained better attention to pre-dialysis care than those in the countryside.
According to data from the United States Renal Data System, 80.3% of patients were using a catheter as the initial access for RRT in 2014, which has changed little since 2005. In 2015, it was reported that 22% of patients started dialysis in America without any specific nephrological follow-up and pre-dialysis care, reason for starting treatment through catheters3.
Despite the KDOQI recommendations, the United States also failed to achieve optimal fistula rates3.
The work of the Fistula First Catheter Last (FFCL) Workgroup Coalition is focused on supporting the community of renal patients and has a current goal that 68% of patients start treatment with fistulas, with at least half in use and the other half awaiting maturation50; goals very different from the reality of Ceará and there is no accurate and current data on the Brazilian reality.
Sesso et al. (2008)10 found that 34% of patients who started hemodialysis used fistulas. The other 66% were referred to the nephrologist to immediately start hemodialysis through a catheter51. The findings in Ceará were lower than the national ones for 2008 and there are not such comprehensive data for comparison.
Silva et al.51, in Minas Gerais (2011), showed that 31% had a fistula as an initial access, data even higher than in Ceará. He also identified that in his sample, if these patients were not diagnosed one year before starting hemodialysis, they would be 3.4 times more likely to start therapy with a temporary catheter.
Not having health insurance increased this probability of starting catheter therapy by almost 1.56 times, and patients living in the northeast were 2.9 times more likely to start hemodialysis through a catheter51.
Silva et al.51 concluded that patients with health plans have more access to start treatment with active fistula due to early referral to the nephrologist and vascular surgeon, and were assisted in 80% of the cases. Patients from the Unified Health System (SUS) sought emergency medical services and started catheter dialysis in dialysis emergency52,53.
The conclusion of the study by Silva et al.51 may be suggested for the population of Ceará due to the high number of admissions to a dialysis program through catheters, that is, the need for immediate vascular access associated with the late diagnosis of end-stage renal disease54,55.
The United Kingdom Renal Registry reports 38.4% admissions through fistulas56; in Australia and New Zealand, 40% and 25%, respectively. Health authorities in Australia and New Zealand consider the results to be inadequate and are aware of the need to improve57. Data still far superior to those of Ceará, whether in the countryside or in the metropolitan region.
Al-Jaishi et al.58, Canada, refer to late referral, health system barriers, long waiting times for appointments in surgical centers as the main causes of initial access to dialysis through catheters.
The NKF-DOQI also recommends that 65% of patients on a regular hemodialysis program undergo treatment through fistulas59. Ceará exceeded the recommendation and 80% of patients are on a dialysis program through fistulas with no differences between the two areas studied (p=0.156).
In this context, it is assumed that most patients start treatment inappropriately through catheters and are led to the creation of a fistula after admission to a service with specialized professionals. Thus, the dialysis services in Ceará are able to maintain a rate above the advisable.
There is a differentiated attention and a concern of the dialysis centers, different from when the patient is unattended by the specialized teams.
Linard et al.13, in a study involving 2559 patients and 23 hemodialysis clinics in Brazil, observed that 93.4% used fistulas. The use of catheters ranged from 0% to 21.7% between clinics. Among the states, it varied from 1.0% in Rio Grande do Sul to 11.3% in Bahia. Among geographic regions, from 3.0% in the South region to 11.1% in the Northeast region.
Sesso et al.10 found that catheters were the access for 20.5% of hemodialysis patients through a dialysis census of the Brazilian Society of Nephrology.
Finally, the results since 2003 were not different from those found in Ceará when compared to the national scenario, but they were different for the southern regions of the country, mainly Rio Grande do Sul.
The variations found can perhaps be explained by the fact that there are structural differences between the units and the profile of patients treated in some clinics, especially hospitals, being patients with acute renal failure, which increases the use of catheters for hemodialysis, as these patients arrive at the unit in dialysis urgency and without a definitive access route13.
Data from 2014 from the United States Renal Data System still had a prevalence of 63.4% of patients with fistulas in use3. It is assumed that there is still better acceptance of fistulas by Brazilians than by Americans, which is the reason for the better rates and that the catheter would be of use almost restricted to waiting periods for a definitive vascular access13.
The DOPPS V-The Dialysis Outcomes and Practice Patterns Study, conducted by America and participating countries, found that the frequency of fistulas ranged from 49% in Canada to 92% in Russia60.
In some countries, the data are conflicting. In India, there was a decrease in patients with fistulas from 92 to 56% between 2003 and 2013, unlike other countries such as Spain and the United States61.
In addition to Russia, a high percentage of fistulas was established in Japan (91%), China (87%), Turkey (83%), Australia and New Zealand (82%), while in most European countries this percentage is less than 80%60.
A report from the ERA-EDTA Registry - European Renal Association - European Dialysis and Transplant Association, pointed out that the percentage of prevalent fistulas decreased from 66 to 62% and the use of catheters increased from 28 to 32%62. In a study in Serbia, the percentage of fistulas in use is 89 to 93%60. The only data similar to Serbia are data from Macedonia, with 89% of patients prevalent with AVF63.
In this context, the rate of fistulas in use in Ceará is higher than that guided by the NKF/DOQI, lower than those found in European and Asian countries. If we make a comparison between economically similar countries, such as India, the state of Ceará-Brazil exceeds the rates of fistulas in use found by Hashidi et al.61 in this country.
In addition to the number of vascular accesses being in accordance with international guidelines and there being no differences between the accesses in use between interior and RMF, it is also reported that the location with the highest prevalence was radiocephalic, above 43% in both regions.
There is no way to define the patency rate of a primary fistula due to the lack and discontinuity of data in Ceará, but the United States Renal Data System's guidance is to make fistulas, preferably the most distal and in the upper extremities whenever possible3.
Also in Ceará, the preference was given to making fistulas in the following sequence whenever possible: primary radiocephalic fistula, primary brachiocephalic elbow, superficialized brachial basilica in the arm, and as a last option, fistulas with graft, inside than expected in the international literature64.
As for the puncture site, there was consistency with the international literature. The preferred insertion site for catheters was the right internal jugular vein, and it was most significantly identified in the interior. Subclavian access was avoided.
The subclavian vein catheter is more associated with central venous stenosis65-67. Significant subclavian vein stenosis usually precludes use of the entire ipsilateral arm for vascular access and may cause vascular insufficiency. Thus, implantation of catheters in this vein should be avoided, even as temporary accesses64.
CONCLUSION
In the final model, there is a deficiency in pre-dialysis care that results in the failure to establish an arteriovenous vascular access for patients with terminal chronic disease in Ceará, whether in the countryside or in the metropolitan region.
Hemodialysis services in Ceará are able to implement an adequate vascular access program after the patient is under specific care.
REFERENCES
1.Hill NR, Fatoba ST, Oke JL, et al. Global Prevalence of Chronic Kidney Disease - A Systematic Review and Meta-Analysis. PLoS One 2016; 11: e0158765. 2016/07/08. DOI: 10.1371/journal.pone.0158765 [ Links ]
2.Lugon JR and Strogoff-de-Matos JP. Comparing costs of renal replacement therapy in a Brazilian city: a case for improvement of our health policies. J Bras Nefrol 2017; 39: 106-107. 2017/10/27. DOI: 10.5935/0101-2800.20170027 [ Links ]
3.Saran R, Robinson B, Abbott KC, et al. US Renal Data System 2016 Annual Data Report: Epidemiology of Kidney Disease in the United States. Am J Kidney Dis 2017; 69: A7-A8. 2017/02/27. DOI: 10.1053/j.ajkd.2016.12.004 [ Links ]
4.Passos VM, Barreto SM, Lima-Costa MF, et al. Detection of renal dysfunction based on serum creatinine levels in a Brazilian community: the Bambui Health and Ageing Study. Braz J Med Biol Res 2003; 36: 393-401. 2003/03/18. [ Links ]
5.Glassock RJ, Warnock DG and Delanaye P. The global burden of chronic kidney disease: estimates, variability and pitfalls. Nat Rev Nephrol 2017; 13: 104-114. 2016/12/13. DOI: 10.1038/nrneph.2016.163 [ Links ]
6.Wheeler DC and Becker GJ. Summary of KDIGO guideline. What do we really know about management of blood pressure in patients with chronic kidney disease? Kidney Int 2013; 83: 377-383. 2013/01/18. DOI: 10.1038/ki.2012.425 [ Links ]
7.Gordon CE, Balk EM, Becker BN, et al. KDOQI US commentary on the KDIGO clinical practice guideline for the prevention, diagnosis, evaluation, and treatment of hepatitis C in CKD. Am J Kidney Dis 2008; 52: 811-825; 2008/10/31. DOI: 10.1053/j.ajkd.2008.08.005 [ Links ]
8.Abboud O, Becker G, Bellorin-Font E, et al. KDIGO clinical practice guidelines on hepatitis C in chronic kidney disease acknowledged by ISN. Nat Clin Pract Nephrol 2008; 4: 648-649. 2008/09/25. DOI: 10.1038/ncpneph0953 [ Links ]
9.Ene-Iordache B, Perico N, Bikbov B, et al. Chronic kidney disease and cardiovascular risk in six regions of the world (ISN-KDDC): a cross-sectional study. Lancet Glob Health 2016; 4: e307-319. 2016/04/23. DOI: 10.1016/S2214-109X (16)00071-1 [ Links ]
10.Sesso RC, Lopes AA, Thome FS, et al. Brazilian Chronic Dialysis Survey 2016. J Bras Nefrol 2017; 39: 261-266. 2017/10/19. DOI: 10.5935/0101-2800.20170049 [ Links ]
11.Webster AC, Nagler EV, Morton RL, et al. Chronic Kidney Disease. Lancet 2017; 389: 1238-1252. 2016/11/27. DOI: 10.1016/S0140-6736(16)32064-5 [ Links ]
12.Lugon JR, Gordan PA, Thome FS, et al. A Web-Based Platform to Collect Data from ESRD Patients Undergoing Dialysis: Methods and Preliminary Results from the Brazilian Dialysis Registry. Int J Nephrol 2018; 2018: 9894754. 2018/04/26. DOI: 10.1155/2018/9894754 [ Links ]
13.Linardi F, Linardi FdF, Bevilacqua JL, et al. Acesso vascular para hemodiálise: avaliação do tipo e local anatômico em 23 unidades de diálise distribuídas em sete estados brasileiros. Revista do Colégio Brasileiro de Cirurgiões 2003; 30: 183-193. [ Links ]
14. Machado GRG PF. Tratamento de diálise em pacientes com Insuficiência Renal Crônica. Cadernos UniFOA 2014; 9. [ Links ]
15.Samtleben W and Blumenstein M. [Indications for and selection of dialysis methods in acute and chronic renal failure including continuous methods]. Internist (Berl) 1999; 40: 3-12. 1999/03/23. [ Links ]
16. Hillebrand GF, Schlosser S, Schneeberger H, et al. No clinical evidence of hyperlipidemia as a risk factor for chronic renal allograft failure. Transplant Proc 1999; 31: 1391-1392. 1999/03/20. [ Links ]
17.Rodriguez JA, Armadans L, Ferrer E, et al. The function of permanent vascular access. Nephrol Dial Transplant 2000; 15: 402-408. 2000/02/29. [ Links ]
18.Centofanti G, Fujii EY, Cavalcante RN, et al. An experience of vascular access for hemodialysis in Brazil. Int Arch Med 2011; 4: 16. 2011/05/17. DOI: 10.1186/1755-7682-4-16 [ Links ]
19. Bonucchi D, D'Amelio A, Capelli G, et al. Management of vascular access for dialysis: an Italian survey. Nephrol Dial Transplant 1999; 14: 2116-2118. 1999/09/17. [ Links ]
20.Bonucchi D, D'Amelio A, Grosoli M, et al. Vascular access for haemodialysis: from surgical procedure to an integrated therapeutic approach. Nephrol Dial Transplant 1998; 13 Suppl 7: 78-81. 1998/12/31. [ Links ]
21. Grapsa E, Pantelias K, Vourliotou A, et al. Factors influencing first vascular access placement in patients starting hemodialysis. Minerva Urol Nefrol 2016; 68: 39-44. 2016/02/10. [ Links ]
22. O'Shaughnessy MM, Montez-Rath ME, Zheng Y, et al. Differences in Initial Hemodialysis Vascular Access Use Among Glomerulonephritis Subtypes in the United States. Am J Kidney Dis 2016; 67: 638-647; 2016/01/18. DOI: 10.1053/j.ajkd.2015.11.019 [ Links ]
23.Rao A, Evans R, Wilkie M, et al. UK Renal Registry 18th Annual Report: Chapter 11 2014 Multisite Dialysis Access Audit in England, Northern Ireland and Wales and 2013 PD One Year Follow-up: National and Centre-specific Analyses. Nephron 2016; 132 Suppl. 1: 253-278. 2016/04/27. DOI: 10.1159/000444825 [ Links ]
24.Bonucchi D, Palmieri L, Arletti S, et al. Vascular access scenario in Italy: evolution and comparison by two surveys (1998-2013). J Vasc Access 2016; 17: 401-404. 2016/07/05. DOI: 10.5301/jva.5000575 [ Links ]
25. Castelbranco O, Soares F and Pinho C. [The role of colour Doppler ultrasound in the creation, maturation and evaluation of arteriovenous fistula for hemodialysis]. Rev Port Cir Cardiotorac Vasc, 2012; 19: 31-36. 2012/01/01. [ Links ]
26.Gunawansa N, Sudusinghe DH and Wijayaratne DR. Hemodialysis Catheter-Related Central Venous Thrombosis: Clinical Approach to Evaluation and Management. Ann Vasc Surg 2018; 51: 298-305. 2018/05/18. DOI: 10.1016/j.avsg.2018.02.033 [ Links ]
27. Besarab A and Pandey R. Catheter management in hemodialysis patients: delivering adequate flow. Clin J Am Soc Nephrol, 2011; 6: 227-234. 2010/12/01. DOI: 10.2215/CJN.04840610 [ Links ]
28. Ramanathan V and Darouiche RO. Prevention and management of hemodialysis catheter infections. Expert Rev Anti Infect Ther, 2012; 10: 1447-1455. 2012/12/21. DOI: 10.1586/eri.12.134 [ Links ]
29. Katneni R and Hedayati SS. Central venous catheter-related bacteremia in chronic hemodialysis patients: epidemiology and evidence-based management. Nat Clin Pract Nephrol 2007; 3: 256-266. 2007/04/26. DOI: 10.1038/ncpneph0447 [ Links ]
30.Wasse H, Kutner N, Zhang R, et al. Association of initial hemodialysis vascular access with patient-reported health status and quality of life. Clin J Am Soc Nephrol 2007; 2: 708-714. 2007/08/21. DOI: 10.2215/CJN.00170107 [ Links ]
31.Arnold WP. Improvement in hemodialysis vascular access outcomes in a dedicated access center. Semin Dial 2000; 13: 359-363. 2000/12/29. [ Links ]
32.III. NKF-K/DOQI Clinical Practice Guidelines for Vascular Access: update 2000. Am J Kidney Dis 2001; 37: S137-181. 2001/03/07. [ Links ]
33.NKF-DOQI clinical practice guidelines for vascular access. National Kidney Foundation-Dialysis Outcomes Quality Initiative. Am J Kidney Dis 1997; 30: S150-191. 1997/10/27. [ Links ]
34. Vascular Access Work G. Clinical practice guidelines for vascular access. Am J Kidney Dis 2006; 48 Suppl 1: S248-273. 2006/07/04. DOI: 10.1053/j.ajkd.2006.04.040 [ Links ]
35.Chin AI, Chang W, Fitzgerald JT, et al. Intra-access blood flow in patients with newly created upper-arm arteriovenous native fistulae for hemodialysis access. American journal of kidney diseases: the official journal of the National Kidney Foundation 2004; 44: 850-858. [ Links ]
36. Goldfarb-Rumyantzev AS, Leypoldt JK, Nelson N, et al. A crossover study of short daily haemodialysis. Nephrology, dialysis, transplantation: official publication of the European Dialysis and Transplant Association - European Renal Association 2006; 21: 166-175. DOI: 10.1093/ndt/gfi116. [ Links ]
37. Mendelssohn DC, Ethier J, Elder SJ, et al. Haemodialysis vascular access problems in Canada: results from the Dialysis Outcomes and Practice Patterns Study (DOPPS II). Nephrology, dialysis, transplantation: official publication of the European Dialysis and Transplant Association - European Renal Association 2006; 21: 721-728. DOI: 10.1093/ndt/gfi281 [ Links ]
38.Kusumoto L, Marques S, Haas VJ, et al. Adultos e idosos em hemodiálise: avaliação da qualidade de vida relacionada à saúde. Acta Paulista de Enfermagem 2008; 21: 152-159. [ Links ]
39.de Oliveira HM, Jr., Formiga FF and Alexandre Cda S. Clinical and epidemiological profile of chronic hemodialysis patients in Joao Pessoa--PB. J Bras Nefrol 2014; 36: 367-374. 2014/10/16. [ Links ]
40. Cherchiglia ML, Machado EL, Szuster DA, et al. Epidemiological profile of patients on renal replacement therapy in Brazil, 2000-2004. Rev Saude Publica 2010; 44: 639-649. 2010/08/03. [ Links ]
41. Burille A and Gerhardt TE. Doenças crônicas, problemas crônicos: encontros e desencontros com os serviços de saúde em itinerários terapêuticos de homens rurais. Saúde e Sociedade 2014; 23: 664-676. [ Links ]
42. de Medeiros AP, de Menezes Mde F and Napoleao AA. [Risk factors and prevention actions in prostate cancer: fundamentals for nursing]. Rev Bras Enferm 2011; 64: 385-388. 2011/07/15. [ Links ]
43.Lima-Costa MF, Matos DL, Camargos VP, et al. Tendências em dez anos das condições de saúde de idosos brasileiros: evidências da Pesquisa Nacional por Amostra de Domicílios (1998, 2003, 2008). Ciência & Saúde Coletiva 2011; 16: 3689-3696. [ Links ]
44. Eurosurveillance editorial t. WHO launches the World Health Statistics 2012. Euro Surveill 2012; 17 2012/05/31. [ Links ]
45.Neves Junior MAd, Petnys A, Melo RC, et al. Acesso vascular para hemodiálise: o que há de novo? Jornal Vascular Brasileiro 2013; 12: 221-225. [ Links ]
46. Malta DC, Bernal RTI, Lima MG, et al. Noncommunicable diseases and the use of health services: analysis of the National Health Survey in Brazil. Revista de Saúde Pública 2017; 51. [ Links ]
47. Malta DC, Stopa SR, Szwarcwald CL, et al. Surveillance and monitoring of major chronic diseases in Brazil - National Health Survey, 2013. Rev Bras Epidemiol 2015; 18 Suppl 2: 3-16. 2016/03/24. DOI: 10.1590/1980-5497201500060002 [ Links ]
48. Marinho AWGB, Penha AdP, Silva MT, et al. Prevalência de doença renal crônica em adultos no Brasil: revisão sistemática da literatura. Cadernos Saúde Coletiva 2017; 25: 379-388. [ Links ]
49. Rosa-Diez G, Gonzalez-Bedat M, Pecoits-Filho R, et al. Renal replacement therapy in Latin American end-stage renal disease. Clin Kidney J 2014; 7: 431-436. 2014/10/29. DOI: 10.1093/ckj/sfu039 [ Links ]
50. Sequeira A, Naljayan M and Vachharajani TJ. Vascular Access Guidelines: Summary, Rationale, and Controversies. Tech Vasc Interv Radiol 2017; 20: 2-8. 2017/03/11. DOI: 10.1053/j.tvir.2016.11.001 [ Links ]
51. Silva GM, Gomes IC, Andrade EI, et al. Permanent vascular access in patients with end-stage renal disease, Brazil. Rev Saude Publica 2011; 45: 241-248. 2011/02/24. [ Links ]
52.Blay SL, Fillenbaum GG, Andreoli SB, et al. Equity of access to outpatient care and hospitalization among older community residents in Brazil. Med Care 2008; 46: 930-937. 2008/08/30. DOI: 10.1097/MLR.0b013e318179254c. [ Links ]
53.Mendoza-Sassi R and Beria JU. Prevalence of having a regular doctor, associated factors, and the effect on health services utilization: a population-based study in Southern Brazil. Cad Saude Publica 2003; 19: 1257-1266. 2003/12/11. [ Links ]
54.Park HS, Lee YH, Kim HW, et al. Usefulness of assisted procedures for arteriovenous fistula maturation without compromising access patency. Hemodial Int 2017; 21: 335-342. 2016/10/08. DOI: 10.1111/hdi.12499. [ Links ]
55. Goel N, Kwon C, Zachariah TP, et al. Vascular access placement in patients with chronic kidney disease Stages 4 and 5 attending an inner city nephrology clinic: a cohort study and survey of providers. BMC Nephrol 2017; 18: 28. 2017/01/18. DOI: 10.1186/s12882-016-0431-3. [ Links ]
56.UK Renal Registry 19th Annual Report (December 2016): Appendix F Additional Data Tables for 2015 new and existing patients. Nephron 2017; 137 Suppl 1: 351-392. 2017/09/21. DOI: 10.1159/000481382. [ Links ]
57. Polkinghorne KR, Chin GK, MacGinley RJ, et al. KHA-CARI Guideline: vascular access - central venous catheters, arteriovenous fistulae and arteriovenous grafts. Nephrology (Carlton) 2013; 18: 701-705. 2013/07/17. DOI: 10.1111/nep.12132. [ Links ]
58. Al-Jaishi AA, Lok CE, Garg AX, et al. Vascular access creation before hemodialysis initiation and use: a population-based cohort study. Clin J Am Soc Nephrol 2015; 10: 418-427. 2015/01/09. DOI: 10.2215/CJN.06220614. [ Links ]
59. Biuckians A, Scott EC, Meier GH, et al. The natural history of autologous fistulas as first-time dialysis access in the KDOQI era. J Vasc Surg 2008; 47: 415-421; discussion 420-411. 2008/02/05. DOI: 10.1016/j.jvs.2007.10.041. [ Links ]
60. Jemcov T and Dimkovic N. Vascular access registry of Serbia: a 4-year experience. Int Urol Nephrol 2017; 49: 319-324. 2016/07/29. DOI: 10.1007/s11255-016-1378-9. [ Links ]
61. Shahidi SH and Soheilipour M. Comparison of vascular access use in hemodialysis patients in Isfahan in 2003 and 2013. Indian J Nephrol 2015; 25: 16-20. 2015/02/17. DOI: 10.4103/0971-4065.134656. [ Links ]
62. Noordzij M, Jager KJ, van der Veer SN, et al. Use of vascular access for haemodialysis in Europe: a report from the ERA-EDTA Registry. Nephrol Dial Transplant 2014; 29: 1956-1964. 2014/07/26. DOI: 10.1093/ndt/gfu253. [ Links ]
63.Jemcov T, Dimkovic N, Jovanovic D, et al. Erratum to: Vascular access registry of Serbia: a 4-year experience. Int Urol Nephrol 2017; 49: 367. 2017/01/26. DOI: 10.1007/s11255-017-1511-4. [ Links ]
64.Navuluri R and Regalado S. The KDOQI 2006 Vascular Access Update and Fistula First Program Synopsis. Seminars in interventional radiology 2009; 26: 122-124. DOI: 10.1055/s-0029-1222455. [ Links ]
65.Barrett N, Spencer S, McIvor J, et al. Subclavian stenosis: a major complication of subclavian dialysis catheters. Nephrology, dialysis, transplantation: official publication of the European Dialysis and Transplant Association - European Renal Association 1988; 3: 423-425. [ Links ]
66. Marx AB, Landmann J and Harder FH. Surgery for vascular access. Current problems in surgery 1990; 27: 1-48. [ Links ]
67.Ponz E, Campistol Plana JM, Almirall J, et al. Mechanism of hemodialysis-associated subclavian vein stenosis. Nephron 1990; 56: 227-228 [ Links ]
 Correspondence:
Correspondence:
João Kennedy Teixeira Lima
drjoaokennedy@gmail.com
Manuscript received: may 2021
Manuscript accepted: november 2021
Version of record online: june 2022


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}