










Serviços Personalizados
Journal

artigo
 Inglês (pdf)
Inglês (pdf)
 Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
Indicadores
Compartilhar

 Permalink
PermalinkJournal of Human Growth and Development
versão impressa ISSN 0104-1282versão On-line ISSN 2175-3598
J. Hum. Growth Dev. vol.31 no.1 Marília jan./abr. 2021
https://doi.org/10.36311/jhgd.v31.11084
ORIGINAL ARTICLE
Socioeconomic characteristics influence attitudes towards sexuality in adolescents
Juliani da Silva Araújo AlvesI; Silvana Granado Nogueira da GamaII; Maria Carmen Moldes VianaIII; Katrini Guidolini MartinelliIV; Edson Theodoro dos Santos NetoIII
IPrograma de Pós-graduação em Saúde Coletiva. Mestre em Saúde Coletiva. Federal University of Espirito Santo. Vitoria. Espírito Santo. CEP: 29040-090. Brazil
IIEscola Nacional de Saúde Pública Sérgio Arouca. Pesquisadora do Departamento de Métodos Quantitativos. Oswaldo Cruz Fundation. Rio de Janeiro. Rio de Janeiro. CEP: 21041-210. Brazil
IIIPrograma de Pós-graduação em Saúde Coletiva. Professor da Pós-graduação. Federal University of Espirito Santo. Vitoria. Espirito Santo. CEP: 29040-090. Brazil
IVPrograma de Pós-graduação em Saúde Coletiva. Pós-doutoranda em Saúde Coletiva. Federal University of Espirito Santo. Vitoria. Espirito Santo. CEP: 29040-090. Brazil
ABSTRACT
BACKGROUNG: Attitudes Towards Sexuality in Adolescents (ATSA) are built according to the experiences and different social contexts.
OBJECTIVES: to analyze attitudes towards sexuality itself, according to socioeconomic factors in adolescents aged.
METHODS: Cross-sectional school-based study was carried out with 2,292 adolescents enrolled in high school, in 54 schools, through interviews using the Attitudes Toward Sexuality in Adolescents (AFSA) instrument that has four dimensions, and measures the Permissiveness, Communion, Instrumentality and Sexual Practices. Then, the attitude of each adolescent was classified as: unfavorable, indifferent and favorable. Pearson's Chi-square test and Multinomial Logistic Regression were used in statistical analyses.
RESULTS: It was verified that the majority of the adolescents presented unfavorable AFSA, being these behaviors directly associated to: age of 15/16 and 17 years (OR=0.59; OR=0.47); lower secondary education (OR=2.03); adolescent's head of family having low education (OR=2.00); to live with the partner (OR=2.77); race / color black (OR=2.04) and brown (OR=1.88); and lower family income (OR=2.50).
CONCLUSION: Adolescents with lower socioeconomic status are more likely to have unfavorable attitudes towards their own sexuality.
Keywords: sexuality, adolescent health, sex education, unprotected sex.
Authors summary
Why was this study done?
Epidemiological studies on adolescents aged 15 to 19 years, late adolescence, are scarce in Brazil. In this age group, sexual initiation occurs for most adolescents. Therefore, the investigation of attitudes towards sexuality becomes relevant to identify elements that can function as risk factors for the health of adolescents and their insertion in adulthood.
What did the researchers do and find?
From an epidemiological investigation, with a representative sample in high schools in a Brazilian metropolitan region, attitudes towards sexuality in adolescents and the social factors that determine more favorable and less favorable attitudes were investigated. The result of the Multinominal Logistic Regression identified an adolescent profile that has a greater chance of developing unfavorable attitudes towards sexuality, such as: being older, attending the initial grades of high school, living with a partner, being black (black or brown), having head of the family with low education and with lower family income.
What do these findings mean?
These findings indicate that the most vulnerable socioeconomic condition, obtained by the combination of the analyzed variables, is still a factor of damage to the health of adolescents in this phase of sexual initiation and transition to adulthood. In this sense, the approach to sex education by the family-school-health services triad, with an approach from the perspective of the adolescent, considering individuality and respecting them as individuals with rights, focused on the most vulnerable, can resolve attitudes towards sexuality more unfavorable conditions and promote health.
INTRODUCTION
Human sexuality has undergone transformations in the last decades, which have changed rigid norms of behavior, generating doubt and insecurity, especially in adolescents1.
The concept of sexuality is multidimensional and includes, in addition to biological and psychological formation, production in the cultural, social and historical context, in which the individual is inserted2,3. It integrates personality development, the learning process, as well as the adolescent's physical and mental health4 and is linked to personal values and desires, in addition to being a structuring and forming element of identity5.
In Brazil, adolescent sexual health continues to challenge health policies6, not only on issues related to biological aspects, but also psychosocial7. According to data from the last Brazilian census8, the adolescent population (10 to 19 years old) corresponds to 17.9% of the Brazilian population, a population that needs to have their sexual and reproductive rights assured.
In this sense, the Atitudes Face à Sexualidade em Adolescentes (Attitudes Towards Sexuality in Adolescents/AFSA) will also be built according to the experiences and different social contexts. These contexts can determine these attitudes as positive or negative, and they are not watertight, but can be modified1, becoming a way of measuring sexuality through the attitudes reported by individuals.
In adolescents, even if in a introverted way, sexual education has been exerting positive influences on AFSA, since they can promote the exchange of experience, dialogue, reflecting in greater autonomy in the exercise of sexuality and favoring the reduction of possible undesirable consequences arising from practices sexual9,10. Therefore, identifying the AFSA becomes a fundamental tool for the exercise of sex education and health promotion.
Since the beginning of the 20th century, sex education has been instituted in Brazil, but it was only in 1990 that it started to be supported in a citizenship perspective, seeking to promote autonomy, considering the sexual rights of adolescents, causing changes in a totally preventive approach11. These changes stem from the need to develop practices aligned with the adolescent's comprehensive health, with an emphasis on sexual and reproductive health12.
In this new approach to sex education, it is understood that adolescents have special needs related to sexual health, and that it can produce empowerment for the experience of sexuality, contributing to the consistent use of methods of protection and contraception13. Recent data show that diseases related to sexuality and teenage pregnancy are still a public health problem, with negative individual, biopsychosocial and socioeconomic consequences14,15.
This is due to the high prevalence of sexual initiation among adolescents without using a condom16. However, it must be emphasized that socioeconomic factors can be deterministic to modulate attitudes towards adolescents' sexuality in a pre-established social context of vulnerabilities. Thus, the objective is to analyze attitudes towards sexuality itself, according to socioeconomic factors in adolescents.
METHODS
Study Design
Observational cross-sectional study carried out through a school-based epidemiological survey, with the objective of measuring the exposure of adolescents to various risk behaviors, diseases and conditions that can affect the development of physical and mental health.
Study Location and Period
This research was carried out in public and private high schools in the Região Metropolitana da Grande Vitória (RMGV-ES), from August 2016 to May 2017.
Study Population and Eligibility Criteria
The sample size was calculated in order to ensure the representation of high school students, considering a population of 65,763 adolescents, enrolled in 168 schools in the Região Metropolitana da Grande Vitória - Espírito Santo (RMGV-ES), Brazil. The prevalence of 50% for the occurrence of Attitudes Towards Sexuality in Adolescents/(AFSA) of adolescents aged 15 to 19 was considered the highest expected proportion, the 95% confidence interval, standard error of 2.5% and 1.5 design effect safeguarding the accuracy of random sampling, resulting in a minimum sample size to be reached of 2,252 adolescents.
Municipal sample quotas were established, according to the percentage distribution of students enrolled in high schools by municipality of RMGV-ES, obtaining: (Cariacica = 19.3%; Fundão = 0.5%; Guarapari = 5.8 %; Serra = 23.2%; Viana = 3.7%; Vila Velha = 22.7%; Vitória = 24.8%). At the end of the research, 2,292 high school students from 54 schools participated, who did not have cognitive, hearing or visual disabilities, who studied in the morning and afternoon shift.
Data Collection
A structured form with closed questions was applied to students. The investigation process, with the participation of interviewers previously trained, was carried out by means of an electronic form, filled out individually by each adolescent in a portable computer.
To describe the socioeconomic profile of the adolescents, the following variables were used: age (15 to 19 years), biological sex (Male/Female), year of high school (1st to 4th year), municipality of residence (Vitória, Serra, Vila Velha, Cariacica, Fundão, Guarapari, Viana), marital status (Lives with a partner/Has a partner, but Does not live with him/does not have a partner), self-declared race/color (Black/Brown/White), paid work (Yes/No), head of the family (Father/Mother/Others), education level of the head of the family (illiterate/incomplete elementary I, complete elementary I/incomplete elementary II, complete elementary II/incomplete high school, complete high school/incomplete higher education, complete higher education), family income (≤ 1 minimum wage, 1 to 3 minimum wages, >3 minimum wages) and separated/divorced parents (Yes/No).
Also, the research instrument called "Scale of attitudes towards sexuality" was used, which consists of 26 items elaborated on an ordinal scale, Likert type, validated in Portuguese and intended to analyze the attitudes of adolescents towards sexuality1. This instrument was created and used in research with adolescents to establish sexual education practices at school. Each item has five answer alternatives and their quotation is processed in ascending order, that is, the first answer option in each item is quoted at 1 and the last at 5, with the following categories: (1) totally disagree, (2) strongly disagree; (3) neither agree nor disagree; (4) strongly agree; (5) totally agree. This scale also has items that are counted inversely. In this case, favorable behaviors on one side and unfavorable behaviors on the other were polarized1.
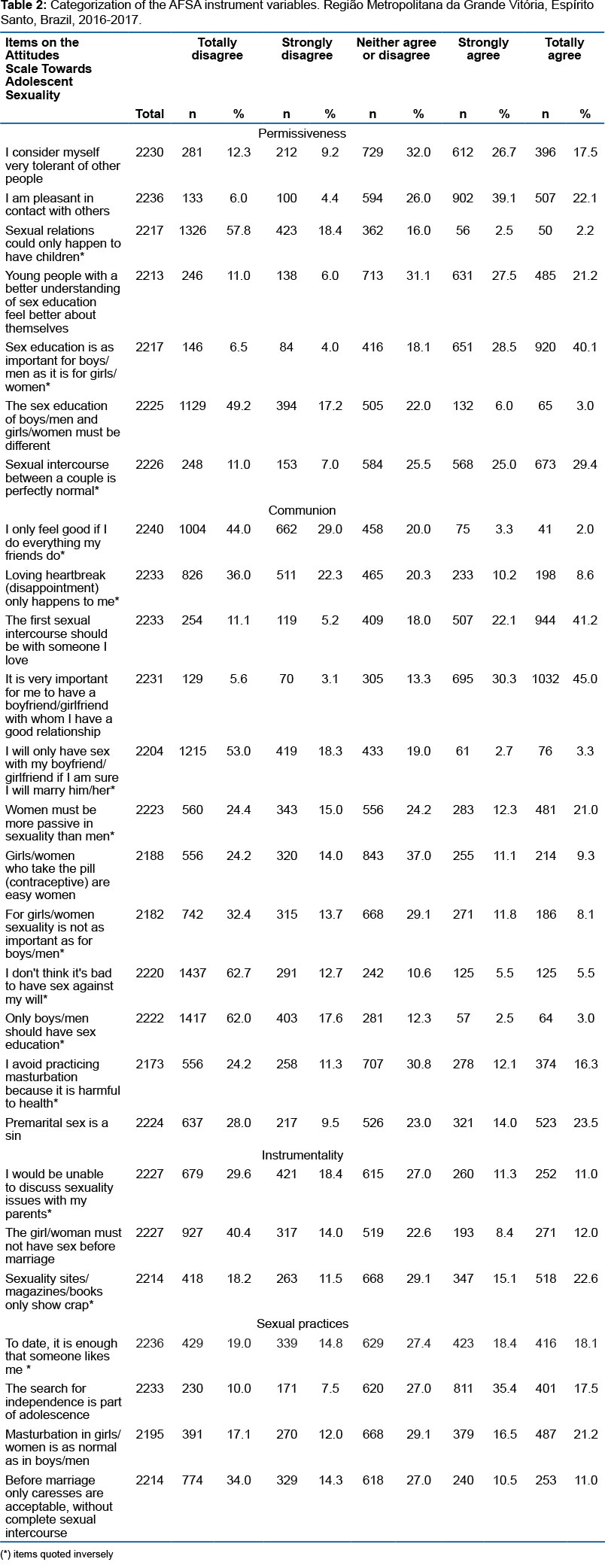
In addition, to present the descriptive results, Alferes's17 proposal was considered, which classifies the AFSA through four dimensions: Sexual permissiveness (attitudes towards the occasional sexual act, the sexual act without commitment and the diversity and simultaneity of partners), Sexual practices (attitudes towards family planning and sex education and acceptance of practices such as masturbation and unconventional sexual intercourse), Communion (attitudes towards sexual intercourse as intimate physical and psychological experience, involvement and sharing of feelings) and Instrumentality (attitudes towards the utilitarian sexual act, obtaining merely physical pleasure). To obtain the percentage of dimensions, the sum of the items for each category is considered (totally disagree, strongly disagree, neither agree nor disagree, strongly agree and totally agree).
Data Analysis
Initially, to test the AFSA instrument, a pilot study was carried out with 46 adolescent students from a public school in the city of Vitoria, Espírito Santo, Brazil. The mean of each answer and the global mean of respondents were calculated, as well as the standard deviation to determine the Attitude Index towards Sexuality in Adolescents. Then, the Kappa adjusted for frequency was applied to all questions of the AFSA instrument, being significant at the level of 5%. And the McNemar test was used to test the tendency of disagreement between the items on the AFSA scale, after reapplying the questionnaire.
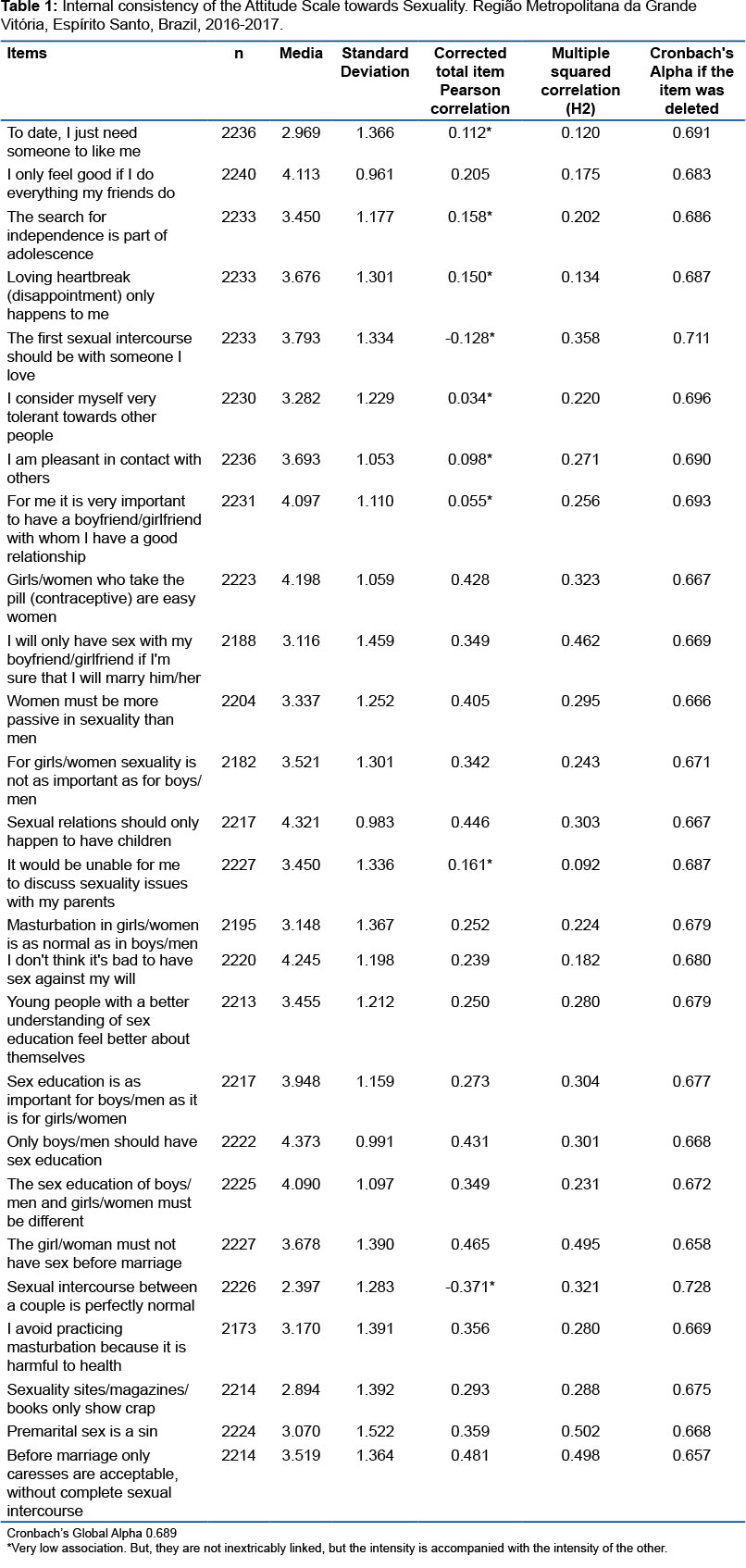
To finish testing the instrument, determining the degree of uniformity and consistency between the students' responses to each of the items that make up the instrument, Pearson's correlation coefficient was performed. And to check the reliability of the instrument, Cronbach's alpha coefficient was applied.
After testing the AFSA instrument, for analysis of the entire sample, the absolute and relative frequencies were calculated, as well as the mean and standard deviation. Then, Pearson's chi-square test was applied to test the association between the pattern of behavior: favorable, indifferent and unfavorable with socioeconomic characteristics. Associations with significance less than 20% were included in the multinomial logistic regression model, with the lowest p-value as an input order criterion. The selection of the adjusted model was performed manually, with only variables with p <0.005 remaining in the model, as the theoretical model allowed. In this study, the indifferent category was not considered for discussion purposes, as it does not bring a relevant theoretical reflection on the topic. In all analyzes, 95% confidence intervals and a significance level of 5% (α = 0.05) were used. The Statistical Package for the Social Sciences (SPSS) version 20.0 was used for statistical analysis.
Ethical and Legal Aspects of the Research
The present study complied with the rules of the Research Ethics Committee (CEP) of the Universidade Federal do Espírito Santo, and was authorized under opinion No. 971.389. The Secretaria Estadual de Educação (State Department of Education/SEDU) also authorized the execution of the research, letter No. 1,223, as well as the author of the instrument.
RESULTS
Initially, when conducting the pilot study to test the AFSA instrument, the score obtained allowed the adolescents to be classified into three groups: I - Global average minus 0.25 standard deviation, means an unfavorable AFSA; II - global average plus 0.25 standard deviation, means a favorable AFSA; III - adolescents with values between these limits were classified as indifferent AFSA. Thus, a global average was obtained: 3.577 and standard deviation: 0.501 with the following classification: Unfavorable AFSA ≤3.452; 3,452≤ Indifferent AFSA ≤3,702 and Favorable AFSA ≥3,702.
When performing the adjusted Kappa, the values ranged from 0.61 to 0.94, being significant at the level of 5%. For the McNemar test, significant disagreement was found only for the item "I would be unable to discuss sexuality issues with my parents" after the questionnaire was reapplied. To check the reliability of the instrument, Cronbach's alpha coefficient was applied, which was considered acceptable for all items and in the global value (r>0.600)18, as shown in Table 1.
The total sample involved 2,292 high school teenagers. The age of 16 years (29.8%) presented the highest frequency, followed by adolescents aged 15 years (25.7%) and 17 years (25.4%). The female sex corresponded to 60.0% of the sample. The year of high school in which most adolescents were enrolled was the first year (47.7%), followed by the second year (27.0%).
When analyzing the dimensions of the AFSA instrument, it is possible to observe that in the Permissiveness dimension, there is a tendency for adolescents to agree on the items that integrate it, representing a favorable attitude towards the occasional sexual act, without commitment and the diversity of sexual partners (42.9%), however, when analyzing the categories in isolation, 25% of the adolescents did not have a formed opinion. In the Communion dimension, there is total disagreement in relation to the items, reflecting an unfavorable attitude of adolescents towards the sexual act as an intimate physical and psychological experience of involvement and sharing of feelings (35.1%). The Instrumentality dimension showed total disagreement in relation to the items, reflecting non-utilitarian attitudes towards the sexual act, aiming at the mere obtaining of physical pleasure (30.3%). The Sexual Practices dimension, related to family planning, sex education and practices such as masturbation and unconventional sexual intercourse, tended to agree (38.4%), but the category neither agree nor disagree also presented a considerable percentage, 28.6 % (table 2).
When analyzing the proportional differences between the classification of the AFSA instrument, which classifies the adolescents' attitudes, and the socioeconomic variables, there was a statistically significant association of attitudes towards sexuality with age (p=0.001), year of high school (p<0.001), education of the head of the family (p<0.001), marital status (p<0.001), race/color (p<0.001), total family income (p <0.001) and municipality of residence (p=0.003), according to Table 3.
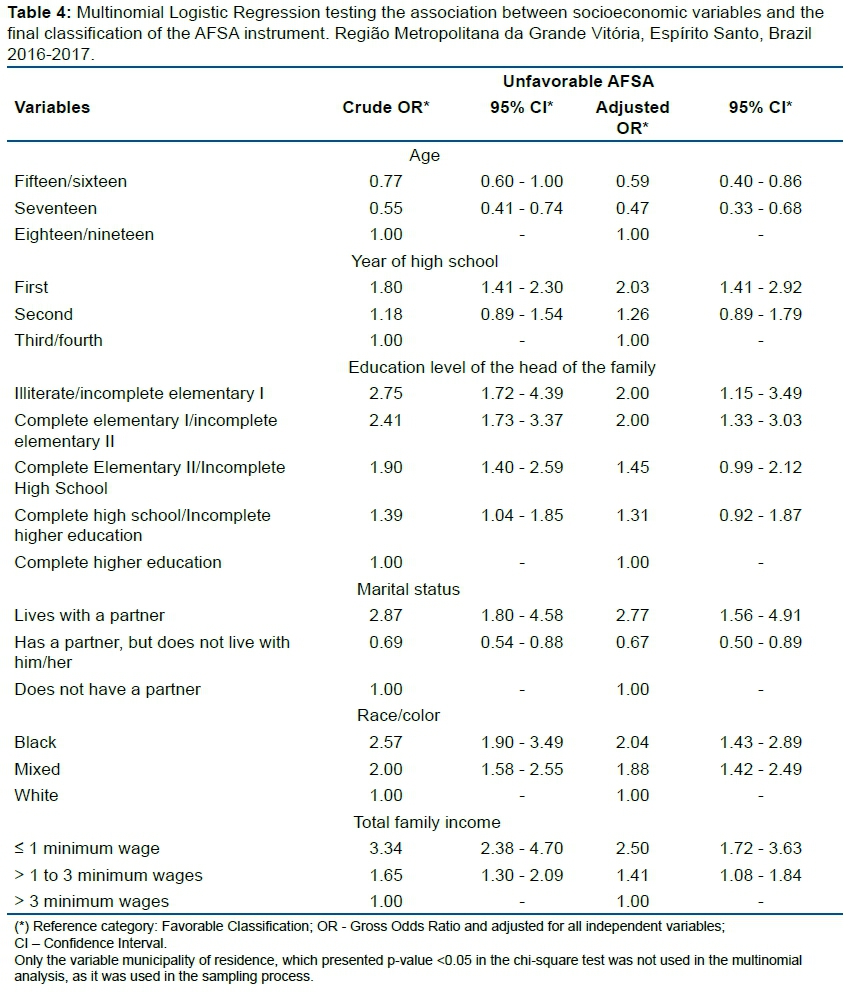
The age of fifteen/sixteen and seventeen years of the adolescents presented itself significantly as a protective factor for unfavorable AFSA (OR = 0.59; 95% CI: 0.40-0.86 and OR = 0.47; 95% CI: 0, 33-0.68) in relation to eighteen/nineteen year old students. However, adolescents attending the first year of high school had a greater chance (OR = 2.03; 95% CI: 1.41-2.92) of unfavorable AFSA compared to those attending the third/fourth year.
The adolescent student who has the head of the family with a very low level of education has a higher risk of having unfavorable sexual attitudes in relation to that the head of the family has a complete higher education (OR = 2.00). It is observed that the lower the level of education, the greater the risk of unfavorable AFSA.
The adolescent's marital status was an unfavorable risk factor for AFSA considering who lives with a partner (OR = 2.77; 95% CI: 1.56-4.91) compared to those who do not have a partner. However, those who have a partner and do not live with him (OR = 0.67; 95% CI: 0.50-0.89) presented an unfavorable protection factor for AFSA in relation to those who do not have a partner.
As for race/color, the adolescent student who defines himself as black has a higher risk (OR = 2.04; 95% CI: 1.43-2.89) compared to white. The same occurs with brown (OR = 1.88; 95% CI: 1.42-2.49) adolescents in relation to white, that is, blacks and browns are at greater risk of having an unfavorable attitude towards whites. Low family income was also another major factor for higher risk of unfavorable AFSA, thus, the lower the family income the greater the risk (OR = 2.50; 95% CI: 1.72-3.63).
DISCUSSION
Most adolescents had predominantly unfavorable AFSA and the socioeconomic factors that influenced to a greater or lesser extent the chance of unfavorable attitudes towards sexuality were: being 18 or 19, being in the first year of high school, belonging to a family where the head has a low level of education, live with a partner, be black/brown and live in a family whose income is low.
Adolescents were favorable to the diversity of partners and sexual relations without the affectivity component, which shows more liberal attitudes towards sexuality. This behavior may be related to changes that have occurred in society from the breaking of paradigms in relation to sexuality through dialogue and social support19. However, care should be taken with these changes, as the diversity of sexual partners increases the chances of exposure to Sexually Transmitted Infections (STIs)20,21.
There was also evidence of disagreement regarding utilitarian attitudes towards the sexual act, and agreement about unconventional sexual relations and masturbation, which can be considered as behaviors that involve controversies and contradictions1. On the other hand, there was agreement among the adolescents regarding family planning and sex education, which may also be related to the social construction of sexuality in adolescence through information acquired at school about reproductive health and sexual health22. In this sense, Carvalho et al.23 argue that the construction of sexuality is based on several social, economic, cultural, family and educational aspects, and that these influences can contribute to the construction of favorable or unfavorable attitudes towards sexuality.
Younger adolescents (fifteen to seventeen years old) had a lower chance of unfavorable attitudes in relation to eighteen/nineteen year old students, probably related to the change in the age profile of adolescents in relation to AFSA. According to the Pesquisa Nacional de Saúde do Escolar, the percentage of schoolchildren between 13 and 15 years of age who reported having started their lives sexually was 30.5% in 200924, to 27.0% in 201525, even with a drop, the percentage is still significant for the age of sexual initiation. Studies also show that adolescent puberty, early sexual initiation and immaturity are important risk factors for sexual and reproductive health26,27, which can be aggravated when associated with smoking, drunkenness and drug use28.
Although the risks contribute to the occurrence of unfavorable outcomes to the adolescent's health, there are protective factors that can contribute to these outcomes being reduced. Some studies show a very significant relationship between educational level and development of skills to avoid unfavorable AFSA and later, risky sexual behavior, suggesting that adolescents with a higher level of education can exercise better sexual behaviors23,29,30. This was corroborated in this study, since the students of the initial grades have a higher risk of unfavorable AFSA compared to the students of the final grades of high school, showing that education can cause changes in the behavior of individuals.
In studies with adolescents, not only intrinsic aspects should be considered, but also those related to the family context in which they are inserted. Fundamentally, parents can play an important role as their children's primary educators, directly influencing AFSA. However, the lack of knowledge, skills or discomfort when talking about sexuality, can prevent them from successfully fulfilling this role31. In this study, the education level of the head of the family was presented as an explanatory variable for unfavorable AFSA. Education at the lowest levels was shown to be an unfavorable risk factor for AFSA in relation to the head who had completed higher education. This fact is worrying, since sex education is partly dependent on the family's educational level32.
Considering that parents are still the greatest source of information at the time of first sexual intercourse, for both girls and boys, adolescent children of better educated parents will have better representation as for AFSA7. The protective influence of sex education is not limited to questions about when or whether sexual activity will start, but extends to questions of successful choices in relation to sexuality9, which may reflect in reducing socioeconomic disparities. Brazil is the fourth country in the world in absolute number of girls married before 18 years of age33, a condition that can contribute to school dropout, making it difficult to enter the labor market and, as a consequence, the perpetuation of poverty32,34. Thus, when analyzing the marital situation of adolescents, the experience with the partner, in this study, represented the greatest risk to unfavorable AFSA in relation to those who do not have a partner.
According to data from UNICEF (2005)35, living with a partner already in childhood and adolescence directly affects the adolescent's health and sexual and reproductive rights, in addition, it may be related to greater exposure to domestic violence or even coercion by the partner for the practice of unfavorable AFSA, due to the lack of perspective and family support. On the other hand, the fact of having a partner, but not living with him, in relationships (dating), presented itself as a protective factor for AFSA unfavorable in relation to those who do not have a partner, being able to demonstrate the experience of sexuality without daily living, showing more stable relationships decreasing the risks to sexual health with or without sexual activity36. It should be noted that, possibly, adolescents who do not have a partner did not initiate sexual activity, therefore, they have more favorable AFSA.
Among the most structural, economic vulnerability is directly associated with low education, varying to a greater or lesser degree of risk depending on the condition of each group34. However, other economic factors may also be related to unfavorable AFSA.
Social inequalities have increased in Brazil, affecting a large part of the Brazilian population, but mainly, the black population, which is the majority among the poorest37. In the present study, black and brown adolescents had a higher risk of unfavorable AFSA compared to whites, as well as a lower income had a higher risk for unfavorable AFSA compared to a higher family income. Another study29 also found that risky sexual behavior was also prevalent among black, low-income and low-education adolescents. Allied to this, the National Health Survey38, highlighted that blacks and browns, without access to education and with less economic conditions, have less access to health services. Evidence that these adolescents need more focused attention from health services, as they may not have access to care for their health and education needs39.
In this study, it is important to note that the sample consists of high school students, properly enrolled and residing in a metropolitan region that has a Municipal Human Development Index (MHDI) equal to 0.772 and MHDI Education equal to 0.69540. And even in this context, inequalities regarding AFSA were found in the sample of adolescents.
It is also necessary to realize that structural health determinants, such as the provision of continuing secondary education, are important aspects to be addressed to improve adolescents' sexual and reproductive results, especially in less favored regions41. Ideally starting with the family, but in conjunction with the school and health services41,42.
Sexual attitudes can be modeled through sex education programs conducted in schools, and these have contributed to developing favorable AFSA. However, they still need to be readjusted not only as a health policy, but also as an educational one9. For Jackson et al.43 government policies must be formulated for the transition period between childhood and adulthood and be inserted early, promoting a broader social change to reduce social influences on the development and behavior of adolescents and to reduce marginalization, social exclusion and vulnerability. This corroborates with this study that showed a greater chance of unfavorable attitudes in more vulnerable adolescents.
The present study brought relevant contributions on the association between Attitudes Towards Adolescents' Sexuality and socioeconomic and demographic factors, as it presents a considerable sample size, includes students from public and private schools and minimizes information bias when applying an electronic form preserving privacy of teenagers. However, it has limitations inherent to the representativeness of students, since there was low adherence by students to participate in the research and the cross-sectional method that does not have temporality, allowing only association and no causal relationship to be established, since the outcome and exposure were measured at the same time. In addition, there was a considerable amount of missing data for the variables family income and race/color (about 25%).
CONCLUSION
Adolescents in transition to adulthood, attending the initial grades of high school, living with a partner, blacks or browns, whose heads of the family have low education and families with low income had a greater chance of unfavorable AFSA, showing that unfavorable socioeconomic factors negatively influenced the reproductive and sexual attitudes of adolescents.
Sex education, when carried out by the school and the health system, is a measure that can minimize the effect of socioeconomic factors on unfavorable attitudes regarding the sexual and reproductive health of adolescents. However, the ideal is the joint work of the family-school-Unified Health System triad. The approach should occur from the perspective of the adolescent, considering individuality and respecting them as individuals with rights.
Acknowledgments:
To the Secretaria Estadual de Educação do Estado do Espírito Santo for the feasibility of data collection in high schools.
Author Contributions:
Juliani da Silva Araújo Alves: Data collection, Data analysis and interpretation, Scientific writing, Final manuscript review.
Silvana Granado Nogueira da Gama: Analysis and interpretation of data, Scientific Writing, Final revision of the manuscript.
Maria Carmen Moldes Viana: Conception and design of the Study, Analysis and interpretation of data, Final revision of the manuscript.
Katrini Guidolini Martinelli: Interpretation of data, Scientific Writing, Final revision of the manuscript.
Edson Theodoro dos Santos Neto: Conception and design of the Study, Coordination of data collection, Analysis and interpretation of data, Scientific Writing, Final revision of the manuscript.
Funding:
Fundação de Amparo à Pesquisa e Inovação do Espírito Santo (FAPES) for financing the project in the EDITAL FAPES N° 007/2014 - UNIVERSAL - PROJETO INTEGRADO DE PESQUISA.
Conflicts of Interest:
There are no conflicts of interest.
REFERENCES
1.Nelas, P.; Fernandes, C.; Ferreira, M.; Duarte, J. & Chaves, C. (2010). Construção e validação da escala de atitudes face à sexualidade em adolescentes (AFSA). In F. Teixeira et al. (Org.), Sexualidade e educação sexual: políticas educativas, investigação e práticas (pp. 180-184). Braga: Edições CIEd. E-book disponível em: <http://www.fpccsida.org.pt/images/stories/Livro_I_CISES.pdf> [ Links ].
2.Castro MG, Abramovay M, Silva LB da. Juventudes e sexualidade. Juventudes e sexualidade. 2004; 428-428. [ Links ]
3.Ohara CV da S, Jardim DP, Brêtas JR da S. O comportamento sexual de adolescentes em algumas escolas no município de embu, são paulo, brasil. Revista Gaúcha de Enfermagem. 2008; 29(4): 581. [ Links ]
4.Amaral MA, Fonseca RMGS da. Entre o desejo e o medo: as representações sociais dos adolescentes acerca da iniciação sexual. Revista da Escola de Enfermagem da USP. dezembro de 2006; 40(4): 469-76. [ Links ]
5.Moreira TMM, Viana D de S, Queiroz MVO, Jorge MSB. Conflitos vivenciados por adolescentes com a descoberta da gravidez. Revista da Escola de Enfermagem da USP. junho de 2008; 42(2): 312-20. [ Links ]
6.Malta DC, Silva MAI, Mello FCM de, Monteiro RA, Porto DL, Sardinha LMV, et al. Saúde sexual dos adolescentes segundo a Pesquisa Nacional de Saúde dos Escolares. Rev bras epidemiol. setembro de 2011; 14(suppl 1): 147-56. [ Links ]
7.Vonk ACRP, Bonan C, Silva KS da. Sexualidade, reprodução e saúde: experiências de adolescentes que vivem em município do interior de pequeno porte. Ciênc saúde coletiva. junho de 2013; 18(6): 1795-807. [ Links ]
8.| do IBGE Censo 2010 [Internet]. [citado 26 de fevereiro de 2021]. Disponível em: https://censo2010.ibge.gov.br/). [ Links ]
9.Alencar R de A, Silva L, Silva FA, Diniz RE da S. Desenvolvimento de uma proposta de educação sexual para adolescentes. Ciênc educ (Bauru). 2008; 14(1): 159-68. [ Links ]
10.Borges ALV, Trindade RFC. Gravidez na adolescência. In: Fujimori, E. Enfermagem e a saúde do adolescente na atenção básica. Barueri: Manole, 2009; p. 334-47. [ Links ]
11.Barreiro L, Teixeira-Filho FS, Vieira PM. Corpo, afeto e sexualidade: uma experiência da abordagem das sexualidades a partir das artes. Rev de Psicologia da UNESP. 2006; 5(1): 13-27. [ Links ]
12.L8069 [Internet]. [citado 26 de fevereiro de 2021]. Disponível em: http://www.planalto.gov.br/ccivil_03/Leis/L8069.htm. [ Links ]
13.Delatorre MZ, Dias ACG. Conhecimentos e práticas sobre métodos contraceptivos em estudantes universitários. Revista da SPAGESP. 2015; 16(1): 60-73. [ Links ]
14.Boletim epidemiológico de hiv/aids 2019 [Internet]. Departamento de Doenças de Condições Crônicas e Infecções Sexualmente Transmissíveis. [citado 26 de fevereiro de 2021]. Disponível em: http://www.aids.gov.br/pt-br/pub/2019/boletim-epidemiologico-de-hivaids-2019. [ Links ]
15.Souza M de L de, Lynn FA, Johnston L, Tavares ECT, Brüggemann OM, Botelho LJ. Taxas de fecundidade e desfechos perinatais da gravidez na adolescência: estudo retrospectivo de base populacional. Rev Latino-Am Enfermagem [Internet]. 2017 [citado 26 de fevereiro de 2021]; 25(0). Disponível em: http://www.scielo.br/scielo.php?script=sci_arttext&pid=S0104-11692017000100325&lng=en&tlng=en [ Links ]
16.Borges ALV, Fujimori E, Kuschnir MCC, Chofakian CB do N, Moraes AJP de, Azevedo GD, et al. ERICA: iniciação sexual e contracepção em adolescentes brasileiros. Rev Saúde Pública [Internet]. 2016 [citado 26 de fevereiro de 2021];50(suppl 1). Disponível em: http://www.scielo.br/scielo.php?script=sci_arttext&pid=S0034-89102016000200307&lng=en&tlng=en [ Links ]
17.Alferes VR. Escala de Atitudes Sexuais. In: Simões MR, Goncalves MM, Almeida LA. Testes e Provas Psicológicas em Portugal. 1997; 2: 131-38. [ Links ]
18.Corrar L.J. Paulo E. Dias Filho JM. Análise multivariada: para os cursos de administração, ciências contábeis e economia. São Paulo: Atlas. 2007; 542. [ Links ]
19.Ribeiro JM, Pontes A, Santos LR. Atitudes enfrentam a sexualidade nos adolescentes no programa de educação sexual. Psicologia, Saúde e Saúde Doenças, doenças. 2012; 13(2): 340-55. [ Links ]
20.Campos HM, Schall VT, Nogueira MJ. Saúde sexual e reprodutiva de adolescentes: interlocuções com a Pesquisa Nacional de Saúde do Escolar (Pense). Saúde em Debate. junho de 2013; 37(97): 336-46. [ Links ]
21.Silva A de SN, Silva BLCN, Silva Júnior AF da, Silva MCF da, Guerreiro JF, Sousa A do SC de A. Início da vida sexual em adolescentes escolares: um estudo transversal sobre comportamento sexual de risco em Abaetetuba, Estado do Pará, Brasil. Rev Pan-Amaz Saude. setembro de 2015; 6(3): 27-34. [ Links ]
22.Brasil, Ministério da Saúde. Secretaria de Atenção à Saúde. Departamento de Ações Programáticas Estratégicas. Diretrizes Nacionais para a Atenção Integral à Saúde de Adolescentes e Jovens na Promoção, Proteção e Recuperação da Saúde. 2010. Série A. Normas e Manuais Técnicos. 1ª edição, Brasília. p. 32-118. [ Links ]
23.Carvalho C, Pinheiro M, Gouveia JÁ, Duarte V. Questionário de Atitudes e Crenças sobre Sexualidade e Educação Sexual (QACSES) para adolescentes: estudos de validação psicométrica. Rev de Psicologia da Criança e do Adolescente. 2016; 7:1-2. http://revistas.lis.ulusiada.pt/index.php/rpca/article/view/2420 [ Links ]
24.PENSE, Pesquisa Nacional de Saúde do Escolar, IBGE, Ministério da Saúde, Ministério do Planejamento, desenvolvimento e gestão, Rio de janeiro. 2009: 37-40. [ Links ]
25.PENSE, Pesquisa Nacional de Saúde do Escolar, IBGE, Ministério da Saúde, Ministério do Planejamento, desenvolvimento e gestão, Rio de janeiro. 2015: 64-5. [ Links ]
26.Henao-Trujillo OM. Factores de riesgo y protectores en las prácticas y comportamientos sexuales de los estudiantes de pregrado presencial en una universidad de la ciudad de Manizales. Rev Univ. salud. 2014; 16(1): 82 - 92. http://www.scielo.org.co/scielo.php?script=sci_arttext&pid=S0124-71072014000100008&lng=en&nrm=iso&tlng=es [ Links ]
27.Beserra EP, Sousa LB, Cardoso VP, Alves MDS. Perception of adolescents about the life activity "express sexuality". Rev Fund Care Online. 2017; 9(2): 340-46. DOI: https://doi.org/10.9789/2175-5361.2017.v9i2.340-346 [ Links ]
28.Goncalves H, Machado EC, Soares ALG, Camargo-Figuera FA, Seerig LM, Mesenburg MA,et al. Início da vida sexual entre adolescentes (10 a 14 anos) e comportamentos em saúde. Rev Bras Epidemiol. 2015; 18(1): 1-18. DOI: https://doi.org/10.1590/1980-5497201500010003 [ Links ]
29.Coelho EAC, Andrade MLS, Vitoriano LVT, Souza JJ, Silva DO, Gusmão MEN, Nascimento ER, Almeida MS. Associação entre gravidez não planejada e o contexto socioeconômico de mulheres em área da Estratégia Saúde da Família. Acta Paul Enferm.2012; 25(3): 415-22. DOI: https://doi.org/10.1590/S0103-21002012000300015 [ Links ]
30.Ahorlu CK, Pfeiffer C, Obrist B. Socio-cultural and economic factors influencing adolescents' resilience against the threat of teenage pregnancy: a crosssectional survey in Accra, Ghana. Reproductive Health. 2015; 12: 117. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4690282/pdf/12978_2015_Article_113.pdf [ Links ]
31.Breuner CC, Mattson G. Sexuality Education for Children and Adolescents. Pediatrics. 2016; 138(2): 1348. DOI: https://doi.org/10.1542/peds.2016-1348 [ Links ]
32.Sousa MCR, Gomes KRO. Conhecimento objetivo e percebido sobre contraceptivos hormonais orais entre adolescentes com antecedentes gestacionais. Cad. Saúde Pública. 2009; 25(3): 645-54. DOI: https://doi.org/10.1590/S0102-311X2009000300019 [ Links ]
33.Taylor A, Lauro G, Segundo M, Greene M. Instituto PROMUNDO. Casamento na infância e adolescência no Brasil, resultados de pesquisa de método misto. Rio de Janeiro, editora sênior e consultora. set. 2015; 1-4. [ Links ]
34.Nery IS, Gomes KRO, Barros IC, Gomes IS, Fernandes ACN, Viana LMM. Fatores associados à reincidência de gravidez após gestação na adolescência no Piauí, Brasil. Epidemiol Serv Saúde. 2015; 24(4): 671-80. DOI: https://doi.org/10.5123/S1679-49742015000400009 [ Links ]
35.UNICEF. 2005. The United Nations Children's Fundation. Early Marriage a Harmful Traditional Practice. A Statistical Exploration Disponível em: https://www.unicef.org/publications/files/Early_Marriage_12.lo.pdf [ Links ]
36.Custódio G, Massuti AM, Schuelter-Trevisol F, Trevisol DJ. Comportamento Sexual e de Risco para DST e Gravidez em Adolescentes. J bras Doenças Sex Transm. 2009; 21(2): 60-64. http://www.dst.uff.br/revista21-2-2009/3%20-%20Comportamento%20sexual%20e%20de%20risco.pdf [ Links ]
37.IBGE. Instituto Brasileiro de Geografia e Estatística. Ministério do Planejamento, Desenvolvimento e Gestão. Síntese de Indicadores Sociais: Uma Análise das Condições de Vida da População Brasileira. Estudos e Pesquisas Informações Demográficas e Socioeconômicas. 2016; 36: 11-97. [ Links ]
38.IBGE. Instituto Brasileiro de Geografia e Estatística. Ministério do Planejamento, Desenvolvimento e Gestão. Pesquisa nacional de Saúde. 2013; 39-54. [ Links ]
39.Taquette SR, Monteiro DLM, Rodrigues NCP, Rozemberg R, Menezes DCS, Rodrigues AO, Ramos JAS. Saúde sexual e reprodutiva para a população adolescente, Rio de Janeiro, Brasil. Ciênc. Saúde Colet. 2017; 22(6): 1923-32. https://doi.org/10.1590/1413-81232017226.22642016 [ Links ]
40.IPEA. Instituto de Pesquisa Econômica e Aplicada. Atlas Do Desenvolvimento Humano Nas Regiões Metropolitanas Brasileiras. IDHM da Região Metropolitana da Grande Vitória. 2010; 109-14. [citado em 10/01/2018]. Disponível em: http://www.ipea.gov.br/agencia/images/stories/PDFs/livros/livros/141125_atlasvitoria [ Links ]
41.Mason-Jones AJ, Sinclair D, Mathews C, Kagee A, Hillman A, Lombard C. School-based interventions for preventing HIV, sexually transmitted infections, and pregnancy in adolescents. Cochrane Database of Systematic Reviews. 2016; 11. (CD006417): 1-90. [ Links ]
42.Grossman JM, Tracy AJ, Charmaraman L, Ceder I, Erkut S. Protective Effects of Middle School Comprehensive Sex Education With Family Involvement. Journal of School Health. 2014; 84(11): 739-47. DOI: https://doi.org/10.1111/josh.12199 [ Links ]
43.Jackson CA, Henderson M, Frank JW, Haw SJ. An overview of prevention of multiple risk behavior in adolescence and young adulthood. Journal of Public Health. 2012; 34(No.S1).i31-i40. DOI: https://doi.org/10.1093/pubmed/fdr113 [ Links ]
 Correspondence:
Correspondence:
edsontheodoro@uol.com.br
Manuscript received: October 2020
Manuscript accepted: December 2020
Version of record online: March 2021


{kind=link}
{kind=link}
{kind=link}
{kind=link}