










Servicios Personalizados
Revista

Articulo
 Inglés (pdf)
Inglés (pdf)
 Articulo en XML
Articulo en XML Referencias del artículo
Referencias del artículo
 Curriculum ScienTI
Curriculum ScienTIIndicadores
Compartir

 Permalink
PermalinkJournal of Human Growth and Development
versión impresa ISSN 0104-1282
Rev. bras. crescimento desenvolv. hum. vol.24 no.3 São Paulo 2014
ORIGINAL RESEARCH
The importance of congenital malformations at birth
Ruy LaurentiI; Arnaldo Augusto Franco de SiqueiraII; M. Helena P. de Mello JorgeI; Sabina Lea Davidson GotliebI; Elaine Cristina PimentelIII
IDepartment of Epidemiology of the School of Public Health/USP
IIDepartment of Maternal and Child Health of the School of Public Health/USP
IIIResident in Obstetrical Nursing - School of Nursing/USP
ABSTRACT
INTRODUCTION: Countries that have overcome high infant mortality rates show, nowadays, concentration of deaths in the neonatal period and, within it, mainly in the first week of life (early neonatal deaths). Regarding causes of death, as some diseases have started to be controlled, a significant proportional increase in the participation of congenital malformations has been verified.
OBJECTIVE: To describe the prevalence of congenital malformations (CM) at birth in conceptuses (stillbirths and live births) of women hospitalized in institutions located in the city of São Paulo, Brazil.
METHODS: Descriptive, cross-sectional study carried out at 4 hospitals in the city of São Paulo during 3 months in the 2nd semester of 2011. Data were collected by means of interviews with the women and examinations of hospital records. The CM were studied according to variables of epidemiological and socio-demographic interest. The deaths were analyzed according to underlying and associated causes.
RESULTS: The results showed the occurrence of 9.1% of CM registered among stillbirths and 4.3% among live births. Among the latter - 238 newborns - 284 CM were registered, totaling 1.2 CM per live birth with CM registered. Among the 238 newborns that had a CM register, there were 10 deaths by CM (4.2%). This value differs from the one verified among the live births without CM register that died (19 out of 5,341 or 0.4%). Aiming to identify possible occurrences of death after hospital discharge, a linkage was performed between the official mortality database of the city of São Paulo and the study's database. The occurrence of 18 deaths was found in this way, 4 of which were caused by CM. Thus, the total of deaths in the 1st year of life was 47, and 14 of them had CM as the underlying cause, which leads to a proportional infant mortality by CM equal to 29.8% and an infant mortality coefficient by CM of 2.5%o live births. The data show a high undercount of CM in the registers of the official information systems (regarding SINASC, the prevalence of CM in the study was three times the prevalence for the city of São Paulo and 5.4 times the prevalence for Brazil.
CONCLUSION: It is necessary to implement measures to improve the register of CM in the information systems, such as: raising doctors' awareness concerning the importance of diagnosing CM and registering it in the newborn's hospital records, creating a specific space to register the CM in the newborn's hospital records, and qualifying and monitoring the personnel in charge of filling in the Certificate of Live Birth and transcribing it to the information systems.
Key words: congenital malformations, live births and still births, maternal and child health.
INTRODUCTION
Countries that have overcome high infant mortality rates show, nowadays, concentration of deaths in the neonatal period and, within it, mainly in the first week of life (early neonatal deaths)1,2. Regarding causes of death, as some diseases have started to be controlled, a significant proportional increase in the participation of congenital malformations has been verified3.
This group of causes has been responsible for a non-negligible amount of deaths of infants and children younger than 5 years. In the United States, congenital malformations constitute the main cause of death in the first year of life2,4 and, in the period from 1968 to 1995, their frequency in mortality increased from 14% to 22%5. In order to know about and monitor congenital malformations, some countries have created information systems that reveal their prevalence and types6, independently of their behavior among deaths.
In Brazil, there is no special register for congenital malformations. Their occurrence is monitored by the Sistema de Informações sobre Mortalidade (SIM/MS - Mortality Information System/Ministry of Health). In 1989/90, when the Sistema de Informações sobre Nascidos Vivos (SINASC - Live Births Information System) was created, there was the intention to include a variable to register congenital malformations at birth in the Certificate of Live Birth; however, this occurred only in 19995,7. This information has been revealing, even though with fails, the frequency of this problem in the country, as well as its most common types. It is necessary to highlight that, according to values observed worldwide, the estimated frequency of congenital malformations at birth can vary between 2 and 5%8, although some authors have observed higher values. Official data for Brazil show a frequency of 0.8% in 2011, which demonstrates that the undercount of these registers in the country still exists and is still high9. In the city of São Paulo, where the Municipal Health Department has been encouraging hospitals to improve the quality of this information, the prevalence of congenital malformations among live births is around 1.5%10.
The frequency of malformations has been evaluated through mortality data, as it was mentioned before. Nevertheless, it is known that, in most cases, these problems are not causes of death, as some types of congenital malformations are mild and others, moderated. The latter are usually responsible for severe conditions, and they often lead to successive hospitalizations in order to correct birth defects, or to control their complications. Thus, these malformations interfere in the child's quality of life; furthermore, they cause family traumas and difficulty in adapting to society11. The World Report on Disability mentions that a "legion" of people experience disability in the world today as a result of congenital malformations12.
Congenital malformations or birth defects - CM - are morphological and/or functional alterations detectable at birth. Morphological or anatomical alterations range from mild dysmorphias to complex defects of organs or body segments13 and, depending on the condition, they may cause different clinical manifestations.
The nomenclature and classification of CM have a great variation: minor congenital malformations - more frequent in the population in general; most of the times, they do not cause problems to the individuals who have them - and major congenital malformations, with important consequences; they require specialized treatment and may leave sequelae13. This classification is adopted by the Estudo Colaborativo Latino-Americano de Mal Formações Congênitas (ECLAMC - Collaborative Latin American Study of Congenital Malformations).14 Their etiology, genetic study and determinants, although absolutely fundamental, will not be the object of this study.
This paper aims to analyze the occurrence of congenital malformations in newborns in hospitals in the city of Sao Paulo, in order to provide subsidies to a more complete view of its frequency, so that studies of this nature can be based on more complete and correct data.
METHODS
This is a cross-sectional and descriptive study, concerning parturients admitted to six maternity hospitals in the State of São Paulo15,16. Five of them were run by the Sistema Único de Saúde (SUS - Brazil's National Health System) or assisted patients through this System and one provided only private assistance. The study was carried out during three months in the second semester of 2011. All women hospitalized at the evaluated institutions in the period of data collection were invited to participate in the research and signed a consent document.
The data were obtained directly, in interviews with the hospitalized women, and collected from: hospital records, the delivery room register, the prenatal assistance card and similar documents, and they were recorded in a specific form. The women' socio-demographic variables were collected, as well as personal story, specific morbidity, and previous and current gestational story.
Concerning the conceptus, the variables that were considered were: sex; gestation's outcome (live birth/stillbirth); birth weight; type of delivery; presence of other diseases (according to the hospital records); type of outcome (discharge/death/transfer). Regarding the CM, their presence at birth was investigated and the information was extracted from the hospital records and from the delivery room register. The malformations were classified according to the ICD-10, both to live births and to stillbirths. The groupings and categories of the Chapter Congenital Malformations, Deformations and Chromosomal Abnormalities17 were used and, according to national and international determinations, some conditions classified in other Chapters13,14. For the newborns that died, the reasons for the deaths were studied by underlying or associated causes coded according to international rules17.
The research was funded by FAPESP (Proc. No. 09/53253-8) and it was authorized by the Research Ethics Committees of the School of Public Health of Universidade de São Paulo (USP) (Protocol no. 2188/11) and of each hospital that participated in the study.
For this paper, only the cases that occurred at four hospitals in the city of São Paulo, State of São Paulo, were selected, as it was possible, for these cases, to conduct a subsequent search of deaths among the live births of the study within one year after the delivery date. At the end of this period, the study's database was compared to the official mortality database (PROAIM - Municipal Health Department of São Paulo), in order to obtain what was called "subsequent death", that is, the death of the conceptus that occurred after it was discharged of the birth hospital.
Concerning the 5,623 conceptuses, the following aspects were verified: presence/absence of CM register, type of malformation and some characteristics of the mother, of the gestation, of the delivery and of the children themselves.
RESULTS
Figure 1 shows the distribution of the 5,623 conceptuses according to live birth or stillbirth, presence of CM register, the evolution of live births according to type of outcome, as well as deaths per CM.
Congenital malformations in stillbirths
There were 44 cases of stillbirths, of which 4 presented a register of CM at birth (9.1%). One case, although its cause of death was registered as "Multiple congenital malformations" and the gestational age was registered as 26 weeks, was not included in the study as stillbirth (rather, it was considered an abortion), as the weight was lower than 500g.
Some characteristics of the mother, of the gestation and of the delivery, as well as of the conceptuses themselves, are described on Table 1.
It is important to notice that, when a comparison was drawn to the official Declarations of Stillbirths, in 1 case this connection could not be made, as it was considered an abortion by the hospital; in 1 case, the underlying cause of teath was "unspecified", and in 2 cases (50%), the official information about the underlying cause of death confirmed the CM detected by the study.
Congenital malformations in live births
Among the live births - 5,579 -, it was verified that, regarding the number of malformations, of the 238 children who presented this condition (4.3%), 206 had 1 described congenital malformation (86.6%); 24 (10.1%) had 2; 5 (2.1%) had 3; 2 (0.8%) had 4; and 1 live birth had 7 congenital malformations registered in its hospital record (0.4%) (Table 2). The total number of registered malformations was 284 - a relationship of 1.2 CM per live birth with CM.
It is important to notice, however, that these CM include the cases of "cardiac murmur", to which there is no consensus concerning whether they should be considered CM or not. Overall, there were 42 cases of newborns in which there was only the register of "cardiac murmur" in the hospital records, without mention to other malformations. On the other hand, there were 6 cases in which the referred murmur was accompanied by another malformation. It is known that the existence of a delay in the closure of the ductus arteriosus is relatively frequent and this motivates the occurrence of a murmur which, after some days, may disappear. In these cases, therefore, there would not be, in fact, a congenital malformation, only a transitory and functional murmur that would disappear as soon as the ductus closes. Thus, if these cases are not included among the CM, the new (minimum) values become those presented on Table 3, in which the maximum values (with the inclusion of the murmur cases) can also be seen. Their frequencies were, respectively, 3.5% and 4.3%, and the average number of CM per live birth with malformation, 1.20 and 1.19, respectively.
Regarding the specified type of CM, it can be verified that, of the total number of referred CM, 214 (75.3%) were included in the Chapter Congenital Malformations, Deformations and Chromosomal Abnormalities (Chapter XVII of ICD-10) and 70 (24.7%) were coded outside this chapter, according to international recommendations. Table 4 specifies the different types of CM found in the 238 live births. The high proportion of CM of the musculoskeletal system stands out (28.9%), followed by CM of the genital organs (10.2%), of the circulatory system (9.5%), and CM of eye, ear, face and neck, with 7% (Table 4).
Concerning those considered CM but classified outside Chapter XVII of ICD-10, the most frequent was "cardiac murmur", mentioned above, followed by haemangioma, hydrocele and umbilical hernia.
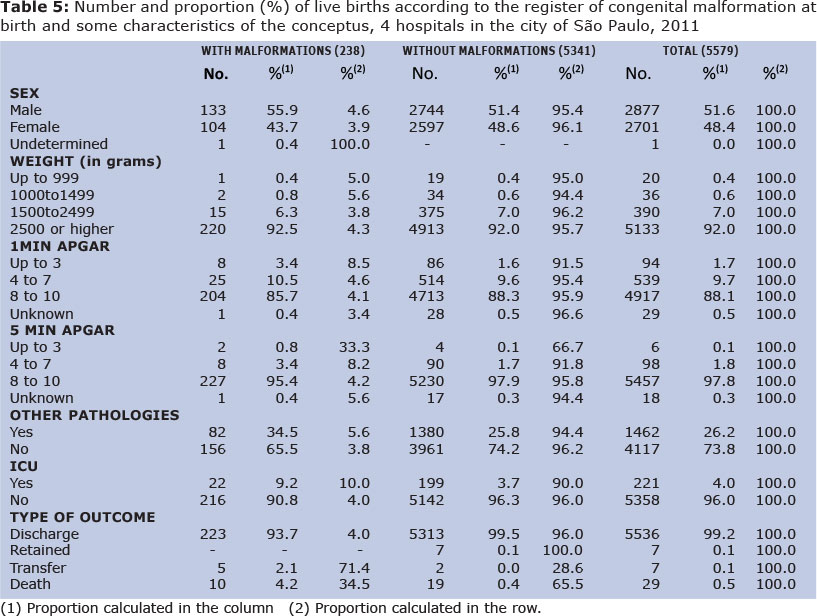
As for the occurrence of CM according to characteristics of the newborn (Table 5), 55.9% of the cases with malformations were boys and 43.7% were girls (1 case of undetermined sex due to the existent malformation). The distribution according to birth weight showed that, among the live births with low birth weight, 4% presented CM; no difference was noticed in relation to the cases of weight equal to or higher than 2,500g (4.3%). The occurrence of other associated pathologies also stands out - 34.5% among the infants with CM and 25.8% among the newborns without CM -, not to mention the need of ICU while they were at the hospitals in which they were born. More than twice the proportion of live births with CM register used ICU (9.2% compared to 3.7% for newborns without CM). Furthermore, the distribution of live births according to type of outcome is noteworthy: 99.5% of the children without CM were discharged and 0.4% died at the hospital where they were born, while in the group of live births with CM, 93.7% were discharged and there were 4.2% of deaths. Because of the need of treatment at a more specialized or more complex hospital, 2.1% (5 cases) of live births with CM were transferred and, among the 5,341 who did not have CM, only 2 cases were transferred.
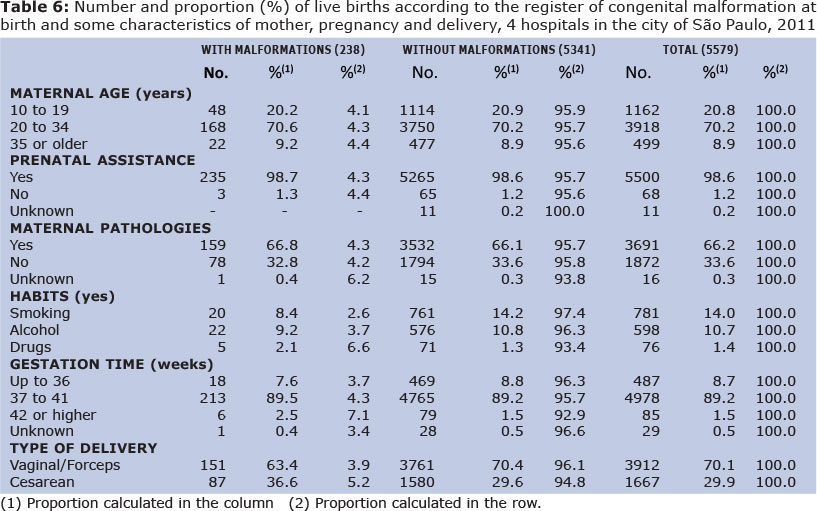
Concerning the variables related to the mothers (Table 6): maternal age, prenatal assistance and presence of pathologies, no differences were verified between live births with and without CM register.
Congenital malformations in the live births that died
Among the 238 live births that had registers of CM diagnosed at birth, 10 died due to this cause while they were still at the same hospital where they were born (here called "Stage I deaths"). These deaths represented 4.2% of the live births with CM, a proportion that is different from the one verified in the group of live births without CM, in which the relative frequency was 0.4%.
From the quantitative point of view, the deaths of newborns whose underlying cause was a congenital malformation represented 34.5% of the deaths of the study in the city of São Paulo (Figure 1, Stage I deaths).
After the comparison between the official database (PROAIM) and the study's database, 18 new deaths were identified in the cohort of live births of the study, referring to the newborns whose type of outcome was "discharge", "transfer" or newborns that remained hospitalized when the study was concluded (a group that was called "retained"). Among these cases, 4 deaths had a CM as underlying cause of death, and it is important to notice that all of them originated from the group that already presented a CM register at birth.
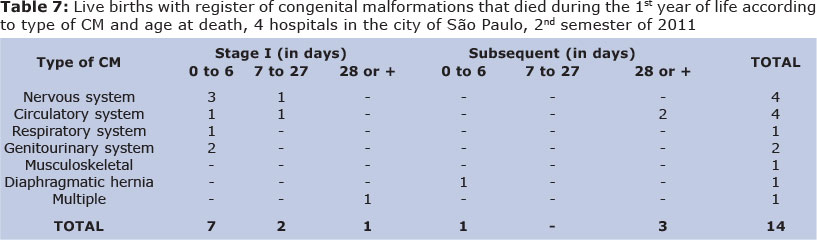
As for the specified causes (Table 7), it is possible to verify a higher frequency of CM of the nervous system, represented by cases of anencephaly and hydrocephalus, whose deaths occurred mainly in the early moments after delivery. In the subsequent deaths, CM of the circulatory system prevailed, signaling deaths that occurred more tardily (4 and 5 months).
There was 1 case of death (originated from the 228 with CM that were discharged) whose underlying cause of death was considered "undetermined"; however, it is important to mention that the study's form already recorded Moebius Syndrome (not registered in the opinion issued by the official Medical Service of Autopsies and not present in the official Death Certificate). On the other hand, it should be mentioned that, when the two databases (the study's and PROAIM) were compared, one case was selected by mistake in which the age was 1 year and 14 days. It is important to notice that, although the underlying cause of death was registered as CM (atrioventricular communica-tion), there was no record about it in the study's form.
Figure 1 also shows that, among the 5,579 live births of the study in the city of São Paulo, there was a total number of 47 deaths in the first year of life, of which 14 had a CM as the underlying cause. This means that the infant mortality coefficient by CM was 2.5 per one thousand live births and the proportional infant mortality by CM was 29.8%.
DISCUSSION
The frequency of CM has been calculated based on mortality information, and its increase has been observed (relative increase in infant deaths) as the infant mortality rate decreases. This has also been verified in deaths of children younger than five years - the data have shown that countries with lower rates present the highest proportions of CM as the cause of death. For example, in the years of 2000 and 2010, in developed countries, the values were: Germany, 33% and 31%; Austria, 38% and 32%; Australia, 17% and 22%. In less developed countries, the proportion of CM in the mortality of children younger than 5 years is much lower (Bolivia, 4% and 7%; Bangladesh, 4% and 7%; and Benin, 4% and 4%). In Brazil, it was observed that 13% (2000) and 19% (2010) of the deaths of children younger than 5 years were caused by CM18. However, knowledge about its prevalence in live births and stillbirths is still precarious, and that is why research studies like the one that is being presented here are important. The frequency of CM obtained in the study was 9.1% for stillbirths and 3.5% and 4.3% for live births, respectively without and with the inclusion of cases of cardiac murmur, as it was mentioned above. To calculate the number and the characteristics of the newborns, the cases of murmur were included, due to the fact that the evolution of each case is unknown, as it was commented.
Among the stillbirths, it is not possible to draw a comparison with other areas regarding its frequency or type, as not always are these conceptuses registered and, when they are, this aspect is not usually studied. Nevertheless, its high prevalence stands out, and it is possible to consider that, in fact, this value would be even higher, as the technological advances in the area of Fetal Medicine have enable the diagnosis of congenital intrauterine malformations, which, in turn, has been leading to a possible increase in cases of pregnancy interruption - eugenic abortion (see judicial authorizations in cases of anencephaly, for example). NAZER and col., 201119, from Universidad de Chile, studied urinary malformations in newborns based on ECLAMC data in the period from 1998 to 2010 (23495 live births and 194 stillbirths) and found 8.4% of CM in live births and 33.5% in stillbirths. In addition, the authors showed a remarkable increase in the prevalence of urinary malformations, from 0.93%o live births in 1971-77, to 15.5%o in 1982-97, and 69.5%o in the period 1998-2010. They attribute this increase to greater diagnostic precision, with the use of prenatal ultrasound, as, according to the authors, it is very difficult to make this diagnosis after birth.
It is important to recognize, like in the study conducted by LUQUETTI and KOIFMAN, 200920, that the frequency of CM at birth is much higher in hospitals that participate in the ECLAMC, possibly due to their interest and technical qualification targeted at searching for CM.
Concerning the live births, it is possible to state that the official data for Brazil and the city of São Paulo present values that are much lower than the one found in the study: for Brazil, 0.8% in 2011, higher in the South and Southeast and lower in the North and Central-West, and 1.5% for the city of São Paulo, according to data from the Sistema de Informação sobre Nascidos Vivos (SINASC - Live Birth Information System) for 20119.
It is important to highlight that, although the information provided by SINASC has been improving, the official data are still far from portraying the real situation of CM in the country.
Some hypotheses that have been raised to explain this situation are:
1) the obstetrician/pediatrician/neonatologist may not diagnose CM at birth;
2) the obstetrician/pediatrician/neonatologist diagnoses the CM, but may not write it down on the child's or mother's record, considering that there is no specific space for it;
3) when the doctor writes it down, the person who fills in the Certificate of Life Birth may not recognize all the CM as such, mainly the syndromes; therefore, he/she writes on the Certificate only the most common types or only those preceded by the expression "congenital malformation of…". Concerning this, the study conducted by Luquetti and Koifman20, mentioned above, comments that "the person responsible (for filling in the Certificate of Live Birth) may not know that trysomy 21 is the same as Down's syndrome". Minton and Seegmiller, 198621 found improvements in the quality of the information when the newborn's physician became responsible for the information about the case and a specially trained person was designated to fill in the Certificate of Live Birth. Qualifying the individuals responsible for this task in maternity hospitals could be valuable. In fact, Luquetti and Koifman evaluated, in their study, the quality of the information about birth defects at a reference hospital located in the city of Campinas (State of São Paulo), which has been participating in the ECLAMC for more than 20 years, and concluded that the information on CM provided by the Certificate of Live Birth still presents limitations regarding the accuracy of prevalence estimates20;
4) this study analyzed hospitals that provide care for a population that is assisted through the SUS; thus, it was expected that the register of CM on the record would be higher. At private hospitals, even in the presence of a congenital malformation, the families might ask the doctors not to register this condition on the hospital record/Certificate of Live Birth and, therefore, its frequency would be lower than the one verified at public hospitals;
5) the development of Fetal Medicine, which enables to detect congenital intrauterine malformations, could provoke an increase in the cases of abortion, which might be different depending on whether the population is assisted by SUS or not.
GEREMIAS and col., 200922, studying data from SIM and SINASC for the city of São Paulo, verified a 14.3% increase in the prevalence of CM in SINASC, based on the retrieval of data from SIM (linkage between SINASC - Live Births Information System - and SIM - Mortality Information System). They concluded that SINASC can be used as a source of data to monitor CM in the city of São Paulo and they believe that, although there has been an improvement, it is still necessary to enhance the quality of the register of CM in the Certificate of Live Birth.
MUÑOZ and col., 200123, in Colombia, based on data from VERACC, a local modality of the ECLAMC, analyzed the prevalence of CM in newborns at six hospitals in the period from 1982 to 1993. The prevalence at each hospital varied between 1.21% and 3.07% and the total prevalence for the six hospitals in the period was 1.81% of the newborns.
As for the types of CM, the most common among the live births were: malformations of the musculoskeletal system (28.9%), mainly CM of the hip-joint; CM of the genital organs (10.2%), mainly cryptorchidism; CM of the circulatory system (9.5%), among which the malformations of the cardiac chambers and congenital heart defects stand out; and malformations of the eye, ear, face and neck (7%), as well as those of the nervous system (4.9%), and chromosomal abnormalities (4.6%).
The fact that the register of the frequency of CM at birth is not adequate (nor complete, nor correct) has been extensively discussed, as what usually happens is that the CM that are registered are those which are more apparent or visible externally, and not necessarily the most severe ones. Although this argument is true, the distribution of the cases found in our study was very similar to that of other areas. In a recent study about epidemiological surveillance of CM, Luquetti and Koifman24 argue that the prevalence of CM has evidently been underestimated, and in a random way: many major CM are not registered due to the absence of a diagnosis in time for them to be registered on the Certificate of Live Birth, and many minor CM are not registered because they are considered unimportant. Finally, they emphasize the advantage of linking the Certificates of Live Births with other databases: Death Certificate, morbidity registers, hospitalization records, reports issued by specialized clinics and schools, for example. They conclude that the Certificate of Live Birth can be useful and it would serve as a baseline, that is, it would show the lower limit of prevalence of CM in a society.
Congenital malformations classified outside Chapter XVII totaled 24.7% and were represented, mainly, by hemangiomas, hydroceles and one case of a conceptus with diaphragmatic hernia which, transferred from the hospital where it was born to a more specialized one, died at the age of five days, during a surgery. The cases of cardiac murmur, with the reservations mentioned above, were present in 48 cases.
With regard to maternal and fetal characteristics, no differences were observed between mothers and conceptuses in the groups with and without CM register. In addition, as the sample was not a probability sample, the intention here was not to infer population trends. Thus, on Table 5, the distribution of frequencies in the two groups for the variables of the conceptus were very similar, except for type of outcome, in which the group with CM register presented 34.5% of deaths and the one without CM register, only 0.4%. On Table 6 (maternal variables), the values were also very similar in the two groups.
Concerning the cases of live births that died at the study's Stage I (deaths at the same hospital where the birth occurred), the total was 10 deaths with CM as underlying cause of deths, among the 29 deaths that occurred due to all causes (34.5%). At Stage II, which was constituted by a search for what was called here "subsequent deaths", 4 deaths by CM occurred within a total of 18 that could be captured (22.2%), and it is important to notice that all of them originated from the group "with CM register at birth". These values allowed to calculate the weight of the CM within the total number of deaths in the first year of life, which was equal to 29.8%.
Regarding the most common types of CM among the live births that died (Stage I and Stage II), there were 28.6% of cases of CM of the nervous system and the same value was verified for CM of the circulatory system; 14.3% for CM of the genitourinary system and of the respiratory system; multiple malformations, other malformations and umbilical hernia were represented by 7.1% each. These values differ from the distribution found for deaths by CM in Brazil concerning infants younger than one year: 38.8% were caused by CM of the circulatory system, 17.3% of the nervous system and 13.7% by other malformations (SIM, 2011) 25. However, concerning the CM of the nervous system and of the circulatory system, the differences found concerning age at death stand out: for the first group, 3 cases in the early neonatal period and 1 on the eighth day of life; for the second group, 1 day, 27 days and 4 and 5 months of life. These data clearly show the greater incompatibility of CM of the nervous system with life, in view of the existence of 3 cases of anencephaly and 1 of hydrocephalus.
As for the most common types of CM among the live births, the important presence of CM of the hip-joint and polydactyly was verified among the CM of the musculoskeletal system; cryptorchidism among the CM of the genital system; malformations of the cardiac chambers and congenital heart defects among the CM of the circulatory system; cleft palate; and anencephaly and hydrocephalus among the CM of the nervous system.
Concerning mortality by CM in infants younger than 1 year, of the 47 deaths that occurred among the studied live births - by all causes -, 14 had a CM as underlying cause of deths, corresponding to 29.8% (in 2011, this value was 20% in Brazil and 21.3% in the city of São Paulo - data obtained from the SIM database).
The present study aimed to investigate the distribution of CM among live births and stillbirths, products of gestations of women assisted for delivery at four hospitals in the city of São Paulo in the second semester of 2011.
Regarding frequency, the study showed that the SINASC data are underestimated: the value obtained in the study was three times the official datum for the city of São Paulo and 5.4 times that for Brazil. These values signal that the health authorities should strive, in the information area, to warn doctors of the importance of diagnosing and registering the CM in the hospital records, moreover, nurses and other professionals should be warned to "search" for CM in the records in a more detailed way and to register them in the Certificate of Live Birth, so that the System is able to perform, in its totality, the "task" that has been assigned to it.
The increasing relative importance of CM as cause of infant mortality - in this study, practically 30% of the infant deaths had a CM as underlying cause of deths - contrasts clearly with the poverty of actions, programs and policies targeted at the problem. Not to mention the high price paid besides the mortality issue: sequelae, malformations, surgeries, developmental delays, inclusion difficulties, high costs deriving from special needs throughout life, years of potential life lost.
It is not possible to ignore the difficulties to advance towards the enhancement of knowledge about the etiology (only 50% of the CM has identified causes), early diagnosis (intrauterine) and treatment of CM. Still, the mismatch between the importance and severity of the problem and the responses/proposals to face it seems evident. The generalized impression is that the Brazilian society still views CM as rare events whose etiology is not clear and which are difficult to prevent and much less important than problems like gastroenteritis, pneumonia, measles and polio. Above all, like many of the prenatal causes, they are viewed as "refractory" to public policies.
Aligned with other authors19-24, we recognize the importance of including, in the Certificate of Live Birth, a space for registering the occurrence of CM. Despite the advance that this has represented and in spite of the improvement that has been observed in the quality of the information that has been included in the Certificate, the reliability of the information about CM is still debatable. Measures to enhance the quality of its register in the Certificate of Life Birth and mainly in hospital records have become fundamental, with qualification programs and supervision of the inclusion of information. Thus, we would like to suggest, like Minton and Seegmiller21 did in 1981, the inclusion of a specific space (in the parturient's/conceptus' records) referring to the presence of CM in newborns, as well as the training of professionals, which has been extensively discussed.
It is important to recognize - and not only in our field - the need of studies, despite the methodological difficulties, that aim to better quantify and describe the CM, as well as to identify and estimate risk factors. After all, in spite of its "rarity", we are facing a problem that is responsible for almost one third of infant deaths; therefore, it should be faced as a true epidemic.
REFERENCES
1. Horovitz DDG, LlerenaJR JC, Mattos RA. Atenção aos defeitos congênitos no Brasil: panorama atual. Cad. Saúde Pública, Rio de Janeiro, 21(4): 1055-1064, 2005. [ Links ]
2. Amorim MMR, Vileza PC, Santos ARVD e col. Impacto das malformações congênitas na mortalidade perinatal e neonatal em uma maternidade escola do Recife. Rev. Brasil. Saúde Marterno-Infantil, V6 - Suplemento, Recife, 2006. [ Links ]
3. Ortiz LP,Camargo ABM. Mortalidade infantil no Estado em 2003. Resenha de Estatísticas Vitais do Estado de São Paulo, Fundação SEADE do Estado de São Paulo, 2004. [ Links ]
4. Paho: Pan American Health Organization Health Situation in the Americas. Basic Indicators. Washington, 2012. [ Links ]
5. Guerra FAR,Llerena JR, JC, Gama SGN e col. Defeitos Congênitos no Município do Rio de Janeiro, Brasil: uma avaliação através do SINASC (2000-2004). Cadernos de Saúde Pública, Rio de Janeiro, 24(1): 140-149, 2008. [ Links ]
6. Moratilla NA, Garcia AMG, Benavides FG. El conjunto mínimo básico de dados al alta hospita-laria como fuente da información para el estudo de las anomalias congênitas. Rev. Esp. Salud Publica, 73(1); Madrid, 1999. [ Links ]
7. Mello J, MHP, GotliebSLD, Soboll MLMS e col. Avaliação do Sistema de Informações sobre nascidos vivos - SINASC - e o uso de seus dados em epidemiologia e estatísticas de saúde. Rev. Saúde Pública, São Paulo, 27(1), 1993. [ Links ]
8. Pinto CO,Nascimento LFC. Estudo da prevalência de defeitos congênitos no Vale do Paraíba Paulista. Rev. Paulista Pediatria, 25(3), 2007. [ Links ]
9. MS/SINASC: Ministério da Saúde. Sistema de Informações sobre Nascidos Vivos (disponívelem: http://www2.datasus.gov.br/DATASUS/index.php?area=0205&VObj=http://tabnet.datasus.gov.br/cgi/deftohtm.exe?sinasc/cnv/nv). [ Links ]
10. SÃO PAULO:Secretaria Municipal de Saúde, CEINFO São Paulo, 2013. [ Links ]
11. Polita NB,Ferrari RA,Moraes PS e col. Anomalias congênitas: internações em unidades pediátricas. Rev. Paulista de Pediatria, 2013: 31(2): 205-10. [ Links ]
12. OMS: Organização Mundial da Saúde. Relatório Mundial sobre Deficiência (Trad. Secretaria dos Direitos da Pessoa com Deficiência, São Paulo, 2011. [ Links ]
13. SÃO PAULO: Secretaria Municipal de Saúde. CEINFO. Manual de aperfeiçoamento no Diagnóstico de Anomalias Congênitas. São Paulo, 2012. [ Links ]
14. ECLANC: Estudo Colaborativo Latino-Americano sobre Anomalias Congênitas, disponível em: http://www.eclamc.org. [ Links ]
15. Mello J, MHP, LaurentiR,GotliebSLD, Oliveira BZ, PimentelEC. Características das gestações de adolescentes internadas em maternidades do Estado de São Paulo, 2011. Epidemiol. Serv. Saúde. Brasília. 23(1) 45-56,jan-mar 2014. [ Links ]
16. Laurenti R, Siqueira AAF, Mello J, MHP, Gotlieb SLD, Pimentel EC. Perinatal Mortality in hospitals of the state of São Paulo: methodological aspects and some characteristics of mothers and conceptuses. Journal of Human Growth and Development. 2013, 23(3): 261-269. [ Links ]
17. OMS: Organização Mundial da Saúde. Classificação Estatística Internacional de Doenças e Problemas Relacionados à Saúde. 10ª Revisão. Centro Brasileiro de Classificação de Doenças, São Paulo, 1996. [ Links ]
18. Organizacion Mundial de la Salud. Estatisticas Sanitarias, 2012. Geneva, 2012. [ Links ]
19. Nazer JH, Cifuentes LO, Ramirez CR. Malformações urinárias delrecién nascido. Estudo ECLAMC 1998 - 2010. Revista Chilena de Pediatria, 2011, 82 (6): 512 - 519. [ Links ]
20. LuquettiDV,KoifmanRJ. Quality of reporting on birth defects in birth certificados: case study from a Brazilian reference hospital. Cad. Saúde Pública, Rio de Janeiro, 25 (8): 1721 - 1731, ago, 2009. [ Links ]
21. Minton SD,SeegmillerRE. An improved system for reporting congenital malformation. JAMA, Dec 5, 1986 - v. 256 nº 21. [ Links ]
22. Geremias AL, Almeida MF, Flores LPO. Avaliação das declarações de nascidos vivo com fonte de informação sobre defeitos congênitos. Rev. Bras. Epidemiol., 2009; 12(1): 60 - 68. [ Links ]
23. Muñoz J, Bustus I, Quintero C ,Giraldo A. Fac-tores de riesgo para algumas anomalías congénitas em población colombiana. Rev. Salud Pública, 3(3): 268 - 282, 2001. [ Links ]
24. Luquetti DV, Koifman RJ. Surveillance of birth defects: Brazil and the US. Ciência e Saude Coletiva. 16 (supl. 1) 777 - 785, 2011. [ Links ]
Manuscript submitted Aug 07 2014
Accepted for publication Sep 26 2014
Corresponding author: afsiqueira@uol.com.br

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}