










Serviços Personalizados
Journal

artigo
 Inglês (pdf)
Inglês (pdf)
 Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
Indicadores
Compartilhar

 Permalink
PermalinkJournal of Human Growth and Development
versão impressa ISSN 0104-1282
Rev. bras. crescimento desenvolv. hum. vol.22 no.1 São Paulo 2012
ORIGINAL RESEARCH
Influence of the nutritional intervention in complementary feeding practices in infants
Camila Yukie TorigoeI; Leiko AsakuraII; Anita SachsIII; Clarissa Viana Demézio da SilvaIV; Ana Cristina Freitas de Vilhena AbrãoV; Gianni Mara Silva dos SantosVI; Lucíola de Castro CoelhoVII
IDietitian - Federal University of Sao Paulo - UNIFESP
IIProfessor of Nutrition, PhD - Department of Preventive Medicine - Federal University of Sao Paulo - UNIFESP
IIIProfessor of Nutrition, PhD - Department of Preventive Medicine - Federal University of Sao Paulo - UNIFESP
IVDietitian, MS - Department of Preventive Medicine - Federal University of Sao Paulo - UNIFESP
VProfessor of Nursing, PhD - coordinator of Center for Promotion and Support of Breastfeeding / Human Milk Bank - Federal University of Sao Paulo - UNIFESP
VIProfessor of Statistics, MS - Federal University of Sao Paulo - UNIFESP
VIIDietitian - Department of Preventive Medicine - Federal University of Sao Paulo - UNIFESP
ABSTRACT
The objective of the present study was to evaluate the effectiveness of nutritional guidance to lactating infants undergoing the phase of complementary feeding introduction and to verify the association of food practices with age and maternal education. It is a descriptive historical cohort study in which secondary data were evaluated from 92 lactating infants who had at least 3 nutritional counselings at the "Center for Promotion and Support of Breastfeeding" from the Federal University of Sao Paulo (UNIFESP), between October 2005 and March 2010. The information of food consumption was obtained from 24 hours food records which were qualitatively analyzed according to the presence of food groups (cereals/tubers, beef/egg, legumes, fruits/vegetables). The nutritional guidance for the introduction of the complementary food was based on the 10 Steps of a Healthy Diet for Brazilian Children under 2 years of age from the Health Ministry. For the Block Non-parametric Variance Analyses children were separated in 2 groups (Lac A = those who were already on a supplementary feeding; Lac B = those who were not on a supplementary feeding). The means and standard deviations of the number of food groups consumed at moments 0,1 and 2 for Lac A were 2.3 (SD = 0.8); 2.9 (SD = 0.8) and 3.2 (SD = 0.6), respectively. For Lac B at times 1 and 2 were 2.6 (SD = 0.9) and 3.1 (SD = 0.7), respectively. There was a statistic increase of the food groups with time for Lac A (moments 0 - 1 (p = 0.001), 0 - 2 (p < 0.001), 1 - 2 (p = 0.033)) and Lac B (moments 1 - 2 (p < 0.001)). Among the inadequate offered foods, those which had reduction were sugar (from 22.2% to 8.7%) and "petit suisse" cheese (from 11.1% to 4.3%). No relation between the presence of food groups and age and maternal education was observed. The nutritional orientation over time was effective what resulted in a better quality of the complementary feeding, independent of age and maternal education.
Key words: supplementary feeding; infant; food consumption.
INTRODUCTION
Breast milk is able to fulfill all the needs of an infant during the first months of life. However, up to six months of age, complementary feeding is essential with introduction of adequate quali-quantitative food to meet the nutritional needs and prevent infant morbid-mortality.
The introduction of inappropriate complementary feeding practices may result in several damages to children´s growth and development. The early introduction of complementary feeding increases the children morbid-mortality rate due to the reduced intake of protective factors present in breast milk. Children also become more vulnerable to infectious diseases and malnutrition, mainly within children living in poor environment. It also interferes with nutrient absorption of breast milk, such as iron and zinc, and increases the possibility of food allergy2-4. On the other hand, the late introduction of foods is also unfavorable once breast milk alone does not meet the energy requirements of infants resulting in the decrease of growth, increasing the risk of malnutrition and micronutrient deficiencies1.
Considering the introduction of food practices, the role of the mother should be emphasized as she is the main reference to provide the child care. Thus, it is crucial that mothers and relatives receive orientation to the appropriate introduction of complementary feeding5. It is known that maternal care is essential to the children's health and that schooling and the age of the mother , besides time the mother has available to take care of her child may affect information regarding health.
Despite the fact that important advances in the promotion of breastfeeding have occurred in the last years, the promotion of adequate complementary feeding has had a lower progress. Although these actions depend on healthcare professionals and mothers, their executions and final success also depend on the definition of adequate governmental policies as well as participation and civil supports of the whole society2.
Some programs of nutrition education intervention were performed in developing countries in order to provide information and motivation to caretakers to modify feeding practices. These studies showed evidences that educational intervention may improve the caretakers´ food practices and child´s food intake7,8.
Due to the importance of these right practices and their reflections on the development of lactating infants, the objective of this study was to evaluate the effectiveness of the nutritional guidance of lactating infants undergoing the phase of complementary feeding introduction and to verify the association of food practices with age and maternal education.
METHODS
It was a descriptive historical cohort study in which secondary data were evaluated from lactating infants undergoing the phase of complementary feeding introduction and attending the Infant Nutrition Clinic of "Center for Promotion and Support of Breastfeeding" (CIAAM) of the Federal University of Sao Paulo (UNIFESP), Brazil.
CIAAM has the aim of promoting the necessary assistance to the establishment and maintenance of breastfeeding to lactating women, carried out by an interdisciplinary team, including obstetric nurse, pediatrician, neonatologist, nutritionist and psychologist.
The admission of mother-child pair at CIAMM takes place, in most cases, through Breastfeeding Outpatient Clinic which receives mothers whose children were born in Hospital Sao Paulo (HSP-UNIFESP), as well as other Birthing Centers. Mother and child remain on follow-up at the outpatient clinic while keeping exclusive breastfeeding. After the introduction of another food which is non maternal milk or when lactating infants are 6 months, mother-child pair is sent to pediatrician and Infant Nutrition Clinic to follow-up.
In rare situations, lactating infants between 6 and 12 months are sent by others Outpatient Clinics from UNIFESP and attended by the nutrition outpatient clinic. Infant Nutrition Clinic is composed of trained nutritionists who counsell lactating infants individually till one year old being the frequency of these consultations is based on the "Minimal Calendar of Consultation for Assistance to the Child" from Brazilian Ministry of Health9. It is also determined by the current situation of the lactating infants in relation to the introduction of food and their individual demand, occurring monthly or every two months.
The nutritional orientation given to mothers in all consultations are qualitative, done verbally and transcribed in proper hard copy and based on the Ten Steps of a Healthy Diet for Brazilian Children under 2 years of age from the Health Ministry which are:
(1) Breast milk should be given up to 6 months, with no water, teas or any other foods;
(2) From 6 months on, other foods should be slowly and gradually introduced, maintaining breast milk in the diet until two years of age or more;
(3) After 6 months, complementary foods (cereals, tubers, meat, fruit and vegetables) should be given three times a day, if child receives breast milk;
(4) The complementary feeding should be offered according to family mealtime, with regular intervals and respecting the child´s appetite;
(5) Complementary feeding should be thick since the beginning and given with a spoon, beginning with pasty foods (mashes/ purees) and, gradually, increase the consistency until the child is eating family meals;
(6) Different types of foods should be offered each day. A variety of food is a colorful plate;
(7) Stimulate the daily consumption of fruits and vegetables in meal time;
(8) Avoid sugar, coffee, canned food, fried food, sodas, candies, snacks and other sweets during the first years and use salt in moderation;
(9) Hygiene and cares during the preparation and manipulation of foods should be followed in order to guarantee adequate storage and conservation;
(10) Stimulate sick and convalescent child to eat, offering the preferred food, respecting his/ her acceptance.
The complementary feeding is composed of a set of foods, in addition to breast milk, offered during the period of breastfeeding, in the first year of life. However, these foods may be or not suitable for the child, such as tea and water with sugar, cow's milk etc1.
In order to develop this study, data were gathered from the children´s medical records counselled between October 2005 and March 2010, totalizing 272 records. From these records, 60 were excluded because they were preterm lactatings, 87 attended only 1 or 2 nutritional consultations and 33 had incomplete data, totalizing a sample of 92 children´s medical records that performed at least 3 nutritional consultations.
Age, marital status, schooling and mother parity and gender, age of nutritional follow-up, weight and food consumption of lactating were investigated in each consultation.
Information regarding food consumption of lactating children was obtained from 24 hours Food Records (R24h) collected during three nutritional counselings, named moment 0 (first consultation), moments 1 and 2 (subsequent consultations). Qualitative analysis of lactating infant feeding was based on the presence of foods in R24h, according to food groups contained in Step 3 (cereals/tubers, meat/egg, legumes, fruits/vegetables) and those which were avoided in the first year of life, contained in Step 8, presented in the "Ten Steps of a Healthy Diet for Brazilian Children under 2 years of age"10.
To punctuate the number of food groups in Step 3 which was presented in each R24h evaluated at the different moments, it was considered the presence of at least one food from the group cereals/ tubers, meat/egg, legumes and from the group fruits/vegetables, the presence of at least a combination of fruit and vegetable.
It was also determined a time interval between each consultation in months, being T0-1, the interval between 0, 1 and T1-2, the interval between moments 1 and 2.
The evolution of children´s nutritional status was showed considering the age and weight measured in those three nutritional counselings. Those data were converted into Score-Z weight/age and classified according to the growth curve proposed by World Health Organization11.
As weight measuring instrument, a digital pediatric scale (Filizola BP Baby®) with capacity/ division of 15kg/5g and technical standards of measurement were applied according to anthropometric album of System of Food and Nutritional Surveillance (SISVAN)12.
Statistical analysis was initially performed descriptively. To the quantitative variables, some summary-measures were calculated such as mean, standard deviation (sd), minimum and maximum values. The quantitative variables were analyzed through the absolute and relative frequency calculations.
Inference analyses used to confirm or not the evidences found in the descriptive analyses were: Block non-parametric variance analyses, to evaluate the number of food groups consumed at moments 0, 1 and 2, and multiple linear regression model to evaluate the relationship among the number of consumed food groups and age and mother schooling. To analyze the Block Non-parametric Variance Analyses children were separated in 2 groups (Lac A = those who were already on a complementary feeding; Lac B = those who were not on a complementary feeding).
A 5% significance level of was used for the inferential analyses obtained. Data were stored in electronic spreadsheets (Microsoft Excel® 2007) for Windows and statistical analyses and charts were done using Statistical Package for the Social Sciences software, version 15.0 for Windows ND r-Program version 2.11.1. Anthro 2005 software was used to analyze anthropometric data.
The study was approved by the Research Ethics Committee from UNIFESP/EPM (nº 0880/10).
RESULTS
The selected sample was composed of 92 lactating infants, being 54 boys (58.7%). Children mean age at the beginning of the nutritional follow-up was 6.2 months, ranging from four to eight months, with standard deviation of 0.9 month.
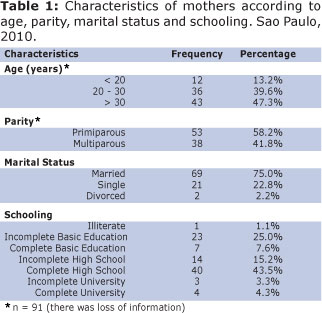
According to Table 1, approximately 43 mothers (47.3%) were more than 30 years old, 53 were primiparous (58.2%) , 69 were married (75.0%) and 40 had complete high school (43.5%).
Thirty two children (34.8%) arrived in the first counseling receiving solid foods (group LAC A), that is, the introduction of complementary feeding initiated. Children mean age of this group was 6.7 months, ranging from five to eight months, with standard deviation of 0.8 month. The group of children who arrived in the first counseling without receiving complementary feeding (group Lac B), presented mean age of 6.0 months, ranging from four to eight months, with standard deviation of 0.9 month.
At moments 1 and 2, children mean age of group Lac A was 8.0 months (sd = 1.1 months) and 9.8 months (sd = 1.1 months), respectively. Children mean age of group Lac B was 7.3 months (sd=1.4 months) at moments 1 and 2 and 9.1 months (sd=1.6 months), respectively. The mean time interval between the first and second counseling in group Lac A was 1.5 months (sd = 0.6 month) and between the second and third counseling was 1.7 months (sd = 0.6 month). In the group Lac B, the mean time interval, between the first and second counseling was 1.4 months (sd = 1.1 months). The mean time interval between the second and third counselings was 1.7 months (sd=0.9 month).
Referring to the feeding characteristics in the first counseling, 80 children (87.0%) received breast milk. Forty nine children (53.3%) used baby bottle being five (10.2%) with sugar, six (12.2%) with food thickener and four (8.2%) with both.
Among inadequate foods offered to children in the first year, there was the addition of sugar in milk and juice and petit suisse cheese. It was observed that at moment 0 the intake of sugar and petit suisse were 22.2% and 11.1%, reducing to 7.1% and 7.1% at moment 1 and after increasing to 8.7% and 4.3% at moment 2, respectively, for the total sample.
According to Figures 1 and 2, it was observed an increase intake of food groups (cereals/tubers, meat/egg and legumes) over time, for both groups.
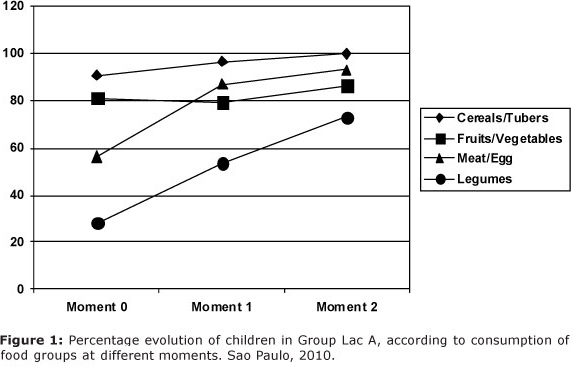
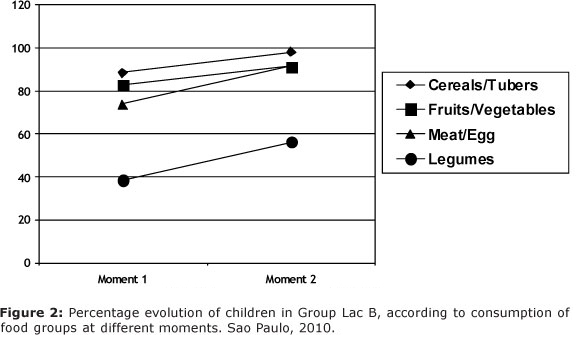
Regarding the intake of food groups at moments 0, 1 and 2, the group Lac A presented mean of 2.3 (sd = 0.8), 2.9 (sd = 0.8) and 3.2 (sd = 0.6), respectively, while group Lac B at moments 1 and 2 presented mean of 2.6 (sd = 0.9) and 3.1 (sd = 0.7), respectively. In group Lac A at the moment 0 there was a lower number of offered food groups when comparing to moment 1 (p = 0.001) and to moment 2 (p < 0.001). The moment 1 showed lower number of offered food groups with regard to moment 2 both for group Lac A (p = 0.033) and group Lac B (p < 0.001).
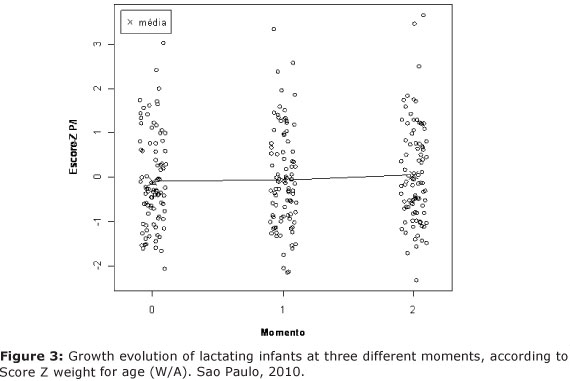
Referring to children nutritional status, the weight for age mean values of Scores Z at moments 0, 1 and 2 were - 0.09 (sd = 1.05), - 0.05 (sd = 1.10) and 0.06 (sd = 1.11), respectively, being that most part of the population was adequate (Score - z d" - 2 and < + 2), as observed in Figure 3.
When relating the number of offered food groups with age and maternal education it was not observed, at all moments, a relationship between number of food groups, age and maternal education. Only at moment 2 it was observed a tendency with maternal education (p = 0.051), the more schooling the higher number of consumed food groups.
DISCUSSON
The results in this present study showed that most part of the children has already received breast milk at the beginning of the follow-up, but more than a half has already been using baby bottle. National data14 from the II Breastfeeding Prevalence Research (II PPAM) showed that the probability of a child to be breastfeeding at 180 days of life was 72.0% and 77.6%, in Sao Paulo and Brazil, respectively, being the values lower when compared to the present study. Referring to the use of baby bottle, the same study showed that approximately 65.0% and 58.0% of children under 12 months used it in Sao Paulo and Brazil, respectively, showing that it was a very prevalent practice among Brazilian mothers.
Additionally to the use of baby bottle, the addition of some components in the milk such as sugar and food thickener were frequent in this present study and in a research carried out in three Brazilian cities, which showed a high frequency of sugar, cereal and chocolate addition in food preparation, even for children under six months15.
The introduction of sugar in feeding, when it is a phase that the child is building his/ her habits, may contribute to a higher intake of this kind of food. Preparations such as milk and chocolate, porridge, sweet and stuffed cookies please children, taking them to big quantities of food consumed, increasing the total energy value of the diet and the risk of overweight and obesity16.
In the period prior to the intervention, the intake of petit suisse cheese was relatively high, supporting other studies carried out in different parts of Brazil which showed an important participation of this kind of food in the diet of children under two years old.6,17. Notwithstanding, when evaluating the addition of sugar in milk and juice at moment 0 and after at moment 2, a reduction of this food intake was observed.
Positive results of a nutritional intervention were also observed in the study from Vitolo et al., 201018, who verified that sugar was introduced lately at the intervention group compared to the control group, and the previous intake of foods such as cookies, petit suisse cheese, honey and soda were higher in the control group. The consumption of snacks in the first year of life was 40.0% lower in the intervention group.
In the present study it was observed that one third of the children has already arrived in the first counseling receiving some solid foods, before six months of life, supporting other data from II PPAM14, in which approximately ¼ of the children from three to six months had salty foods and fruits. The reasons that mothers offered an early feeding were not investigated in that occasion. In a study performed by Caetano et al., 201015, , mothers reported that infant food practices were, mainly, based on their own life experience or their families' habits, and the second and third places were the pediatrician and media, respectively.
When analyzing qualitatively the food offered to these children at moment 0 it was observed low presence of the food groups beef/ egg and legumes, food sources of important nutrients to infant development such as iron.
Similar results, when some foods were introduced, were observed in other studies, which verified that fruits were in the first block of foods to be introduced in children´s feeding while the foods considered source of iron (beans and meat) were incorporated later to diet .
There was a study which verified that even the mothers who received orientation on introduction of complementary feeding by a professional nurse, 79.2% of children did not have an adequate feeding introduction as emphasized by Health Ministry. Among several reasons given by the mothers to justify why they did not follow-up the orientation, were the child´s non-acceptance, grandmothers interference and comfort and practice in preparation and offer of porridge in relation to salty food. These findings, together with the present study, support the idea that the orientation processes should be constant, once the number of food groups in children´s feeding increased significantly according to performed counseling, for both groups of children, showing a positive effect on done interventions, once it is recommended that the child should consume all food groups from six months of year n.
The results of the nutritional evaluation in the present study showed a frequency of weight deficit under national mean, with children at the same age, 1.8% and 3%, respectively, according to data from National Demographic and Health Survey 2006 (PNDS, 2006) 22.
Despite the results in the present study did not show any relationship among the presence of food groups with age and maternal education, other studies showed association among low education and maternal age with inadequate infant feeding practices6,23,24
A study conducted by Corrêa et al., 20096 showed that mothers with less than eight years of schooling presented more chances to offer bread group foods, sweets, starch and milk, showing that mothers with lower school education and a per capita income lower than the basic salary tend not to offer frequently foods with fruits and vegetables. In a study with American mothers, it was also observed that a lower offer of fruits and vegetables, and also the introduction of cow milk before 12 months, were more prevalent among mothers with low school education. However, it should be noticed that all mothers have received the same orientations to complementary feeding introduction in this present study, regardless of age and maternal education, what may have contributed to the lack of results referring to the association among the factors.
Additionally, an analyzes done in five European countries showed that the early introduction of complementary feeding occurred in 37% of formula-fed infants and 17% of breast-fed infants, being that younger mothers (d" 25 years) of feeding children with infant formula, introduced solid foods significantly earlier during the first four months of life, and also the lower maternal education increases in 1.8 the risk of introducing some solid foods at the fourth month of age.
Currently, due to the high prevalence of overweight/ obesity for both infants and adults, the concern for the adequate practice of the introduction of complementary feeding becomes essential to avoid future nutritional risks. According to data from PNDS 200622, the prevalence of weight for height excess in Brazilian children under five years old, was of 6.6%, showing a moderate risk of obesity exposure in infants and the necessity of attention to the feeding of this population.
A study from Schack-Nielsen et al., 201025 based on a Danish cohort with approximately 5,000 individuals indicated that early introduction of complementary feeding may be associated with an increased Body Mass Index (BMI) and risk of overweight in adulthood. Per 1-month delay of later introduction of complementary feeding (considering ages 2-6 months), the risk of obesity at 42 years old was reduced to 6-10%.
The application of nutritional intervention programs in this stage of the feeding transition is also necessary to promote improved nutrient adequacy of lactating infants and caregiver behaviors. The results of the studies on childhood and infant feeding indicate that food practices may have positive results in growth and development, especially in developing countries.7,8,26,27. According to the results found in this study, the interventions were effective once the feeding qualitative composition of lactating infants improved over time.
Family environment, parents' life style and interfamilial relationship have great influence on lactating infants feeding and on their feeding preferences and may affect the energetic balance on feeding by the availability and composition of foods28. Other important fact is related to the way of selection and choice of foods employed in feeding in different social classes. Such choices are defined by economic, cultural and social specificity, including psychological reasons for acceptance or rejection of foods 6.
One limitation of this present study is the lack of familiar income data as it is a factor that may interfere in the acquisition and offer of foods. It is also important to notice that the limitations regarding retrospective studies, based on medical record reviews, take to loss of information and used tools to analysis qualitatively the feeding, once R24h is a single day-intake and, probably, configures only a few representativeness of children usual consumption.
The finding results suggest that nutritional orientation over time was effective and resulted in a better quality of the complementary feeding, independent of age and maternal education. Nevertheless, other studies are needed in order to identify the main maternal difficulties in this phase so as to improve applied intervention programs.
REFERENCES
1. Brasil. Ministério da Saúde/Organização Pan-Americana da Saúde. Guia alimentar para crianças menores de 2 anos de idade. Série A. Normas e manuais técnicos. Brasília: Ministério da Saúde; 2002. [ Links ]
2. Monte CMG, Giugliani ERJ. Recomendações para alimentação complementar da criança em aleitamento materno. J Pediatr. 2004; 80 (Supl 5):S131-41. [ Links ]
3. Dias MCAP, Freire LMS, Franceschini SCC. Recomendações para alimentação complementar de crianças menores de dois anos. Rev Nutr. 2010; 23(3):475-86. [ Links ]
4. Michaelsen KF, Larnkjaer A, Lauritzen L, Molgaard C. Science base of complementary feeding practice in infancy. Curr Opin Clin Nutr Metab Care. 2010; 13(3) 277-83. [ Links ]
5. Brasil. Ministério da Saúde. Secretaria de Atenção à Saúde. Departamento de Atenção Básica. Saúde da criança: nutrição infantil: aleitamento materno e alimentação complementar. Série A. Normas e manuais técnicos. Brasília: Ministério da Saúde; 2009. [ Links ]
6. Corrêa EM, Corso AC, Moreira EAM, Kazapi IAM. Alimentação complementar e características maternas de crianças menores de dois anos de idade em Florianópolis (SC). Rev Paul Pediatr. 2009; 27(3):258-64. [ Links ]
7. Hotz C, Gibson RS. Participatory nutrition education and adoption of new feeding practices are associated with improved adequacy of complementary diets among rural Malawian children: a pilot study. Eur J Clin Nutr. 2005; 59(2):226-37. [ Links ]
8. Bhandari N, Mazumder S, Bahl R, Martines J, Black RE, Bhan MK. An Educational Intervention to Promote Appropriate Complementary Feeding Practices and Physical Growth in Infants and Young Children in Rural Haryana, India. J Nutr. 2004; 134(9): 2342-48. [ Links ]
9. Brasil. Ministério da Saúde. Secretaria de Políticas de Saúde. Departamento de Atenção Básica. Saúde da criança: acompanhamento do crescimento e desenvolvimento infantil / Ministério da Saúde. Secretaria de Políticas de Saúde. Brasília: Ministério da Saúde; 2002. [ Links ]
10. Brasil. Ministério da Saúde/Organização Pan-Americana da Saúde. Dez passos para uma alimentação saudável: guia alimentar para menores de dois anos: um guia para o profissional da saúde na atenção básica. Série A. Normas e manuais técnicos. Brasília: Ministério da Saúde; 2010. [ Links ]
11. World Health Organization. Multicentre Growth Reference Study Group. WHO Child Growth Standards: Length/height-for-age, weight-for-age, weight-for-length, weight-for-height and body mass index-for-age: Methods and development. Geneva: WHO; 2006. [ Links ]
12. Vigilância alimentar e nutricional - Sisvan: orientações básicas para a coleta, processamento, análise de dados e informação em serviços de saúde / [Andhressa Araújo Fagundes et al.]. - Brasília: Ministério da Saúde, 2004. Disponível em http://189.28.128.100/nutricao/docs/geral/orientacoes_basicas_sisvan.pdf. Acesso em 03 de outubro de 2011. [ Links ]
13. Neter J, Kutner MH, Nachtsheim CJ, Wasserman W. Applied linear statistical models. 4. ed. Boston: Irwin, 1996. [ Links ]
14. Brasil. Ministério da Saúde. II Pesquisa de Prevalência de Aleitamento Materno nas Capitais Brasileiras e Distrito Federal. Brasília: Ministério da Saúde; 2009. [ Links ]
15. Caetano MC, Ortiz TTO, Silva SGL, Souza FIS, Sarni ROS. Alimentação complementar: práticas inadequadas em lactentes. J Pediatr (Rio J). 2010; 86(3):196-201. [ Links ]
16. Simon VGN, Souza JMP, Souza SB. Aleitamento materno, alimentação complementar, sobrepeso e obesidade em pré-escolares. Rev Saúde Pública. 2009; 43(1):60-9. [ Links ]
17. Oliveira LPM, Assis AMO, Pinheiro SMC, Prado MS, Barreto ML. Alimentação complementar nos primeiros dois anos de vida. Rev Nutr. 2005; 18(4):459-69. [ Links ]
18. Vitolo MR, Bortolini GA, Feldens CA, Drachler ML. Impactos da implementação dos dez passos da alimentação saudável para crianças: ensaio de campo randomizado. Cad Saúde Pública. 2005; 21(5):1448-57. [ Links ]
19. Simon VGN, Souza JMP, Souza SB. Introdução de alimentos complementares e sua relação com variáveis demográficas e socioeconômicas, em crianças no primeiro ano de vida, nascidas em Hospital Universitário no município de São Paulo. Rev Bras Epidemiol. 2003; 6(1):29-38. [ Links ]
20. Modesto SP, Devincenzi UM, Sigulem DM. Práticas alimentares e estado nutricional de crianças no segundo semestre de vida atendidas na rede pública de saúde. Rev Nutr. 2007; 20(4):405-15. [ Links ]
21. Santos CS, Lima LS, Javorski M. Fatores que interferem na transição alimentar de crianças entre cinco e oito meses: investigação em Serviço de Puericultura do Recife, Brasil. Rev Bras Saúde Matern Infant. 2007; 7(4):373-80. [ Links ]
22. Brasil. Ministério da Saúde. Pesquisa Nacional de Demografia e Saúde da Criança e da Mulher - PNDS 2006: Dimensões do Processo Reprodutivo e da Saúde da Criança. Brasília: Ministério da Saúde; 2009. [ Links ]
23. Fein SB, Labiner-Wolfe J, Scanlon KL, Grummer-Strawn LM. Selected Complementary Feeding Practices and Their Association With Maternal Education. Pediatrics. 2008; 122 (Suppl 2):S91-7. [ Links ]
24. Schiess S, Grote V, Scaglioni S, Luque V, Mortin F, Stolarczyk A et al. Introduction of Complementary Feeding in 5 European Countries. J Pediatr Gastroenterol Nutr. 2010; 50(1):92-8. [ Links ]
25. Schack-Nielsen L, Sorense TI, Mortensen EL, Michaelsen KF. Late introduction of complementary feeding, rather than duration of breastfeeding, may protect against adult overweight. Am J Clin Nutr. 2010; 91(3):619-27. [ Links ]
26. Saha KK, Frongillo EA, Alam DS, Arifeen SE, Persson LA, Rasmussen KM. Appropriate infant feeding practices result in better growth of infants and young children in rural Bangladesh. Am J Clin Nutr. 2008; 87(6):1852-9. [ Links ]
27. Shi L, Zhang J, Wang Y, Caulfield LE, Guyer B. Effectiveness of an educational intervention on complementary feeding practices and growth in rural China: a cluster randomised controlled trial. Public Health Nutr. 2009; 13(4):556-65. [ Links ]
28. Vieira GO, Silva LR, Vieira TO, Almeida JAG, Cabral VA. Hábitos alimentares de crianças menores de 1 ano amamentadas e não-amamentadas. J Pediatr. 2004; 80(5):411-16. [ Links ]
 Corresponding author:
Corresponding author:
lccoelho@unifesp.br
Manuscript submitted Aug 09 2011
Accepted for publication Oct 16 2011.
Center for Promotion and Support of Breastfeeding / Human Milk Bank and Department of Medicine - Federal University of Sao Paulo - UNIFESP
