










Servicios Personalizados
Revista

Articulo
 Inglés (pdf)
Inglés (pdf)
 Articulo en XML
Articulo en XML Referencias del artículo
Referencias del artículo
Indicadores
Compartir

 Permalink
PermalinkRevista Psicologia e Saúde
versión On-line ISSN 2177-093X
Rev. Psicol. Saúde vol.10 no.1 Campo Grande enero/abr. 2018
https://doi.org/10.20435/pssa.v9i1.375
10.20435/pssa.v9i1.375 ARTIGOS
Post-Surgery support group for bariatric patients1
Grupo de apoio psicológico pós-operatório para pacientes bariátricos
Grupo de apoyo psicológico postoperatorio para los pacientes bariátricos
Michele Daiane BirckI; Terezinha de Camargo VianaII
IDoctorate in progress in Clinical Psychology and Culture of the University of Brasilia. Psychologist, member of the multidisciplinary team of Dr. Sergio Arruda Clinic, Brasilia, Brazil. Member COESAS of SBCBM, IFSO and ABESO. E-mail: micheledaianepsi@yahoo.com.br
IIDoctor in Sociology, Deputy Professor of Psychology Institute of the University of Brasilia, Brazil. E-mail: tcviana@unb.br
ABSTRACT
In Brazil, due to the increase in the number of people undergoing bariatric surgery, it is essential to develop studies on clinical monitoring, especially in the post-surgical period. In a specialized service, a psychoeducational group intervention was implemented with duration of two hours, totalizing nine meetings with monthly intervals. There was no restriction of gender, operative technique or time elapsed since surgery. The main topics addressed were: alcohol use, anxiety and depression, weight loss and self-esteem, compulsion change, eating disorders, weight regain, body image, social and family support, sexual and affective life. This systematic activity proved to be a protective factor in relation to episodes of sadness, anxiety and impulsive eating behaviors, contributing to the maintenance of healthier behaviors and lifestyles.
Keywords: obesity, support groups, bariatric surgery, psychology, postoperative period
RESUMO
No Brasil, em razão do crescimento do número de pessoas submetidas à cirurgia bariátrica, é indispensável o desenvolvimento de estudos sobre o acompanhamento clínico, notadamente no período pós-cirúrgico. Em um serviço especializado, foi implementada uma intervenção grupal psicoeducativa com duração de duas horas, totalizando nove encontros com intervalo mensal. Não houve restrição de gênero, técnica operatória ou tempo transcorrido desde a cirurgia. As principais temáticas abordadas foram: uso de álcool, ansiedade e depressão, perda de peso e autoestima, troca de compulsões, transtornos alimentares, reganho de peso, imagem corporal, apoio social e familiar, vida sexual e afetiva. Essa atividade sistemática revelou-se como fator protetor em relação a episódios de tristeza, ansiedade e condutas alimentares impulsivas, contribuindo para manutenção de comportamentos e estilos de vida mais saudáveis.
Palavras-chave: obesidade, grupos de apoio, cirurgia bariátrica, psicologia, pós-operatório
RESUMEN
En Brasil, debido al creciente número de personas sometidas a cirugía bariátrica, es esencial para desarrollar estudios sobre el seguimiento clínico, especialmente en el período postoperatorio. En un servicio especializado se llevó a cabo una intervención psicológica y educativa en grupo de dos horas de duración, con un total de nueve reuniones a intervalos mensuales. No hubo restricciones de género, técnica de operación ni tiempo transcurrido desde la cirugía. Los principales temas abordados fueron: alcohol, ansiedad y depresión, pérdida de peso y autoestima, cambio de compulsiones, trastornos de la alimentación, el peso recuperado, imagen corporal, apoyo social y familiar, vida sexual y afectiva. Esta actividad sistemática demostró ser un factor de protección en relación a los episodios de tristeza, la ansiedad y comportamientos alimentarios impulsivos, lo que contribuye a lo mantenimiento de los comportamientos y estilos de vida más saludables.
Palabras clave: obesidad, grupos de apoyo, cirugía bariátrica, psicología, postoperatorio
Introduction
In current contexts, with the prevalence of obesity-friendly environments, the effective treatment of the disease is a major challenge to health teams. The high prevalence of clinical comorbidities associated as well as large functional and psychological consequences that it generates, make obesity a serious health problem that requires intervention of multiprofessional teams. Thus, the treatment of obesity involves a multidisciplinary work and there are few satisfactory results in the long term without major changes in the habits of individual's life, with emphasis on changes in the eating pattern and adoption of physical activities.
For individuals with body mass index (BMI) above or equal to 40, or above or equal to 35 with presence of comorbidities, bariatric surgery has been singled out as the best treatment, considering conditions of weight loss and maintenance (Weineland, Arvidsson, Kakaulidis, & Dahl, 2012), as well as reversing adverse effects of obesity (Tayyem, Ali, Atkinson, & Martin, 2011).
Despite the fact that bariatric surgery has quite satisfactory results regarding life quality of the morbidly obese person, it can also bring some complications in the postoperative period. Among them, we can mention food intolerance, persistent vomiting and nutrient deficiency. Beyond nutritional risks, weight regain is also one of the surgery limitations (Gomes, 2015).
Likewise, bariatric surgery is a procedure that can mislead patients by creating the perception that the temporary weight loss will be permanent. Patients may believe erroneously that the surgical procedure would cure obesity and would bring inherent behavior changes necessary to maintain weight loss and reduce mortality. These facts increase the risk of psychological problems, given the tension that can occur due to "expectations of success" versus "surgical failure". To achieve and maintain the ideal weight loss after bariatric surgery, concomitant lifestyle changes are essentials (Birck, in press). Among the most common recommendations in literature a good postoperative period include nutritional optimization, commitment to regular exercise, stress management, setting realistic goals, strategies for environmental control, life support systems and cognitive restructuring (Thin & cols., 2008).
In this sense, support groups can be an effective option of psychological intervention after bariatric surgery. According to Saunders (2004) and Schopler and Galinsky (1993), support groups aim to help people to cope with stress related to crisis situations, life transitions and stages of economic hardship. In addition, it aim to join people with similar problems, willing to share their personal experiences and to engage in the development of a cohesive and supportive process.
As a recognized psychological assistance technique, the group approach adjust with the current paradigms in health and education, placing the person in the center of his/her learning process, as subject and protagonist in the promotion of health, the construction of knowledge and the senses that give meaning to human experience (Pereira, 2013; Soares & Ferraz, 2007).
The Support Group Purpose
The psychological support group in post bariatric surgery has been offered to patients after gastric bypass in an obesity specialized and bariatric surgery clinic in Brasilia/DF. It was conceived from demands of the operated patients to get opportunities for exchanging experiences. His approach is psychoeducational (Griffiths, 2006) and its purpose is to work with emotional issues arising from the surgical process and slimming, to recognize the inner resources of each patient, to share experiences among the members as well as to provide technical information.
According to Griffiths (2006), the psychoeducation is a therapeutic approach that focuses on setting goals, teaching skills, satisfaction and goals achievement. It focuses on increasing the patient's compliance, on early identification of clinical signs that indicate there is a disease, on the importance of a good lifestyle, exploring beliefs in individual health and awareness of the disease. It allows the patient to understand a little more the complex relationship between symptoms, personality, interpersonal environment and side effects of the medication. The author adds that in group interactions participants have the opportunity to express and validate their concerns and issues, show positive models of health and behavior as well as feel part of a tight-knit group that faces similar difficulties.
The clinic where the work is performed has a multidisciplinary team from which the first author, who is a psychologist, developed this project driven academically by the second author. The group meets monthly, guided by a psychologist, open for patients operated of bariatric surgery without delimitation of surgical time, gender restriction or surgical technique. The invitation to participate is done through social networks, during appointments with the professionals of the team, by email and by telephone.
The subjects covered in the group meetings are chosen from the clinical and academic experience of the authors, as well as based on suggestions from researchers in health and other reference centers in bariatric surgery in Brazil (Benedetti, 2009; Duarte, 2012; Franques, 2009; Mensorio, 2013).
The Experience of the Support Group
The group is structured in nine annual meetings to discuss issues related to post-operative bariatric surgery (table 1). Due to school and work vacation of both health professionals and patients, in July, December and January the meetings have not been done. The meetings have the duration of two hours, and at the end of each meeting new participants are invited to anonymously evaluate the work and provide suggestions for the next group meetings so that they are constantly being improved. In order to ensure the right of privacy, the clinic does not disclose the identity of the participants.
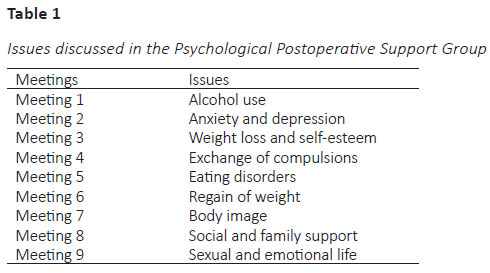
Below we show the main contents that have been discussed in each meeting.
Meeting one - Alcohol Use. A research developed by the Medical Center of the University of Pittsburgh in the United States showed that people undergoing bariatric surgery have a higher risk of becoming alcohol addicted. The beverage is metabolized differently in the body, one feels drunk faster and takes longer to return to sobriety (King et al., 2012). In the postoperative, there is greater risk of exposure to alcohol because social life tends to be more intense. On the other hand, there is the lonely consumption of alcohol in an effort to relax or to forget loneliness because of boredom. Special attention should be given to patients with prior report of consumption or abuse of alcohol and those patients with family report of alcohol or other drugs.
Meeting two - Anxiety and Depression. An interesting question regarding depression in patients eligible for bariatric surgery is that most patients seem to be depressed because of their weight and limitations related to it. In addition, when they take an active role in changing their lives through surgery, depression presents a visible decrease (Hout, Verschure, & Heck, 2005). If depression increases in the postoperative, it is likely that other factors are related to sadness, such as conflicts that begin to appear and mourning the loss of the primordial relationship with food. Studies show that bariatric surgery can lead to a significant reduction in depression and anxiety (Tae et al., 2014). If anxiety increases in the postoperative, it is likely that the rapid weight loss could have aroused hidden issues of obesity that were possibly still unexploited.
Meeting three - Weight Loss and Self-Esteem. An analysis of the literature seems to suggest that bariatric surgery improves self-esteem, self-confidence and expressiveness of the patients. These changes seem to be correlated to significant improvement in body image and weight loss satisfaction after surgery. However, residual dissatisfaction with body image due to the increasement and/or sagging skin has been reported as high and it is worrying (Kubik, Gill, Laffin, & Karmali, 2013).
Meeting four - Exchange of Compulsions. The simple elimination of a symptom (food) through bariatric surgery without proper psychological work can lead the patient to a non-conscious choice of a new symptom to decrease the tension of the psychic apparatus. The person does not know what has been lost, there is no representation and therefore the tension cannot be eliminated through a secondary process. While the network representations are not made, the patient would continue to seek for an escape of this excess by a compulsive act (Ribeiro & Cremasco, 2014). We alert patients to a possible occurrence of other compulsive symptoms, such as to games (bingo, cards), compulsive shopping, abuse of drugs (especially alcohol), and excessive use of internet or video games and compulsive sex.
Meeting five - Eating Disorders. While longitudinal researches are needed to determine whether eating disorder is a cause, a correlation or a consequence of the worst weight loss results after surgery, studies suggest that eating disorders can be the worst prognosis and a suitable target for post-surgery intervention (Kalarchian et al., 2002). We warn patients to pay attention to the emotional triggers that have led them to eat inappropriately, and how much they are still present in the postoperative period.
Meeting six - Weight Recurrence. Behavioral factors that are more emphasized in the literature as those responsible for the recurrence of weight are related to excessive alcohol consumption, grazing, a sedentary lifestyle, a preference for mushy food, excessive consumption of sweet, and as a more common phenomenon in patients who do not participate in multidisciplinary counseling over the postoperative period (Odom et al., 2010). Regarding cognitive factors, studies show the prevalence of self-destructive beliefs (Moorehead, 2011). Incipient researches suggest as morbid obesity features: compulsion to food similar to the characteristics of drug addiction, worrying incidence of child sexual abuse in this population (Moorehead, 2011), immature affective regulation (Kiesewetter et al., 2010), dysfunctional dynamic family, suppressed aggression and hostility (Otto & Ribeiro, 2012), in addition to obesity understood as a defense mechanism (Faden, Leonard, O'Reardon, & Hanson, 2013). But studies are necessary that can investigate the presence or absence of these factors also in weight regain.
Meeting seven - Body Image. The dissatisfaction with body image, commonly perceived in obese patients, is strongly correlated with symptoms of depression, and this is particularly true for women, given the greater political control over their bodies (Kubik, Gill, Laffin, & Karmali, 2013; Wolf, 1992). The dissatisfaction related to weight, which can lead to a negative body image comes from a cultural emphasis in thinness and social stigma of obesity. Most studies about body image is focused in reflection about dissatisfaction, depreciation and distorted body image, under the influence of sociocultural factors (Castro, Carvalho, Ferreira, & Ferreira, 2010).
Meeting eight - Social and Family Support. Regarding obesity, studies claim that interventions based on family participation as well as the presence of a person providing social support, among other variables, facilitate weight reduction and maintenance of weight loss. Social support, especially members of the family core, has been considered a strong predictor of adherence to health treatment (Abreu-Rodrigues, 2014). We alert patients and their families that there may be families that overly protect the patient of external overload and do not give them conditions to overcome frustrations; there are other families that may overload the patient and any carelessness in nutritional education is considered as a crime, a sin. The two familiar ways of working may spoil post-surgical results.
Meeting nine - Sexual and Emotional Life. Obesity has been associated with changes in sexual function and undesirable changes in reproductive hormones in women. A recent study found that women who have undergone bariatric surgery had significant improvement in overall sexual functioning, the main reproductive hormones and psychosocial status (Sarwer et al., 2014). In men, excess abdominal fat, cardiovascular disease, elevated blood lipids and type 2 diabetes have been associated with erectile dysfunction. Obese women report more sexual impairment than obese men. However, this complaint may be more related to low self-esteem, unsatisfactory relationships, social stigma, and other psychological problems.
Results and Discussion
The project of psychological support group for operated patients began to be prepared along the doctorate of the first author (Birck, in press). The organization and execution of the groups have followed some Brazilian guidelines, which are highlighted below.
Officially, the presence of a psychologist in bariatric surgery teams in Brazil was established by a resolution of the Federal Council of Medicine (CFM) under the number 1.766, published in the Government Official Newspaper of July, 11th 2005, amended by CFM Resolution nº 1942/2010, that indicates that the team needs to be able to monitor or to take care of the patient in the pre and trans-operative periods. Moreover, it should be composed of: a surgeon with specific training, an endocrinologist, a nutritional doctor or nutritionist, a psychiatrist or psychologist (CFM, 2010).
Regarding the psychological assessment before bariatric surgery and the respective postoperative follow-up, the lack of agreement on the psychologist role has been worrying. However, in 2014, in an attempt to change this panorama, it was published by SBCBM the first protocol of psychological care in bariatric surgery. The preparation of the protocol counted on the participation of 13 psychologists of the COESAS (Commission of Associated Specialties) of SBCBM. Among the recommendations is that the psychologist who works in the area must have been registered for at least two years in the Regional Council of Psychology and must have the title of specialist in clinical psychology and/or hospital psychology and technical-scientific consistent and updated background in psychology, obesity, eating disorders and Bariatric and Metabolic Surgery (SBCBM, 2014).
In the same protocol, in relation to the main goals of psychological care provided in the postoperative phase and follow-up, it is advised to: (1) increase the self-knowledge of the patient and family to facilitate understanding and adaptation before the changes caused and required by surgery (habits, body image); (2) stimulate self-care, motivation and adherence to treatment and the guidelines of the team; (3) assess the evolution of the adaptation to a new lifestyle (prevention of nutritional deficiencies and weight regain); (4) assist the patient in restarting or developing life projects after surgery; and (5) facilitate the management of daily stressors and the search for life quality. In addition, as main psychology methodologies and interventions, it is suggested: (1) individual and group psychological monitoring; (2) psychoeducation - guidelines and general information about the postoperative period; (3) family counselling; and (4) psychotherapy.
For this study, it was found few Brazilian scientific works about psychological support groups offered to the bariatric patients. It is likely that this panorama is due to a counseling practice preferably within the individual classical model of psychological and clinical care, especially for the newness of bariatric surgery in Brazil.
Regarding the positive aspects of the group reported by patients, we can highlight: (1) exchange of experiences and ideas among patients; (2) psychoeducative approach of the meetings; (3) the spontaneity of the participants; (4) the relevance of the topics covered; (5) verification of common points; (6) the establishment of new individual and group goals; (7) the elaboration of objectives; (8) the problem identification; (9) and self-evaluation. It is noticed that patients created friendships that have been held over time, as well as greater empowerment of patients, mutual support, as well as the autonomy to create other forms of meetings and exchange between them.
Regarding the suggestions for next meetings, patients have requested the participation of other specialties in the team. In a casual meeting the group can count on the participation of a physical educator. This request invites us to think about how each member of the multidisciplinary team is important to address the doubts, concerns and orient patients, and makes us boost future projects. Formally, the reported critic was related to the day of the meetings (Saturdays morning) and, informally, difficulties of some patients in group relationship.
On average, the meetings have counted with the presence of six patients, (minimum 2, maximum 12). It is avoided to set the dates in long holidays, commemorative dates, and participation has been satisfactory. The group began its fourth consecutive year of meetings.
Conclusion
It was demonstrated that, above all, working with group has been shown to be a protective factor for a series of emotional problems emerging in the postoperative period, among them: episodes of sadness and anxiety, as well as impulsive food behaviors. In addition, the group instructional and periodic characteristic has helped in maintaining behaviors and healthier lifestyles. The fact that the patients experience situations similar to their peers make them feel understood. In addition, continuous patients' participation in the group indicates a continuous movement of self-evaluation, self-monitoring and self-care.
However, one of the major limitations of this study is that there is no comparison with the control group, in order to objectively measure how much psychological group support improves the emotional indicators of participants. This work is limited to one report and initial analysis of experiencing psychological group intervention to patients on the postoperative of bariatric surgery.
Furthermore, with regard to future developments, the format of the groups is being reviewed from the demand of participants and the psychologist (the one who coordinates the group) perception. Still on a trial basis, the groups are being offered every month and there is no preset themes for the meetings. That is, the themes that have emerged in the psychological support groups have been spontaneous and related to post-op bariatric surgery. We consider a constant challenge a greater adherence to postoperative psychological service.
Competing Interests
The authors have no competing interests to declare.
Acknowledgments
The authors would like to acknowledge the University of Brasilia and the multidisciplinary team of Dr. Sergio Arruda Clinic.
References
Abreu-Rodrigues, M. A. (2014). Apoio social e reganho de peso pós cirurgia bariátrica: Efeitos de intervenção comportamental com cuidadores (Doctoral thesis, Universidade de Brasília, Brasília, DF, Brasil). [not published].
Benedetti, C. (2009). Preparo psicológico em grupo para cirurgia da obesidade. In E. Ximenes, E. (Org.). Cirurgia da obesidade: Um enfoque psicológico (pp. 79-89). São Paulo: Editora Santos. [ Links ]
Birck, M. D. (in press). Uma compreensão psicológica do reganho de peso após a cirurgia bariátrica (Doctoral thesis, Universidade de Brasília, DF, Brasil). [not published].
Castro, M. R., Carvalho R. S., Ferreira V. N., Ferreira M. E. C. (2010). Função e imagem corporal: Uma análise a partir do discurso de mulheres submetidas à cirurgia bariátrica. Revista Brasileira da Ciência e do Esporte, 32, 167-183. [ Links ]
Conselho Federal de Medicina. (2010). Resolução nº 1.942/2010. Estabelece normas seguras para o tratamento cirúrgico da obesidade mórbida, definindo indicações, procedimentos e equipe. Brasília: CFM. [ Links ]
Duarte, A. N. (2012). Avaliação de grupo de educação nutricional para mulheres com excesso de peso. (Masters Dissertation, Universidade de Brasília, DF, Brasil). [not published].
Faden, J., Leonard, D., O´Reardon, J., & Hanson, R. (2013). Obesity as a defense mechanism. International Journal of Surgery Case Reports, 4,127-129. [ Links ]
Franques, A. R. M. (2009). Adesão ao tratamento pós-operatório: Por que é tão difícil? In E. Ximenes (Org.). Cirurgia da obesidade: Um enfoque psicológico (pp. 99-107). São Paulo: Editora Santos. [ Links ]
Gomes, D. L. (2015). Efeitos metabólicos e nutricionais da suplementação proteica em mulheres com reganho de peso após 24 meses de cirurgia bariátrica: Um ensaio clínico randomizado (Doctoral thesis, Universidade de Brasília, DF, Brasil). [not published].
Griffiths, C. A. (2006). The theories, mechanisms, benefits, and practical delivery of psychosocial educational interventions for people with mental health disorders. International Journal of Psychosocial Rehabilitation, 11,21-28. [ Links ]
Hout, G. C, M., Verschure, S. K. M, & Heck, G. L. (2005). Psychosocial predictors of success following bariatric surgery. Obesity Surgery, 15, 552-560. [ Links ]
Kalarchian, M. A., Marcus, M. D., Wilson, G. T., Labouvie, E. W., Brolin, R. E., & LaMarca, L. B. (2002). Binge eating among gastric bypass patients at long-term follow-up. Obesity Surgery, 12,270-275. [ Links ]
Kiesewetter, S., Köpsel, A., Köpp, W., Kallenbach-Dermutz, B., Pfeiffer, A. F. H., Spranger, J., & Deter, H. C. (2010). Psychodynamic mechanism and weight reduction in obesity group therapy - First observations with different attachment styles. GMS Psycho-Social-Medicine, 7, 1-9. [ Links ]
Kubik, J. F., Gill, R. S., Laffin, M., & Karmali, S. (2013, March 28). The impact of bariatric surgery on psychological health. Journal of Obesity, pp. 1-5. [ Links ]
King, W. C., Chen, J. Y., Mitchell, J. E., Kalarchian, M. A., Steffen, K. J., Engel, S. G., ... Yanovski, S. Z. (2012). Prevalence of alcohol use disorders before and after bariatric surgery. JAMA, 307(23),2516-2524. [ Links ]
Magro, D. O., Geloneze, B., Delfini, R., Pareja, B. C., Callejas, F., & Pareja, J. C. (2008). Long-term weight regain after gastric bypass: A 5-year prospective study. Obesity Surgery, 18,648-651. [ Links ]
Mensorio, M. S. (2013). Análise de estratégias de enfrentamento, ansiedade e hábitos em pacientes elegíveis à cirurgia bariátrica, com e sem acompanhamento psicológico (Masters Dissertation, Universidade de Brasília, DF, Brasil). [not published].
Moorehead, M. K. (2011). A cirurgia bariátrica é uma cirurgia comportamental e um milagre terrestre: perspectiva de uma psicóloga clínica. In A. R. M. Franques, & M. S. Arenales-Loli (Org.). Novos corpos, novas realidades: Reflexões sobre o pós-operatório da cirurgia da obesidade (pp. 171-207). São Paulo: Vetor. [ Links ]
Odom, J., Zalesin, K. C., Washington, T. L., Miller, W. W., Hakmeh, B., Zaremba D. L., ... McCullough, P. A. (2010). Behavioral predictors of weight regain after bariatric surgery. Obesity Surgery, 20,349-356. [ Links ]
Otto, A. F. N., & Ribeiro, M. A. (2012). Unidos em torno da mesa: a dinâmica familiar na obesidade. Estudos de Psicologia, 17(2),255-263. [ Links ]
Pereira, T. T. S. O. (2013). Pichon-Rivière, a dialética e os grupos operativos: implicações para a pesquisa e intervenção. Revista da SPAGESP, 14, 21-29. [ Links ]
Ribeiro, C. C. & Cremasco, M. V. F. (2014) Quando a cirurgia falha: as implicações da melancolia no tratamento cirúrgico da obesidade. [ Links ] Proceedings of the VI International Congress of Fundamental Psychopathology and XII Brazilian Congress of Fundamental Psychopathology, Belo Horizonte, Minas Gerais, Brasil.
Sarwer, D. B., Spitzer, J. C., Wadden, T. A., Mitchell, J. E., Lancaster, K., Courcoulas, A., ... Christian, N. J. (2014). Changes in sexual functioning and sex hormone levels in women following bariatric surgery. JAMA, 149(1),26-33. [ Links ]
Saunders, R. (2004). Post-surgery group therapy for gastric bypass patients. Obesity Surgery, 14,1128-1131. [ Links ]
Schopler, J. H., & Galinsky, M. J. (1993). Support groups as open systems: A model for practice and research. Health & Social Work, 18,195-207. [ Links ]
Soares, S. M., & Ferraz, A. F. (2007). Grupos operativos de aprendizagem nos serviços de saúde: sistematização de fundamentos e metodologias. Escola Anna Nery Revista de Enfermagem, 11, 52-57. [ Links ]
Sociedade Brasileira de Cirurgia Bariátrica e Metabólica. (2014). Especialistas da SBCBM lançam consenso clínico inédito na área de psicologia. Retrieved from http://www.sbcbm.org.br/wordpress/especialistas-da-sbcbm-lancam-consenso-clinico-inedito-na-area-de- psicologia/ [ Links ]
Tae, B., Pelaggi, E. R., Moreira, J. G., Waisberg, J. Matos, L. L., & D`Elia, G. (2014). O impacto da cirurgia bariátrica nos sintomas depressivos e ansiosos, comportamento bulímico e na qualidade de vida. Revista do Colégio Brasileiro de Cirurgiões, 41,155-160. [ Links ]
Tayyem, R., Ali, A., Atkinson, J., & Martin, C. R. (2011). Analysis of health-related quality of life instruments measuring the impact of bariatric surgery: Systematic review of the instruments used and their content validity. The Patient - Centered Outcomes Research, 4,73-87. [ Links ]
Weineland, S., Arvidsson, D., Kakoulidis, T., & Dahl, J. (2012). Acceptance and commitment therapy for bariatric surgery patients, a pilot RCT. Obesity Research & Clinical Practice, 6,21-30. [ Links ]
Wolf, N. (1992). O mito da beleza: Como as imagens de beleza são usadas contra as mulheres. Rio de Janeiro: Rocco. [ Links ]
 Corresponding author at:
Corresponding author at:
Corresponding author at
Michele Daiane Birck
Instituto de Psicologia (IP), Universidade de Brasília (UnB), Campus Universitário Darcy Ribeiro
ICC - Ala Sul, Bloco A, Térreo
CEP: 70910-900, Brasília, DF, Brazil
E-mail: micheledaianepsi@yahoo.com.br
Received: 12/10/2016
Revision received: 15/05/2017
Accepted: 22/05/2017
1 This research received financial support of The National Counsel of Technological and Scientific Development of Brazil.

