










Serviços Personalizados
Journal

artigo
 Inglês (pdf)
Inglês (pdf)
 Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
 Curriculum ScienTI
Curriculum ScienTIIndicadores
Compartilhar

 Permalink
PermalinkPsicologia: teoria e prática
versão impressa ISSN 1516-3687
Psicol. teor. prat. vol.20 no.3 São Paulo set./dez. 2018
https://doi.org/10.5935/1980-6906/psicologia.v20n3p86-99
ARTIGOS
PSYCHOLOGICAL EVALUATION
Screening for ASD signs in very low birth weight preterm infants
Rastreo de señales sugestivas de TEA en prematuros con muy bajo peso al nacer
Vivian Renne Gerber LedermanI; Ana Lucia GoulartII; Amélia Miyashiro Nunes dos SantosII; José Salomão SchwartzmanI
IMackenzie Presbyterian University – UPM, SP, Brazil
IIFederal University of São Paulo – EPM/Unifesp, SP, Brazil
ABSTRACT
Prematurity has been associated with Autism Spectrum Disorders (ASD), and the early diagnosis is relevant for this population. This study compares the frequency of positive screening for ASD signs using M-CHAT at 18-24 months (n = 60) and ABC questionnaires at 30-36 months (n = 58) of corrected age in toddlers born prematurely with birth weight < I500g and investigates ASD diagnosis in suspected cases. Toddlers screened positive were evaluated with a DSM-5 diagnostic protocol. 6.7% of toddlers screened positive for M-CHAT and 5.2% for ABC. ASD diagnosis was confirmed for 3.3% of children. An agreement between M-CHAT and ABC questionnaires was low (k = 0.241, p = 0.063). The frequency of suggestive signs of ASD detected by the M-CHAT and the ABC at different moments was similar, and the diagnosis rate of ASD was high. The screening at I8-24 month added to the screening at 30-36 months increased the frequency of positive screening for signs of ASD in preterm.
Keywords: autism; Autism Spectrum Disorders; premature infant; very low birth weight preterm infant; preterm.
RESUMEN
Prematuridad es asociada al Transtorno del Espectro del Autismo (TEA). Diagnóstico precoz es relevante para esta población. Este estudio comparó la frequen-cia de rastreo positivo para senales de TEA utilizando los questionários M-CHAT a los 18-24 meses (n = 60) y ABC a los 30-36 meses (n = 58) de edad corregida em prematuros nacidos com peso < 1.500 g, y averiguo diagnóstico de TEA em los casos sospe-chosos, con protocolo diagnóstico siguiendo DSM-5. 6,7% de los prematuros fueron positivos para M-CHAT y 5,2% para ABC. Diagnóstico de TEA fue confirmado en 3,3% de los prematuros. Hubo baja concordância entre M-CHAT y ABC (k = 0,241, p = 0,063). La frequencia de senales de TEA detectada por los dos instrumentos en diferentes momentos fue similar, y la tasa de diagnóstico de TEA fue alta. El rastreo a los 18-24 meses, sumado al rastreo a los 30-36 meses aumenta la frequência de rastreo positivo para senales de TEA en prematuros.
Palabras clave: autismo; Transtorno del Espectro del Autismo; prematuro; prematuro de muy bajo peso; precocidad.
Introduction
Autism Spectrum Disorder (ASD) is characterized by an atypical development in social interaction and communication and by the presence of a markedly restricted behavioral repertoire of activities and interests (American Psychiatric Association, 2013). It is a disorder that emerges in a genetically vulnerable individual, exposed to external sources of stress, during critical moments of development (Casanova, 2007). The risk groups for ASD include premature infants, low-birth-weight preterm (below 2,500g), and premature infants of very low birth weight (below 1,500 g). To date, screening rates for signs suggestive of ASD found in preterm infants vary between 3.7% and 12.5%, compared to 1-1.5% in full-term infants (Kuzniewicz et al., 2014; Gray, Edwards, O'Callaghan, & Gibbsons, 2015, Guy et al., 2015). The increased risk of ASD in preterm infants can be explained by increased maternal morbidity, birth characteristics and neonatal complications (Kuzniewicz et al., 2014).
Premature infants often present difficulties in social and emotional communication and joint attention, which are consistent with signs suggestive of ASD (Johnson et al., 2010; De Schuymer et al., 2011). In this population, the presence of a high number of developmental delays makes specific screening particularly important (Johnson et al., 2010).
Although developmental delays may or do not necessarily confirm the diagnosis of ASD in a later stage, the identification of these signs through screening instruments favors early intervention and improvement in the condition and early referral for diagnosis (Hofheimer, Scheinkpf, & Eyler, 2014).
Among the instruments available to screen for ASD signs, the Modified Checklist for Autism in Toddlers - M-CHAT (Robins, Fein, Barton, & Green, 2001) and the Autism Behavior Checklist - ABC questionnaires (Krug, Arick, & Almond, 1980) stand out. Although these questionnaires do not have diagnostic value, they permit the selection of suspect cases for future evaluations. In addition to guidance in screening for signs of ASD at 18 and 24 months of age, Ozonoff et al. (2012) recommend an additional screening after two years of age, which allows for the observation of signs that would not be present previously. The diagnosis of ASD, in turn, should include clinical examination with anamnesis, direct observation, neuropsychological and multidisciplinary evaluations, and complementary tests (Velloso et al., 2011).
Considering that preterm infants are a risk group for ASD and whose developmental delays may or may not constitute the diagnosis subsequently, we believe it is important to evaluate screening instruments in this population. In this context, the objective of this study was to compare the frequency of positive screening for ASD signs, using the M-CHAT questionnaires at 18-24 months and the ABC at 30-36 months corrected age in children born prematurely with very low weight, and subsequent diagnostic evaluation of ASD according to the DSM-5 (American Psychiatric Association, 2013) in suspected cases.
Method
Participants
It is a prospective study conducted with a convenience sample of preterm infants of very low birth weight. The inclusion criteria were: premature infants between 18 and 24 months of corrected age, of both sexes, born before 37 weeks of gestational age and weighing less than 1500 g, followed at the Outpatient Clinic of the Federal University of São Paulo, Brazil. In this outpatient clinic, children born before 37 weeks of gestation with very low birth weight are regularly followed from the neonatal unit to adolescence by a multiprofessional team, consisting of pediatricians, neuropediatricians, physiotherapists, speech therapists, occupational therapists, ophthalmologists, nutritionists, psychologists, dermatologists, dentists, and social workers. Exclusion criteria were: the presence of motor deficiencies, severe visual and auditory impairment, and/or genetic syndrome, according to the diagnosis recorded in the children's histories by the multiprofessional team that accompanied the children after their discharge from the neonatal unit. The preterm infants eligible for the study were selected from a clinical database of the children attending said outpatient clinic, according to the inclusion and exclusion criteria established for this study.
Instruments
Two instruments were used to screen for signs of ASD: the M-CHAT (Robins, Fein, Barton, & Green, 2001) and the ABC (Krug, Arick, & Almond, 1980), both translated into Portuguese (Losapio & Pondé, 2008; Marteleto & Pedromônico, 2005). The M-CHAT was used to screen for ASD signs between 18 and 24 months of corrected age, and the ABC between 30 and 36 months of corrected age.
The M-CHAT (Robins, Fein, Barton, & Green, 2001) is a questionnaire to track the signs of ASD in children between 16 and 30 months, with a sensitivity of 0.85 and a specificity of 0.93. It consists of 23 questions to be answered by the parents or guardians of the child. Each M-CHAT question, if scored, is worth 1 point. Questions 2, 7, 9, 13, 14, and 15 are considered critical for signs of ASD and evaluate social aspects and joint attention, such as pointing at objects, imitation, and social interest. The other questions also evaluate sensory stimuli, relationship, and motor aspects. Children who fail three or more questions, or two critical questions, present positive screening for ASD signs (Losapio & Pondé, 2008).
The ABC (Krug, Arick, & Almond, 1980) consists of a list of atypical behaviors. It was designed for screening as from 18 months of age with suspected ASD and should be answered by the child's parents or guardians. Its sensitivity is 0.38-0.56 and specificity 0.76-0.97. It consists of 57 questions related to five areas: sensory stimulus (SS), relating (RE), body and object use (BO), language (LG), and social and self-help skills (SSH). Each question has a variable score between 1 and 4, being 1 point for behaviors less related to autism (such as getting dressed alone) and 4 for those more related to the condition (such as turning around oneself). In the original study, the authors proposed that a final score equal to or greater than 68 would classify for autism; scores between 54 and 67 would be considered a moderate possibility of autism; scores between 47 and 53 would be inconclusive; and for scores inferior to 47 points, the child would not be considered autistic (Krug, Arick, & Almond, 1980). For Brazil, however, Marteleto & Pedromônico (2005) suggested that the appropriate score to characterize the individual within the autism spectrum, using the Portuguese translation, was 49 points, which increases the sensitivity of the instrument, maintaining its specificity. Therefore, the present study adopted this score.
Procedure
This study was conducted after the approval # 497,957 (12/13/2013) from the Mackenzie Presbyterian University and the Federal University of São Paulo's # 604,039-0 (01/22/2013) Ethics Committees and after all parents or guardians had signed the consent form.
Initially, the M-CHAT questionnaire was applied to the guardians of the preterm infants included in the study, with corrected age between 18 and 24 months, during the routine visit to the outpatient clinic. The children who screened positively at this stage were referred to the psychology or speech therapy service. One year after the first evaluation, the participants were submitted to the second evaluation with the ABC questionnaire. After the second evaluation, at 36 months of corrected age, preterm infants who screened positively on either instrument, the M-CHAT and/or the ABC, were referred to the TEA-MACK Laboratory at Mackenzie Presbyterian University for diagnostic evaluation. The diagnosis of ASD, according to the DSM-5 criteria (American Psychiatric Association, 2013), was based on a multidisciplinary evaluation, following the evaluation protocol of the TEA-MACK Laboratory, which includes patient history, neuropsychological, language and communication assessments, as well as assessments of social, physical and neurological cognition, and visual screening (Velloso et al., 2011).
Socioeconomic data, clinical characteristics of the preterm infants included in this study, as well as clinical evolution during the hospitalization period in the neonatal intensive care unit were collected from the charts.
Statistical analysis
Statistical analysis was performed using SPSS for Win/v.17.0 program (SPSS Statistics, Somers, NY), considering a significant difference, p < 0.05. Numerical variables were expressed as means and standard deviations or medians and were compared by means of Student's t-test (normal distribution) or the Mann-Whitney test (non-normal distribution). Categorical variables were expressed in absolute and percentage frequencies and were compared by the Chi-square test (χ2) or Fisher's Exact Test.
To verify the level of agreement between the results of the M-CHAT and the ABC, the Kappa Concordance Coefficient was calculated.
Results
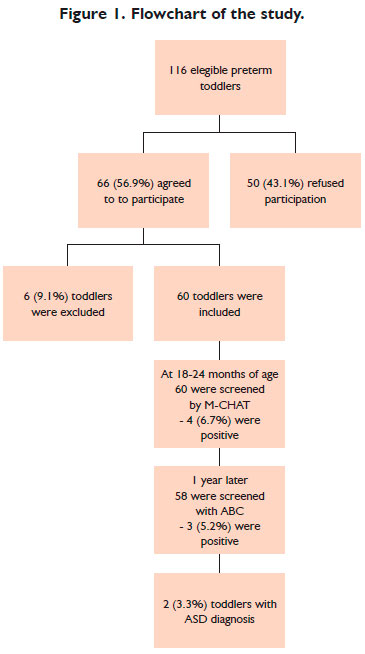
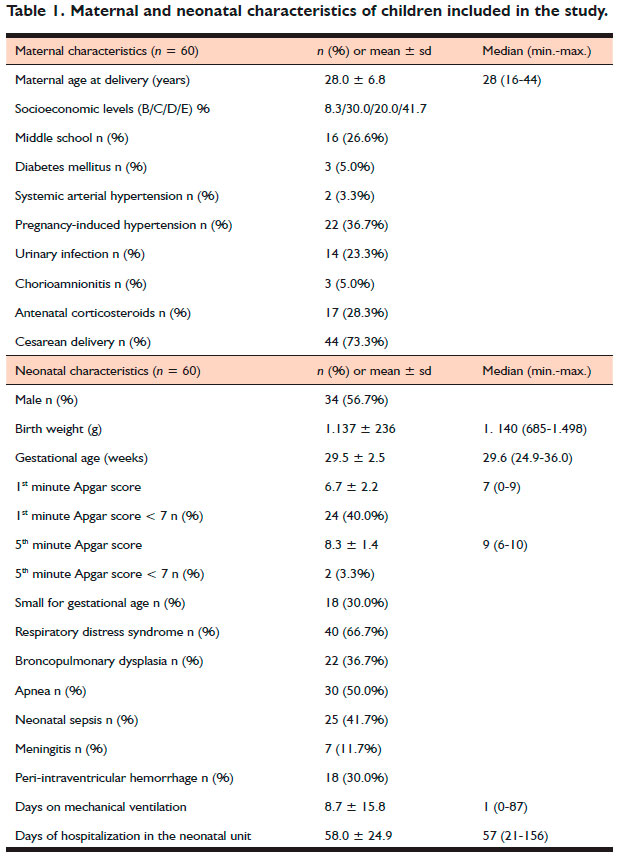
Of the 116 preterm infants eligible for the study, 66 caregivers (56.9%) agreed to participate. Of these, six children (9.1%) were excluded, one due to the genetic syndrome and five due to cerebral palsy. Thus, 60 infants born prematurely with very low birth weight were included in the study (Figure 1). Maternal and neonatal characteristics are shown in Table 1:
The first evaluation of the 60 premature infants was performed at 18 to 24 months of corrected age, with a mean age of 20 ± 2.0 months. Fifty-three mothers (88.3%), four parents (6.7%), two grandparents (3.4%), and one responsible caregiver of sheltered children (1.7%) completed the M-CHAT questionnaires. One year later, the ABC questionnaires were completed by a similar profile: 50 mothers (86.3%), five fathers (8.6%), one grandmother (1.7%), one uncle (1.7%), and one caregiver (1.7%). All parents or guardians confirmed contact and daily care for the child.
In the M-CHAT, four preterm infants screened positively (6.7%; 95% CI: 2.6-15.9%). All children presented impairments in joint attention, such as not pointing at objects or interest in other children, or bringing objects to parents, and only one scored for auditory sensitivity (Figure 1).
Preterm infants who scored positively and negatively on the M-CHAT presented similar gestational age (28.5 ± 1.5 versus 29.0 ± 3.1 weeks, p = 0.646) and similar mean birth weight (1163 ± 405 versus 1135 ± 226 grams, p = 0.898), respectively, as well as similar clinical evolution during hospitalization in neonatal care.
Regarding the distribution of the M-CHAT scores across the sample, 32% of the children did not score any questions and 68% scored at least one question. Questions related to auditory sensitivity had high scores: question 11 related to noise sensitivity was scored by 51% of premature infants and question 20, related to hearing loss, by 23%. Fewer than 10% of preterm infants scored on any other question.
The second screening with the ABC questionnaire was applied to 58 premature infants and took place between 30 and 36 months, with the corrected mean age of 33.6 ± 1.8 months. The ABC questionnaire was applied to 58 preterm infants between 30 and 36 months of corrected age. In this evaluation, three (5.2%; 95% CI: 1.8% -14.1%) children presented positive signs of ASD, with two new suspected cases and one previously screened with the M-CHAT (Figure 1). The three preterm infants presented high scores in the five ABC categories, with important impairments in all of them: sensory stimulus, relating, body and object use, language and social, and selfhelp skills. There were no significant differences in neonatal characteristics or gestational age (29.0 ± 3.0 vs. 28.9 ± 3.0 weeks, p = 0.968) or birth weight (1367 ± 210 vs. 1126 ± 237g, p = 0.091) among those who were screened positive or negatively. There was a significant difference in the presence of urinary tract infection during gestation, present in 100% of mothers of preterm infants who were screened positively and only 18.2% of the mothers of premature infants screened negatively (p = 0.009).
Mothers of preterm infants who screened positively and negatively on the M-CHAT presented similar education level (median 11.0 versus 11.0 years, p = 0.921), as well as family income (median U$ 375.00 versus 300.00, p = 0.970). The same was observed in relation to the mothers of premature infants who scored positively and negatively with the ABC: 11 versus 11 years of education (p = 0.939) and average family income U$ 300.00 versus U$ 345.00 (p = 0.259).
The median ABC score for preterm infants was similar for those who scored positively or negatively on the M-CHAT (28.5 versus 13.0, p = 0.097), respectively (Figure 2).
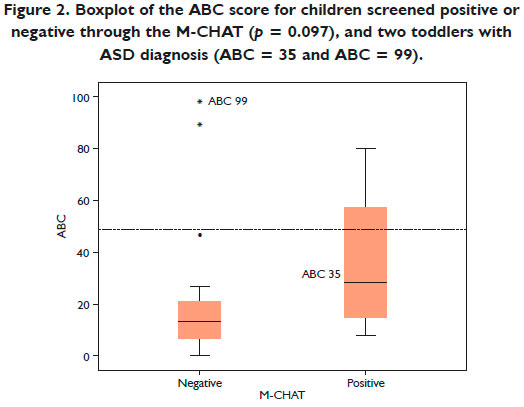
Of the four preterm infants (two girls and two boys) who had scored positively on the M-CHAT, only one boy scored positively on the ABC (positive on both instruments). An increase in symptoms was noticed: not only losses in joint attention, already detected with the M-CHAT, but also impairments in language, sensory stimuli, and social self-help skills (79 points on the ABC).
In the ABC questionnaire, three boys were screened positively: in addition to the above, another two new suspect cases that had not been screened with the M-CHAT (90 and 99 points on the ABC respectively). There was a low agreement between the M-CHAT and the ABC questionnaires (Fisher's Exact Test, p = 0.196, kappa concordance coefficient = 0.241, p = 0.063).
After 36 months of age, the six preterm infants who were screened positively in any of the instruments, the M-CHAT or the ABC, were referred to the TEA-MACK Laboratory for diagnostic evaluation. Two boys (3.3%) were diagnosed as having ASD according to the DSM-5 (American Psychiatric Association, 2013), one of them was screened positively with both instruments and the other only in the second screening using the ABC questionnaire. Both had persistent deficits in communication and social interaction, in addition to restricted and repetitive behavioral patterns and interests. These losses were in agreement with the signs appointed during the ABC screening. One of the preterm infants had a gestational age of 27.3 weeks and a birth weight of 970 grams, and the other was born at 32.1 weeks' gestation and weighed 1475 grams.
Discussion
In this study, the percentage of preterm infants screened positively for signs of ASD with M-CHAT at 18-24 months of corrected age, and with ABC a year later, corresponded to 6.7% (four premature infants) and 5.2% (three preterm infants), respectively. Of the six preterm infants screened positively with either instrument, two boys had a diagnosis of ASD confirmed at 36 months of age, representing 3.3% of the sample. The concordance between the M-CHAT and the ABC, each applied at different ages, was low as demonstrated with the Kappa coefficient. The impairment in joint attention, observed in all infants screened positively, is a suggestive sign of relevant
ASD, and its presence reinforces the need for screening and early diagnosis of this population. Our results emphasize the American Academy of Pediatrics (AAP) recommendation to screen for signs compatible with ASD at 18-24 months of age, and also suggest the follow-up of children at risk during childhood, such as preterm infants, as they may show signs of ASD after this age group (Ozonoff et al., 2012).
No perinatal clinical characteristics were found that could identify positivity on the M-CHAT or the ABC, as similar gestational ages, birth weight and clinical evolution were observed in premature infants who scored positively and negatively on both questionnaires. The only exception was related to the rate of maternal urinary infection during pregnancy. Despite the reduced sample, these results agree with the study by Hadjkacem et al. (2016) who, when comparing ASD children and their unaffected siblings, reported urinary tract infection during pregnancy as a possible risk factor for ASD.
Our results are in line with recent studies indicating that preterm infants and very low birth weight infants are at increased risk of screening for ASD signs (Gray, Edwards, O'Callaghan, & Gibbsons, 2015). Some environmental factors may modulate a genetic predisposition for ASD, such as maternal chorioamnionitis and hemorrhage, use of mechanical ventilation and infections in the neonatal period. Kuzniewicz et al. (2014) showed that ASD was three times more prevalent in children born before 27 weeks of gestation, compared to those born at term, and also found an increase in ASD signs as the gestational age decreases, in the presence of environmental risk factors. In our study, the two boys diagnosed with ASD were born with very low birth weight and with gestational age inferior to 33 weeks.
There was a low agreement between positive M-CHAT and ABC screenings, with only one (25%) of the four infants screened positive on the M-CHAT also screening positively on the ABC. The other two preterm infants screened positive on ABC had not been screened on M-CHAT. Screening for ASD at 18-24 months is recommended by AAP and helps increase the possibility of early intervention and diagnosis, but a second follow-up would help include children who do not yet demonstrate developmental delays at the first screening stage. It is possible that risk groups, such as preterm infants or groups with longer developmental delays, if evaluated only once at 18-24 months, may lead to increased false-positive results, while a two-stage screening may be more effective to identify children with ASD (Gray, Edwards, O'Callaghan, & Gibbsons, 2015; Hardy, Haisley, Manning, & Fein, 2015). M-CHAT-R/F (Robins et al., 2014) has been used as a substitute for M-CHAT because it is an instrument with better sensitivity and specificity and, therefore, has greater screening power. In addition to reducing the number of questions, the M-CHAT-R/F assumes a follow-up interview for those cases that scored more than questions, which favors the distinction between ASD suspects. In the case of premature infants, the subsequent interview could favor the reduction of false-positives, as exceeded delays due to prematurity can be taken as signs of ASD in a first evaluation without follow-up interview. That tool could not be used in this study though because it was not available locally.
In our study, the frequency of positive screening with the M-CHAT and the ABC was similar; different children were detected though. This result highlights not only the different moments at which signs of ASD develop but also the possible loss of these signs by some premature infants. Typical child development is variable, and some children present developmental delays that are naturally overcome in the subsequent months (Hofheimer, Scheinkpf, & Eyler, 2014). Interventions help minimize or even correct these delays. In our study, children screened positively on the M-CHAT were referred for intervention. Of the four preterm infants who presented signs suggestive of ASD at 18-24 months of age, two girls did not present them at 30-36 months. At the end of the evaluations, however, two boys were diagnosed with ASD, which is according to the literature, with ASD being more prevalent in boys than in girls, at a ratio of 1:4 (Zwaigenbaum, Bryson, & Garon, 2013). The interventions, during the interval between the two screenings, could have contributed to the fact that some of the children with signs suggestive of ASD in the first evaluation did not score in the second assessment. The delays initially screened may have been overcome in some cases due to the intervention, which could represent a limitation of the study.
After the age of 24 months, some signs suggestive of ASD become more apparent and, either due to Regressive Autism or to the fact that other developmental milestones are already reached, and these signs stand out. This can be observed during our study when two preterm infants screened positively for ASD between 30 and 36 months of age, but did not show signs compatible with ASD and were not screened positively when the M-CHAT was applied at 18 months of age. In relation to Regressive Autism, it is discussed if the signs were present in a very subtle way from the beginning and, therefore, difficult to perceive, or if they actually appeared after 24 months of age. Screening at 18-24 months favors early diagnosis for ASD though, which can be determined up to 18 months earlier than in children who are not screened (Daniels & Mandell, 2013).
Although the diagnosis of ASD is more frequent in premature infants, behaviors suggestive of ASD, such as communication difficulties, social reciprocity, sensory hypersensitivity and repetitive movements may eventually have a different meaning in premature infants and should be analyzed within the framework of complications of prematurity (Hofheimer, Scheinkpf, & Eyler, 2014). The diagnosis of ASD can be an extreme and severe part of a more global profile of functional, cognitive, and attention impairment of prematurity (Johnson et al., 2010). Whether these signs suggestive of ASD are corroborated or not by a subsequent diagnosis of ASD, the premature infant may gain from appropriate interventions (Zanon et al., 2017). Thus, early screening for signs of ASD may be clinically relevant not only for the diagnosis of ASD but also to identify a group of children who may subsequently present developmental difficulties or sequelae (Johnson et al., 2010, Guy et al., 2015).
The limitations of the study include the small convenience sample used and the lack of a control group, which prevents definitive conclusions. Term infants were not included in this study, being performed at a referral outpatient clinic for premature infants. Another limitation is the lack of diagnostic tools such as the Autism Diagnostic Interview-Revised (ADI) or the Autism Diagnostic Observation Schedule (ADOS), not available at the time of the study. The use of multidisciplinary evaluation for diagnosis following the DSM-5 sought to remedy this aspect. Another limitation in this study was the impossibility of a complete evaluation of the entire sample at 36 months of age, even for those who were not screened with signs suggestive of ASD.
We concluded that the frequency of signs suggestive of ASD among premature infants born with very low birth weight, evaluated with the M-CHAT at 18-24 months and with the ABC at 30-36 months of age was similar, and the confirmation of the ASD diagnosis after 36 months, according to the DSM-5 criteria, was high. Screening at 18-24 months of age plus a screening at 30-36 months increases the frequency of positive screening for signs of ASD in preterm infants.
References
American Psychiatric Association - APA (2013). Diagnostic of mental disorders (5th ed.). Arlington: American Psychiatric Association. [ Links ]
Casanova, M. F. (2007). The neuropathology of autism. Brain Pathology, 77(4),422-433. doi:10.1111/j.1750-3639.2007.00100.x [ Links ]
Daniels, A. M., & Mandell, D. S. (2013). Children's compliance with American Academy of Pediatrics' well-child care visit guidelines and the early detection of autism. Journal of Autism Developmental Disorders, 43(12),2844-2854. doi:10.1007/s10 803-013-1831-x [ Links ]
De Schuymer, L., De Groote, I., Striano, T., Stahl, D., & Roeyers, H. (2011). Gaze aversion during social interaction in preterm infants: a functiooon of attention skills? Infant Behaviour and Development, 35(1),129-139. doi:10.1016/j.infbeh.2010.12.007 [ Links ]
Gray, P. H., Edwards, D. M., O'Callaghan, M. J., & Gibbsons, K. (2015). Screening for autism spectrum disorders in very preterm infants during early childhood. Early Human. Development, 97,271-276. doi:10.1016/j.earlhumdev.2015.02.007 [ Links ]
Guy, A., Seaton, S. E., Boyle, E. M., Draper, E. S., Field, D. J., Manktelow, B. N. N., Smith, L. K., & Johnson, S. (2015). Infants born late/moderately preterm are at increased risk for a positive autism screen at 2 years of age. The Journal of Pediatrics, 766(2),269-275. doi:10.1016/j.jpeds.2014.10.053 [ Links ]
Hadjkacem, I., Ayadi, H., Turki, M., Yaich, S., Khemekhem, K., Walha, A., Cherif, L., Moalla, Y., Ghribi, F. (2016). Prenatal, perinatal and postnatal factors associated with autism spectrum disorder. The Journal of Pediatrics, 92(6),595-601. doi:10.1016/j.jped.2016.01.012 [ Links ]
Hardy, S., Haisley, L., Manning, C., & Fein, D. (2015). Can screening with the ages and stages questionnaire detect autism? Journal of Developmental Behavior Pediatrics, 36(7),536-543. doi:10.1097/DBP.0000000000000201 [ Links ]
Hofheimer, J., Scheinkpf, S. J., & Eyler, L. T. (2014). Autism risk in very preterm infants: new answers, more questions. The Journal of Pediatrics, 164(91),6-8. [ Links ]
Johnson, S., Hollis, C., Kochhar, P., Hennessy, E., Wake, D., & Marlow, N. (2010). Autism spectrum disorders in extremely preterm children. The Journal of Pediatrics, 156(94),525-531. [ Links ]
Krug, D. A., Arick, J. R., & Almond, P. (1980). Behavior checklist for identifying severely handicapped individuals with high levels of autistic behavior. Journal of Child Psychology and Psychiatry, 121(3),221-229. [ Links ]
Kuzniewicz, M. W., Wi, S., Qian, Y., Walsh, E. M., Armstrong, M. A., & Croen, L. A. (2014). Prevalence and neonatal factors associated with autism spectrum disorders in preterm infants. The Journal of Pediatrics, 164(1),20-25. doi:10.1016/j.jpeds.2013.09.021 [ Links ]
Losapio, M. F., & Pondé, M. P. (2008). Tradução para o português da escala M-CHAT para rastreamento precoce de autismo. Revista Brasileira de Psiquiatria, 33(3),221-229. [ Links ]
Marteleto, M. R. F., & Pedromônico, M. R. M. (2005). Validity of Autism Behavior Checklist (ABC): preliminary study. Revista Brasileira de Psiquiatria, 27(4),295-301. [ Links ]
Ozonoff, S., Iosif, A. M., Baguio, F., Cook, I. C., Hill, M. M., Hutman, T., ... Young, G. S. (2010). A prospective study of the emergence of early behavioral signs of autism. Journal of the American Academy of Children & Adolescent Psychiatry, 49(3),256-266. doi:10.1542/peds.2010-2825 [ Links ]
Robins, D., Casagrande, K., Barton, M., Chen, C. M. A., Dumont-Mathieu, T., & Fein, D. (2014). Validation of the Modified Checklist for Autism in Toddlers Revised With Follow-up (M-CHAT-R/F). Pediatrics, 133(1),37-46. doi:10.1542/peds.2013-1813 [ Links ]
Robins, D. L., Fein, D., Barton, M. L., & Green, J. A. (2001). The Modified Checklist for Autism in Toddlers: an initial study investigating the early detection of autism and pervasive developmental disorders. Journal of Autism Developmental Disorders, 31(2),131-144. doi:10.1023/A:1010738829569 [ Links ]
Velloso, R. L., Vinic, A. A., Duarte, C. P., D'Antino, M. H. F., Brunoni, D., & Schwartzman, J. S. (2011). Protocolo de avaliação diagnostica multidisciplinar da equipe de transtornos globais do desenvolvimento vinculado à pós-graduação em distúrbios do desenvolvimento da Universidade Presbiteriana Mackenzie. Cadernos de Pós-graduação em Distúrbios do Desenvolvimento, 11,9-11. [ Links ]
Zanon, R. B., Backes, B., & Bosa, C. A. (2017). Diagnóstico do autismo: relação entre fatores contextuais, familiares e da criança. Psicologia: Teoria e Prática, 19(3),33-42. doi:10.5935/1980-6906 [ Links ]
Zwaigenbaum, L., Bryson, S., & Garon, N. (2013). Early identification of autism spectrum disorders. Behavioural Brain Research, 251,133-146. doi:10.1016/j.bbr. 2013.04.004. [ Links ]
 Mailling address:
Mailling address:
Vivian R.G. Lederman
Alameda Franca 660/15
São Paulo, SP, Brasil. CEP 01422-000
E-mail: vlederman26@gmail.com
Submission: 22.4.18
Acceptance: 27.7.18
Author's note: We would like to thank all the families of the Outpatient Clinic of the Federal University of São Paulo/EPM who agreed to participate in this study.


{kind=link}