










Servicios Personalizados
Revista

Articulo
 Inglés (pdf)
Inglés (pdf)
 Articulo en XML
Articulo en XML Referencias del artículo
Referencias del artículo
Indicadores
Compartir

 Permalink
PermalinkJournal of Human Growth and Development
versión impresa ISSN 0104-1282versión On-line ISSN 2175-3598
J. Hum. Growth Dev. vol.31 no.3 Santo André sep./dic. 2021
https://doi.org/10.36311/jhgd.v31.12744
ORIGINAL ARTICLE
DOI: 10.36311/jhgd.v31.12744
Analysis of COVID-19 mortality and case-fatality in a low- income region: an ecological time-series study in Tocantins, Brazilian Amazon
Andre Evaristo Marcondes CesarI; Blanca Elena Guerrero DaboinI; Tassiane Cristina MoraisII, III; Isabella PortugalIV; Jorge de Oliveira EcheimbergV; Luciano Miller Reis RodriguesV; Lucas Cauê JacinthoVI; Rodrigo Daminello RaimundoV; Khalifa ElmusharafI; Carlos Eduardo SiqueiraI, VII
IMaster of Public Health Program, School of Medicine, University of Limerick, V94 T9PX, Limerick, Ireland
IIEscola Superior de Ciências da Santa Casa de Misericórdia (EMESCAM), 29045-402 Vitória, ES, Brazil
IIIDepartamento de Educação Integrada em Saúde, Universidade Federal do Espírito Santo, 29075-910 Vitória, ES, Brazil
IVDepartamento de Clínica Médica, Faculdade de Medicina da Universidade de São Paulo, 05403-000 São Paulo, SP, Brazil
VLaboratório de Delineamento de Estudos e Escrita Científica, Centro Universitário FMABC, 09060-870 Santo André, SP, Brazil
VIDivisão de Imunologia e Alergia Clínica, Departamento de Medicina, Faculdade de Medicina da Universidade de São Paulo, 05403-000 São Paulo, SP, Brazil
VIIDepartment of Urban Planning and Community Development, School for the Environment, University of Massachusetts Boston, 100 Morrissey Boulevard, Boston, MA 02125
ABSTRACT
INTRODUCTION: Inserted in the vulnerable context of the Brazilian Amazon, the state of Tocantins has suffered damages with the dissemination of COVID-19 in its territory; however, little evidence is published from this state.
OBJECTIVE: This study aims to analyze the case-fatality, mortality, and incidence of COVID-19 in Tocantins.
METHODS: This is an ecological study, population-based, time-series analysis of COVID-19 cases and deaths in the state of Tocantins from March 2020 to August 2021.
RESULTS: During the examined period, 219,031 COVID-19 cases, and 3,594 deaths were registered due to disease. Two possible occurrence peaks were characterized in this time-series analysis. Remarkably, the Second Wave had the highest lethality rates (3.02% - April 2021), mortality (39.81 deaths per 100,000 inhabitants - March 2021), and incidence (1,938.88 cases per 100,000 inhabitants - March 2021). At the end of the period, mortality, incidence, and lethality showed flat trends, suggesting a positive outcome of the vaccination program.
CONCLUSION: The prevention, surveillance, and control actions of COVID-19 cases in Tocantins State have been directed to mitigate the deleterious effects of the pandemic. Nevertheless, efforts are still needed to decrease lethality, mortality, and incidence trends, and ultimately to achieve control of the COVID-19 pandemic in the region
Keywords: COVID-19, case fatality, incidence, mortality, trends.
Authors summary
Why was this study done?
This study was carried out due to gaps in the scientific literature about the evolution of COVID-19 in the state of Tocantis, northern Brazil, in addition to the need for constant monitoring of epidemiological indicators of incidence, mortality and lethality of COVID-19 in areas inserted in a context of vulnerability as is the case of territory belonging to the Brazilian Legal Amazon.
What did the researchers do and find?
The researchers conducted an ecological study with temporal analysis of the incidence, mortality and lethality rates of COVID-19 in Tocantins from March 2020 to August 2021. The researchers found the formation characteristic of two possible waves of COVID-19 in Tocantins; it was during the second wave that the state recorded the highest rates of incidence, lethality and mortality. However, at the end of August 2021 the incidence, mortality and lethality rates showed flat trends suggesting a positive outcome of the vaccination program.
What do these findings mean?
Efforts are still needed to decrease lethality, mortality, and incidence trends in order to reach the control of the COVID-19 pandemic in the Tocantins.
INTRODUCTION
The COVID-19 pandemic has beaten Brazil hardly, ranking second in deaths, behind the United States of America. This South American country has been confronting one of the most complex hospital and health system crises ever1. Since its first confirmed COVID-19 case reported on February 26, 20202, Brazil has exhibited critical epidemiological circumstances in its enormous territorial dimension, ranging in severity from region to region3.
These geographical differences in population density, access to health services, age, and socioeconomic factors have accentuated inequities, mainly impacting the country's most impoverished regions, such as the Northern region4. This region suffers the imbalances in the failures of social security, and the lack of adequate and integrated control measures aggravate mortality and social vulnerability rates5.
In the vulnerable context of Northeast Brazil, Tocantins contributes approximately 0.5% to the national gross domestic product, being one of the states that provides the least6. Furthermore, 93% of its population depends on the National Health System7.
Like other states of the Amazonian region, Tocantins is an endemic area for other infectious ailments clinically similar to COVID-19, increasing the arena of differential diagnosis. To illustrate, there is evidence of co-infections of SARS-CoV-2 with dengue8. This syndemic context complicates COVID-19 detection and treatment in the region.
The mortality rate is one of the main characteristics differentiating the coronavirus from the Severe Acute Respiratory Syndrome (SARS) and the Middle East Respiratory Syndrome (MERS) outbreaks9. Given the fluctuations detected in the incidence and lethality of COVID-19, it is relevant to study and understand regional factors that affect the contagion and spread of this new virus. Besides, time-series studies are helpful to analyze the pandemic behavior curves10.
The first confirmed case of COVID-19 in Tocantins was reported in the state capital, on March 18, 2020, by a traveler returning from Fortaleza, an urban city in the Northeast11. A month later, State authorities reported its first death due to this disease12. The situation worsened significantly; more than a year after registering its first COVID-19 case2; however, little evidence is published on this state, which is the newest of the Brazilian federative units and concentrates only 0.7% of the country's total population6.
Therefore, this study analyzed the case-fatality, mortality, and incidence of COVID-19 in Tocantins, Brazil, from March 2020 to August 2021.
METHODS
This is an ecological study of population-based time-series analyzing COVID-19 cases and deaths in the state of Tocantins (figure 1). This study is part of a population-based umbrella project, where each state of Brazil was analyzed separately, following a standard protocol for ecological time-series studies as described by Abreu, Elmusharaf and Siqueira10
Data were obtained directly from the COVID-19 Electronic Database of the Health Department of Tocantins. It is a State public database that contains official information on cases and deaths caused by COVID-19 without patient identification13.
From March 2020 to August 2021, a total of 219,031 accumulated cases and 3,594 deaths were caused by COVID-19. All cases and deaths with laboratory, clinical or epidemiological confirmation of COVID-19 were included in the study. The cases were classified according to test date and death date; those with missing date information were excluded. Two different researchers collected data to avoid collection bias. Then, the extracted information was organized in the Excel spreadsheet software (Microsoft Corp., Redmond-WA, USA, 2021) for further analysis. The database was updated on September 29, 2021.
The incidence (1) and mortality rates (2) by 100,000 inhabitants and the case-fatality (3) (%) were determined with the following equations:

The population used for calculations was obtained from the Federal Court of Accounts (TCU population). It corresponded to the resident people in Tocantins and was estimated at 1,572,866 inhabitants for 201914.
For trends analysis, the period was split into two waves: the First Wave (W1), from March to November 2020, and the Second Wave (W2), from December 2020 to August 2021. Noteworthy, the W1 ended with the lowest mortality rate in November 2020, according to the analysis of the curve shape.
The Prais-Winsten regression model for population mortality rates was used to build a time series as well as to determine incidence, case-fatality and mortality trends15. Probability (p) and Daily Percent Change (DPC) were estimated considering a 95% level significance, according to equations (1), (2), and (3):
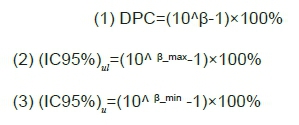
In these equations, we considered β as the angular coefficient from the linear regression, the indexes ul as the upper limit, and ll as the lower limit of the confidence level.
Statistical analyses were performed using the STATA 14.0 software (College Station, TX, U.S. 2013). The effective reproductive number (Rt) was estimated using R studio software EpiEstim package16, version 2.2.4, a time-varying reproduction number for epidemics developed by Thompson and colleagues17. We used a mean serial interval of 2.97 days with a mean, standard deviation of 3.29 days, as described in previous studies18,19.
Then, we performed a Spearman correlation analysis between Rt and daily new cases, Rt and daily deaths, and Rt and lethality.
RESULTS
Among the Amazonian states, Tocantins is probably one of the less known in Brazil and the country outside. Table 1 describes some of the sociodemographic characteristics and inherent information of the hospital system infrastructure in Tocantins State.

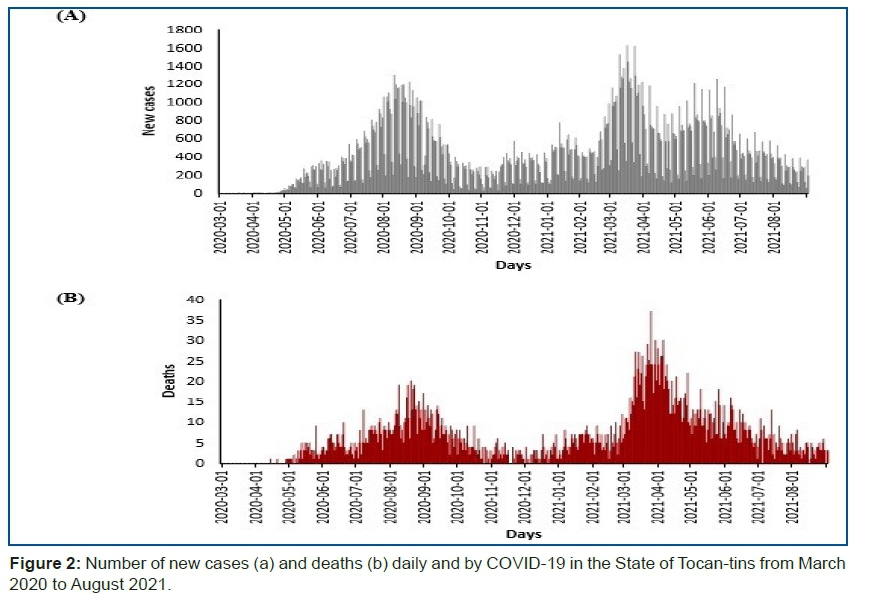
Throughout the period studied, we identified 219,031 cases (Figure 2a) and 3,594 deaths (Figure 2b).
Figure 3 exhibits two possible waves: the first occurred in 2020 from March to November, and the second from December 2020 to August 2021. The highest lethality rate in the period (3.02%) was in April 2021 (Figure 3a), and the highest mortality (39.81 deaths per 100,000 inhabitants) and incidence (1,938.88 cases per 100,000 inhabitants) rates were in March 2021 (Figure 3b and 3c).
Furthermore, Table 2 shows stationery trends in mortality and case fatality rates during the W1 although the incidence trend was increased, p< 0.05. The trends of all indicators were flat during the W2.
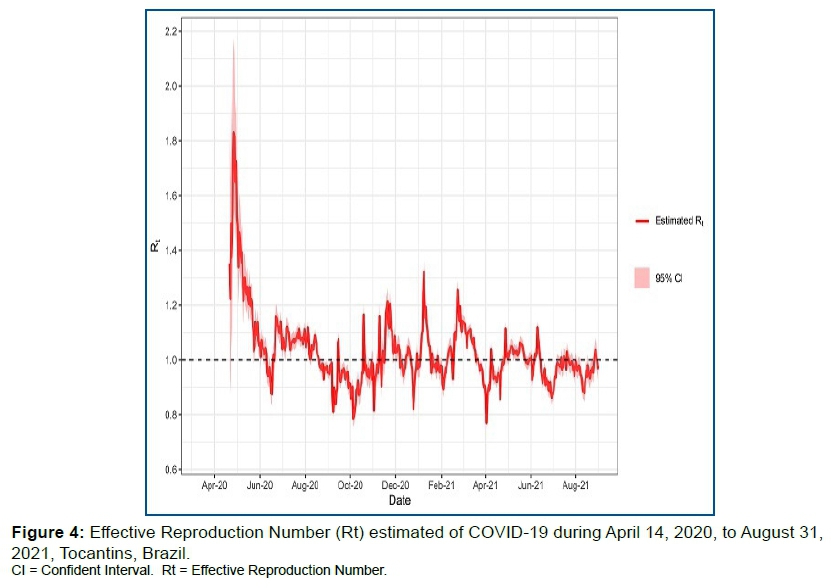
Figure 4 indicates the Rt value, as a function of time for the evaluated period. The estimated Rt value of COVID-19 experienced fluctuations over this period. There was a significant growth peak between April and May 2020, then a predominance of Rt indexers below one (1) from August 2020, with an increase in viral transmissibility after October 2020. Then, during the W2, a peak is observed in January 2021 with a predominance of Rt above one (1) until June 2021, with a stationary behavior for the remaining months (Rt <01).
This pattern appears similar to the time series of new cases. Therefore, correlation analyzes were performed between Rt and daily new cases, between Rt and daily deaths, and between Rt and lethality. The results for Spearman's ρ coefficients are shown in Table 3.
In addition, the correlation coefficient between Rt and deaths showed to be significant in Table 3. That is, the behavior of the frequency of deaths is negatively associated with Rt despite the low intensity of the correlation. The expected value for the correlation coefficient between these variables would be ρ ~ 0. Therefore, despite having statistical significance, the value of ρ suggests that Rt is weakly dependent on the number of daily deaths and that Rt has a behavior contrary to this number. There is no significant correlation between Rt and new cases. This result is opposed to what was expected; it is presumed that an increment in Rt implies an increase in the number of new daily cases. However, the correlation coefficient ρ = 0.026 and the p-value = 0.562, which is at least ten times greater than the α significance, revealed these variables are independent. For the correlation be-tween Rt and lethality, ρ = -0.246 with p-value < 0.001 was found, suggesting a significant negative association between Rt and lethality. That is, as the number of infections in-creases, lethality decreases.
DISCUSSION
From March 2020 to August 2021, Tocantins was affected by 219,031 cases of COVID-19, in which 3,594 of them evolved to death. During this period, there was the formation of two possible waves. The mortality and fatality rates remained flat during the W1, but the incidence had an increasing trend. Prevention initiatives were implemented22, and social distancing measures were adapted to reduce the risk of transmission. Immediately after confirming the first case, the local authorities declared a state of public calamity, including restrictions on non-essential activities such as commerce and tourism23. On the other hand, a process of (re) planning, (re) organization, (re) allocation of human and financial resources must be implemented by the State to have a rapid and effective response during public health emergencies, such as (1) continuity of essential services; (2) well-coordinated implementation of priority actions; (3) clear and accurate internal and external communication; (4) rapid adaptation to increasing demands; (5) effective use of scarce resources; and (6) safe environment for healthcare professionals and patients24.
The importance of these non-pharmacological actions to prevent the increase in infections was probably not given at the beginning of the pandemic, especially in urban areas, which influenced the increasing number of new cases and benefit the beginning of a new wave at the end of November 2020. However, according to the bulletin from May to June25, the capital of Tocantins was among the urban cities that adopted more rigorous policies for long periods. It would be possible that the population was not prepared to practice individual and community mask use, distancing, and hand hygiene measures for prolonged periods26.
The case-fatality rate of 2.38% marked the onset of the pandemic in April 2020, when the first deaths (n=3) of COVID-19 fatal victims were reported. This result matches the COVID-19 case-fatality published by the State Government of Tocantins at the beginning of the pandemic, with a lethality record of 2.03% in May 202027. However, this fatality is lower than that found in other states such as Piauí (9.09%), Pernambuco (7.35%), and São Paulo (5.97%), during the 13th epidemiological week28.
According to the COVID-19 Observatory report of Fundação Oswaldo Cruz, on the first six months of the pandemic, Tocantins had one of the highest incidence rates in the country despite its low population. In August 2020 reached the third-highest rate in the Northern region, with trends increasing incidence and mortality rates29. Similar to our findings, peaks of incidence (1,585.66 cases per 100,000 inhabitants) and mortality (22.89 deaths per 100,000 inhabitants) happened in August 2020, during the W1. Despite the high increments in the indicators of incidence and mortality described in August 2020, the W2 presented more distressing circumstances. The alarming rates of incidence and mortality reported in March 2021 (Figures 3b and 3c) almost doubled the number of deaths of the worst month during the W1.
In March 2021, the Fundação Oswaldo Cruz (FIOCRUZ) issued a special bulletin warning on a simultaneous worsening across Brazil of the various indicators, with an increase in the number of cases and deaths of COVID-19, the maintenance of high levels of incidence of SARS, high rates of test positivity and hospital overload. During this period, all states in Northeast Brazil, including Tocantins, had above 80% occupancy rates of COVID-19 ICU beds for adults30.
The high rates indicate that even after a year of a pandemic, Tocantins and Brazil faced a challenging scenario of catastrophic conditions to control the spread of COVID-19. Several factors may have contributed to this situation, such as typical Brazilian festivities like carnival and the infection with new variants. The high peak of cases and deaths observed during the W2, in March 2021, happened after the carnival holidays. Although the official carnival was canceled31, still, people gathered in the streets and private parties, which furthered the spread of the virus. Besides, during this period, the P1 (Manaus) variant of SARS-CoV-2 was detected for the first time, presenting greater transmissibility32. In this controversial scenario, not enough tests were performed to detect the disease, so there was no factual knowledge regarding asymptomatic patients.
It is possible that the stated factors contributed to Tocantis reaching, in April 2021, the highest case-fatality rate (3.02%) since the beginning of the pandemic; however, in this period, the viral transmissibility rates were predominantly controlled (Rt <1). In this study, a negative correlation was found between Rt and lethality. Still, these results should be interpreted with caution, as many other factors influence the fatal repercussions of COVID-19, such as gender, ethnicity, and risk factors33,34.
Furthermore, most Brazilian states adopted more restrictive measures to mitigate the spread of SARS-CoV-2, only while experiencing a scenario characterized by a high number of deaths and high hospital bed occupancy rates. In this sense, the Rt would be one of the leading indicators to be considered during government decision-making to contain the spread of the disease and future collapses in health systems.
Monitoring Rt scores is essential to implement strategies for pandemic coping. Relaxation measures to control population mobility should only be adopted when the Rt values are below 1 where the situations can still be handled35. The population care can be directed to the primary care services, which is essential to sustain the health systems, protecting against the excessive demands generated by the pandemic.
However, at the end of August 2021, the trend for mortality, fatality, and incidence was flat. Although this fact could have been a positive outcome of the vaccination program, with a predominance of Rt below than one (1), it is noteworthy that the pandemic scenario is always in constant change. Thus, current efforts must be intensified to contain the spread of SARS-CoV-2 in this region and minimize catastrophic consequences in the future. Specific determinants are affecting the pandemic situation in Tocantins, such as its geographical location as a strategical State Road junction. A vast interchange through highways leads to cities in the North, Northeast, and Central-west regions36, facilitating the spread of the new coronavirus.
The demographic density of Tocantins is 4.98 inhabitants/km26. In contrast, the average number of people in the urban area per household is three20, which affects the high incidence of infections by COVID-1937,38. Besides, people have isolation limitations39. These variables primarily impact Palmas, the capital city.
In addition, data from the Tocantins State Health Secretary40 revealed that 7,886 indigenous people and 6,551 individuals of African descent (Quilombos) communities live on the banks of the rivers in houses where a high number of individuals congregate. The crowded boats through the rivers of the Amazon area41 are also a risk factor to spread the SARS-CoV-2.
Tocantins was one of the first states to present a contingency plan to face COVID-19. Likewise, they created a crisis committee with authorities representing each power, control and security body, and health authorities and professionals. These initiatives were carried out to debate and seek joint actions and strategies to minimize the impact of the pandemic42.
However, this state suffers health services constraints at regular times. During the pandemic, the authorities have to deal with a crisis that requires an urgent response mainly because the fatality, mortality, and incidence rates highly rely on poor socioeconomic indexes and local health infrastructure.
The measures were stricter in Palmas, the most populated urban area43. The number of beds was increased from 163 to 467 for the exclusive treatment of COVID-19, from April 2020 to April 2021, health professionals were hired, and personal protective equipment was made available27. However, the consolidated number of ICU beds (public and private) is approximately 0.9 per 10,000 inhabitants, an indicator that is below 2.2, which is the national average44.
According to the FIOCRUZ observatory45, the occupancy rate of intensive care beds in Tocantins has dropped to 75%. Still, this percentage is high, but one of the factors that may have influenced this improvement is the immunization process, with 718,000 people vaccinated. The vaccination plan against COVID-19 has followed the national guidelines, in which the priority groups included indigenous people, afro-descendant communities (Quilombos), and traditional riverine communities27.
The actions of the leaders of this federative unit to apply prevention, surveillance, and control measures are key elements to minimize the spread of the virus SARS-CoV-2 because Brazil does not have a homogeneous strategy to manage the pandemic of COVID-19. The State governments are accountable for planning and executing non-pharmacological and distancing strategies46.
The mandatory use of masks and distancing measures must remain to mitigate and restrain the effects of the pandemic in this Brazilian Amazon territory. It is required to monitor mortality, lethality, and incidence indicators and develop further studies comparing those indicators before and after vaccination.
Limitations
It must be considered that the COVID-19 tests were only carried out on people with clinical manifestations of the disease. The deaths related data is counted based on the previous day, but there may be cases of a delay in the notification.
Some Tocantins municipalities with reduced technical staff and access to digital tools have difficulties in the production and systematization of COVID-19 related data47.
As the pandemic is still in evolution, all the data examined in this research correspond to partial analysis.
CONCLUSION
The W1 showed flat trends in lethality and mortality with an increasing trend in incidence rates, with a Daily Percent Change of 2.23%. The W2 had a more shocking aspect and the highest peaks of mortality, lethality, and incidence occurred in March 2021. However, all indicators showed flat trends at the end of August that may be influenced by the effect of the vaccination.
During the study period, the prevention, surveillance, and control actions of COVID-19 cases in Tocantins were managed to mitigate the effects of the pandemic. However, efforts are still needed to show decreasing trends in lethality, mortality, and incidence.
Author Contributions
Conceptualization, A.E.M.C., B.E.G.D., T.C.M., I.P. and L.C.A.; methodology, A.E.M.C., T.C.M., J.O.E., L.C.J., R.D.R., K.E., C.E.S. and L.C.A.; software, J.O.E., L.C.J.; validation, T.C.M., J.O.E., L.M.R.R., C.E.S. and L.C.A.; data curation, A.E.M.C., T.C.M., L.C.A.; writing-review and editing, all the authors; visualization, all the authors; supervision, K.E., C.E.S. and L.C.A.; project administration, C.E.S. and L.C.A. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Data Availability Statement
Data were extracted from a population database in a COVID-19 dashboard, freely accessible on the Health Department of the State of Tocantins website http://integra.saude.to.gov.br/covid19/.
Acknowledgments
We want to thank Célia Guarnieri da Silva for providing the map illustrated in this study and Henrique Moraes Ramos da Silva for his support in retrieving and handling the data.
Conflicts of Interest
The authors declare no conflict of interest.
REFERENCES
1.Abreu LC de. The path of humanity in the pandemic of COVID-19: the choice of the realistic, optimist or pessimist scenario. J Hum Growth Dev. 2021; 31(1): 05-08. DOI: http://dx.doi.org/10.36311/jhgd.v31.11683 [ Links ]
2.Painel coronavírus [Internet]. [cited 2021 jul. 12]. Available from: https://covid.saude.gov.br/ [ Links ]
3.Lobo AP, Cardoso-Dos-Santos AC, Rocha MS, Pinheiro RS, Bremm JM, Macário EM, Oliveira WK, França GVA. COVID-19 epidemic in Brazil: Where are we at? COVID-19 epidemic in Brazil: Where are we at? Int J Infect Dis. 2020; 97: 382-385. DOI: 10.1016/j.ijid.2020.06.044 [ Links ]
4.Coelho FC, Lana RM, Cruz OG, Villela DAM, Bastos LS, Pastore Y Piontti A, Davis JT, Vespignani A, Codeço CT, Gomes MFC. Assessing the spread of COVID-19 in Brazil: Mobility, morbidity and social vulnerability. PLoS One. 2020; 15(9): e0238214. DOI: 10.1371/journal.pone.0238214 [ Links ]
5.Brasil. Ministério da Saúde. Secretaria de Vigilância em Saúde. Programa Nacional de Prevenção e Controle da Malária. Ministério da Saúde: Brasília, Brasil, 2003. [ Links ]
6.Brasil em síntese: Panoramas [Internet]. [cited 2021 May 10]. Available from: https://cidades.ibge.gov.br/brasil/to/panorama [ Links ]
7.Relatório anual de gestão da Secretaria de Saúde do Estado do Tocantins RAG 2018 [Internet]. [cited 2021 Jul. 05]. Available from: https://central3.to.gov.br [ Links ]
8.Quental KN, Leite AL, Feitosa ADNA, Oliveira ZNP, Tavares LVS, Tavares WGS, Pinheiro EF, Lacsina JR, DeSouza-Vieira T, Silva JBNF. SARS-CoV-2 co-infection with dengue virus in Brazil: A potential case of viral transmission by a health care provider to household members. Travel Med Infect Dis. 2021; 40: 101975. DOI: 10.1016/j.tmaid.2021.101975 [ Links ]
9.Pimentel RMM, Daboin BEG, Oliveira AG, Macedo JrH. The dissemination of COVID-19: an expectant and preventive role in global health. J Hum Growth Dev. 2020; 30(1): 135-140. [ Links ]
10.Abreu LC, Elmusharaf K, Siqueira CEG. A time-series ecological study protocol to analyze trends of incidence, mortality, lethality of COVID-19 in Brazil. J Hum Growth Dev. 2021; 31(3):491-495. DOI: 10.36311/jhgd.v31.12667 [ Links ]
11.Tocantins registra 1º caso confirmado do Covid-19 [Internet]. [cited 2021 jul. 12]. Available from: https://www.to.gov.br/noticias/tocantins-registra-1o-caso-confirmado-do-covid-19/6edmfivjmco1 [ Links ]
12.Boletim Epidemiológico. Notificações para COVID-19 n°33 [Internet]. [cited 2021 jul. 12]. Available from: https://central3.to.gov.br/arquivo/504397/ [ Links ]
13.Secretaria de Saúde do Estado de Tocantins. Integra. [Internet]. [cited 2021 jul. 12]. Available from: http://integra.saude.to.gov.br/covid19/InformacoesEpidemiologicas [ Links ]
14.Datasus. Informações de Saúde - TABNET. Demográficas e Socioeconômica. População residente [Internet]. [cited 2021 jul. 20]. Available from: http://www2.datasus.gov.br/DATASUS/index.php?area=0206&id=6942 [ Links ]
15.Antunes JLF, Cardoso MRA. Uso da análise de séries temporais em estudos epidemiológicos. Epidemiol Serv Saúde 2015; 24(3): 565-576. DOI:10.5123/S1679-49742015000300024 [ Links ]
16.Cori A, Ferguson NM, Fraser C, Cauchemez S. A new framework and software to estimate time-varying reproduction numbers during epidemics. Am J Epidemiol. 2013; 178(9): 1505-1512. DOI: 10.1093/aje/kwt133 [ Links ]
17.Thompson RN, Stockwin JE, van Gaalen RD, Polonsky JA, Kamvar ZN, Demarsh PA, Dahlqwist E, Li S, Miguel E, Jombart T, Lessler J, Cauchemez S, Cori A. Improved inference of time-varying reproduction numbers during infectious disease outbreaks. Epidemics. 2019; 29: 100356. DOI: 10.1016/j.epidem.2019.100356 [ Links ]
18.Ali ST, Yeung A, Shan S, Wang L, Gao H, Du Z, Xu XK, Wu P, Lau EHY, Cowling BJ. Serial intervals and case isolation delays for COVID-19: a systematic review and meta-analysis. Clin Infect Dis. 2021:ciab491. DOI: 10.1093/cid/ciab491 [ Links ]
19.Prete CA, Buss L, Dighe A, Porto VB, da Silva Candido D, Ghilardi F, Pybus OG, de Oliveira WK, Croda JHR, Sabino EC, Faria NR, Donnelly CA, Nascimento VH. Serial interval distribution of SARS-CoV-2 infection in Brazil. J Travel Med. 2021 Feb 23; 28(2):taaa115. DOI: 10.1093/jtm/taaa115 [ Links ]
20.Sistema IBGE de Recuperação Automática. Banco de tabelas estatística [Internet]. [cited 2021 jun. 15]. Available from: https://sidra.ibge.gov.br/home/ipp/brasil [ Links ]
21.CNESNet. Cadastro Nacional de Estabelecimentos de Saúde [Internet]. [cited 2021 jun. 20]. Available from: http://cnes.datasus.gov.br/ [ Links ]
22.Decreto nº 6.065, de 13 de março de 2020. Determina ação preventiva para o enfrentamento do Covid-19: novo Coronavírus [Internet]. [cited 2021 jul. 14]. Available from: https://central.to.gov.br/download/46143 [ Links ]
23.Decreto nº 6.072, de 21 de março de 2020. Declara estado de calamidade pública em todo o território do Estado do Tocantins afetado pela COVID-19 (novo Coronavírus): Codificação Brasileira de Desastre 1.5.1.1.0, e adota outras providências. [Internet]. [cited 2021 jul. 14]. Available from: https://central.to.gov.br/download/46146 [ Links ]
24.Ferreira da Silva R, Helfenstein Albeirice da Rocha MD. La pandemia en un hospital universitario en el norte del Brasil. Revista Subjetividad y Procesos Cognitivos. 2020; 24(2): 145-1600. [ Links ]
25.COVID-19 e medidas legais de distanciamento social isolamento social, gravidade da epidemia e análise do período de 25 de maio a 7 de junho de 2020 (Boletim 5) [Internet]. [cited 2021 nov. 02]. Available from: http://repositorio.ipea.gov.br/bitstream/11058/10073/1/NT_22_Dinte_Covid_19%20e%20medidas%20legais%20de% 20distanciamento%20social_bolet%205.pdf [ Links ]
26.Ramírez JD, Sordillo EM, Gotuzzo E, Zavaleta C, Caplivski D, Navarro JC, Crainey JL, Bessa Luz SL, Noguera LAD, Schaub R, Rousseau C, Herrera G, Oliveira-Miranda MA, Quispe-Vargas MT, Hotez PJ, Paniz Mondolfi A. SARS-CoV-2 in the Amazon region: A harbinger of doom for Amerindians. PLoS Negl Trop Dis. 2020; 14(10): e0008686. DOI: 10.1371/journal.pntd.0008686 [ Links ]
27.Relatório Situacional da COVID-19 no estado do Tocantins [Internet]. [cited 2021 jul. 13]. Available from: http://integra.saude.to.gov br/covid19/RelatorioSituacional [ Links ]
28.Souza CDF, Paiva JPS, Leal TC, Silva LFD, Santos LG. Spatiotemporal evolution of case fatality rates of COVID-19 in Brazil, 2020. J Bras Pneumol. 2020; 46(4): e20200208. DOI: 10.36416/1806-3756/e20200208 [ Links ]
29.Semanas epidemiológicas 33 e 34, de 9 a 22 de Agosto de 2020. Boletim Observatório Covid-19. [Internet]. [cited 2021 jul. 13]. Available from: https://agencia.fiocruz.br/sites/agencia.fiocruz.br/files/u35/boletim_covid_semana_33-34_v13-2020-08-26-_0.pdf [ Links ]
30.Boletim extraordinário de 2 de março de 2021, Boletim Observatório COVID-19. [Internet]. [cited 2021 jul. 14]. Available from: https://agencia.fiocruz.br/sites/agencia.fiocruz.br/files/u35/boletim_extraordinario_2021-marco-03.pdf [ Links ]
31.Governo do Tocantins decide não decretar ponto facultativo no carnaval para evitar aglomerações e proliferação da Covid-19. [Internet]. [cited 2021 jul. 14]. Available from: https://www.to.gov.br/noticias/governo-do-tocantins-decide-nao-decretar-ponto-facultativo-no-carnaval-para-evitar-aglomeracoes-e-proliferacao-da-covid-19/4tejrg5qz9oe [ Links ]
32.RedeVírus MCTI identificou e sequenciou 6 genomas de SARS-CoV-2 de amostras coletadas em Araguaína/TO [Internet]. [cited 2021 jul. 14]. Available from: https://www.gov.br/mcti/pt-br/acompanhe-o-mcti/noticias/2021/03/redevirus-mcti-identificou-e-sequenciou-6-genomas-de-sars-cov-2-de-amostras-coletadas-em-araguaina-to [ Links ]
33.Castro APB, Moreira MF, Bermejo PHS, Rodrigues W, Prata DN. Mortality and Years of Potential Life Lost Due to COVID-19 in Brazil. Int J Environ Res Public Health. 2021 Jul 18; 18(14): 7626. DOI: 10.3390/ijerph18147626 [ Links ]
34.Zimmermann IR, Sanchez MN, Frio GS, Alves LC, Pereira CCA, Lima RTS, Machado C, Santos LMP, Silva END. Trends in COVID-19 case-fatality rates in Brazilian public hospitals: A longitudinal cohort of 398,063 hospital admissions from 1st March to 3rd October 2020. PLoS One. 2021; 16(7): e0254633. DOI: 10.1371/journal.pone.0254633 [ Links ]
35.Musa KI, Arifin WN, Mohd MH, Jamiluddin MS, Ahmad NA, Chen XW, Hanis TM, Bulgiba A. Measuring Time-Varying Effective Reproduction Numbers for COVID-19 and Their Relationship with Movement Control Order in Malaysia. Int J Environ Res Public Health. 2021; 18(6):3273. DOI: 10.3390/ijerph18063273 [ Links ]
36.Ligações rodoviárias e hidroviárias 2016 [Internet]. [cited 2021 jul. 14]. Available from: https://www.ibge.gov.br/apps/ligacoes_rodoviarias/ [ Links ]
37.Rozenfeld Y, Beam J, Maier H, Haggerson W, Boudreau K, Carlson J, Medows R. A model of disparities: risk factors associated with COVID-19 infection. Int J Equity Health. 2020 Jul 29; 19(1): 126. DOI: 10.1186/s12939-020-01242-z [ Links ]
38.Maroko AR, Nash D, Pavilonis BT. COVID-19 and Inequity: a Comparative Spatial Analysis of New York City and Chicago Hot Spots. J Urban Health. 2020; 97(4): 461-470. DOI: 10.1007/s11524-020-00468-0 [ Links ]
39.Smith JA, Judd J. COVID-19: Vulnerability and the power of privilege in a pandemic. Health Promot J Austr. 2020; 31(2): 158-160. DOI: 10.1002/hpja.333 [ Links ]
40.Plano Estadual de Operacionalização da Vacinação Contra a Covid-19 [Internet]. [cited 2021 jul. 14]. Available from: http://integra.saude.to.gov.br/covid19/BaixarArquivoImunizacao/1 [ Links ]
41.Ramírez JD, Sordillo EM, Gotuzzo E, Zavaleta C, Caplivski D, Navarro JC, Crainey JL, Bessa Luz SL, Noguera LAD, Schaub R, Rousseau C, Herrera G, Oliveira-Miranda MA, Quispe-Vargas MT, Hotez PJ, Paniz Mondolfi A. SARS-CoV-2 in the Amazon region: A harbinger of doom for Amerindians. PLoS Negl Trop Dis. 2020; 14(10): e0008686. DOI: 10.1371/journal.pntd.0008686 [ Links ]
42.Cunha, A. Governo do Tocantins Garante que Medidas de Prevenção Serão Mantidas; Prefeitura de Palmas Também Reforça Ações 2020 [Internet]. [cited 2021 jun. 10]. Available from: https://conexaoto.com.br/2020/03/25/governo-do-tocantins-garante-que-medidas-de-prevencao-serao-mantidas-prefeitura-de-palmas-tambem-reforca-acoes [ Links ]
43.Decreto nº 1.859, de 18 de março de 2020. Altera o Decreto nº 1.856, de 14 de março de 2020, que declara situação de emergência em saúde pública no município de Palmas e dispõe sobre medidas de enfrentamento da pandemia provocada pelo coronavírus (COVID-19), nas partes que especifica. [Internet]. [cited 2021 jul. 14]. Available from: https://www.legisweb.com.br/legislacao/?id=391153 [ Links ]
44.Associação brasileira de terapia intensiva, 2020, AMIB apresenta dados atualizados sobre leitos de UTI no Brasil. [Internet]. [cited 2021 nov. 02]. Available from: https://www.amib.org.br/pagina-inicial/ [ Links ]
45.Semana epidemiologica del 4-10 julho 2021. Boletim Observatório Covid-19. [Internet]. [cited 2021 jul. 13]. Available from: https://portal.fiocruz.br/sites/portal.fiocruz.br/files/documentos/boletim_extraordinario_2021-julho.pdf. [ Links ]
46.Touchton M. COVID-19 Observatory. Observatory for the Containment of COVID-19 in the Americas. Brazil'. Observatory Miami. [Internet]. [cited 2021 jul. 14]. Available from: http://observcovid.miami.edu/brazil/ [ Links ]
47.Ferracini R, Maia O, Luz RA da L, Bottura AC, Gomes ACSL, Silva LS da, Azevedo MEA. Observatório socioespacial do Covid-19 no Tocantins. Metodologias E Aprendizado. 2020; 3: 184-191. DOI: https://doi.org/10.21166/metapre.v3i0.1366 [ Links ]
 Correspondence:
Correspondence:
luizcarlos.deabreu@ul.ie
Manuscript received: september 2021
Manuscript accepted: october 2021
Version of record online: november 2021


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}