










Servicios Personalizados
Revista

Articulo
 Inglés (pdf)
Inglés (pdf)
 Articulo en XML
Articulo en XML Referencias del artículo
Referencias del artículo
Indicadores
Compartir

 Permalink
PermalinkPsicologia Clínica
versión impresa ISSN 0103-5665versión On-line ISSN 1980-5438
Psicol. clin. vol.30 no.3 Rio de Janeiro sept./dic. 2018
https://doi.org/10.33208/PC1980-5438v0030n03A06
SEÇÃO O LIVRE
In search of connection: towards a transdiagnostic view of dissociative phenomena through Research Domain Criteria (RDoC) framework
Em busca de conexão: rumo a uma visão transdiagnóstica de fenômenos dissociativos mediante o paradigma do Research Domain Criteria (RDoC)
En busca de conexión: hacia una visión transdiagnóstica de los fenómenos disociativos mediante el paradigma del Research Domain Criteria (RDoC)
Pamela IndelliI; J. Landeira-FernandezII; Daniel C. MograbiIII
IMestranda pela Universidade Federal do Rio de Janeiro (UFRJ), Rio de Janeiro, Brasil. indellipamela@gmail.com
IIDoutor pela University of California (UCLA), Los Angeles, United States of America; Professor Adjunto do Departamento de Psicologia da Pontifícia Universidade Católica do Rio de Janeiro (PUC-Rio), Rio de Janeiro, Brasil
IIIDoutor pelo King's College London, Institute of Psychiatry, Psychology and Neuroscience, London, United Kingdom; Professor Adjunto do Departamento de Psicologia da Pontifícia Universidade Católica do Rio de Janeiro (PUC-Rio), Rio de Janeiro, Brasil
ABSTRACT
Current psychiatric nosological classifications maintain a heterogeneous categorical view of clinical presentations that contribute to overlapping symptoms across different disorders, thus influencing appropriate diagnosis and treatment. The United States National Institute of Mental Health (NIMH) proposed the Research Domain Criteria (RDoC) project as an alternative dimensional approach that comprises different units of analysis across psychopathology. Although it may represent a paradigm shift, investigations of its application for dissociative phenomena that are present in various clinical conditions are still lacking. The present review examines theoretical models of dissociation and their presence in a wide range of clinical conditions. The literature review indicated the suitability of a transdiagnostic concept of altered states of consciousness by considering dimensions of temporality, narrative, embodiment, affect, and intersubjectivity.
Keywords: dissociation; psychopathology; altered states of consciousness; research domain criteria.
RESUMO
As classificações nosológicas psiquiátricas atuais mantêm uma visão categórica heterogênea das apresentações clínicas que contribuem para a sobreposição de sintomas entre diferentes distúrbios, influenciando, assim, o diagnóstico e o tratamento adequados. O United States National Institute of Mental Health (NIMH) propôs o projeto Research Domain Criteria (RDoC) como uma abordagem dimensional alternativa que engloba diferentes unidades de análise para a compreensão da psicopatologia. Embora essa perspectiva possa representar uma mudança de paradigma, ainda faltam investigações sobre sua aplicação para fenômenos dissociativos presentes em várias condições clínicas. A presente revisão analisa modelos teóricos de dissociação e sua presença em uma ampla gama de condições clínicas. A revisão da literatura indicou a adequação de um conceito transdiagnóstico de estados alterados de consciência, considerando dimensões de temporalidade, narrativa, corporificação, afeto e intersubjetividade.
Palavras-chave: dissociação; psicopatologia; estados alterados de consciência; research domain criteria.
RESUMEN
Las clasificaciones nosológicas psiquiátricas actuales mantienen una visión categórica heterogénea de las presentaciones clínicas que contribuyen a la superposición de los síntomas en diferentes trastornos, lo que influye en el diagnóstico y el tratamiento adecuados. El United States National Institute of Mental Health (NIMH) propuso el proyecto Research Domain Criteria (RDoC) como un enfoque dimensional alternativo que comprende diferentes unidades de análisis para la comprensión de la psicopatología. Aunque esta perspectiva puede representar un cambio de paradigma, aún faltan investigaciones sobre su aplicación para los fenómenos disociativos que están presentes en diversas condiciones clínicas. La presente revisión examina modelos teóricos de disociación y su presencia en una amplia gama de condiciones clínicas. La revisión de la literatura indicó la idoneidad de un concepto trans diagnóstico de estados alterados de conciencia al considerar dimensiones de temporalidad, narrativa, corporificación, afecto e intersubjetividad.
Palabras clave: disociación; psicopatología; estados alterados de conciencia; research domain criteria.
Introduction
Although the concept of dissociation has been a subject of discussion, it can be broadly defined as a condition in which mental functions that are usually integrated automatically operate outside of conscious awareness (Ludwig, 1983). This phenomenon was one of the first topics of interest in psychiatry in the 18th and 19th centuries, but the concept gradually diminished in importance during the second half of the 20th century, with a backlash movement against it in the 1990s, maintaining its related psychopathology away from social and scientific recognition (Dalenberg et al., 2007).
Even though there has been some increase in the exploration of this topic in the past few decades, research in this area is still insufficient (Sar & Ross, 2014). Such dismissal of the topic reflects the stigma around dissociative symptoms, with considerable disbelief by both clinicians and the general public with regard to their existence or relevance (Spiegel, 2006).
Epidemiological studies indicate a substantial prevalence of dissociative symptomatology in clinical populations, with considerable underdiagnosis compared with other clinical conditions (Foote et al., 2006; Mueller-Pfeiffer et al., 2013). Nevertheless, dissociation itself or as a comorbidity is known to be related to increases in dysfunctionality, the risk of suicidal behavior, and the worse prognosis of various mental disorders (Sar & Ross, 2006; Sperandeo et al., 2017; Lyssenko et al., 2018). Moreover, little evidence supports the effective psychopharmacological treatment of this condition (Sar, 2014; Moghaddas et al., 2017).
Considering the growing interest in dissociative phenomena after a long historical hiatus and the underdiagnosis of these symptoms despite their clinical importance, the present review explores theoretical models of dissociation and its presence in a wide range of clinical conditions. This review is divided into three sections. The first section provides an overview of central theories that seek to explain dissociative phenomena and discusses its underlying functions. The second section discusses the identification of dissociative symptoms in a wide range of mental disorders. Since the advances in mental health research have not been consistent in specifying the mechanisms involved in the occurrence of dissociative symptoms (Avdibegović, 2012), suggestions regarding transdiagnostic dimensional perspectives will be discussed in the third section.
Historical overview of the concept of dissociation
Initial formulations
The first attempt to explore disruptions in consciousness can be traced back to studies of somnambulism and hypnosis by Puységur (1751-1825), who considered the existence of a disconnection between memory and thought operations in such states. In 1845, Moreau de Tours introduced the term "dissociation", defined as disintegrated ideas, followed by the study by Gross-Jean (1855) with patients with different personalities that could operate at the same time (Crabtree, 1993). Richet (1884) also described three main categories presumed in dissociation of intellectual functions: personality, the perception of events as disconnected from the self, and the awareness of observing and acting (van der Hart & Horst, 1989).
After clinicians in France associated the presentation of hysteria with a split of consciousness or personality, Charcot (1893) proposed a relationship between hysterical symptoms (e.g., paralysis, amnesia, sensory loss, and convulsions) and hypnotic states. He asserted that hypnotic states had a psychological nature and suggested a link between such symptoms and subconscious ideas that do not surface into conscious awareness. These suggestions led to Pierre Janet's theory of dissociation as an underlying cause of hysteria, defining it as a consequence of constitutional vulnerabilities and emotional imprints following traumatic experiences that lead to an integrative failure of functional systems that are related to affect, behavior, and a distinct sense of self (van der Hart & Boon, 1997). Janet suggested that traumatic memories become primary fixed ideas that return in the form of intrusions, with dreams and fantasies being secondary fixed ideas because they are not directly based on real events but still related to them to some extent (van der Hart, Witztum & Friedman, 1993).
Along with these theories, many other concepts added diverging terms to explain dissociative presentations, such as intellectual duality (Tascher, 1855), double consciousness (Binet, 1890), multiple personalities (Bourru & Burot, 1888), and subliminal consciousness (Myers, 1893). Myers (1940) stated that soldiers who returned from World War I reexperienced symptoms that could be best described as a personality dissociation, forming an Emotional Personality (EP) distinct from an Apparently Normal Personality (ANP). The EP would be in control, with direct contact to all aversive trauma-related memories that lead to such reexperiences, until the ANP gradually returns and retains only a distant memory of the emotional trauma (van der Hart & Brown, 1992).
Alternative propositions
Breuer and Freud (1893) later introduced an idea that contrasted with Janet's conceptualization of dissociative tendencies, declaring that constitutional predispositions do not cause a split of consciousness but rather that the splitting itself prompts psychological vulnerability. In this context, the concept of repression, used interchangeably with dissociation, was developed through investigations of traumatic events that were excluded from memory (e.g., memories of childhood sexual abuse).
In Freud's description of the etiology of neurosis, he proposed the so-called seduction theory (Freud, 1896), implying that sexual seduction and abuse were the origin of hysteria, reinforcing an external causality of psychic trauma. From 1897, Freud departed from this line of thought and considered inner conflicts as the cause of neurosis, suggesting that hysteria was not a consequence of the direct experience of childhood sexual seduction but rather a consequence of childhood fantasies of sexual seduction. Nonetheless, his past propositions were revived through considerations of ego defense mechanisms.
Within the latter perspective, repression or dissociation was interpreted as a mechanism of ego defense that retains unpleasant traumatic registers away from consciousness, thus provoking such clinical symptoms as amnesia, trance, and hallucinatory states. Similarly, Ferenczi considered that the impact of childhood trauma on the psyche leads to the formation of splits in personality. Fairbairn used the term "schizoid" to define a similar defensive mechanism (Tarnopolsky, 2003).
Spiegel (1963) agreed with these ideas and proposed one of the first dynamic models regarding a dissociation-association continuum. Another author who suggested the possibility of placing dissociation on a continuum was Ludwig (1966), which he described as Altered States of Consciousness (ASC). Followed by Tart's (1969) work on altered states in absorption, trance states, depersonalization, and derealization, Ludwig questioned whether it would be more appropriate to allocate dissociation as a subcategory of ASC or within a spectrum of other conditions (e.g., alpha rhythm and transcendental meditative states).
Ludwig's explanation of what constituted altered states of consciousness considered several distinctive features, such as alterations of thinking, disturbances in time sense, loss of control, changes in emotional expression, changes in body image, perceptual distortions, changes in meaning or significance, sense of the ineffable, and hypersuggestibility. Ludwig reinforced an evolutionary perspective, claiming that they served biological, psychological, and social functions and represented different types of experiences and expression that range from adaptive to maladaptive though ultimately having survival value for the species.
Psychiatric manuals
With regard to psychiatric classification systems, the Diagnostic and Statistical Manual of Mental Disorders, 2nd edition (DSM-II; American Psychiatric Association, 1968), and the International Statistical Classification of Diseases and Related Health Problems, 9th revision (ICD-9; World Health Organization, 1979), formalized dissociative symptoms by considering hysterical and other neurotic conditions (e.g., depersonalization). The revised third version of DSM-III (American Psychiatric Association, 1980) incorporated a change toward a phenomenological view that divided these diagnoses into two different groups of disorders: dissociative disorders (depersonalization/derealization) and somatoform disorders (conversion). Subsequently, in both the DSM-IV (American Psychiatric Association, 1994) and DSM-V (American Psychiatric Association, 2013) diagnostic criteria, Dissociative Disorders (DD) included categories of dissociative amnesia, fugue, depersonalization, derealization, dissociative identity, other specified dissociative disorders, and unspecified dissociative disorders. The DSM-V describes dissociative symptoms as the following:
a disruption of and/or discontinuity in the normal integration of consciousness, memory, identity, emotion, perception, body representation, motor control, and behavior […] experienced as a) unbidden intrusions into awareness and behavior, with accompanying losses of continuity in subjective experience (i.e., "positive" dissociative symptoms such as fragmentation of identity, depersonalization, and derealization) and/or b) inability to access information or to control mental functions that normally are readily amenable to access or control. (American Psychiatric Association, 2013, p. 328)
This definition supports theories that assert that dissociation affects all areas of psychological functioning (Spiegel et al., 2013; Spiegel et al., 2011). Based on this perspective, the ICD-10 (World Health Organization, 2004) went further than its previous version and specified more than eight dissociative-related categories, including stupor, convulsions, sensory loss, trance, and possession.
Finally, the most recent version of the ICD (ICD-11; World Health Organization, 2018) included revised categories of dissociative neurological symptoms, dissociative amnesia, trance disorder, possession trance disorder, dissociative identity disorder (DID), partial dissociative identity disorder, depersonalization-derealization disorder, secondary dissociative syndrome, and Ganser syndrome. Although these new shifts strengthen the perception of dissociative symptoms from a dimensional perspective, this was not the common understanding of theoretical models that emerged in those decades.
Theoretical models of dissociation
Typological perspectives
Traditional typological perspectives suggest the existence of only two distinct forms of dissociative presentation, categorically defined as pathological or not. The non-pathological view of dissociation arose from the idea that it can involve normal aspects of everyday functioning. In this type of presentation, dissociative symptoms include benign conditions with only a partial reduction of awareness of internal states (e.g., absorption, daydreaming, and automatized motor activities; Lynn & Rhue, 1994). A pathological form of dissociation would require a persistent state implicated in long-term interferences with the person's experience and capacity to maintain contact with others and the environment (e.g., amnesia, depersonalization, and identity confusion; Putnam, 1985).
Another typological distinction was proposed in a bipartite model that recognized detachment and compartmentalization as qualitatively distinct and autonomous types of dissociation. Holmes et al. (2005) defined detachment as an altered state of consciousness that is characterized by a sense of separation of one's body, emotional experience, a sense of self and its surroundings, and feelings of being disconnected or in a dream. This protective mechanism would serve the purpose of attenuating aversive effects of intense traumatic events. In contrast, compartmentalization refers to a deficit in the deliberate control of specific psychobiological processes, impairing the ability to bring accessible information into conscious awareness. However, these processes can still operate and influence ongoing cognition, emotion, and action.
Dimensional perspectives
A dimensional model of dissociative presentations was proposed by Braun (1988), based on the central idea of dissociation that derived from a failure of associative processes. According to his BASK model, dissociative processes can affect four independent levels concerning (1) behavior, (2) affect, (3) sensation, and (4) knowledge. The range in which they can vary goes from a fully preserved conscious state to suppression, denial, repression, up to a dysfunctional dissociative condition.
Hence, Braun considered continuous dimensions of altered states of consciousness that are related to processing event-related information and behaviors, meaning making, affective experiences, and related bodily sensations. Braun argued that a preserved memory capacity requires a dynamic interaction between all four levels; thus, dissociative disorders are generated through the disruption of memory functions and identity.
Likewise, Thompson and Zahavi (2007) constructed a phenomenological model with four dimensions that described qualitative aspects of human consciousness and subjectivity, being: (1) temporality (i.e., the sense of time and memory), (2) narrative (i.e., the story-like quality of thought), (3) embodiment (i.e., the sense of having and consciously belonging to a body), and (4) affect (i.e., the emotional experience).
These authors specified what they considered the main topics of relevance in the construction of consciousness theories (i.e., intentionality, time-consciousness, embodiment, intersubjectivity, self-awareness, and the first-person perspective) to elucidate a broad spectrum that might comprise altered states of consciousness. Their perspective argued for the need to consider the integration of aspects based on phenomenological, cognitive-scientific, and analytic approaches.
Traits vs. peritraumatic reactions
An alternative way to distinguish dissociation would be differentiating as dissociative traits or dissociative reactions. Marmar, Weiss, and Metzler (1997) used the term "peritraumatic reactions" to describe the way in which a person could react during or immediately after a traumatic experience. Thus, peritraumatic dissociation can be defined as a dissociative response that occurs during or in the aftermath of a traumatic event. This reaction is correlated with event-related memory reduction, vague or fragmented recollections, amnesia, and other symptoms (e.g., confusion, derealization, and depersonalization).
In contrast, the concept of dissociative traits represents characteristics that significantly influence a person's identity, with more diffuse and prolonged expression compared with dissociative reactions, such as in dissociative identity disorder (Eisen & Lynn, 2001). Studies that have investigated risk factors for Posttraumatic Stress Disorders have shown that peritraumatic reactions are the best predictors of the future development of PTSD (Briere, Scott & Weathers, 2005; Murray, Ehlers & Mayou, 2002). However, the dissociative response during a traumatic event is not itself pathological, although it can be in cases in which it leads to conditioned dissociative reactions and impairments in the processing and integration of traumatic event-related information, which can provoke subsequent intrusions (Spiegel & Cardeña, 1991; Spiegel, Koopman & Classen, 1994).
Conceptual mismatch
The debate about the presence of dissociative states in clinical populations and its implication in the maintenance and treatment of various conditions is still far from conclusive. The main challenges include a broad range of definitions, the misuse of technical terms that refer to dissociative phenomena, and the absence of coherent common ground to discuss their presentations (Brown, 2006). In this regard, Dalenberg and Paulson (2014) summarized the categories whereby scientists have discussed the pathological nature of dissociative experiences in accordance to (1) type, (2) level, (3) timing, (4) relationship to defense, (5) frequency, and (6) purpose. Additionally, they mentioned the wide variety of concepts that could be found in research that references dissociation (Table 1).
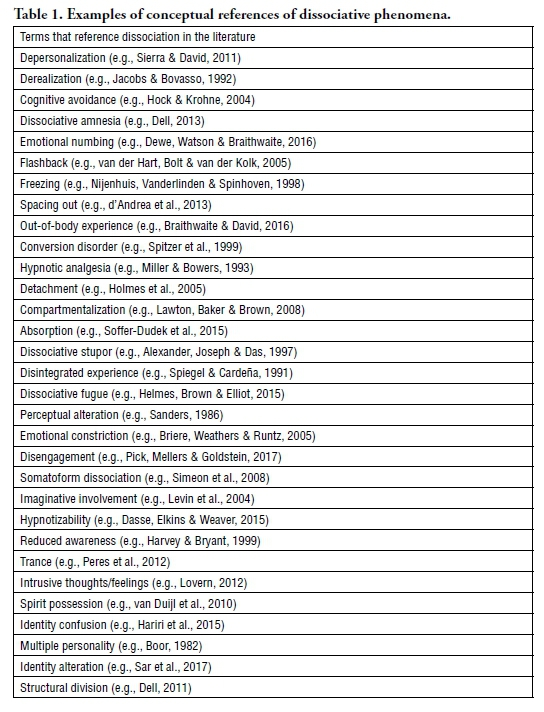
Considering this heterogeneity, Cardeña (1994) reviewed various applications of the term "dissociation" and proposed three main categories in which dissociative phenomena are considered in the literature. The first category involves the idea of nonconscious or nonintegrated mental modules or systems, which can be subdivided into (1) dissociation as the absence of the conscious awareness of impinging stimuli or ongoing behaviors; (2) dissociation as the coexistence of separate mental systems that should be integrated in the person's consciousness, memory, or identity; and (3) dissociation as ongoing behavior or perception that is inconsistent with a person's introspective verbal report.
The second category alludes to not only impairments in mental processes integration but also qualitative changes in altered states of consciousness. Most importantly, there is an appeal to not consider momentary states of partial disconnection, such as daydreaming or meditative states, as genuine dissociative experiences. Thus, he offers a definition of dissociation as an alteration of consciousness that comprises disconnection/disengagement from the self or the environment as a fundamental aspect of the experience.
The third category reinforces the psychoanalytic understanding of dissociation as a defense mechanism. The organism, while dealing with an ongoing danger or threat to its survival, goes into a dissociative state to preserve its psychological integrity. This perspective raises the question about how dissociative experiences that are originally protective of the psyche can become maladaptive. A few theories of traumatic dissociation have been proposed in an attempt to provide greater clarity concerning this topic (Dell & O'Neil, 2009), but numerous questions remain.
Essentially, all of these various terms and categories of dissociative phenomena, shifting between references to an intrapsychic structure, process, psychological defense, deficit, or a long list of symptoms, can ultimately cause widespread conceptual confusion. This conceptual confusion hinders research efforts to better inform diagnosis and treatment, not only for dissociative disorders but also for other mental disorders that include dissociative experiences in their symptomatology.
Dissociation in psychopathology
Dissociation in posttraumatic stress symptoms
Although traumatic experiences were extensively contemplated throughout the 18th and 19th centuries literature with regard to their association with dissociative phenomena, the inclusion of dissociative symptoms in the diagnosis of PTSD required a longer time to be officially recognized in psychiatric manuals (Wolf et al., 2012). Posttraumatic stress disorder was mainly considered a fear disorder, emphasizing the role of hyperarousal in its symptomatology. This perspective reflected studies that used animal models to investigate the neurocircuitry that is involved in threat responses and its association with the maintenance of threat responses even in the absence of threatening stimuli (LeDoux, 2015). As a result, the vast majority of theoretical models of PTSD included reexperiencing, avoidance, and physiological hyperarousal as central symptoms of the disorder (Foa, Steketee & Rothbaum, 1989).
Psychological trauma and PTSD were not included in the DSM until 1980, when the psychiatry community could no longer ignore the symptoms that were presented by soldiers who returned from war, as well as victims of sexual abuse, domestic violence, and other forms of traumatic experiences (van der Kolk, 2014). However, in contrast to the prevalence of dissociative symptoms in Acute Stress Disorder (AST), the diagnosis of PTSD in the DSM-III (American Psychiatric Association, 1980) and DSM-IV (American Psychiatric Association, 1994) only addressed symptoms that were categorized into four clusters: (1) intrusive reexperiencing, (2) avoidance, (3) hyperarousal, and (4) hypervigilance. Despite multiple clinical and epidemiological sources of evidence that indicated the importance of recognizing a different presentation of posttraumatic stress reactions involving dissociative states (Lanius et al., 2012; Stein et al., 2013), only the most recent DSM-V (American Psychiatric Association, 2013) publication recognized a dissociative subgroup within the PTSD diagnosis.
The DSM-V (American Psychiatric Association, 2013) predicts the occurrence of symptoms of depersonalization (i.e., experiences of unreality or detachment from one's mind, self, or body) and derealization (i.e., experiences of unreality or detachment from one's surroundings) symptoms along with the other PTSD clusters, but it does not consider other forms of dissociative states. The changes that were made in the DSM-V were considered quite modest because there was an appeal to also include an alternative form of the disorder (Pai, Suris & North, 2017), such as Herman's (1992) proposal of a diagnosis of complex PTSD as a result of repeated or prolonged exposure to multiple traumas, usually in an interpersonal context. A significant amount of evidence indicates that prolonged exposure to trauma causes more dysfunction in other domains that are related to emotional dysregulation, dysfunctional self-beliefs, and relational impairments (Ford & Courtois, 2009).
Recognition of complex PTSD and clinical implications
Already included as Disorders of Extreme Stress Not Otherwise Specified (DESNOS) in the DSM-IV (American Psychiatric Association, 2013), an alternative diagnosis of complex PTSD was formalized only in the most recent version of the ICD-11 (World Health Organization, 2018), which included the same criteria that were already present in the PTSD diagnosis, with three additional clusters: (1) severe and pervasive problems in affect regulation; (2) persistent beliefs about oneself as diminished, defeated, or worthless, accompanied by deep and pervasive feelings of shame, guilt, or failure related to the traumatic event; and (3) persistent difficulties in sustaining relationships and in feeling close to others. This elaborated presentation has a much closer connection to dissociative symptoms, since problems with emotional regulation and attachment can impair the safety perception of internal and external environments that can potentially induce dissociative responses (Porges, 2011).
Supported by a meta-analysis indicating the best clinical interventions for PTSD (Powers et al., 2010), formal treatment guidelines recognize prolonged exposure therapy as one of the most effective treatments for this disorder (Foa et al., 2009; Rauch, Eftekhari & Ruzek, 2012). Developed within the cognitive behavioral therapy (CBT) premises, the protocol is based on a "desensitization" process through gradual exposure to traumatic memories, with the aim of reducing the intense reactivity that is generated by contact with trauma-related content, consequently leading to cognitive restructuring toward threat perception and fear-related beliefs.
Conversely, several authors discussed whether this treatment model is potentially flawed for the treatment of recent symptoms that were included within the category of Posttraumatic stress diagnosis in the DSM-V (American Psychiatric Association, 2013) and the ICD-11 (World Health Organization, 2018), such as shame, self-blame, and dissociative symptoms (Dorahy et al., 2013). In fact, the treatment proposals of the International Society for Traumatic Stress Studies (ISTSS) highlight interventions that focus on affective, relational, and physiological components (e.g., Attachment, Regulation and Competency - ARC; Skills Training in Affective and Interpersonal Regulation - STAIR-NT; Accelerated Experiential Dynamic Psychotherapy - AEDP) as more coherent models to attenuate pervasive symptoms that are related to prolonged exposure to trauma (Cloitre et al., 2012).
Treatment indications for complex PTSD follow a three-phase model (Herman, 1992; van der Hart & Boon, 1997), considering stages of (1) safety and emotion regulation, (2) trauma processing, and (3) social engagement. Similarly, the recently updated version of the guidelines of the International Society for the Study of Trauma and Dissociation (ISSTD) asserts that trauma-related dissociation requires the acknowledgment of distinctive features, highlighting three central intervention components of stabilization, trauma work, and integration (Chu et al., 2011).
Trauma-related dissociation models
Evidence indicates that exposure to severe trauma increases the probability of alterations of consciousness (Putnam et al., 1996; Vermetten & Spiegel, 2014; Dalenberg et al., 2012). Studies have reported an overlap between complex posttraumatic stress disorder (C-PTSD), dissociative disorder (DD) and borderline personality disorder (BPD) symptoms (Kienle et al., 2017; Giourou et al., 2018).
Based on this understanding, Frewen and Lanius (2014) constructed a four-dimensional model of trauma-related altered states of consciousness by considering data from neuroimaging studies that revealed distinct patterns of neural activation in PTSD patients who presented with dissociative symptoms. This research revealed the excessive inhibition of limbic circuits in this group of patients, resulting in blunted affect and disconnected experiences that are similar to a state of depersonalization (Lanius et al., 2002), together with potential mixed dissociative states with co-occurring symptoms of hyper and hypoarousal in this clinical subgroup (Bremner et al., 1998).
Accordingly, their 4-D model considered altered states of consciousness on a continuum that varied from normal waking consciousness alterations (NWC) to more pathological trauma-related altered states of consciousness (TRASC), with the latter associated with dimensions of time (e.g., reminder distress to flashbacks), thought (e.g., negative self-other-referential thinking to hearing voices), body (e.g., hyperarousal to depersonalization), and emotion (e.g., general negative affect to compartmentalized emotion). These dimensions are not independent but rather different categories of dissociative presentations in trauma-related psychopathology.
In contrast, van der Hart et al. (2004) refuted attempts to conceptualize dissociation that included mild presentations of altered states of consciousness, suggesting an exclusive consideration of the construct of a structural division of the personality as a consequence of traumatic experiences. Based on their explanations of trauma-related and dissociative disorder-related psychopathology, the personalities formed functions relatively apart. The apparently normal personalities (ANPs) are responsible for everyday functions, whereas the emotional personalities (EPs) can be divided into engaged (hyperaroused emotional personalities) and disengaged (hypoaroused emotional personalities), incorporating defensive systems against threats and attachment loss.
In this structural dissociation model (van der Hart, O.; Nijenhuis, E. R. S. & Steele, K., 2006), each part has independent psychological, physiological, and neural profiles when exposed to threat cues that are mediated by different parasympathetic branches. The structural dissociation of personality could be primary (i.e., involving a single ANP and EP, as in detachment), secondary (i.e., beyond a single ANP and EP, as in complex trauma-related disorder) or tertiary (i.e., division of ANP in addition to dissociation among EPs, as in dissociative identity disorder). Moreover, there are implications of a more complex presentation with possible comorbidities, considering personality disorders and other diagnoses in which dissociation is part of their symptomatology.
Other comorbidities
In accordance with the proposition of van der Hart et al. (2004), in which the diagnoses of PTSD and DID are on a continuum of severity, clinical studies of dissociative presentations in psychopathology discuss the possibility of an overlap of complex PTSD, dissociative disorders, and borderline personality disorder symptoms (Ford & Courtois, 2014; Scheiderer, Wood & Trull, 2015; van Dijke, Hopman & Ford, 2018). High comorbidity even led a few authors to propose the inclusion of BPD within the trauma spectrum (Vermetten & Spiegel, 2014). Additionally, in an attempt to find common ground between diagnoses, BPD disorder and chronic complex dissociative disorders have been conceptualized as disorders of emotion dysregulation that are directly influenced by a history of trauma (Brand & Lanius, 2014).
Furthermore, dissociative symptoms are found across various other diagnoses. A recent meta-analysis of studies that used the Dissociative Experiences Scale (DES) (Lyssenko et al., 2018) measured dissociative symptoms across mental disorders and found the highest prevalence in dissociative disorders (mean scores > 35), followed by PTSD, BPD and conversion disorder (mean scores > 25), and also in somatic symptom disorder, addictive disorders, eating disorders, schizophrenia, anxiety disorder, obsessive-compulsive disorder, and affective disorders (mean scores > 15). Additionally, an epidemiological study of 933 psychiatric outpatients identified significant risk factors for dissociative symptom severity, including the presence of borderline and narcissistic personality disorders, substance abuse disorders, psychopathologic traits of anger, psychoticism, and obsessiveness (Sperandeo et al., 2017). These results showed that dissociation can be present at different levels but in almost all clinical populations.
Acknowledging these comorbidities, much criticism has been levied against the continually longer lists of various mental disorders (Maj, 2005; Galatzer-Levy & Bryant, 2013). The high prevalence of the same symptomatology across different diagnoses highlights issues in the mental health field that are related to intervention decisions for patients who present a substantial number of symptoms that overlap in clinical evaluations (Regier, Kuhl & Kupfer, 2013). Some authors appealed to clarifying the processes that underlie specific conditions and recognizing idiosyncratic factors when addressing functional impairments (Frías & Palma, 2015; McNally et al., 2015; Knefel, Tran & Lueger-Schuster, 2016), especially when they involve dissociative presentations (Sar, 2014; Lyssenko et al., 2018).
Dissociative experiences using Research Domain Criteria
Central aspects of Research Domain Criteria
According to Kraepelin's typology, current diagnostic systems reflect a paradigm in crisis (Moskowitz, 2011). The development of the Diagnostic and Statistical Manual of Mental Disorders (DSM) and the International Classification of Diseases (ICD) was largely based on clinical observations and patients' self-reports of symptoms. Hence, some authors have criticized the premature recognition of these conditions as real disease entities (Hyman, 2010; Kozak & Cuthbert, 2016). Due to its categorical view of mental disorders, a consensus has been reached with regard to recognizing excessive heterogeneity in individuals who are diagnosed with the same disorder (Kozak & Cuthbert, 2016). Additionally, accumulating evidence in the fields of neuroscience and genetics has not been appropriately applied to understanding and treating psychiatric nosologies (Kose & Cetin, 2017).
Further problems would include the limited validity of conventional diagnoses, the overlap of symptoms between disorders, subthreshold symptoms and particularities that affect clinical evaluation and outcome, implicit assumptions of biological etiologies, and investigative techniques that are applied to inadequately conceptualized mental illnesses. Reflecting on these issues, the NIMH Research Domain Criteria (RDoC) project suggested an alternative system to organize psychopathology within a transdiagnostic framework that is not limited to specific groups of disorders. This initiative seeks to apply scientific knowledge to establish dimensions of functions, varying between pathological and non-pathological presentations and intending to gain a better understanding of clinical conditions (Kozak & Cuthbert, 2016).
Rather than being a substitute for current psychiatric nosologies, the RDoC project is not intended to disrupt the already acquired knowledge of mental disorders but rather to encourage more efforts in scientific research that apply multidisciplinary empirical evidence to more accurately investigate the processes that underlie these symptoms (Krueger & Markon, 2014). Refining available treatments for specific targets will advance interventions in psychiatry and psychology by considering idiosyncratic features in clinical evaluations. These efforts seek to inform better clinical decision-making, with a focus on impaired mechanisms causing the dysfunctions that are presented by patients, instead of a broad inaccurate description of symptom clusters (Kose & Cetin, 2017).
Conceptual organization of RDoC
As Kozak and Cuthbert (2016) described, NIMH convened workgroups to discuss dimensional constructs that meet the following requirements: (1) previously validated constructs through studies from multiple laboratories; (2) evidence of an underlying neural circuit or system that is related to its functions; and (3) link to a psychiatric clinical phenomenon. The group developed systematic guidance to define equally relevant units of analysis that are necessary for the proposition of constructs, resulting in specific units that are related to genes, molecules, cells, circuits, physiology, behaviors, and self-reports of symptoms. Environmental and developmental factors were also inserted as essential contexts for conceptualizing a functional impairment (Fig. 1).
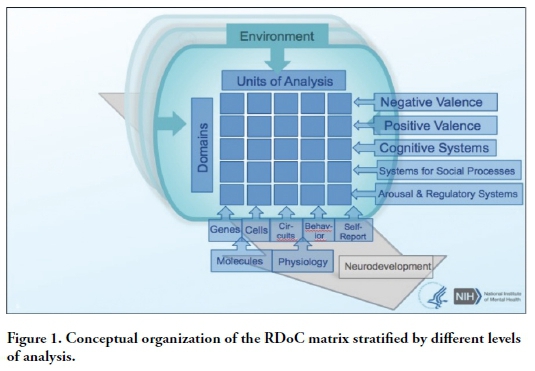
The domains and their related constructs that have been proposed to date encompass (1) Negative Valence Systems (including acute threat, potential threat, sustained threat, loss, and frustrative nonreward); (2) Positive Valence Systems (including reward responsiveness, reward learning, and reward valuation); (3) Cognitive Systems (including attention, perception, declarative memory, language, cognitive control, and working memory); (4) Systems for Social Processes (including affiliation and attachment, social communication, the perception and understanding of self, and the perception and understanding of others); and (5) Arousal/Regulatory Systems (including arousal, circadian rhythms, and sleep and wakefulness). A core objective for future explorations is to investigate the components of each construct, interactions between these components, and the ways in which they are related to other systems in the promotion of clinical phenomena (Kozak & Cuthbert, 2016).
Dissociation within the framework of RDoC
Cardeña (1994) used the term "constellation" to describe a viewpoint for conceptualizing dissociative phenomena as caused by the activity of multiple systems outside conscious awareness. Based on this perspective, the author suggested that dissociation should be investigated from a broad perspective, requiring the study of connections between various systems (i.e., memory, consciousness, identity, and emotion). Considering that one of the central objectives of the RDoC project is to encourage research that addresses the ways in which underlying systems of constructs or domains are connected, dissociative states might be an interesting line of investigation.
Research that investigates impairments in dissociative states has found a complex dysfunctional system that is related to the avoidance of aversive stimuli, dysfunctional self-perception, blunted autonomic reactivity (Schäflein et al., 2018a), disrupted affective-cognitive processing (Krause-Utz & Elzinga, 2018), impairments in interoceptive accuracy, and alterations of cardiac vagal tone (Schäflein et al., 2018b). Another group of deficits included emotional numbing, memory disruptions (Krause-Utz & Elzinga, 2018), lower pain sensitivity (Ludäscher et al., 2010), emotion dysregulation that is linked to discontinuity in dyadic socio-affective interactions (Forrest, 2001), lower mentalization and empathetic capacities (Schimmenti, 2016), and amnesia for autobiographical events that is caused by breakdown between memory, the sense of self, and overall metacognitive processes (Sar, Dorahy & Kruger, 2017).
These impaired functions may indicate the possible relevance of various constructs within RDoC's domains: acute and sustained threat (Negative Valence Systems), responsiveness to reward and reward learning (Positive Valence Systems), attention, perception, memory, and cognitive control (Cognitive Systems); all four constructs in Systems for Social Processes (i.e., affiliation/attachment, social communication, the perception/understanding of self, and the perception/understanding of others); and arousal (Arousal/Modulatory Systems). Additionally, developmental factors (e.g., prolonged exposure to trauma in early developmental stages) and environmental aspects that are related to family, society, and culture (e.g., denial, reality distortions, paranoia, boundary violations, and narcissism) have been found to be correlated with more severe presentations of dissociative symptoms (Sar, Dorahy & Krüger, 2017; Sundermann, Chu & DePrince, 2013). Therefore, dimensions that are related to developmental and environmental factors that are predicted in the RDoC matrix are also relevant to understanding this condition.
Despite efforts to explore neurobiological correlates of dissociative phenomena (Vermetten, Dorahy & Spiegel, 2007; Lanius, Paulsen & Corrigan, 2014, Lanius et al., 2006; Reinders et al., 2003; Lanius, 2015; Krause-Utz & Elzinga, 2018; Brand & Lanius, 2014; Sperandeo et al., 2017; Moskowitz, 2011; van der Kruijs et al., 2014; Jay et al., 2014), current studies are still mainly based on categorical classification systems, with most data circumscribed to a group or subgroup within specific mental disorders (e.g., only DID sample or only PTSD dissociative subgroup sample) or based only on different conceptual references for dissociation (e.g., dissociative symptoms, structural dissociation, and peritraumatic dissociation). With no agreement in the literature with regard to a definition of dissociation and comparisons among heterogeneous clinical samples, it is still not possible to review data on all units of analysis as required by RDoC for a construct/domain proposal.
Therefore, it is important to acknowledge the need for conceptual common ground for future transdiagnostic studies of all of these units of analysis. It would be worthwhile to consider dissociation as a phenomenon that crosses domains and requires the consideration of functional connections between constructs, as other authors have proposed by suggesting new insertions into the RDoC matrix (Fernandez, Jazaieri & Gross, 2016; Gur & Gur, 2016; Schmidt & Vermetten, 2017). In any case, conceptualizing dissociative presentations as part of altered states of consciousness that varies along a continuum (i.e., less or more pathological forms) appears to be a perspective that is more suited to RDoC's continuum approach to constructs, considering their range from normal to abnormal levels.
Novel domains
A potential issue with inserting dissociation into the RDoC matrix is related to the requirement that the constructs are sufficiently narrow to be analyzed as a circumscribed clinical problem with specific signatures in all units of analysis. The consideration of dissociative phenomena as a unitary construct, in a domain-extent or, instead, as a result of functional connectivity between systems, will depend on theoretical references that are chosen to describe this condition. In this regard, proposals of additional domains of Social Cognition, Emotion Regulation, and Maintenance of Consciousness to be admitted in the RDoC project (Fernandez, Jazaieri & Gross, 2016; Gur & Gur, 2016; Schmidt & Vermetten, 2017) could add great value to the consideration of aspects related to altered states of consciousness.
The proposal of a Social Cognition domain was based on applied measures in patients with schizophrenia, depression, and bipolar disorder that validated emotion identification deficits across a range of groups. The authors suggested that features of social cognition would be related to complementary dimensions of negative/positive valence, intensity/arousal, and social approach/avoidance (Gur & Gur, 2016).
Similarly, the Emotion Regulation domain was also proposed as a relevant transdiagnostic factor for the onset and maintenance of various forms of psychopathology (Fernandez, Jazaieri & Gross, 2016). Conceptualized as an affective regulatory process that is the functional consequence of interactions between constructs in the five existing RDoC domains, the authors described different directions for intrapersonal emotion regulation (more oriented by the Cognitive Systems domain) and interpersonal emotion regulation (more oriented by the Social Processes domain).
Finally, Schmidt and Vermetten (2017) reviewed the translation of central dysfunctions that are found in PTSD patients and discussed their application within the RDoC matrix. They reinforced the need for a domain that is specifically related to emotion regulation (Stress and Emotional Regulation domain), also suggesting the inclusion of a Maintenance of Consciousness domain that comprises dissociative presentations that are detected in the recently formalized PTSD dissociative subgroup. These authors defended the idea that although a change in consciousness could be a result of cognitive processes, it cannot be fully explained solely by considering these processes.
Their shared foundation relies on the notion that a system is more than just the sum of its parts, which has been applied within the concept of integration in consciousness theory (Tononi, 2015) and is in accordance with proposals regarding human brain functionality as a complex network with structural and functional dynamics of high specialization and integration (Sporns, 2011).
Therefore, this perspective asserts the possibility of inserting altered states of consciousness in the RDoC matrix as a potential phenomenon that emerges from connectivity between multiple systems. Particular considerations of each related construct might not be sufficient to reach a full understanding of the processes that are involved in such a complex phenomenon as consciousness. On the other hand, once the system gets impaired, it would be beneficial to more specifically identify affected functions to achieve a more targeted model of intervention (Young & Pigott, 1999).
Conclusions
Defining a common framework to discuss dissociation in the literature is crucial for establishing alternative conceptual models that serve as guidelines for sounder psychiatric and psychological interventions. The transdiagnostic recognition of dissociative presentations, as in the RDoC matrix, requires the further refinement of underlying processes that can help improve the treatment of different conditions, including impairments in systems that are related to consciousness, memory, affect, and identity. Altogether, the present conceptual review suggests the suitability of a theoretical definition that assumes a combination of four central premises based on the theories discussed herein. Dissociation could be described as (1) a form of altered states of consciousness (Ludwig, 1983), (2) related to dimensions of temporality, narrative, embodiment, affect, and intersubjectivity (Thompson & Zahavi, 2007), (3) with each varying along a continuum of dysfunctionality (Braun, 1988; Frewen & Lanius, 2014), and (4) caused by a failure in the integration of various systems (van der Hart & Boon, 1997).
Future studies should focus on neuroimaging analyses to explore the underlying neurocircuitry that is related to all of these proposed dimensions by considering both healthy participants and individuals with a wide range of clinical diagnoses to define common targets for further investigations of the fundamental processes that are involved in these functions. Moreover, research that addresses possible interactions between systems can inform better translational efforts to achieve a transdiagnostic view of dysfunctional changes in consciousness, going beyond correlational data and investigating causality as well.
The identification of circuitry abnormalities in key systems will advance the development of more consistent explanations that comprise multidisciplinary information to surpass traditional theoretical models of dissociation that rely simply on limited levels of analysis. This could fill a gap in current knowledge toward more accurate transdiagnostic conceptualizations and treatment protocols that are effective in addressing dissociative states across conditions.
References
Alexander, P. J.; Joseph, S.; Das, A. (1997). Limited utility of ICD-10 and DSM-IV classification of dissociative and conversion disorders in India. Acta Psychiatrica Scandinavica, 95(3), 177-182. [ Links ]
American Psychiatric Association (1968). Diagnostic and statistical manual of mental disorders, 2nd ed. Washington, DC: American Psychiatric Association. [ Links ]
American Psychiatric Association (1980). Diagnostic and statistical manual of mental disorders, 3rd ed. revised. Washington, DC: American Psychiatric Press. [ Links ]
American Psychiatric Association (1994). Diagnostic and statistical manual of mental disorders, 4th ed. Washington, DC: American Psychiatric Association. [ Links ]
American Psychiatric Association (2013). Diagnostic and statistical manual of mental disorders, 5th ed. Washington, DC: American Psychiatric Press. [ Links ]
Avdibegović, E. (2012). Contemporary concepts of dissociation. Psychiatria Danubina, 24(Suppl. 3), 367-372. [ Links ]
Binet, A. (1890). On double consciousness: experimental psychological studies. Chicago: Open Court. [ Links ]
Boor, M. (1982). The multiple personality epidemic: additional cases and inferences regarding diagnosis, etiology, dynamics, and treatment. Journal of Nervous and Mental Disease, 170(5), 302-304. [ Links ]
Bourru, H; Burot, P. (1888). Variations de la personnalité. Paris: J. B. Baillière et fils. [ Links ]
Braithwaite, J. J.; David, A. S. (2016). Out of body, out of mind? An examination of out-of-body experiences and dissociative disorders. Cognitive Neuropsychiatry, 21(5), 373-376. [ Links ]
Brand, B. L.; Lanius, R. A. (2014). Chronic complex dissociative disorders and borderline personality disorder: disorders of emotion dysregulation?. Borderline Personality Disorder and Emotion Dysregulation, 1, 13. [ Links ]
Braun, B. G. (1988). The BASK model of dissociation. Dissociation: Progress in the Dissociative Disorders, 1(1), 4-23. [ Links ]
Bremner, J. D.; Krystal, J. H.; Putnam, F. W.; Southwick, S. M.; Marmar, C.; Charney, D. S.; Mazure, C. M. (1998). Measurement of dissociative states with the Clinician Administered Dissociative States Scale (CADSS). Journal of Traumatic Stress, 11, 125-136. [ Links ]
Breuer, J.; Freud, S. (1893). On the psychical mechanism of hysterical phenomena. In: Freud, S. The standard edition of the complete psychological works of Sigmund Freud, v. II (1893-1895): Studies on hysteria, 1-17. [ Links ]
Briere, J.; Scott, C.; Weathers, F. (2005). Peritraumatic and persistent dissociation in the presumed etiology of PTSD. American Journal of Psychiatry, 162, 2295-2301. [ Links ]
Briere, J.; Weathers, F. W.; Runtz, M. (2005). Is dissociation a multidimensional construct? Data from the Multiscale Dissociation Inventory. Journal of Traumatic Stress, 18(3), 221-231. [ Links ]
Brown, R. J. (2006). Different types of "dissociation" have different psychological mechanisms. Journal of Trauma and Dissociation, 7(4), 7-28. [ Links ]
Cardeña, E. (1994). The domain of dissociation. In: Lynn, S. J.; Rhue, J. W. (eds.). Dissociation: clinical and theoretical perspectives, p. 15-31. New York: Guilford Press. [ Links ]
Charcot, J. M. (1893). La foi qui guérit. Archives de Neurologie, 25, 72-87. [ Links ]
Chu, J. A.; Dell, P. F.; Van der Hart, O.; Cardeña, E.; Barach, P. M.; Somer, E.; Loewenstein, R. J.; Brand, B.; Golston, J. C.; Courtois, C. A.; Bowman, E. S.; Classen, C.; Dorahy, M.; Şar, V.; Gelinas, D. J.; Fine, C. G.; Paulsen, S.; Kluft, R. P.; Dalenberg, C. J.; Jacobson-Levy, M.; Nijenhuis, E. R. S.; Boon, S.; Chefetz, R. A.; Middleton, W.; Ross, C. A.; Howell, E.; Goodwin, G.; Coons, P. M.; Frankel, A. S.; Steele, K.; Gold, S. N.; Gast, U.; Young, L. M.; Twombly, J. (2011). Guidelines for treating dissociative identity disorder in adults, third revision. Journal of Trauma and Dissociation, 12, 115-187. [ Links ]
Cloitre, M.; Courtois, C. A.; Ford, J. D.; Green, B. L.; Alexander, P.; Briere, J.; Herman, J.; Lanius, R.; Pearlman, L. A.; Stolbach, B.; Spinazzola, J.; van der Kolk, B.; van Der Hart, O. (2012). The ISTSS expert consensus treatment guidelines for complex PTSD in adults. https://www.istss.org/ISTSS_Main/media/Documents/ISTSS-Expert-Concesnsus-Guidelines-for-Complex-PTSD-Updated-060315.pdf. [ Links ]
Crabtree, A. (1993). From Mesmer to Freud: magnetic sleep and the roots of psychological healing. New Haven: Yale University Press. [ Links ]
d'Andrea, W.; Pole, N.; DePierro, J.; Freed, S.; Wallace, D. B. (2013). Heterogeneity of defensive responses after exposure to trauma: blunted autonomic reactivity in response to startling sounds. International Journal of Psychophysiology, 90(1), 80-89. [ Links ]
Dalenberg, C. J.; Brand, B. L.; Gleaves, D. H.; Dorahy, M. J.; Loewenstein, R. J.; Frewen, P. A.; Spiegel, D. (2012). Evaluation of the evidence for the trauma and fantasy models of dissociation. Psychological Bulletin, 138(3), 550-588. [ Links ]
Dalenberg, C.; Loewenstein, R.; Spiegel, D.; Brewin, C.; Lanius, R.; Frankel, S.; Gold, S.; Van der Kolk, B.; Simeon, D.; Vermetten, E.; Butler, L.; Koopman, C.; Courtois, C.; Dell, P.; Nijenhuis, E.; Chu, J.; Sar, V.; Palesh, O.; Cuevas, C.; Paulson, K. (2007). Scientific Study of the Dissociative Disorders. Psychotherapy and Psychosomatics, 76:400-401. [ Links ]
Dalenberg, C. J.; Paulson, K. (2014). The case for the study of "normal" dissociation processes. In: Dell, P. F.; O'Neil, J. A. (eds.). Dissociation and the dissociative disorders: DSM-V and beyond, p. 145-154. New York: Routledge. [ Links ]
Dasse, M. N.; Elkins, G. R.; Weaver, C. A. (2015). Correlates of the multidimensional construct of hypnotizability: paranormal belief, fantasy proneness, magical ideation, and dissociation. International Journal of Clinical and Experimental Hypnosis, 63(3), 274-283. [ Links ]
Dell, P. F. (2011). An excellent definition of structural dissociation and a dogmatic rejection of all other models. Journal of Trauma and Dissociation, 12(4), 461-464; discussion 469-473. [ Links ]
Dell, P. F. (2013). Three dimensions of dissociative amnesia. Journal of Trauma and Dissociation, 14(1), 25-39. [ Links ]
Dell, P. F.; O'Neil, J. A. (eds.). (2009). Dissociation and the Dissociative Disorders: DSM-V and Beyond. New York: Routledge. [ Links ]
Dewe, H.; Watson, D. G.; Braithwaite, J. J. (2016). Uncomfortably numb: new evidence for suppressed emotional reactivity in response to body-threats in those predisposed to sub-clinical dissociative experiences. Cognitive Neuropsychiatry, 21(5), 377-401. [ Links ]
Dorahy, M. J.; Corry, M.; Shannon, M.; Webb, K.; McDermott, B.; Ryan, M.; Dyer, K. F. (2013). Complex trauma and intimate relationships: the impact of shame, guilt and dissociation. Journal of Affective Disorders, 147, 72-79. [ Links ]
Eisen, M. L.; Lynn, S. J. (2001). Dissociation, memory and suggestibility in adults and children. Applied Cognitive Psychology, 15, S49-S73. [ Links ]
Fernandez, K. C.; Jazaieri, H.; Gross, J. J. (2016). Emotion regulation: a transdiagnostic perspective on a new RDoC domain. Cognitive Therapy and Research, 40(3), 426-440. [ Links ]
Foa, E. B.; Keane, T. M.; Friedman, M. J.; Cohen, J. A. (2009). Effective treatments for PTSD: practice guidelines from the International Society for Traumatic Stress Studies, 2nd ed. New York: Guilford Press. [ Links ]
Foa, E. B.; Steketee, G.; Rothbaum, B. O. (1989). Behavioral/cognitive conceptualizations of post-traumatic stress disorder. Behavior Therapy, 20, 155-176. [ Links ]
Foote, B.; Smolin, Y.; Kaplan, M.; Legatt, M. E.; Lipschitz, D. (2006). Prevalence of dissociative disorders in psychiatric outpatients. American Journal of Psychiatry, 163(4), 623-629. [ Links ]
Ford, J. D.; Courtois, C. A. (2009). Defining and understanding complex trauma and complex traumatic stress disorders. In: Courtois, C. A.; Ford, J. D. (eds.). Treating complex traumatic stress disorders: an evidence-based guide, p. 13-30. New York: Guilford Press. [ Links ]
Ford, J. D.; Courtois, C. A. (2014). Complex PTSD, affect dysregulation, and borderline personality disorder. Borderline Personality Disorder and Emotion Dysregulation, 1, 9. [ Links ]
Forrest, K. A. (2001). Toward an etiology of dissociative identity disorder: a neurodevelopmental approach. Consciousness and Cognition, 10(3), 259-293. [ Links ]
Freud, S. (1896). The aetiology of hysteria. 3:191-221. [ Links ]
Frewen, P. A.; Lanius, R. A. (2014). Trauma-related altered states of consciousness: exploring the 4-D model. Journal of Trauma and Dissociation, 15(4), 436-456. [ Links ]
Frías, Á.; Palma, C. (2015). Comorbidity between post-traumatic stress disorder and borderline personality disorder: a review. Psychopathology, 48, 1-10. [ Links ]
Galatzer-Levy, I. R.; Bryant, R. A. (2013). 636,120 Ways to have posttraumatic stress disorder. Perspectives on Psychological Science, 8(6), 651-662. [ Links ]
Giourou, E.; Skokou, M.; Andrew, S. P.; Alexopoulou, K.; Gourzis, P.; Jelastopulu, E. (2018). Complex posttraumatic stress disorder: the need to consolidate a distinct clinical syndrome or to reevaluate features of psychiatric disorders following interpersonal trauma?. World Journal of Psychiatry, 8(1), 12-19. [ Links ]
Gross-Jean (1855). Seconde lettre de GrosJean à son évêque au sujet des tables parlantes, des possessions, des Sybilles, du magnétisme et autres diabléries. Paris: Ledoyen. [ Links ]
Gur, R. C.; Gur, R. E. (2016). Social cognition as an RDoC domain. American Journal of Medical Genetics Part B: Neuropsychiatric Genetics, 171B, 132-141. [ Links ]
Hariri, A. G.; Gulec, M. Y.; Orengul, F. F.; Sumbul, E. A.; Elbay, R. Y.; Gulec, H. (2015). Dissociation in bipolar disorder: relationships between clinical variables and childhood trauma. Journal of Affective Disorders, 184, 104-110. [ Links ]
Harvey, A. G.; Bryant, R. A. (1999). Dissociative symptoms in acute stress disorder. Journal of Traumatic Stress, 12(4), 673-680. [ Links ]
Helmes, E.; Brown, J. M.; Elliott, L. (2015). A case of dissociative fugue and general amnesia with an 11-year follow-up. Journal of Trauma and Dissociation, 16(1), 100-113. [ Links ]
Herman, J. L. (1992). Complex PTSD: a syndrome in survivors of prolonged and repeated trauma. Journal of Traumatic Stress, 5(3), 377-391. [ Links ]
Hock, M.; Krohne, H. W. (2004). Coping with threat and memory for ambiguous information: testing the repressive discontinuity hypothesis. Emotion, 4, 65-86. [ Links ]
Holmes, E. A.; Brown, R. J.; Mansell, W.; Fearon, R. P.; Hunter, E. C.; Frasquilho, F.; Oakley, D. A. (2005). Are there two qualitatively distinct forms of dissociation? A review and some clinical implications. Clinical Psychology Review, 25, 1-23. [ Links ]
Hyman, S. E. (2010). The diagnosis of mental disorders: the problem of reification. Annual Review of Clinical Psychology, 6, 155-179. [ Links ]
Jacobs, J. R.; Bovasso, G. B. (1992). Toward the clarification of the construct of depersonalization and its association with affective and cognitive dysfunctions. Journal of Personality Assessment, 59(2), 352-365. [ Links ]
Jay, E. L.; Sierra, M.; Van den Eynde, F.; Rothwell, J. C.; David, A. S. (2014). Testing a neurobiological model of depersonalization disorder using repetitive transcranial magnetic stimulation. Brain Stimulation, 7(2), 252-259. [ Links ]
Kienle, J.; Rockstroh, B.; Bohus, M.; Fiess, J.; Huffziger, S.; Steffen-Klatt, A. (2017). Somatoform dissociation and posttraumatic stress syndrome: two sides of the same medal? A comparison of symptom profiles, trauma history and altered affect regulation between patients with functional neurological symptoms and patients with PTSD. BMC Psychiatry, 17, 248. [ Links ]
Knefel, M.; Tran, U. S.; Lueger-Schuster, B. (2016). The association of posttraumatic stress disorder, complex posttraumatic stress disorder, and borderline personality disorder from a network analytical perspective. Journal of Anxiety Disorders, 43, 70-78. [ Links ]
Kose, S.; Cetin, M. (2017). The Research Domain Criteria framework: transitioning from dimensional systems to integrating neuroscience and psychopathology. Psychiatry and Clinical Psychopharmacology, 27, 1-5. [ Links ]
Kozak, M. J.; Cuthbert, B. N. (2016). The NIMH Research Domain Criteria Initiative: background, issues, and pragmatics. Psychophysiology, 53(3), 286-297. [ Links ]
Krause-Utz, A.; Elzinga, B. (2018). Current understanding of the neural mechanisms of dissociation in borderline personality disorder. Current Behavioral Neuroscience Reports, 5(1), 113-123. [ Links ]
Krueger, R. F.; Markon, K. E. (2014). The role of the DSM-5 personality trait model in moving toward a quantitative and empirically based approach to classifying personality and psychopathology. Annual Review of Clinical Psychology, 10, 477-501. [ Links ]
Lanius, R. A. (2015). Trauma-related dissociation and altered states of consciousness: a call for clinical, treatment, and neuroscience research. European Journal of Psychotraumatology, 6, 27905. [ Links ]
Lanius, R. A.; Bluhm, R.; Lanius, U.; Pain, C. (2006). A review of neuroimaging studies in PTSD: heterogeneity of response to symptom provocation. Journal of Psychiatric Research, 40, 709-729. [ Links ]
Lanius, R. A.; Brand, B.; Vermetten, E.; Frewen, P. A.; Spiegel, D. (2012). The dissociative subtype of posttraumatic stress disorder: rationale, clinical and neurobiological evidence, and implications. Depression and Anxiety, 29(8), 701-708. [ Links ]
Lanius, R. A.; Williamson, P. C.; Boksman, K.; Densmore, M.; Gupta, M.; Neufeld, R. W.; Gati, J. S.; Menon R. S. (2002). Brain activation during script-driven imagery induced dissociative responses in PTSD: a functional magnetic resonance imaging investigation. Biological Psychiatry, 52(4), 305-311. [ Links ]
Lanius, U. F.; Paulsen, S. L.; Corrigan, F. M. (2014). Neurobiology and treatment of traumatic dissociation: toward an embodied self. New York: Springer. [ Links ]
Lawton G.; Baker, G. A.; Brown, R. J. (2008). Comparison of two types of dissociation in epileptic and nonepileptic seizures. Epilepsy and Behavior, 13(2), 333-336. [ Links ]
LeDoux, J. E. (2015). Anxious: using the brain to understand and treat fear and anxiety. New York: Viking. [ Links ]
Levin, R.; Sirof, B.; Simeon, D.; Guralnick, O. (2004). Role of fantasy proneness, imaginative involvement, and psychological absorption in depersonalization disorder. Journal of Nervous and Mental Disease, 192(1), 69-71. [ Links ]
Lovern, J. (2012). Posthypnotic state changes and flashbacks: analogous processes?. Journal of Trauma Dissociation, 13(5), 568-581. [ Links ]
Ludäscher, P.; Valerius, G.; Stiglmayr, C.; Mauchnik, J.; Lanius, R. A.; Bohus, M.; Schmahl, C. (2010). Pain sensitivity and neural processing during dissociative states in patients with borderline personality disorder with and without comorbid posttraumatic stress disorder: a pilot study. Journal of Psychiatry and Neuroscience, 35(3), 177-184. [ Links ]
Ludwig, A. M. (1966). Altered states of consciousness. Archives of General Psychiatry, 15, 225-234. [ Links ]
Ludwig, A. M. (1983). The psychobiological functions of dissociation. American Journal of Clinical Hypnosis, 26(2), 93-99. [ Links ]
Lynn, S. J.; Rhue, J. W. (1994). Dissociation: clinical and theoretical perspectives. New York: Guilford Press. [ Links ]
Lyssenko, L.; Schmahl, C.; Bockhacker, L.; Vonderlin, R.; Bohus, M.; Kleindienst, N. (2018). Dissociation in psychiatric disorders: a meta-analysis of studies using the Dissociative Experiences Scale. American Journal of Psychiatry, 175(1), 37-46. [ Links ]
Maj, M. (2005). Psychiatric comorbidity: an artefact of current diagnostic systems?. British Journal of Psychiatry, 186, 182-184. [ Links ]
Marmar, C. R.; Weiss, D. S.; Metzler, T. J. (1997). The Peritraumatic Dissociative Experiences Questionnaire. In: Wilson, J. P.; Keane, T. M. (eds.). Assessing psychological trauma and PTSD, p. 412-428. New York: Guilford Press. [ Links ]
McNally, R. J.; Robinaugh, D. J.; Wu, G. W. Y.; Wang, L.; Deserno, M.; Borsboom, D. (2015). Mental disorders as causal systems: a network approach to posttraumatic stress disorder. Clinical Psychological Science, 3, 836-849. [ Links ]
Miller, M. E.; Bowers, K. S. (1993). Hypnotic analgesia: dissociated experience or dissociated control?. Journal of Abnormal Psychology, 102(1), 29-38. [ Links ]
Moghaddas, A.; Dianatkhah, M.; Ghaffari, S.; Ghaeli, P. (2017). The potential role of naltrexone in borderline personality disorder. Iranian Journal of Psychiatry, 12(2), 142-146. [ Links ]
Moskowitz, A. (2011). Schizophrenia, trauma, dissociation, and scientific revolutions. Journal of Trauma and Dissociation, 12(4), 347-357. [ Links ]
Mueller-Pfeiffer, C.; Moergeli, H.; Schumacher, S.; Martin-Soelch, C.; Wirtz, G.; Fuhrhans, C.; Hindermann, E.; Rufer, M. (2013). Characteristics of child maltreatment and their relation to dissociation, posttraumatic stress symptoms, and depression in adult psychiatric patients. Journal of Nervous and Mental Disease, 201, 471-477. [ Links ]
Murray, J.; Ehlers, A.; Mayou, R. A. (2002). Dissociation and post-traumatic stress disorder: two prospective studies of road traffic accident survivors. British Journal of Psychiatry, 180(4), 363-368. [ Links ]
Myers, C. S. (1940). Shell shock in France 1914-18. Cambridge: Cambridge University Press. [ Links ]
Myers, F. W. H. (1893). The subliminal consciousness: Chapter 6. The mechanism of hysteria. Proceedings of the Society for Psychical Research, 9, 3-25. [ Links ]
Nijenhuis, E. R.; Vanderlinden, J.; Spinhoven, P. (1998). Animal defensive reactions as a model for trauma-induced dissociative reactions. Journal of Traumatic Stress, 11(2), 243-260. [ Links ]
Pai, A.; Suris, A. M.; North, C. S. (2017). Posttraumatic stress disorder in the DSM-5: controversy, change, and conceptual considerations. Behavioral Sciences, 7(1), E7. [ Links ]
Peres, J. F.; Moreira-Almeida, A.; Caixeta, L.; Leao, F.; Newberg, A. (2012). Neuroimaging during trance state: a contribution to the study of dissociation. PLoS One, 7(11), e49360. [ Links ]
Pick, S.; Mellers, J. D.; Goldstein, L. H. (2017). Dissociation in patients with dissociative seizures: relationships with trauma and seizure symptoms. Psychological Medicine, 47(7), 1215-1229. [ Links ]
Porges, S. W. (2011). The polyvagal theory: neurophysiological foundations of emotions, attachment, communication, and self-regulation. New York: WW Norton. [ Links ]
Powers, M. B.; Halpern, J. M.; Ferenschak, M. P.; Gillihan, S. J.; Foa, E. B. (2010). A meta-analytic review of prolonged exposure for posttraumatic stress disorder. Clinical Psychology Review, 30, 635-641. [ Links ]
Putnam, F. W. (1985). Dissociation as a response to extreme trauma. In: Kluft, R. P. (ed.). Childhood antecedents to multiple personality, p. 66-97. Washington, DC: American Psychiatric Press. [ Links ]
Putnam, F. W.; Carlson, E. B.; Ross, C. A.; Anderson, G.; Clark, P.; Torem, M.; Bowman, E. S.; Coons, P.; Chu, J. A.; Dill, D. L.; Loewenstein, R. J.; Braun, B. G. (1996). Patterns of dissociation in clinical and nonclinical samples. Journal of Nervous and Mental Disease, 184, 673-679. [ Links ]
Rauch, S. A.; Eftekhari, A.; Ruzek, J. I. (2012). Review of exposure therapy: a gold standard for PTSD treatment. Journal of Rehabilitation Research and Development, 49(5), 679-687. [ Links ]
Regier, D. A.; Kuhl, E. A.; Kupfer, D. J. (2013). The DSM-5: classification and criteria changes. World Psychiatry, 12, 92-98. [ Links ]
Reinders, A. A. T. S.; Nijenhuis, E. R. S.; Paans, A. M. J.; Korf, J.; Willemsen, A. T. M.; den Boer, J. A. (2003). One brain, two selves. NeuroImage, 20(4), 2119-2125. [ Links ]
Richet, C. (1884). L'homme et l'intelligence: fragments de physiologie et de psychologie. Paris: Alcan. [ Links ]
Sanders, S. (1986). The Perceptual Alteration Scale: a scale measuring dissociation. American Journal of Clinical Hypnosis, 29(2), 95-102. [ Links ]
Sar, V. (2014). The many faces of dissociation: opportunities for innovative research in psychiatry. Clinical Psychopharmacology and Neuroscience, 12(3), 171-179. [ Links ]
Sar, V.; Ross, C. (2006). Dissociative disorders as a confounding factor in psychiatric research. Psychiatric Clinics of North America, 29(1), 129-144. [ Links ]
Sar, V.; Ross, C. A. (2014). A research agenda for the dissociative disorder field. In: Dell, P. F.; O'Neil, J. A. (eds.). Dissociation and the dissociative disorders: DSM-V and beyond, p. 693-708. New York: Routledge. [ Links ]
Sar, V.; Dorahy, M. J.; Krüger, C. (2017). Revisiting the etiological aspects of dissociative identity disorder: a biopsychosocial perspective. Psychology Research and Behavior Management, 10, 137-146. [ Links ]
Sar, V. M.; Alioğlu, F. M.; Akyuz, G. M.; Tayakısı, E.; Öğülmüş, E. F.; Sönmez, D. (2017). Awareness of identity alteration and diagnostic preference between borderline personality disorder and dissociative disorders. Journal of Trauma Dissociation, 18(5), 693-709. [ Links ]
Schäflein, E.; Sattel, H.; Schmidt, U.; Sack, M. (2018a). The enemy in the mirror: self-perception-induced stress results in dissociation of psychological and physiological responses in patients with dissociative disorder. European Journal of Psychotraumatology, 9(Suppl. 3), 1472991. [ Links ]
Schäflein, E.; Sattel, H. C.; Pollatos, O.; Sack, M. (2018b). Disconnected: impaired interoceptive accuracy and its association with self-perception and cardiac vagal tone in patients with dissociative disorder. Frontiers in Psychology, 9, 897. [ Links ]
Scheiderer, E. M.; Wood, P. K.; Trull, T. J. (2015). The comorbidity of borderline personality disorder and posttraumatic stress disorder: revisiting the prevalence and associations in a general population sample. Borderline Personality Disorder and Emotion Dysregulation, 2, 11. [ Links ]
Schimmenti, A. (2016). Dissociative experiences and dissociative minds: exploring a nomological network of dissociative functioning. Journal of Trauma and Dissociation, 17, 338-361. [ Links ]
Schmidt, U.; Vermetten, E. (2017). Integrating NIMH research domain criteria (RDoC) into PTSD research. Current Topics in Behavioral Neuroscience, 38, 69-91. [ Links ]
Sierra, M.; David, A. S. (2011). Depersonalization: a selective impairment of self-awareness. Consciousness and Cognition, 20(1), 99-108. [ Links ]
Simeon, D.; Smith, R. J.; Knutelska, M.; Smith, L. M. (2008). Somatoform dissociation in depersonalization disorder. Journal of Trauma and Dissociation, 9(3), 335-348. [ Links ]
Soffer-Dudek, Nirit; Lassri, D.; Soffer-Dudek, Nir; Shahar, G. (2015). Dissociative absorption: an empirically unique, clinically relevant, dissociative factor. Consciousness and Cognition, 36, 338-351. [ Links ]
Sperandeo, R.; Monda, V.; Messina, G.; Carotenuto, M.; Maldonato, N. M.; Moretto, E.; Leone, E.; De Luca, V.; Monda, M.; Messina, A. (2017). Brain functional integration: an epidemiologic study on stress-producing dissociative phenomena. Neuropsychiatric Disease and Treatment, 14, 11-19. [ Links ]
Spiegel, D. (2006). Recognizing traumatic dissociation. American Journal of Psychiatry, 163(4), 566-568. [ Links ]
Spiegel, D.; Cardeña, E. (1991). Disintegrated experience: the dissociative disorders revisited. Journal of Abnormal Psychology, 100(3), 366-378. [ Links ]
Spiegel, D.; Koopman, C.; Classen, C. (1994). Acute stress disorder and dissociation. Australian Journal of Clinical and Experimental Hypnosis, 22(1), 11-23. [ Links ]
Spiegel, D.; Lewis-Fernández, R.; Lanius, R.; Vermetten, E.; Simeon, D.; Friedman, M. (2013). Dissociative disorders in DSM-5. Annual Review of Clinical Psychology, 9, 299-326. [ Links ]
Spiegel, D.; Loewenstein, R. J.; Lewis-Fernandez, R.; Sar, V.; Simeon, D.; Vermetten, E.; Cardeña, E.; Brown, R. J.; Dell, P. F. (2011). Dissociative disorders in DSM-5. Depression and Anxiety, 28(12), E17-E45. [ Links ]
Spiegel, H. (1963). The dissociation-association continuum. Journal of Nervous and Mental Disease, 136(4), 374-378. [ Links ]
Spitzer, C.; Spelsberg, B.; Grabe, H. J.; Mundt, B.; Freyberger, H. J. (1999). Dissociative experiences and psychopathology in conversion disorders. Journal of Psychosomatic Research, 46(3), 291-294. [ Links ]
Sporns, O. (2011). The human connectome: a complex network. Annals of the New York Academy of Sciences, 1224, 109-125. [ Links ]
Stein, D. J.; Koenen, K. C.; Friedman, M. J.; Hill, E.; McLaughlin, K. A.; Petukhova, M.; Ruscio, A. M.; Shahly, V.; Spiegel, D.; Borges, G.; Bunting, B.; Caldas-de-Almeida, J. M.; de Girolamo, G.; Demyttenaere, K.; Florescu, S.; Haro, J. M.; Karam, E. G.; Kovess-Masfety, V.; Lee S.; Matschinger, H.; Mladenova, M.; Posada-Villa, J.; Tachimori, H.; Viana, M. C.; Kessler, R. C. (2013). Dissociation in posttraumatic stress disorder: evidence from the World Mental Health Surveys. Biological Psychiatry, 73, 302-312. [ Links ]
Sundermann, J. M.; Chu, A. T.; DePrince, A. P. (2013). Cumulative violence exposure, emotional nonacceptance, and mental health symptoms in a community sample of women. Journal of Trauma and Dissociation, 14(1), 69-83. [ Links ]
Tarnopolsky, A. (2003). The concept of dissociation in early psychoanalytic writers. Journal of Trauma and Dissociation, 4, 7-25. [ Links ]
Tart, C. T. (1969). Altered states of consciousness. New York: Wiley. [ Links ]
Tascher, P. (1855). Seconde Lettre de Gros-Jean à Son Évèque au Sujet des Tables Parlantes, des Possessions, des Sibylles, du Magnétisme et Autres Diableries. Paris: Ledoyen. [ Links ]
Thompson, E.; Zahavi, D. (2007). Philosophical issues: phenomenology. In: Zelazo, P. D.; Moscovitch, M.; Thompson, E. (eds.). The Cambridge handbook of consciousness, p. 67-88. New York: Cambridge University Press. [ Links ]
Tononi G. (2015). Integrated information theory. Scholarpedia, 10, 4164. [ Links ]
van der Hart, O.; Bolt, H.; van der Kolk, B. A. (2005). Memory fragmentation in dissociative identity disorder. Journal of Trauma and Dissociation, 6(1), 55-70. [ Links ]
van der Hart, O.; Boon, S. (1997). Treatment strategies for complex dissociative disorders: two Dutch case examples. Dissociation: Progress in the Dissociative Disorders, 10(3), 157-165. [ Links ]
van der Hart, O.; Brown, P. (1992). Abreaction re-evaluated. Dissociation, 5, 127-140. [ Links ]
van der Hart, O.; Horst, R. (1989). The dissociation theory of Pierre Janet. Journal of Traumatic Stress, 2(4), 397-412. [ Links ]
van der Hart, O.; Nijenhuis, E. R. S.; Steele, K. (2006). The haunted self: structural dissociation and the treatment of chronic traumatization. New York: W. W. Norton. [ Links ]
van der Hart, O.; Nijenhuis, E. R. S.; Steele, K.; Brown, D. (2004). Trauma-related dissociation: conceptual clarity lost and found. Australian and New Zealand Journal of Psychiatry, 38(11-12), 906-914. [ Links ]
van der Hart, O.; Witztum, E.; Friedman, B. (1993). From hysterical psychosis to reactive dissociative psychosis. Journal of Traumatic Stress, 6(1), 43-64. [ Links ]
van der Kolk, B. A. (2014). The body keeps the score: brain, mind and body in the healing of trauma. New York: Viking. [ Links ]
van der Kruijs, S. J.; Bodde, N. M.; Carrette, E.; Lazeron, R. H.; Vonck, K. E.; Boon, P. A.; Langereis, G. R.; Cluitmans, P. J.; Feijs, L. M.; Hofman, P. A.; Backes, W. H.; Jansen, J. F.; Aldenkamp, A. P. (2014). Neurophysiological correlates of dissociative symptoms. Journal of Neurology, Neurosurgery and Psychiatry, 85(2), 174-179. [ Links ]
van Dijke, A.; Hopman, J. A. B.; Ford, J. D. (2018). Affect dysregulation, psychoform dissociation, and adult relational fears mediate the relationship between childhood trauma and complex posttraumatic stress disorder independent of the symptoms of borderline personality disorder. European Journal of Psychotraumatology, 9(1), 1400878. [ Links ]
van Duijl, M.; Nijenhuis, E.; Komproe, I. H.; Gernaat, H. B.; de Jong, J. T. (2010). Dissociative symptoms and reported trauma among patients with spirit possession and matched healthy controls in Uganda. Culture, Medicine and Psychiatry, 34(2), 380-400. [ Links ]
Vermetten, E.; Dorahy, M. J.; Spiegel, D. (2007). Traumatic dissociation: neurobiology and treatment. Arlington: American Psychiatric Publishing. [ Links ]
Vermetten, E.; Spiegel, D. (2014). Trauma and dissociation: implications for borderline personality disorder. Current Psychiatry Reports, 16(2), 434. [ Links ]
Wolf, E. J.; Lunney, C. A.; Miller, M. W.; Resick, P. A.; Friedman, M. J.; Schnurr, P. P. (2012). The dissociative subtype of PTSD: a replication and extension. Depression and Anxiety, 29, 679-688. [ Links ]
World Health Organization (1979). International statistical classification of diseases, injuries, and causes of death, 9th revision. Geneva: World Health Organization. [ Links ]
World Health Organization (2004). International Statistical Classification of Diseases and Related Health Problems, 10th revision. Geneva: World Health Organization. [ Links ]
World Health Organization (2018). International Statistical Classification of Diseases and Related Health Problems, 11th revision. Geneva: World Health Organization. [ Links ]
Young, G. B.; Pigott, S. E. (1999). Neurobiological basis of consciousness. Archives of Neurology, 56, 153-157. [ Links ]
Recebido em 30 de julho de 2018
Aceito para publicação em 16 de setembro de 2018

