










Servicios Personalizados
Revista

Articulo
 Inglés (pdf)
Inglés (pdf)
 Articulo en XML
Articulo en XML Referencias del artículo
Referencias del artículo
Indicadores
Compartir

 Permalink
PermalinkJournal of Human Growth and Development
versión impresa ISSN 0104-1282versión On-line ISSN 2175-3598
J. Hum. Growth Dev. vol.26 no.1 São Paulo 2016
https://doi.org/10.7322/jhgd.113733
ORIGINAL RESEARCH
Suicidal behaviour in adolescents: characteristics and prevalence
Carlos Alencar Souza Alves Junior*; Heloyse Elaine Gimenes Nunes; Eliane Cristina de Andrade Gonçalves; Diego Augusto Santos Silva
Universidade Federal de Santa Catarina (UFSC) - Florianópolis (SC), Brasil
ABSTRACT
INTRODUCTION: Suicide refers to the conscious desire to die, and suicidal behavior is divided into three stages (thinking, planning and attempted suicide).
OBJECTIVE: To estimate the prevalence of thinking, planning and suicide attempt and identify the sociodemographic characteristics and lifestyle among adolescents in southern Brazil.
METHODS: Cross-sectional study with 1,132 adolescents from public schools in São José, Santa Catarina, Brazil, aged 14-19 years. The thinking, planning and attempted suicide were evaluated by three different questions, taken from the questionnaire Youth Risk Behavior Survey (YRBS). The independent variables were gender, age, skin color, economic status, sleep quality, perception of body weight, level of physical activity and alcohol consumption.
RESULTS: The prevalence of thinking, planning and attempted suicide were respectively 13.8%, 10.5% and 5.5%. Neither crude nor adjusted analysis, the younger adolescents (14-16 years) had the characteristic of suicidal thinking. Teens who slept well had not characteristic they thought, planning and suicide attempt. Finally, adolescents with poor perception of body weight had the characteristic of suicidal thinking.
CONCLUSION: Adolescents with suicidal thinking presented characteristic of being young and having inadequate body weight perception. One in ten teenagers thought and planned suicide. Regarding suicide attempt, the ratio was less than one. In addition, adolescents affected by thinking, planning and suicide attempt, had the characteristic not sleep well.
Keywords: suicide, suicidal ideation, adolescent, cross-sectional studies.
INTRODUCTION
Suicide refers to the conscious desire to die and the consequences that such an act can generate1. Suicidal behaviour is divided into three stages (thinking, planning and attempted suicide). An individual who commits suicide, can demonstrates earlier signs of being a threat to their own life, following these steps1. Suicide is a global public health problem: it is among the 10 leading causes of death in all age groups in the global population2.
In adolescents, suicidal behaviours occur due to conflicts characteristic of adolescence, through physical and sociocultural transformations, favouring increased levels of anxiety and depression, the main risk factor for suicide2. Thus, the period of adolescence is considered as having higher vulnerability to suicidal behaviours1.
Each year, more than a million people in the world commit suicide3. The prevalence of suicide in children and adolescents in Brazil increased between 2000 and 2010, from 0.9 to 1.1 per 100,000 children and teenagers, putting Brazil 60 out of 98 countries; a relatively good situation when compared to other countries4. In Brazil, the southern region has higher than average suicidal behaviour when compared to other regions of the country1,2.
Studies show that the characteristics of adolescents with suicidal behaviours are that they are male, over 18 years old, with black skin colour, and a high economic status3-5. However, research has shown contrary data, presenting adolescents with suicidal behaviours with different characteristics: female, age less than 18 years, white skin colour and from a poor economic background6-8. The sociodemographic characteristics in adolescents with suicidal behaviours are controversial, raising the need for further investigations for a better understanding of this phenomenon1.
Among the lifestyle factors, not sleeping well, poor perception of body weight, physical inactivity, and high intake of alcoholic drinks are characteristics of adolescents with suicidal behaviours6,9-11. The identification of these modifiable factors is useful in order to anticipate and apply appropriate interventions to prevent these3 behaviours. However, these factors may not be universal3. For this reason, studies allowing the assessment of lifestyle factors for suicidal behaviours are needed in several localities of Brazil, a country with great cultural diversity3.
Individuals affected by suicidal behaviour show different demographic characteristics: economic, social, cultural, and lifestyle3,12. The identification of these characteristics in different places make it possible to identify the individuals at risk of being affected by suicidal behaviour, enabling the monitoring of them and also contributing to the reduction of this problem1. Thus, the objective of this study is to estimate the prevalence of thought, planning and attempted suicide among adolescents, and to identify the sociodemographic characteristics and lifestyles of the same population in southern Brazil.
METHODS
Population and sample
An analytical study of the transverse type was carried out, from the basis of the 'Brazilian guide to the evaluation of health-related physical fitness and life habits - Phase I', under the CAAE Protocol: 33210414.3.0000.0121, from August to November 2014. The sample was composed of high school adolescents between 14 and 19 years old, enrolled in State public schools in the city of São José, Santa Catarina, Brazil.
Characterisation of the research location
The city of São José has 209,804 inhabitants over a territory of 152,387 sq. km, a municipal human development index of 0.809, a Gini index of 0.44, a per capita income of R$1,157.43, and a life expectancy at birth of 77.81 years. The percentage of young people from 15 to 17 years old with full elementary schooling is 70.94%13.
Determination of the sample
The sampling process was determined in two stages: (1) stratified by State public high schools (n = 11) and (2) conglomeration of classes considering study timetable and teaching class (n = 170 classes). At stage two, all high school students who were present in the classroom on the days of data collection were invited to participate in the study.
To calculate the sample, prevalence was considered to be unknown for the outcome (50%), a tolerable error of five percentage points, a 95% confidence level, and a design effect of 1.5. We added 20% for losses and refusals and 20% more for association study. Considering that 5,182 students were enrolled in high school, the sample size was estimated at 751 adolescents. However, due to sampling by conglomeration, all students of classes were invited to participate in the survey, resulting in 1,132 students with data collected.
It was defined as 'eligible' to be enrolled in a State public school, to be present in a classroom on the day of data collection and to be between 14 and 19 years old. Those who showed no interest in participating in the research were considered as 'refused'.
Dependent variable
The identification of suicidal thoughts was assessed by three questions from the questionnaire Youth Risk Behaviour Survey (YRBS), validated for the Brazilian population14. The first question was in relation to the number of times the teenager thought of committing suicide in the last 12 months, categorised into 'yes' (one or more times) and 'no' (no thoughts at all of committing suicide). The second question dealt with whether the teenager had planned suicide in the last 12 months, split between 'yes' (planned) and 'no' (not planned). Finally, the question about the frequency that the teenager had tried to commit suicide was categorised into 'no/never' and 'one or more times'.
Independent variables
Sociodemographic variables (gender, age, skin colour, and economic status) and lifestyle (sleep, perception of body weight, physical activity, and intake of alcoholic drinks) were collected through a self-administered questionnaire. Gender (female/male) was self-reported by participants. The age was collected as a quantitative discrete variable (in full years), being categorised into '14 to 16 years' and '17 to 19 years', also distributed in three ages in each category. Skin colour was classed as brown, black, white, yellow, or indigenous, as proposed by the Brazilian Institute of Geography and Statistics15. However, this variable was categorised into 'white' and 'black/yellow/brown/indigenous', due to the low occurrence of black (7.2%), yellow (4.4%) and Indian (1.7%) participants. The economic status was investigated by the questionnaire of the Brazilian Association of Research Companies16 that divides the population into eight economic classes in descending order of purchasing power: A1, A2, B1, B2, C1, C2, D, and E.
Due to the low occurrence of adolescents in certain categories (A1 = 0.0%; A2 = 4.2%; B1 = 20.9%; B2 = 42.7%; C1 = 26.1%; C2 = 5.4%; D = 0.7%, and E = 0.0%), it was decided to split this variable into 'high' (A1; A2; B1; B2) and 'low' (C1; C2; D; E).
The variables of lifestyle, sleep quality and perception of body weight were assessed by the questionnaire 'Fantastic Lifestyle', which was translated and validated for the Brazilian population17. Sleep quality was analysed by the question: 'Do you sleep well and feel rested?' It was categorised into 'sleep well' for students who answered 'sometimes', 'fairly often' and 'often', and 'I do not sleep well' for those who answered 'almost never' and 'rarely'. The perception of body weight was measured by the question: 'How do you describe your weight?'. Responses were categorised into 'appropriate' ('the right weight I hope') and 'inappropriate' ('a little below', 'far below what I expect', 'a little above what I would hope', and 'way above what I expect').
Physical activity was assessed with the following question: 'Over the past seven days, on how many days have you been physically active for at least 60 minutes a day?', considered as any time spent in any type of physical activity that has increased heart rate and breathing for some time. The issue was withdrawn from the YRBS questionnaire.14 Teenagers who practiced physical activity five or more days a week were classified as 'physically active'. Those who were active on fewer than five days a week were classified as 'not physically active'18.
Alcohol intake was analysed by the 'Binge Drinking' questionnaire, which identifies alcohol intake in young people14,19,validated for the Brazilian population14. The question was: 'During the last 30 days, on how many days have you had five or more drinks of alcohol on the same occasion?' Alcohol consumption was categorised into 'no' (not consumed) and 'yes' (consumed five or more drinks). The consumption of five or more drinks on a single occasion is considered excessive, independent of the regularity20.
Statistical analysis
The analyses were conducted using the Statistical Package for the Social Sciences (SPSS) version 22.0. In descriptive statistics, averages, standard deviations, medians, interquartile intervals, and frequency distribution are all used. In identifying differences in the prevalence of suicidal thoughts compared with independent variables, the Chi-square test for heterogeneity and linear trend was applied.
Binary logistic regression was conducted with an estimated odds ratio and confidence interval (95%). All variables were introduced in the fitted model independent of p-value in the crude analysis. The adjusted analysis was conducted of21 hierarchical form being divided into two blocks: distal (age, skin colour, and economic status) and proximal (sleep, physical activity, alcohol intake, and perception of body weight). Variables with p-value < 0.2022 remained in the fitted model via the backward. The significance level was established at 5%.
RESULTS
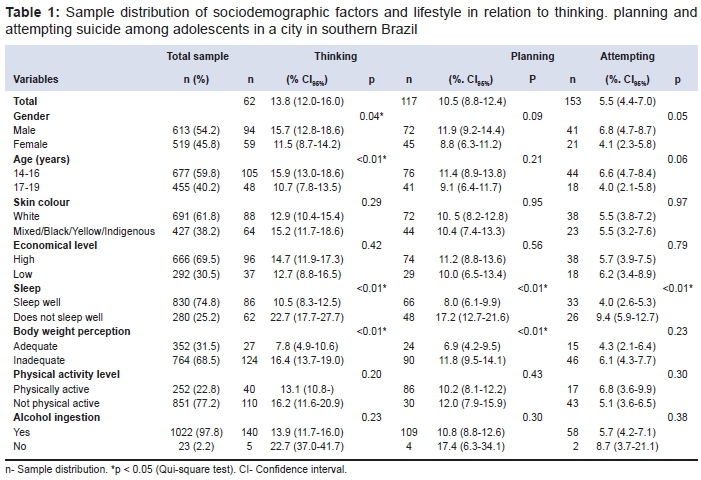
The sample was composed of 1,118 students who were, on average, 16 ± 1.14 years old. The prevalences were 13.8% for suicidal thinking, 10.5% for planning, and 5.5% for suicide attempts.
The majority of the sample (54.2%) were male, between the ages of 14 and 16 years (59.8%), had white skin colour (61.8%), and almost 70% had a high economic status. Approximately 75% of teenagers did not sleep well, 68.5% had poor body weight perception, 77.2%, were physically active, and 97.8% consumed five or more drinks of alcohol on a single occasion (Table 1).
Male adolescents (15.7%) and those at the ages of 14 to 16 (15.9%) had a higher prevalence of suicidal thinking. Higher prevalence of thought (22.7%), planning (17.2%) and suicide attempt (9.4%) were identified in teenagers who did not sleep well (p < 0.01). Teenagers with a poor perception of body weight had a higher prevalence of thought (16.4%) and suicide planning (11.8%) (p < 0.01) (Table 1).
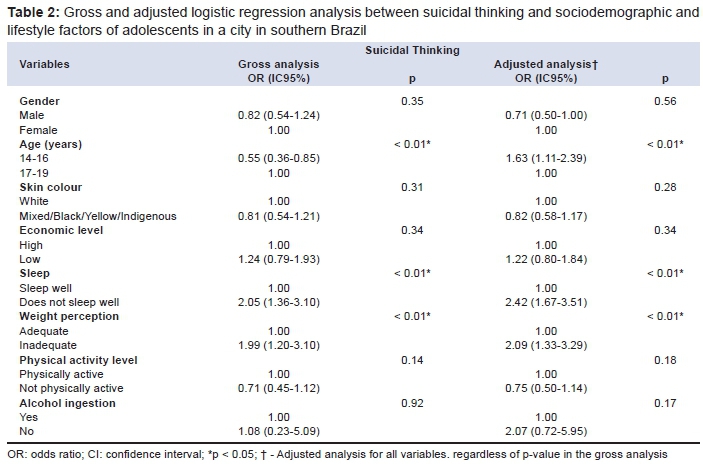
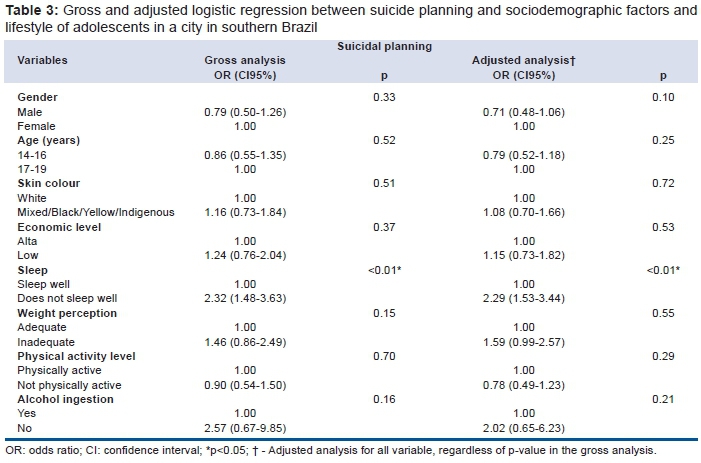
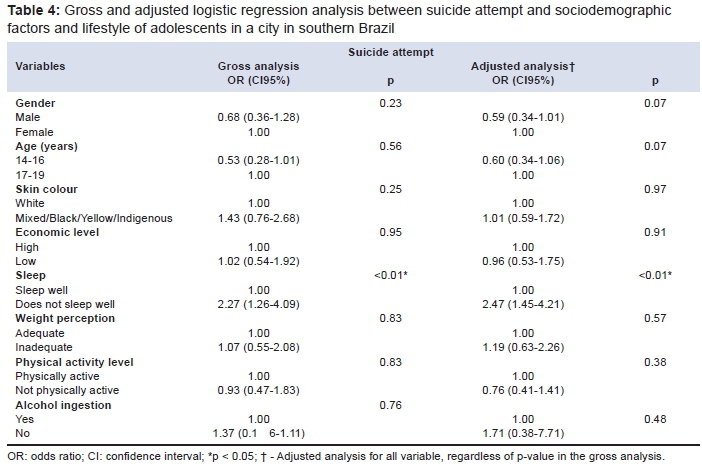
According to logistic and adjusted regression, the teenagers who had suicidal thoughts were the youngest, between 14 and 16. Moreover, adolescents susceptible to thinking, planning and suicide attempt had the characteristic of not sleeping well (Table 2, Table 3 and Table 4, respectively). In the adjusted analysis, adolescents with suicidal thoughts showed a poor perception of body weight (Table 2).
DISCUSSION
In this study, approximately 12.1% of the adolescents had had suicidal ideations (thoughts and planning) and 5.5% had attempted suicide. Suicidal thinking was a characteristic of younger individuals who were not sleeping well and had a poor perception of body weight. Incidences of planning and trying to commit suicide was higher for those who had inadequate sleep.
An analysis of suicide in adolescents has been investigated in relation to thought4,7,23, planning and attempt24. Studies that have examined the prevalence of suicide thoughts found values ranging from 11.2% in adolescents in the State of Pernambuco, Brazil7, to 16.0% in adolescents in Campinas, São Paulo, Brazil23. In relation to planning, a prevalence was found of 4.0% in adolescents of the United States8 to 9.5% in Sergipe, Brazil4. The suicide attempts occurred with varying prevalence of 2.0% in Campinas, São Paulo, Brazil23, to 8.8% in Thai teenagers24.
Some factors increase vulnerability to ideation (thinking and planning) and suicide attempts, such as depression, alcoholism, drug use, exposure to violence, abuse, stress, and learning difficulties1,2,12. As thought, planning and attempt are factors that can predict suicide, the prevalence found can help to prevent a leading cause of death in adolescence1-3. These alert data sometimes might be underestimated, since suicide is permeated by myths, taboos and prejudices concerning morals and religion, resulting in omission of data1.
The present study showed that teenagers who had suicidal thoughts had the characteristic of being in the younger age range. A similar result was found in research conducted with Thai teenagers24. This finding is justified because younger teenagers tend to have less emotional maturity for the resolution of everyday problems, such as family squabbles, emotional relationships, and school affairs, acting with greater impulsivity when thinking about drastic measures such as suicide3,24.
In the study, it was identified that individuals affected by thought, planning and attempt had the characteristic of not sleeping well; this finding was also evidenced in the systematic review9. Changes occur in the level of melatonin, the sleep hormone, during adolescence so, in this period, there is a need for more hours of sleep, which can be explained by the maturation changes25. Although the physiological need during adolescence is nine hours of sleep, most teenagers do not get this, reducing secretion of the hormone serotonin, which is responsible for control of mood, anxiety and impulsivity, which may cause emotional instabilities9.
Teenagers with suicidal thinking were found to have a poor perception of body weight. This finding is consistent with a study of adolescents (12 to 19 years) in Guangzhou, China10, and a longitudinal study with American teenagers11. This is because teenagers tend to value the body too much and want to feel included in the aesthetic patterns associated with youth and beauty, as transmitted by the media, especially television programming. The emotional development of teenagers is affected through psychosocial and cultural pressure10.
One of the limitations of the study is the fact the teenagers knew they were participating in research that would rate lifestyle features; this can, by itself, influence the results, as an under-estimate or over-estimate of these variables. Another limitation is the cross-sectional study type that does not allow us to establish cause and effect relationships.
A strong point of the study is the presentation of data on the characteristics of adolescents with suicidal behaviours a city in southern Brazil, which can serve as a parameter for comparative investigations with young people. In addition, the study associations intensify the need to plan preventative actions on the thought, planning and suicide attempts of teenagers.
The development of programmes to prepare health professionals to deal with topics related to suicidal behaviour is important in the field of public health, because it helps to detect these prior behaviours, fostering appropriate follow-up, to stop the damaging effects of these behaviours that can lead to death12. It is concluded that one in 10 teenagers showed suicidal thinking and planning, and the proportion was less than one for suicide attempts. In addition, the teenagers affected by three suicidal behaviours (thinking, planning and attempt) presented with the feature of not sleeping well. Teenagers susceptible to suicidal thinking had the characteristic of being young and having a poor perception of body weight.
REFERENCES
1. Braga LL, Dell'Aglio DD. Suicídio na adolescência: fatores de risco, depressão e gênero. Contextos Clínicos. 2013;6(1):2-14. DOI: http://dx.doi.org/10.4013/ctc.2013.61.01 [ Links ]
2. Schlösser A, Rosa GFC, More CLOO. Revisão: comportamento suicida ao longo do ciclo vital. Temas Psicol. 2014;22(133):1-145. DOI: http://dx.doi.org/10.9788/TP2014.1-11 [ Links ]
3. Teti GL, Rebok F, Rojas SM, Grendas L, Daray FM. Systematic review of risk factors for suicide and suicide attempt among psychiatric patients in Latin America and Caribbean. Rev Panam Salud Publica. 2014;36(2):124-33. [ Links ]
4. Silva RJS, Santos FAL, Soares NMM, Pardono E. Suicidal ideation and associated factors among adolescents in Northeastern Brazil. Scientific World J. 2014(2014):8. DOI: http://dx.doi.org/10.1155/2014/450943 [ Links ]
5. Perry BL, Stevens-Watkins D, Oser CB. The moderating effects of skin color and ethnic identity affirmation on suicide risk among low-SES African American women. Race Soc Probl. 2013;5(1):1-14. DOI: http://dx.doi.org/10.1007/s12552-012-9080-8 [ Links ]
6. Hawton K, Saunders KE, O'Connor RC. Self-harm and suicide in adolescents. Lancet. 2012;379(9834):2373-82. DOI: http://dx.doi.org/10.1007/s12552-012-9080-8 [ Links ]
7. Carvalho PDD, Barros MVGD, Santos CM, Melo EN, Oliveira NKRD, Lima RA. Prevalência e fatores associados a indicadores negativos de saúde mental em adolescentes estudantes do ensino médio em Pernambuco, Brasil. Rev Bras Saúde Matern Infant. 2011;11(3):227-32. DOI: http://dx.doi.org/10.1590/S1519-38292011000300003 [ Links ]
8. Nock MK, Green JG, Hwang I, McLaughlin KA, Sampson NA, Zaslavsky AM, et al. Prevalence, correlates, and treatment of lifetime suicidal behavior among adolescents. JAMA Psychiatry. 2013;70(3):300-10. DOI: http://dx.doi.org/10.1001/2013.jamapsychiatry.55 [ Links ]
9. Pigeon WR, Martin P, Kenneth C. Meta-analysis of sleep disturbance and suicidal thoughts and behaviors. J Clin Psychiatry. 2013;73(9):1160-67. DOI: http://dx.doi.org/10.4088/JCP.11r07586 [ Links ]
10. Wang J, Deng XJ, Wang JJ, Wang XW, Xu L. The associations between health risk behaviors and suicidal ideations and attempts in an urban Chinese sample of adolescents. J Affect Disord. 2010;126(1-2):180-7. DOI: http://dx.doi.org/10.1016/j.jad.2010.02.121 [ Links ]
11. Lee CG, Seo DC. Trajectory of suicidal ideation in relation to perceived overweight from adolescence to young adulthood in a representative United States sample. J Adolescent Health. 2013;53(6):712-716. DOI: http://dx.doi.org/10.1016/j.jadohealth.2013.06.013 [ Links ]
12. Lima NN, do Nascimento VB, de Carvalho SM, de Abreu LC, Neto ML, Brasil AQ, et al. Childhood depression: a systematic review. Neuropsychiatr Dis Treat. 2013;9:1417-25. DOI: http://dx.doi.org/10.2147/NDT.S42402 [ Links ]
13. Programa das Nações Unidas para o Desenvolvimento (PNUD). O índice de desenvolvimento humano municipal brasileiro. Brasília: PNUD, Ipea, FJP, 2013. [ Links ]
14. Guedes DP, Lopes CC. Validação da versão brasileira do Youth Risk Behavior Survey 2007. Rev Saude Publ. 2010;44(5):840-850. DOI: http://dx.doi.org/10.1590/S0034-89102010000500009 [ Links ]
15. Instituto Brasileiro de Geografia e Estatística (IBGE). Censo Demográfico de 2010: dados preliminares do universo. Disponível em: http://www.ibge.gov.br/home/estatistica/populacao/censo2010/resultados _preliminares/default_resultados_preliminares.shtm. Acesso em: 18 abr. 2015. [ Links ]
16. Instituto Brasileiro de Geografia e Estatística (IBGE). Pesquisa de Orçamentos Familiares, 2008-2009: tabela de medidas referidas para os alimentos consumidos no Brasil. Disponível em: http://www.ibge.gov.br/home/estatistica/populacao/condicaodevida/pof/2008_2009 _medidas/default.shtm. Acesso em: 18 abr. 2015. [ Links ]
17. Rodriguez A, Reis CR, Siqueira R, Petroski EL. Versão brasileira do questionário "estilo de vida fantástico": tradução e validação para adultos jovens. Arq Bras Cardiol. 2008;91(2):102-109. DOI: http://dx.doi.org/10.1590/S0066-782X2008001400006 [ Links ]
18. Strong WB, Malina RM, Blimkie CJ, Daniels SR, Dishman RK, Gutin B, et al. Evidence based physical activity for school-age youth. J Pediatr. 2005; 146(6):732-7. DOI: http://dx.doi.org/10.1016/j.jpeds.2005.01.055 [ Links ]
19. Petit G, Maurage P, Kornreich C, Verbanck P, Campanella S. Binge drinking in adolescents: a review of neurophysiological and neuroimaging research. Alcohol Alcohol. 2014;49(2):198-206. DOI: http://dx.doi.org/10.1093/alcalc/agt172. [ Links ]
20. Midanik LT. Drunkenness, feeling the effects and 5 meassures. Addiction. 1999;94(6):887-97. DOI: http://dx.doi.org/10.1046/j.1360-0443.1999.94688711.x [ Links ]
21. Victora CG, Huttly SR, Fuchs SC, Olinto MT. The role of conceptual frameworks in epidemiological analisys: a hierarchical approach. Int J Epidemiol. 1997;26(1):224-7. DOI: http://dx.doi.org/10.1093/ije/26.1.224 [ Links ]
22. Maldonado G, Greenland S. Simulation study of confounder-selection strategies. Am J Epidemiol. 1998;138(11):923-36. [ Links ]
23. Botega NJ, Marín-León L, Oliveira HB, Barros MBA, Silva VF, Dalgalarrondo P. Prevalência de ideação, plano e tentativa de suicídio: Um inquérito de base populacional em Campinas, São Paulo, Brasil. Cad Saude Pública. 2009;25(1):2632-8. DOI: http://dx.doi.org/10.1590/S0102-311X2009001200010 [ Links ]
24. Peltzer K, Pengpid S. Suicidal Ideation and Associated Factors among School-Going Adolescents in Thailand. Int J Environ Res Public Health. 2012;9(2):462-73.DOI: http://dx.doi.org/10.3390/ijerph9020462 [ Links ]
25. Sarchiapone M, Mandelli L, Carli V, Iosue M, Wasserman C, Hadlaczky G, et al. Hours of sleep in adolescents and its association with anxiety, emotional concerns, and suicidal ideation. Sleep Med. 2014;15(2):248-54. DOI: http://dx.doi.org/10.1016/j.sleep.2013.11.780 [ Links ]
Manuscript submitted: Feb 28 2016
Accepted for publication Mar 10 2016.
* Corresponding author: Carlos Alencar Souza Alves Junior - Universidade Federal de Santa Catarina - Campus Universitário - Trindade - Caixa Postal 476 - CEP 88040-900 - Florianópolis/SC.


{kind=link}
{kind=link}
{kind=link}
{kind=link}