










Serviços Personalizados
Journal

artigo
 Inglês (pdf)
Inglês (pdf)
 Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
Indicadores
Compartilhar

 Permalink
PermalinkContextos Clínicos
versão impressa ISSN 1983-3482
Contextos Clínic vol.10 no.1 São Leopoldo jan./jun. 2017
https://doi.org/10.4013/ctc.2017.101.02
ARTIGOS
Virtual reality exposure therapy for posttraumatic stress disorder of bank employees: a case study with the virtual bank
Terapia de exposição com realidade virtual para transtorno de estresse pós-traumático para bancários: um estudo de caso com o banco virtual
Julia Candia Donat; Marcio Englert Barbosa; Gustavo Ramos Silva; Christian Haag Kristensen
Pontifícia Universidade Católica do Rio Grande do Sul. Av. Ipiranga, 9981, 90619-900, Porto Alegre, RS, Brasil. juliacdonat@gmail.com, marcio.barbosa@pucrs.br, silva.gustavoramos@gmail.com, christian.kristensen@pucrs.br
ABSTRACT
Exposure Therapy (ET) is an established treatment for Posttraumatic Stress Disorder (PTSD), in which patients gradually confront trauma memories through mental imagery. Virtual Reality Exposure (VRE) is an alternative for those who have difficulties in recreating such memories. Most studies develop VRE scenarios of war or accidents; however, traumatic events in Brazil are mainly of urban violence.
OBJECTIVE: To evaluate the quality of the Virtual Bank scenario through a pilot case study of a banker with PTSD through a cognitive behavioral therapy protocol.
METHOD: A 39-year-old bank employee diagnosed with PTSD through the Structured Clinical Interview for DSM-IV Axis I Disorders (SCID) took part on a Cognitive Behavioral Therapy (CBT) protocol including VRE. Patient's symptoms were assessed through Beck's anxiety and depression inventories, the Screen for Posttraumatic Stress Symptoms and Posttraumatic Cognitions Inventory. The therapy protocol was comprised of 16 sessions divided into three blocks: (i) psychoeducation; (ii) exposure and (iii) cognitive restructuring and relapse prevention. Reassessments were conducted at the end of each block. The sense of presence in the Virtual Bank was assessed through the Presence Questionnaire (PQ).
RESULTS: The patient presented at least 60% of reduction on all instruments and no longer met criteria for PTSD at posttreatment. The greatest reduction on PTSD symptoms scores occurred after the VRE block (-44.8%). The mean score of the PQ was 5.24.
CONCLUSION: CBT protocol with VRE was effective in reducing all measures in this case study. Quality evaluation of the Virtual Bank was positive. Results are promising and similar to those of other innovative case studies using VRE for PTSD.
Keywords: Posttraumatic Stress Disorder, Cognitive Behavioral Therapy, Virtual Reality, Trauma, Exposure Therapy.
RESUMO
A Terapia de Exposição é um tratamento padrão-ouro para o Transtorno de Estresse Pós-Traumático (TEPT), na qual os pacientes confrontam gradualmente as memórias traumáticas por meio de imagens mentais. A Terapia de Exposição por Realidade Virtual é uma alternativa para aqueles que têm dificuldades na formação das imagens mentais. Embora a maioria dos cenários de Realidade Virtual seja de guerra ou acidentes, no Brasil, a maior parte dos eventos traumáticos está relacionado com a violência urbana.
OBJETIVO: Avaliar a qualidade do cenário do Banco Virtual por meio de um estudo de caso piloto com uma bancária com TEPT, através de um protocolo de terapia cognitivo comportamental.
MÉTODO: Uma bancária diagnosticada com TEPT pela Entrevista Clínica Estruturada para o DSM-IV (SCID) foi atendida em um protocolo de Terapia Cognitivo Comportamental (TCC) incluindo a Terapia de Exposição por Realidade Virtual. Os sintomas foram investigados por meio dos Inventários Beck de Ansiedade e Depressão, o Inventário de Cognições Pós-traumáticas e o Instrumento para Rastreio de Sintomas Pós-traumáticos. O protocolo foi composto por 16 sessões divididas em três blocos: (i) psicoeducação; (ii) exposição; e (iii) reestruturação cognitiva e prevenção à recaída. Foram conduzidas reavaliações ao final de cada bloco. A sensação de presença foi medida por meio do Questionário de Presença (QP).
RESULTADOS: A paciente apresentou redução de no mínimo 60% em todos os instrumentos e não fechava critério para TEPT ao final do tratamento. A maior redução nos sintomas de TEPT ocorreu após a exposição (-44,8%). A média do QP foi de 5,24.
CONCLUSÕES: O protocolo foi efetivo na redução de todas as medidas nesse estudo de caso. A qualidade do Banco Virtual foi satisfatória. Os resultados são promissores e semelhantes aos de outros estudos de caso inovadores que usaram ERV para o TEPT.
Palavras-chave: Transtorno de Estresse Pós-Traumático, Terapia Cognitivo Comportamental, Realidade Virtual, Terapia de Exposição.
Introduction
Individuals who survive traumatic events may develop Posttraumatic Stress Disorder (PTSD), a diagnosis encompassing symptoms in the form of intrusions, avoidance of trauma-related stimuli, negative alterations in cognitions and mood and accentuated arousal and reactivity (APA, 2013). Studies in Brazil indicate that 90% of individuals residing in urban centers experience a traumatic event in their lifetime, and between 7% and 11.7% are expected to develop PTSD (Ribeiro et al., 2013).
Strong empirical evidence supports the efficacy of Cognitive Behavioral Therapy (CBT) and Exposure Therapy for the treatment of Posttraumatic Stress Disorder (PTSD) (Rothbaum et al., 2010; Watts et al., 2013). Imaginal Exposure (IE) requires that the patient retell the traumatic event repeatedly, accessing its memory through mental imagery. Since avoidance is a core mechanism of PTSD, many patients might be unwilling or unable to re-experience such memories and to emotionally engage in treatment (Difede and Hoffman, 2002). Virtual Reality Exposure (VRE) is an alternative for those patients, since the visual and auditory stimuli of the Virtual Reality (VR) scenario serve as cues or triggers (e.g., gunfire, vehicle sounds, explosions) to traumatic memories (Difede et al., 2006; Rothbaum et al., 2010). Those cues are usually identified through patients' trauma accounts and can be selectively and gradually included in the VR environment by the therapist (Difede et al., 2006).
VRE procedures often involve an initial assessment of posttraumatic symptoms and the account of details regarding the patient's traumatic event, followed by psychoeducation sessions in which PTSD and/or the treatment rationale are explained. Then, patient is presented to the VR apparatus and is immersed in the VR scenario with as few trauma cues as possible. As sessions progress, these cues are gradually presented and the patient's experience in the scenario becomes increasingly similar to his trauma account (Zimand et al., 2003). Treatment protocols of VRE for PTSD are still in an experimental phase, mainly because most studies have small samples and/or no follow up to sustain their findings (Eichenberg and Wolters, 2012). Still, most studies have shown that VRE is as efficacious as IE in the reduction of PTSD symptoms at posttreatment assessments (Gerardi et al., 2010; Gonçalves et al., 2012; Powers and Emmelkamp, 2008; Rigoli and Kristensen, 2014), what shows the potential of this tool for PTSD treatment.
Clinical studies of VRE for PTSD were at first developed for military populations and are therefore conducted with VR environments that recreate war-related scenarios. There are reports for single case studies of VRE for both Vietnam (Rothbaum et al., 1999) and Iraq (Gerardi et al., 2008; Reger and Gahn, 2008; Tworus et al., 2010) war veterans with significant reductions in PTSD symptoms. Those were followed by studies of war related scenarios with larger samples that maintained the positive results (Gamito et al., 2010; Mc-Lay et al., 2011; Ready et al., 2006; Rizzo et al., 2010; Rothbaum et al., 2001; Wood et al., 2007). McLay et al. (2011), with a sample of 20 Iraq veterans, found evidence of better outcomes following VRE than following traditional CBT.
After September 11, 2001, VRE scenarios related to terrorist attacks became relevant. Recreating the attack in New York, Difede et al. (2007) found a greater improvement in a VRE group compared to a waitlist condition. A terrorist bombing attack in Israel was recreated in a VR scenario, with significant reduction in PTSD symptoms in a case report study maintained at a 6 months follow-up (Freedman et al., 2010). Other VR environments have been used to trigger memories of other situations that may lead to PTSD, such as motor vehicle accidents (Beck et al., 2007; Saraiva et al., 2007) and natural catastrophes (Başoğlu et al., 2003) with significant reduction in PTSD symptoms.
In Brazil, traumatic events are commonly related to urban violence, rather than military service or terrorism. Assaults and robberies are among the most usual forms of interpersonal violence reported (Murray et al., 2013) and are especially frequent in certain contexts, such as banks. Bank heists happen regularly and bank employees are subject to a constant state of insecurity and work-related stress (Bucasio et al., 2005). In addition, these professionals often receive scarce mental health or social support after such events (Schaefer et al., 2011). Since PTSD avoidance symptoms usually keep these patients away from their workplace (where the traumatic events took place), it is also important to promote symptom remission efficiently and effectively to prevent patients' further social and economic burdens.
Concerning the urban profile of Brazilian traumatic events, it is relevant to develop VR environments that allow VRE with civilian trauma victims. For that purpose, a VR scenario called Virtual Bank was created. A VR scenario should have as many realistic cues as possible, which would serve as triggers for the traumatic memories (Rothbaum et al., 2010).
As VRE tasks require gradual presentation of stimuli, it was necessary to create daily-based interactions that would be realistic enough for bank employees to feel present in the VR scenario. Presence is defined as the subjective experience of being in one place or environment, even when one is physically situated in another, and it is often linked with the usefulness of VR environments for VRE (Witmer and Singer, 1998).
This paper aims to depict a VR scenario and illustrate its use in the treatment of a civilian trauma PTSD patient. It also explores preliminary evidence of efficacy of a CBT protocol with VRE on anxiety, depression and posttraumatic symptoms and cognitions. Additionally, as this is the first case study conducted with the Virtual Bank, we aimed to evaluate the quality of the scenario (i.e., ability of generating presence, realism according to the patient).
Method
Participant
The participant of this case study is a 39-year-old bank employee who worked as manager of a bank branch for 10 years. She decided to seek treatment after going through five bank heists. After the last of the heists, in which she had a gun pointed to her head, she claimed to have no support whatsoever from her employers, who coerced her to testify and to recognize the thieves in a police station. After testifying, she was transferred to a branch inside a shopping mall, supposedly safer than the one in which she was working before. However, the new branch contained a monitoring station of bank heists, exposing her to frequent trauma-related stimuli. After a few months working in that agency and five attempts at reallocation, she applied for a work license and decided to seek psychological treatment.
In the initial assessment, patient met criteria for PTSD as assessed with the Structured Clinical Interview for DSM-IV (SCID; First et al., 1997). She had PTSD symptoms such as insomnia, excessive sweating, constant nightmares about the robbery, avoiding entering any bank agency or even talking about the robbery or bank related topics. She was also isolated from family and friends. She was taking daily two types of benzodiazepines (flunitrazepam, 1mg; clonazepam, 15mg) and one antidepressant (citalopram, 20mg).
Procedure
Informed consent was obtained at a preliminary screening interview conducted at the Centre of Studies and Research in Traumatic Stress, an outpatient facility of the Pontifical Catholic University of Rio Grande do Sul (Por-to Alegre, Brazil). This facility offers treatment to trauma victims, and maintains a partnership with the local syndicate of bank employees, which often refers patients to the trauma centre. The patient in this case study was the first to be eligible to the study after the Virtual Bank was ready to be utilized. The partnership with the syndicate of bank employees was the only method of recruitment utilized.
A pre-treatment assessment was conducted by a trained cognitive behavior therapist, who reviewed the inclusion (meeting criteria for PTSD through SCID) and exclusion criteria (presence of psychotic symptoms, cognitive deficits or suicidal ideation). Assessment was conducted in three sessions of approximately one and a half hour each. After the assessment, patient was informed about treatment procedures and scheduled her first treatment session.
The following self-report measures in their Brazilian Portuguese versions were utilized during assessment: (1) Beck Depression Inventory (BDI-II) (Beck et al., 1996; Gorenstein et al., 2011): questionnaire with 21 items in a 4-point Likert scale to investigate depression symptoms; (2) Beck Anxiety Inventory (BAI) (Beck and Steer, 1993; Cunha, 2001): 21 items in a 4-point Likert scale to investigate anxiety symptoms; (3) Screen for Posttraumatic Stress Symptoms (SPTSS) (Carlson, 2001; Kristensen, 2005): The scale contains 17 items in a 10-point Likert scale to screen posttraumatic symptoms, evaluating separately symptoms of avoidance/ numbing, re-experience and hyperarousal; (4) Posttraumatic Cognitions Inventory (PTCI) (Foa et al., 1999; Sbardelotto et al., 2013): The inventory contains 36 items in a 7-point Likert scale, assessing negative posttraumatic cognitions about the world, others and self-blame.
Full assessments were conducted at pretreatment, and after all three blocks of therapy (i.e., after four sessions of psycheducation, after six sessions of VRE and after six sessions of cognitive restructuring and relapse prevention). Additionally, the Presence Questionnaire 4.0 (PQ) (Witmer and Singer, 1998) was applied on the first session of VRE, in order to assess the feeling of presence in a VR environment. Four factors are evaluated (Involvement, Adaptation/Immersion, Sensory Fidelity and Interface Quality) through 32 items on a Likert scale from zero to six.
Apparatus and VR environment
Two laptops were utilized simultaneously during the VRE procedure, one by the therapist (who controlled the "armed robber" avatar) and another by the patient (who controlled the "banker" avatar). Both laptops had an Intel Core i5 processor, 4 gigabytes of RAM and a NVIDIA GeForce GT-730M 2 gigabytes video card. The computers were connected by an Ethernet cable. The VR software was custom-built by a technology solutions company (Urizen ltd.) to allow both avatars to join in a single VR session.
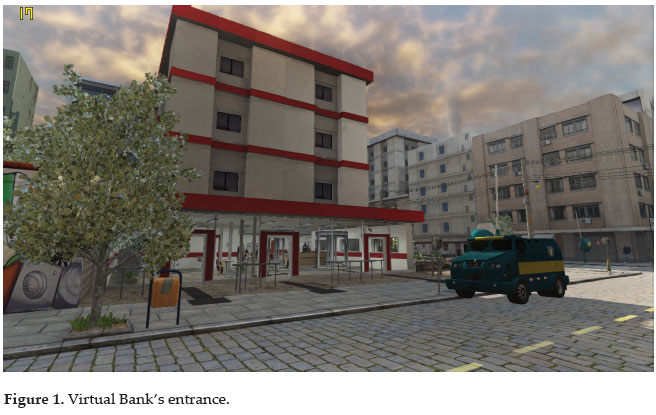
The patient wore a Vuzix iWear VR920 video eyewear, with twin 640x480 LCD screens (equivalent to 62" screens viewed at 9 feet), stereo earphones and integrated head-tracking devices. Both avatars were controlled through the laptops' keyboards and were able to move in the streets surrounding the virtual bank branch and inside the building. The patient was able to trigger certain events when instructed to by the therapist, such as utilizing an ATM or summoning clients that requested random banking services (e.g., opening an account, cashing a check, requesting a loan). The therapist was able (through his avatar) to draw a pistol, fire gunshots, surrender the guards and to take control of the movements of the patient's avatar. The therapist also controlled other stimuli, such as the presence of an armored car, the colors of the bank branch and the robber's body type, skin color and accessories. Figure 1 shows the Virtual Bank's entrance.
Treatment
Treatment protocol included 16 sessions of 50 minutes divided in three blocks. A CBT protocol was conducted as there are certain phases of trauma therapy, such as stabilization and development of a therapeutic relationship, that are recommended to precede the processing of the traumatic experience (Eichenberg and Wolters, 2012). The inclusion of a psychoeducation block is important considering such needs. This first block (Sessions 1 to 4) comprises the following tasks: the therapist explained concepts of cognitive behavioral therapy (e.g., automatic thoughts, schemas) and the cognitive model of PTSD (Ehlers and Clark, 2000), as well as DSM criteria for PTSD. The patient was encouraged to identify which stimuli triggered her avoidance and re-experiencing symptoms. Relaxation exercises (diaphragmatic breathing and muscle relaxation) were also conducted. Homework tasks consisted of practicing relaxation exercises and reviewing treatment goals and expectations.
Sessions 5 to 10 were composed by VRE tasks with the Virtual Bank. In the first session, as recommended by literature (Wiederhold and Wiederhold, 2005), patient was presented to the scenario and how to move around in it. Progressively, during the following sessions, she was stimulated to retell the traumatic event repeatedly, providing more details and exploring the scenario. Aversive stimuli, such as the "robber" avatar, were inserted from the fourth session of VRE.
As homework assignments, the patient was required to listen to the audio recording of every exposure session following the first and to perform in vivo exposure according to an anxiety hierarchy developed in the first exposure session. She decided that the lowest item in the hierarchy would be inviting her family over for dinner, and the highest was to enter the bank agency that she used to work in, at the shopping mall. The patient ceased the use of benzodiazepines before this block of exposure sessions started.
The last block (Sessions 11 to 16) involved cognitive restructuring and relapse prevention. Cognitive restructuring was conducted mostly through Socratic questioning and reevaluation of negative posttraumatic cognitions assessed through the PTCI. The patient had mostly negative cognitions about herself (e.g., thinking she was a weak person for having PTSD) and about the world (e.g., thinking that everyone was dangerous).
Relapse prevention included homework tasks such as listening to exposure audios to find any remaining symptoms and reviewing clinical gains. Furthermore, frequent PTSD comorbidities were explained to the patient and she was trained to notice possible residual symptoms in the future. In the last session, a list of future goals was developed and the importance of social support was reestablished.
Results
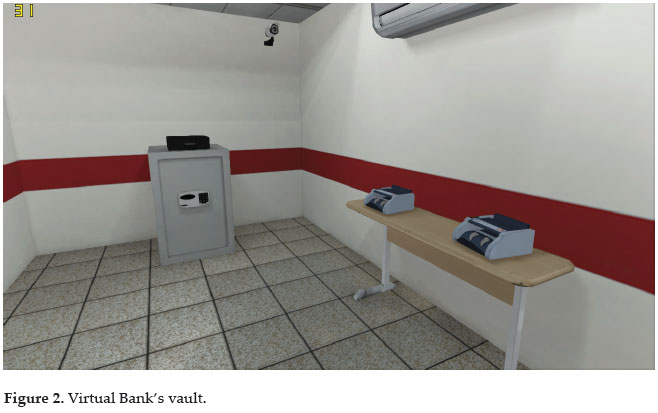
In interviews, patient reported that the Virtual Bank was able to make her feel like she was in an actual bank branch, due to its visual quality and variety of interactions. The vault, showed in Figure 2, was an example of specific stimuli that were important triggers of intrusive memories and psycho-physiological symptoms, such as palpitation. During VRE sessions, the verbal reports and the score on the PQ (M = 5.24, DP = 0.83) indicated an elevated sense of presence in the Virtual Bank.
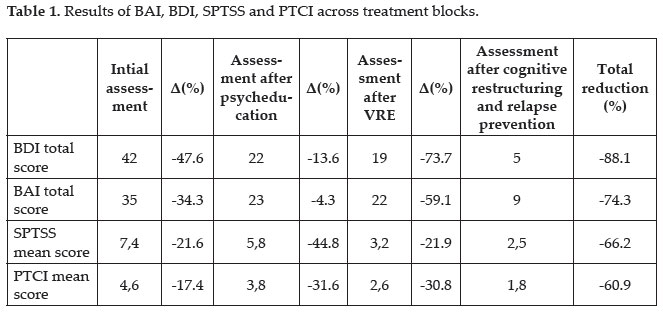
Regarding changes in symptoms across treatment, Table 1 contains all assessment scores for the four self-administered psychological questionnaires (i.e., BAI, BDI, SPTSS, PTCI). Anxiety symptoms, assessed through BAI, decreased slowly from severe in the initial assessment to (1) moderate after psycheducation sessions, (2) low after VRE sessions and (3) minimal after cognitive restructuring and relapse prevention sessions. The biggest reduction in BAI was obtained after the cognitive restructuring and relapse prevention block (-59.1%). Depressive symptoms, assessed through BDI, had a similar path, decreasing from a severe level in the initial assessment to (1) moderate after psycheducation and VRE sessions and (2) minimal after cognitive restructuring and relapse prevention sessions. As in BAI, the biggest reduction in BDI was obtained following the last block of treatment (-73.3%).
Posttraumatic cognitions became less negative during treatment. Even though there is no stablished cut point for the Brazilian version of the PTCI (Sbardelotto et al., 2013), similar reductions in this instrument occurred during the VRE session block (-31.6%) and during the cognitive restructuring and relapse prevention block (-30.8%).
Discussion
The Virtual Bank was an efficacious tool for conducting VRE with a PTSD patient. The patient was able to access her traumatic memories, retell them and imagine them as related to the virtual trauma cues. Even though the PQ has not yet been validated in the Brazilian population, it served as an index for assessing the subjective feeling of "being there" when combined with the patients' reactivity and verbal feedback.
In this case study, CBT with VRE was efficacious for the treatment of PTSD. There was a large pre and posttreatment reduction of symptoms as assessed by all instruments. At the end of treatment, patient did no longer meet criteria for PTSD. As expected, the greatest reduction in posttraumatic symptoms occurred after the VRE sessions, when SPTSS scores went below the cutoff score of 4, proposed as sensitive and specific to PTSD diagnosis (Carlson, 2001). Our protocol preceded symptom score reductions comparable with other similar studies testing novel VR scenarios. In this study, the patient presented a 66.2% reduction of PTSD symptoms at posttreatment. Other studies have found lower rates, such as 55.46% (Gerardi et al., 2008), 49.38% (Reger and Gahn, 2008) and 34% (Rothbaum et al., 1999), with the exception of Freedman et al. (2010), who reported a 100% PTSD symptom reduction, and Difede and Hoffman (2002), who found a 89.1% reduction at posttreatment.
Depressive symptoms presented their greatest reduction after the expected block of therapy (i.e., cognitive restructuring and relapse prevention), even though the patient had already have an important decrease of symptoms after psycheducation sessions. The reduction in depressive symptoms found after our protocol (88.1%) was as good as or even better than that of other novel case report studies of VRE for PTSD. The protocol of Difede and Hoffman (2002) was followed by an 86.4% reduction of symptom scores; Gerardi et al. (2008) found a reduction of only 15.38%; and Rothbaum et al. (1999) reported a 24% reduction. Again, only Freedman et al. (2010) was able to report scores 100% lower at posttreatment, also for depressive symptoms. Reduction in anxiety symptoms were only investigated by Gerardi et al. (2008), with scores lowering 26.32% at posttreatment; and by Rothbaum et al. (1999), who found scores 63% lower following treatment. This time, our protocol have the better results: 74.3%.
Reduction of symptom scores in this study (74%) leads us to believe that the Virtual Bank is an efficacious tool for PTSD treatment because of the similar results when compared to other similar VRE scenarios. It is hard to compare these results properly, as there is not a standardized protocol of VRE for PTSD. Researchers have utilized different types of interventions (i.e., only VRE or combined interventions) and several assessment instruments, what does not allow a proper comparison.
In summary, (1) psychoeducation and relaxation exercises were followed by a general symptom reduction, as observed in previous studies (Okanoya et al., 2015; Shah et al., 2014); (2) VRE seemed to target specific PTSD symptoms; and (3) cognitive restructuring and relapse prevention were followed by a decrease of depression and anxiety symptoms. We expected that anxiety symptoms would decrease more expressively after the relaxation exercises performed during psychoeducation, or even after the VRE sessions. This might be due to a cumulative effect of treatment blocks. However, the reason for this reduction is unclear. Interchanging treatment blocks might be an adequate alternative to investigate this matter in future studies.
Our positive results are similar to other innovative case studies involving VRE. As in the study by Freedman et al. (2010), VR apparently accelerated the effect of exposure. Our hypothesis is that this method may be more effective in activating trauma memories, as it becomes harder for the patient to avoid these memories while being directly exposed to sensory trauma triggers. Once trauma memories are activated, it is also more likely that the patient will emotionally engage in the therapy process, achieving better results (Foa and Kozak, 1986). One way future research could explore this hypothesis is to investigate whether patients who failed to respond to conventional IE because of avoidance would benefit from VRE.
The Virtual Bank, as other VR scenarios described by Beck et al. (2007), Rizzo et al. (2010), McLay et al. (2011), has a range of possibilities in allowing the creation of virtual interactions that match individual feared situations.
We believe that VR scenarios should have enough cues to oppose avoidance mechanisms of PTSD and to allow significant flexibility and control to the therapist. Different styles of VR scenarios exist in literature, with pre-determinated stages of interactions between patient and VR environment (Difede et al., 2007; Gamito et al., 2010) or no triggers at all, allowing free interactions to the patient (Freedman et al., 2011). Future research could investigate differences between treatment protocols with and without the predetermined trauma cues, triggers and interactions inside the VRE scenarios.
The utilization of VRE with a victim of urban trauma is fairly novel, especially in a South American context. Groups at risk for developing PTSD (such as bank employees) might benefit from specific urban VR scenarios, which can be adapted to particularities of different traumatic events in a highly cost-effective manner. Limitations regarding generalization of case studies are well known. Although case studies are a good vehicle for presenting innovative techniques, evidence for effectiveness requires converging results from larger, more generalizable, carefully controlled studies. Our study has another important limitation, common to VRE studies: the lack of follow-up data. We aim to expand sample size and conduct follow-up assessment in order to verify findings. Furthermore, the main change in PTSD diagnosis in DSM 5 (APA, 2013) was the addition of a symptom cluster of alterations in cognitions and mood, which was assessed in the present study through the PTCI. The version of the SCID utilized in our study assessed symptoms of the DSM-IV TR (APA, 2002). There was no validated version of the SCID for the DSM 5 in Brazilian Portuguese at the time we conducted this study. As much as our results are important in demonstrating the potential of VRE, evidence of effectiveness with larger urban samples in controlled studies are required to further understand treatment implications.
References
AMERICAN PSYCHIATRIC ASSOCIATION (APA). 2013. The Diagnostic and Statistical Manual of Mental Disorders: DSM 5. Arlington, American Psychiatric Association, 948 p. [ Links ]
AMERICAN PSYCHIATRIC ASSOCIATION (APA). 2002. Manual diagnóstico e estatístico de transtornos mentais: texto revisado (DSM-IV-TR). Porto Alegre, Artmed, 871 p. [ Links ]
BAŞOĞLU, M.; LIVANOU, M.; ŞALCIOĞLU, E. 2003. A single session with an earthquake simulator for traumatic stress in earthquake survivors. American Journal of Psychiatry, 160(4):788-790. https://doi.org/10.1176/ajp.160.4.788 [ Links ]
BECK, A.T.; STEER, R.A. 1993. Beck Anxiety Inventory: Manual. San Antonio, Psychological Corporation, 23 p. [ Links ]
BECK, A.T.; STEER, R.A.; BROWN, G.K. 1996. Manual for the BDI-II. San Antonio, Psychological Corporation, 38 p. [ Links ]
BECK, J.G.; PALYO, S.A.; WINER, E.H.; SCHWAGLER, B.E.; ANG, E.J. 2007. Virtual reality exposure therapy for PTSD symptoms after a road accident: An uncontrolled case series. Behavior therapy, 38(1):39-48. https://doi.org/10.1016/j.beth.2006.04.001 [ Links ]
BUCASIO, E.; VIEIRA, I.; BERGER, W.; MARTINS, D.; SOUZA, C.; MAIA, D.; FIGUEIRA, I.; JARDIM, S. 2005. Transtorno de estresse pós-traumático como acidente de trabalho em um bancário: relato de um caso. Revista de Psiquiatria do Rio Grande do Sul, 27(1):86-89. https://doi.org/10.1590/S0101-81082005000100011 [ Links ]
CARLSON, E.B. 2001. Psychometric Study of a Brief Screen for PTSD: Assessing the Impact of Multiple Traumatic Events. Assessment, 8(4):431-441. https://doi.org/10.1177/107319110100800408 [ Links ]
CUNHA, J.A. 2001. Manual da versão em português das Escalas Beck. São Paulo, Editora Casa do Psicólogo, 171 p. [ Links ]
DIFEDE, J.; CUKOR, J.; PATT, I.; GIOSAN, C.; HOFFMAN, H. 2006. The application of virtual reality to the treatment of PTSD following the WTC attack. Annals of the New York Academy of Sciences, 1071:500-501. https://doi.org/10.1196/annals.1364.052 [ Links ]
DIFEDE, J.; HOFFMAN, H.G. 2002. Virtual reality exposure therapy for World Trade Center Posttraumatic Stress Disorder: a case report. Cyberpsychology & Behavior: The Impact of the Internet, Multimedia and Virtual Reality on Behavior and Society, 5(6):529-535. https://doi.org/10.1089/109493102321018169 [ Links ]
DIFEDE, J.; CUKOR, J.; JAYASINGHE, N.; HOFFMAN, H.G. 2007. Virtual reality exposure therapy for the treatment of posttraumatic stress disorder following September 11, 2001. Journal of Clinical Psychiatry, 68(11):1639-1647. https://doi.org/10.4088/jcp.v68n1102 [ Links ]
EICHENBERG, C.; WOLTERS, C. 2012. Virtual Realities in the treatment of mental disorders: A Review of the current state of research. In: C. EICHENBERG (ed.), Virtual Reality. Rijeka, Croatia, p. 35-64. https://doi.org/10.5772/50094 [ Links ]
EHLERS, A.; CLARK, D.M. 2000. A cognitive model of posttraumatic stress disorder. Behaviour Research and Therapy, 38(4):319-345. https://doi.org/10.1016/S0005-7967(99)00123-0 [ Links ]
FIRST, M.B.; SPITZER, R.L.; GIBBON, M.; WILLIAMS, J.B.W. 1996. Structured Clinical Interview for DSM-IV Axis I Disorders, clinician version (SCID-CV). Washington, American Psychiatry Press, 84 p. [ Links ]
FOA, E.B.; EHLERS, A.; CLARK, D.M.; TOLIN, D.F.; ORSILLO, S.M. 1999. The Posttraumatic Cognitions Inventory (PTCI): Development and validation. Psychological Assessment, 11(3):303-314. https://doi.org/10.1037/1040-3590.11.3.303 [ Links ]
FOA, E.B.; KOZAK, M.J. 1986. Emotional processing of fear: exposure to corrective information. Psychological Bulletin, 99:20-35. https://doi.org/10.1037/0033-2909.99.1.20 [ Links ]
FREEDMAN, S.A.; HOFFMAN, H.G.; GARCIAPALACIOS, A.; WEISS, P.L.; AVITZOUR, S.; JOSMAN, N. 2010. Prolonged exposure and virtual reality-enhanced imaginal exposure for PTSD following a terrorist bulldozer attack: A case study. Cyberpsychology, Behavior, and Social Networking, 13(1): 95-101. https://doi.org/10.1089/cyber.2009.0271 [ Links ]
GAMITO, P.; OLIVEIRA, J.; ROSA, P.; MORAIS, D.; DUARTE, N.; OLIVEIRA, S.; SARAIVA, T. 2010. PTSD elderly war veterans: a clinical controlled pilot study. Cyberpsychology, Behavior and Social Networking, 13(1):43-48. https://doi.org/10.1089/cyber.2009.0237 [ Links ]
GERARDI, M.; CUKOR, J.; DIFEDE, J.; RIZZO, A.; ROTHBAUM, B.O. 2010. Virtual reality exposure therapy for posttraumatic stress disorder and other anxiety disorders. Current Psychiatry Reports, 12(4):298-305. https://doi.org/10.1007/s11920-010-0128-4 [ Links ]
GERARDI, M.; ROTHBAUM, B.O.; RESSLER, K.; HEEKIN, M.; RIZZO, A. 2008. Virtual reality exposure therapy using a virtual Iraq: Case report. Journal of Traumatic Stress, 21(2):209-213. https://doi.org/10.1002/jts.20331 [ Links ]
GONÇALVES, R.; PEDROZO, A.L.; COUTINHO, E.S.F.; FIGUEIRA, I.; VENTURA, P. 2012. Efficacy of Virtual Reality Exposure Therapy in the Treatment of PTSD: A Systematic Review. PLoS ONE, 7(12):1-7. https://doi.org/10.1371/journal.pone.0048469 [ Links ]
GORENSTEIN, C.; WANG, Y.P.; ARGIMON, I.L.; WERLANG, B.S.G. 2011. Manual do Inventário de Depressão de Beck-BDI-II. São Paulo, Editora Casa do Psicólogo, 172 p. [ Links ]
KRISTENSEN, C.H. 2005. Estresse Pós-Traumático: Sintomatologia e Funcionamento Cognitivo. Porto Alegre, RS. Tese de Douturado. Univesidade Federal do Rio Grande do Sul, 168 p.
MCLAY, R.N.; WOOD, D.P.; WEBB-MURPHY, J.A.; SPIRA, J.L.; WIEDERHOLD, M.D.; PYNE, J.M.; WIEDERHOLD, B.K. 2011. A randomized, controlled trial of virtual reality-graded exposure therapy for posttraumatic stress disorder in active duty service members with combat-related posttraumatic stress disorder. Cyberpsychology, Behavior and Social Networking, 14(4):223-229. https://doi.org/10.1089/cyber.2011.0003 [ Links ]
MURRAY, C.J. et al. 2013. The state of US health, 1990-2010: burden of diseases, injuries, and risk factors. Jama, 310(6):591-606. https://doi.org/10.1001/jama.2013.13805
OKANOYA, J.; KIMURA, R.; MORI, M.; NAKAMURA, S.; SOMEMURA, H.; SASAKI, N.; ITO, Y.; TANAKA, K. 2015. Psychoeducational intervention to prevent critical incident stress among disaster volunteers. The Kitasato Medical Journal, 45(1):62-68. [ Links ]
POWERS, M.B.; EMMELKAMP, P.M.G. 2008. Virtual reality exposure therapy for anxiety disorders: A meta-analysis. Journal of Anxiety Disorders, 22(3):561-569. https://doi.org/10.1016/j.janxdis.2007.04.006 [ Links ]
READY, D.J.; POLLACK, S.; ROTHBAUM, B.O.; ALARCON, R.D. 2006. Virtual Reality Exposure for Veterans with Posttraumatic Stress Disorder. Journal of Aggression, Maltreatment & Trauma, 12(1-2):199-220. https://doi.org/10.1300/J146v12n01_11 [ Links ]
REGER, G.M.; GAHM, G.A. 2008. Virtual reality exposure therapy for active duty soldiers. Journal of Clinical Psychology, 64(8):940-946. https://doi.org/10.1002/jclp.20512 [ Links ]
RIBEIRO, W.S.; MARI, J.J.; QUINTANA, M.I.; DEWEY, M.E.; EVANS-LACKO, S.; VILETE, L.M.P.; FIGUEIRA, I.; BRESSAN, R.A.; MELLO, M.F.; PRINCE, M.; FERRI, C.P.; COUTINHO, E.S.F.; ANDREOLI, S.B. 2013. The Impact of Epidemic Violence on the Prevalence of Psychiatric Disorders in Sao Paulo and Rio de Janeiro, Brazil. PLoS ONE, 8(5):1-13. https://doi.org/10.1371/journal.pone.0063545 [ Links ]
RIGOLI, M.M.; KRISTENSEN, C.H. 2014. Virtual Reality Exposure for PTSD (Posttraumatic Stress Disorder): A Systematic Review Virtual Reality PTSD. Psychology Research, 4(1):1-10. [ Links ]
RIZZO, A.; DIFEDE, J.; ROTHBAUM, B.O.; REGER, G.; SPITALNICK, J.; CUKOR, J.; MCLAY, R. 2010. Development and early evaluation of the Virtual Iraq/Afghanistan exposure therapy system for combat-related PTSD. Annals of the New York Academy of Sciences, 1208(1):114-125. https://doi.org/10.1111/j.1749-6632.2010.05755.x [ Links ]
ROTHBAUM, B.O.; HODGES, L.; ALARCON, R.; READY, D.; SHAHAR, F.; GRAAP, K.; PAIR, J.; HERBER, P.; GOTZ, D.; WILLS, B.; BALTZELL, D. 1999. Virtual reality exposure therapy for PTSD Vietnam Veterans: a case study. Journal of Traumatic Stress, 12(2):263-271. https://doi.org/10.1023/A:1024772308758 [ Links ]
ROTHBAUM, B.O.; RIZZO, A.S.; DIFEDE J. 2010. Virtual reality exposure therapy for combat-related posttraumatic stress disorder. Annals of the New York Academy of Sciences, 1208(1):126-132. https://doi.org/10.1111/j.1749-6632.2010.05691.x [ Links ]
ROTHBAUM, B.O.; HODGES, L.; READY, D.; GRAAP, K.; ALARCON, R.D. 2001. Virtual reality exposure therapy for Vietnam veterans with posttraumatic stress disorder. Journal of Clinical Psychiatry, 62(8):617-622. https://doi.org/10.4088/JCP.v62n0808 [ Links ]
SARAIVA, T.; GAMITO, P.; OLIVEIRA, J.; MORAIS,D.; POMBAL, M.; GAMITO, L.; ANASTÁCIO, M. 2007. The use of VR exposure in the treatment of motor vehicle PTSD: A case-report. Annual Review of CyberTherapy and Telemedicine, 5:199-205. [ Links ]
SBARDELLOTO, G.; SCHAEFER, L.S.; JUSTO, A.R.; LOBO, B.O.M.; KRISTENSEN, C.H. 2013. Adaptation and content validation of the Brazilian version of the Posttraumatic Cognitions Inventory. Revista de Saúde Pública, 47(2):326-334. https://doi.org/10.1590/S0034-8910.2013047003474 [ Links ]
SCHAEFER, L.S.; LOBO, B.O.M.; BRUNNET, A.E.; KRISTENSEN, C.H. 2011. Traumas no trabalho: Impactos da violência para os bancários. In: J.A. NETZ; P.A.B. OLIVEIRA (ed.), Teatro de sombras: Relatório da violência no trabalho e apropriação da saúde dos bancários. Porto Alegre, SindBancários Publicações, p. 25-41. [ Links ]
SHAH, L.B.I.; KLAININ-YOBAS, P.; TORRES, S.; KANNUSAMY, P. 2014. Efficacy of Psycho-education and Relaxation Interventions on Stress-Related Variables in People with Mental Disorders: A Literature Review. Archives of Psychiatric Nursing, 28(2):94-101. https://doi.org/10.1016/j.apnu.2013.11.004 [ Links ]
TWORUS, R.; SZYMANSKA, S.; ILLNICKI, S. 2010. A Soldier Suffering from PTSD Treated by Controlled Stress Exposition Using Virtual Reality and Behavioral Training. Cyberpsychology, Behavior, and Social Networking, 13(1):103-107. https://doi.org/10.1089/cyber.2009.0329 [ Links ]
WATTS, B.V.; SCHNURR, P.P.; MAYO, L.; YOUNGXU, Y.; WEEKS, W.B.; FRIEDMAN, M.J. 2013. Meta-analysis of the efficacy of treatments for posttraumatic stress disorder. The Journal of Clinical Psychiatry, 74(6):e541-e550. https://doi.org/10.4088/JCP.12r08225 [ Links ]
WIEDERHOLD, B.K.; WIEDERHOLD, M.D. 2005. Virtual reality therapy for anxiety disorders: Advances in evaluation and treatment. Washington, American Psychological Association, 225 p. https://doi.org/10.1037/10858-000 [ Links ]
WITMER, B.; SINGER, M. 1998. Measuring presence in virtual environments: A presence questionnaire. Teleoperators and Virtual Environments, 7(3):225-240. https://doi.org/10.1162/105474698565686 [ Links ]
WOOD, D.P.; MURPHY, J.A.; CENTER, K.B.; RUSS, C.; MCLAY, R.N.; REEVES, D.; PYNE, J.; SHILLING, R.; HAGAN, J.; WIEDERHOLD, B.K. 2007. Combat-related posttraumatic stress disorder: a multiple case report using virtual reality graded exposure therapy with physiological monitoring. Studies in Health Technology and Informatics, 132:556-561. [ Links ]
ZIMAND, E.; ROTHBAUM, B.; TANNENBAUM, L.; FERRER, M.S.; HODGES, L. 2003. Technology meets psychology: Integrating virtual reality into clinical practice. The Clinical Psychologist, 56:5-11. [ Links ]
Submetido: 29/07/2016
Aceito: 01/11/2016


{kind=link}
{kind=link}
{kind=link}