










Serviços Personalizados
Journal

artigo
 Inglês (pdf)
Inglês (pdf)
 Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
Indicadores
Compartilhar

 Permalink
PermalinkJournal of Human Growth and Development
versão impressa ISSN 0104-1282versão On-line ISSN 2175-3598
J. Hum. Growth Dev. vol.31 no.2 Santo André maio/ago. 2021
https://doi.org/10.36311/jhgd.v31.11341
ORIGINAL ARTICLE
Olfactory sensory evaluation in newborn children of women infected with COVID-19 during pregnancy
Kassandra Silva Falcão CostaI; Laiane Medeiros RibeiroII; José Alfredo Lacerda de JesusI; Karina Nascimento CostaI; Geraldo Magela FernandesI; Jan SpilskiIII, IV; Thomas LachmannIII, IV; Rosana Maria TristãoI
IFaculty of Medicine and University Hospital, Campus Darcy Ribeiro, University of Brasília, Brasília, DF 70910-900, Brazil;
IIFaculty of Health and University Hospital, Campus Darcy Ribeiro, University of Brasília, Brasília, DF 70910-900, Brazil;
IIICenter for Cognitive Science, University of Kaiserslautern, 67663 Kaiserslautern, Germany;
IVFacultad de Lenguas y Educación, Universidad Nebrija, 28015 Madrid, Spain
ABSTRACT
INTRODUCTION: In adults, olfactory loss is one of the earliest and most frequent acute clinical manifestations of SARS-CoV-2 infection. The number of children infected with SARS-CoV-2 is relatively small, perhaps due to the lower expression of Angiotensin Converting Enzyme 2 (ACE2) in children compared to adults. Little is known about foetal impairment in mothers infected with SARS-CoV-2. This paper describes an ongoing scientific project on smell perception in infants
OBJECTIVE: The goal of the study is to develop and validate a behavioural evaluative scale of olfactory perception in healthy newborns and to apply this scale to newborn children of women infected with COVID-19 during pregnancy comparing to newborn children of women without COVID-19 infection history, in order to compare these groups
METHODS: This is a retrospective comparative analytical cohort study of 300 newborns exposed and unexposed to COVID-19 during pregnancy. The data collection will follow the experimental procedure in a previous study that explored odours of the maternal breastmilk, vanilla (sweet) and distilled water (neutral). A coffee smell was implemented as an addition to this previous study in order to include acid/bitterness category to the categories of stimuli
DISCUSSION: It is feasible to argue the hypothesis of the involvement of the foetus' olfactory bulb as one of the indelible pathophysiological manifestations to the clinical diagnosis of COVID-19 with neurosensory olfactory deficit in foetuses and newborns affected by intrauterine infection. This study aims to investigate if newborn children of women infected with COVID-19 during pregnancy have olfactory sensory changes. The clinical trial was registered in the Brazilian Registry of Clinical Trials (ReBEC- RBR-65qxs2
Keywords: newborn, perception, odors, COVID-19, SARS-CoV-2
Authors summary
Why was this study done?
Olfactory loss in adults is one of the initial and most frequent acute clinical manifestations of SARS-CoV-2 infection. The few studies that have evaluated this alteration in the paediatric range have shown that children have less olfactory sensory loss than adults. One possible explanation would be the lesser expression of ACE2 in the nasal mucosa compared to adults with consequently less binding of SARS-CoV2. The authors propose to evaluate the action of SARS-CoV-2 at the intrauterine level regarding the foetus' olfactory sensory impairment.
What did the researchers do and find?
This study aims to assess the olfactory sensory perception of newborns of women who previously tested positive for COVID-19 during pregnancy compared to newborns of women who did not test positive for COVID-19 during pregnancy. It also aims to develop and validate a behavioural evaluation scale of olfactory sensory-perceptual perception in newborns. This work is based on the scientific literature on the sensory-perceptual development of smell in foetuses and newborns. Newborns will be exposed to four odours: breast milk, vanilla (sweet), coffee (bitter) and distilled water (neutral). The exposure order will be the same in all experiments.
What do these findings mean?
There is a lack of data in the literature regarding foetal impairment by SARS-CoV-2. Younger children have a lower incidence of COVID-19 symptoms compared to adults including low frequency of sensory impairment, especially smell. The results of this study will clarify whether intrauterine SARS-CoV-2 can affect the foetal sensory system or not.
INTRODUCTION
The natural history of COVID-19, caused by the SARThe natural history of COVID-19, caused by the SARS-CoV-2 virus, is still being explored. Little is known about its effects on pregnancy, the puerperium and the health of the mother and foetus, as well as the impact on the long-term development of the children of infected mothers during pregnancy. Based on the positive data to date, the clinical picture of COVID-19 during pregnancy does not seem to differ when observed outside this period. The disease can be asymptomatic or present with clinical manifestations that vary in severity and symptomology, with the most common symptoms being fever (67%) and cough (66%), accompanied less frequently by malaise, dyspnoea, and diarrhoea1.
Vertical transmission of SARS-CoV-2 was previously thoroughly assessed in six pregnant women affected by the disease in the third trimester2. This study tested the amniotic fluid, umbilical cord blood, breast milk and nasopharyngeal swab of newborns, which were all negative for the virus. Subsequently, two systematic review and two studies describing cases of pregnancy infection in hospitals of Wuhan, China and New York City, United States, found no evidence of vertical transmission1,3-5. Inconclusive reports of vertical transmission include that of newborns with specific anti-SARS-CoV-2 IgM, but with negative RT-PCR5, as well as that of a 16h newborn with positive RT-PCR with 16h of life, but specific IgG and IgM remained negative until the 5th day6. The interpretation of these results requires prospective studies, which are known for the accuracy of molecular tests and the kinetics of anti-SARS-CoV-2.
Maternal SARS-CoV-2 infection does not expose the foetus and newborn only to the effects caused directly by the virus, but also to a variety of indirect effects. The consequences of the maternal and foetal inflammatory response, with the production of potentially cytotoxic cytokines, as well as the effect of the use of antiviral medications, have not been studied to date. Another important aspect concerns the risk of contamination of the newborn during or shortly after birth. Practices such as delayed cord clamping and skin-to-skin contact between mothers and newborns are not universally recommended and evidence on the risk of contagion during breastfeeding is still limited7,8.
There are studies reporting infected adults who developed neurological diseases, such as mental confusion, stroke, seizure, or loss of smell, due to a direct or indirect effect on the central nervous system (CNS). Likewise, a picture of acute haemorrhagic encephalopathy diagnosed through magnetic resonance imaging was reported in a woman in the sixth decade of life affected by COVID-199. The prevalence of neurological impairment by the disease is still being observed, but a study of 214 patients in Japan showed that 36% had some clinical finding related to the nervous system10. Though, not enough data is provided about the risk of fetuses or newborn infants being vulnerable to neurological sequels due to the COVID-19 infection.
Problem
Among the symptoms provided by carriers of the new coronavirus, is an olfactory sensory alteration. Olfactory loss in adults is one of the earliest and most frequent acute clinical manifestations of SARS-CoV-2 infection. It is feasible to hypothesize the involvement of the foetus' olfactory bulb during intrauterine life as one of the indelible pathophysiological manifestations to the clinical diagnosis of COVID-19 with neurosensory olfactory deficit in foetuses and newborns affected by intrauterine infection. Based on these evidences, the following research question was raised: do newborn children of women infected with SARS-CoV-2 during pregnancy have olfactory sensory changes? Hence, this work is based on the scientific literature on the sensory-perceptual development of smell in foetuses and newborn babies11-18 and aims to replicate methodological procedures of studies such as Bartocci et al.12, adapting this to the hospital context and expanding it as categories of olfactory stimulus for the implementation of a measure of discrimination sensitivity.
The main goal of the study is to assess the olfactory sensory perception of newborn children of women infected with SARS-CoV-2 during pregnancy. The specific objectives are to develop a behavioural evaluation scale of olfactory perception in infants; to validate this scale in healthy newborns; and to compare the responses with that of newborn children of women infected with COVID-19 during pregnancy.
METHODS
Study Design
The present study is a retrospective comparative analytical cohort research of 300 newborns as part of a major project aiming to follow-up the development of children born from mothers that tested positively for COVID-19 during pregnancy entitled "Clinical outcomes of children of mothers exposed to SARS-CoV-2 infection during pregnancy".
Sample size calculation
No precise figure is available about the prevalence of SARS-CoV-2 infection among pregnant women in Brazil, but international reports estimate up to 15.3% of all pregnancies being exposed1-4. Recent data accounts for a birth rate of 44,195 newborns per year in the Federal District area, where Brasilia the capitol of Brazil, is located. Thus, considering an "infinite" population (>20.000 pregnant women), and assuming a 15% prevalence of SARS-CoV-2 exposed pregnancies, a confidence level of 95% and margin of error of 5%, the minimum size for a random sample of exposed women would be 195, yielding an expected similar figure for the exposed children. Taking into consideration an expected drop-out rate of up to 20% in the BORN sub-study, the required number of exposed mothers (to give birth to the BORN participants) would raise to 234.
Nevertheless, our sampling approach is based on convenience, not random chance, as eligible subjects present to the recruitment centres. The aforementioned calculations served primarily as a reference, so as not to overestimate the inclusion of participants. Given the limited available knowledge regarding the effects of SARS-CoV-2 on pregnancy and child development, thus conferring upon the study an eminently exploratory character, we adopted an approach of "as much as feasible, but no more than reasonable" for the sample size definition.
Everything considered, we set an a priori number of 300 exposed women in the PREGNANT phase, which would result in expected 300 exposed children in the BORN phase. We adopted a 1:1 allocation rate between exposed and controls, thus implying another 300 mothers and 300 children who did not test positive for COVID-19 to constitute the non-exposed control group. Hence, the overall sample size of the PROUDEST study was finally set at 1200 participants (600 mother-child dyads: 300 exposed, 300 control).
Study Location and Period
This study would take place at the outpatient clinic for newborns born to pregnant women with COVID -19 (and Regular Growth and Development Outpatient clinic with newborns born to pregnant women without Covid-19). This outpatient clinic was developed at the University Hospital of Brasília (HUB) aiming at accompanying these newborns up to five years of age. It is composed of a multidisciplinary team, such as paediatric doctors, nurses, occupational therapists, speech therapists and neuropsychologists. This study will investigate infants born between July 2020 and March 2021.
Study Population and Eligibility Criteria
The target group will be composed of newborns up to 14 days old, whose mothers tested positive on a test that detects genetic material of the virus using a laboratory technique called polymerase chain reaction (PCR) for SARS-CoV-2 during pregnancy. The control group will be composed of newborns up to 14 days old, whose mothers did not test positive for SARS-CoV-2 during pregnancy. The inclusion criteria for exposed mother-baby dyads are a maternal age of ≥18 years and laboratory evidence of SARS-CoV-2 infection during pregnancy through RT-PCR or serology (searching for IgG and IgM antibodies) markers. The results of the rapid test accompanied by information about the clinical symptoms or characteristic tomography were collected as supplementary data. For the control group of unexposed mother-baby dyads, the inclusion criteria are a maternal age of ≥18 years and serology for SARS-CoV-2 (IgG and IgM antibodies) at admission for delivery assistance. Exposed newborns will be included evidence of maternal SARS-CoV-2 infection during pregnancy.
Exclusion criteria for exposed women and unexposed women are: pre-existing chronic diseases requiring continuous use of medications, except diabetes and hypertension; smoking and / or alcohol consumption; suspected or confirmed other congenital infections such as toxoplasmosis, syphilis, rubella, herpes, Chagas and ZIKA; and impossibility of sequential follow-up until delivery. Exposed and unexposed newborns will be excluded if there are indications or confirmation of genetic disorder; suspected or confirmed other congenital infections, such as toxoplasmosis, syphilis, rubella, herpes Chagas and ZIKA; and impossibility of sequential follow-up until the age of five.
Data Collection
The maternal epidemiological data will be obtained at the first meeting with the pregnant woman or her legal representative and are those contained in the "Epidemiological data spreadsheet". Clinical data will be obtained during prenatal care, which will occur in consultations with the following maximum interval: monthly between 0 and 34 weeks, twice a week between 34 and 36 weeks and weekly between 36 weeks and delivery. The data referring to childbirth and puerperium assistance will be obtained during hospitalization in the maternity hospital from medical reports. The monitoring of child growth and development will follow the intervals determined by the Ministry of Health of Brazil and will take place in an outpatient clinic specifically created for this purpose, composed of a multidisciplinary team of paediatrics, psychologists, occupational therapists, speech therapists, physiotherapists and nurses. The assessment of child neurodevelopment up to 42 months of life will include cognitive, motor, socioemotional aspects, and aspects related to language and adaptive behaviour and will be carried out with the validated version of the Bayley III Child Development Scale19. As of two and a half years of age, aspects related to intellectual performance will also be assessed through the Wechsler Pre-School and Primary Intelligence Scale20, with a half-yearly interval. The metabolic evaluation will be carried out by measuring blood glucose, insulin, lipid profile (total cholesterol and fractions, triglycerides), thyroid function (TSH, free T4) and basal cortisol at the end of the 12th and 24th months of life. Blood, CSF and placenta samples will be stored following the current rules for handling biological materials until their analysis.
Data Collection Procedure
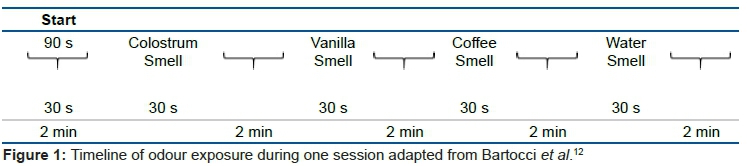
The data collection will follow an experimental procedure from Bartocci et al.12 that explores odours of the maternal breastmilk, vanilla (sweet), coffee (acid/bitter) and distilled water (neutral). The coffee smell is an addition to the previous study in order to include the acid/bitterness category to the categories of stimuli. Each test epoch consists of 30 s of baseline definition followed by 30 s of smell exposure with a two-minute interval for washout effect (figure 1).
The research assistants will wear surgical gloves for each handling of the solutions, and they will be prepared in an auxiliary room to avoid the spread of the smell of the solutions in the environment. Each solution will be kept in a hermetically sealed flask before and during all session to avoid smell impregnation. The room temperature will be maintained between 19-21ºC. The baby will be accommodated and cuddled on the lap of a familiar caregiver to prevent social stress and in a calm, relatively quiet (between 40 and 50dB(A)) environment reserved inside the Hospital Paediatric Follow-Up facility. The behavioral state21 during the session will be monitored and registered for each stage of smell exposure ranging from state 1 (deep sleep) to sate 6 (crying). In case of the baby achieving state level six (cry - intense cry or high motor activity) or in need of a diaper change, the session will be paused and resumed as soon the baby returns to the state five or less. Mothers will be instructed to not use moisturizers or perfumes and to bring the babies already breastfed at least 15 min before the session.
Session phases
Step I
Collection of socio-demographic and clinical information through specific instruments and consultation of the electronic medical record.
Step II
1. Select the sample according to the inclusion criteria - participant invitation.
2. Explain to the mother how the research will be carried out and collect the consent form from the person responsible for the newborn.
3. Ask if the mother had followed the requirement to not use moisturizers or perfumes.
4. Ask the mother to remove 1 ml of breast milk and put it on a hermetic flask.
5. Turn on the video recorder.
6. Follow the following steps with the baby sitting on the companion's lap (not the mother):
A. Basal Phase: start filming the baby's face for at least 30 seconds before the first odour presentation and keep filming the entire session.
B. Stimulus Phase I: present the cotton swab soaked in breast milk for 30 seconds 2 cm from the baby's nose, maintaining the filming throughout this period, discard the cotton swab.
C. Wash out phase I: continue filming the baby for 2 minutes while the research assistant discards the cotton swab dipped in breast milk.
D. Stimulus Phase II: present the cotton swab soaked in vanilla solution for 30 seconds 2 cm from the baby's nose, maintaining the filming throughout this period, discard the cotton swab.
E. Wash out phase II: continue filming the baby for 2 minutes.
F. Stimulus Phase III: present the cotton swab soaked in coffee solution for 30 seconds 2 cm from the baby's nose, maintaining the filming throughout this period, discard the cotton swab.
G. Washout phase I: continue filming the baby for 2 minutes.
H. Control Phase: present the cotton swab soaked in water for 30 seconds 2 cm from the baby's nose, maintaining the filming throughout this period, discard the cotton swab.
J. Washout phase II: continue filming the baby for 2 minutes.
Step III - Image coding
1. Phase I coding: will be carried out for the development of the olfactory sensory evaluation scale. The videos will be analyzed frame by frame to survey categories of behavioural responses to the four different olfactory stimuli. The rating levels will consider two response categories "yes" or "no", for present and absent reaction to the smell. Factor Analysis will be performed with analyses of the main components for the construction of the instrument and analysis of the sample data.
2. Phase II coding: will be carried out for comparative evaluation of newborn children of pregnant women with and without a diagnosis for Covid-19.
Data Analysis
A mixed design will be run, with treatment (colostrum, vanilla, coffee, water) as within-subject variable and COVID-19 (covid vs. noncovid babies) as between-subject variable (group variable). The dependent variable will be the dichotomous responses. Continuous variables will be described as mean and standard deviation or median and interquartile range (IQR), as appropriate. Categorical variables will be described as frequencies and percentages. The analyses will be run to determine the perception thresholds, sensitivity parameters, and ROC curves (Receiver Operating Characteristic). In addition to fixed effects models, random effects models are estimated and also adjusted for possible confounders. Statistical significance will be considered when the p value is less than .05. The data will be stored in a SPSS-21 file, with an alphanumeric code that prevents the identification of the patient; curve fitting will be done with the MATLAB curve-fitting tool. To control for possible selection bias, propensity score matching (PSM) will be performed, followed by re-analyses as part of the robustness analyses.
Ethical and Legal Aspects of the Research
The study was approved by the Research Ethics Committee from the University of Brasilia School of Medicine (http://www.fm.unb.br/cep-fm-CAAE 32359620.0.0000.5558) and was registered in the Brazilian Registry of Clinical Trials (ReBec) under number RBR-65qxs2. The complete protocol can be accessed at ReBec "Effects of COVID-19 on pregnancy, childbirth, puerperium, neonatal period and child development" [cited 2020 Sep 17]. Available from: http://ensaiosclinicos.gov.br/rg/RBR-65qxs2/).
DISCUSSION
Pregnant women can be infected with SARS-CoV-2, with a possible consequent infection of their foetuses and newborns. SARS-COV-2 infection can cause an immune overreaction that is manifested by the excessive activation of immune cells and the production of a large amount of interferon and cytokines that can affect foetal development and increase the risk of neurological diseases in the neonatal period5.
Like SARS-CoV, SARS-CoV-2 uses angiotensin converting enzyme 2 (ACE2) as a functional receptor to infect human cells. Studies have shown that ACE2 is expressed mainly in the respiratory, cardiovascular and digestive systems, which makes these organs more susceptible to this new virus. ACE2 is less mature in the youngest children and thus may not function as an appropriate receptor for SARS-CoV-2. The number of children infected with SARS-CoV-2 is relatively small. Thus, one hypothesis for this low infection rate is the low expression of ACE2 in children. Bunyavanich22 conducted a retrospective study that examined the nasal epithelium of 305 individuals aged 4 to 60 years and observed that the gene expression of ACE2 in the nasal epithelium was age dependent. ACE2 gene expression was lower in younger children and increased with age.
A neurological symptom that has been frequently described in patients who tested positive for COVID-19 is a temporary impairment of taste and smell, which has been reported in 49-70% of infected people23. Somekh et al.24 evaluated sensory function in patients (children and adults) who had COVID-19 documented by laboratory tests. Of the 73 patients, 37 (51%) reported having had a change in taste or smell, 25.8% of which were children. Children aged 5 to 10 years did not report sensory impairment23. However, there are still no reports about infants, especially newborn infants on the risk of being infected during pregnancy or delivery time.
One of the proposed mechanisms for altering smell and taste related to COVID-19 is the ability of SARS-CoV-2 to bind to ACE2 in the nasal and oral mucosa. Among people who tested positive for COVID-19, olfactory sensory sensation was significantly less impaired in children than in adults (p = .00014). The significant difference in olfactory sensory impairment between children and adults, and particularly between younger children and middle-aged adults, is in line with the finding that the expression of ACE2 in the nasal epithelium and in the oral cavity is more intense among adults, corroborating the possibility that the distribution and expression of ACE2 in the oral cavity and nasal epithelium may contribute to differences in sensory impairment22. Little is known about foetal impairment in mothers infected with SARS-CoV-2. By evaluating the olfactory sensory perception of newborns of women infected with COVID-19 during pregnancy, we can quantify such involvement.
Author Contributions
RMT, GMF KSFC and LRM devised the original study protocol, which was amended by TL, JS, JALJ and KNC. RMT, KNC, KSFC wrote the first draft of the manuscript that was then critically reviewed and revised by the other co-authors. All authors approved the final version of the manuscript for submission. RMT is the guarantor, and affirms that the manuscript is an honest, accurate and transparent account of the study being reported; and that any discrepancies from the study as planned have been explained.
Conflicts of Interest
The authors have no conflict of interest to declare.
Acknowledgements
The authors are grateful for the support of Liangqi Yang, Master student of the Cognitive Science Program, Technische Universität Kaiserslautern, Germany, for the Chinese translated version.
REFERENCES
1.Yang H, Sun G, Tang F, Peng M, Gao Y, Peng J, et al. Clinical features and outcomes of pregnant women suspected of coronavirus disease 2019. J Infect. 2020; 81(1); e40-4. DOI: 10.1016/j.jinf.2020.04.003 [ Links ]
2.Hen H, Guo J, Wang C, Luo F, Yu X, Zhang W, et al. Clinical characteristics and intrauterine vertical transmission potential of COVID-19 infection in nine pregnant women: a retrospective review of medical records. The Lancet. 2020; 395(10226): 809-15. DOI: 10.1016/S0140-6736(20)30360-3 [ Links ]
3.Breslin N, Baptiste C, Gyamfi-Bannerman C, Miller R, Martinez R, Bernstein K, et al. Coronavirus disease 2019 infection among asymptomatic and symptomatic pregnant women: two weeks of confirmed presentations to an affiliated pair of New York City hospitals. Am J Obstet Gynecol MFM. 2020; 2(2): 00118. DOI: 10.1016/j.ajogmf.2020.100118 [ Links ]
4.Zaigham M, Andersson O. Maternal and perinatal outcomes with COVID-19: A systematic review of 108 pregnancies. Acta Obstet Gynecol Scand. 2020; 99(7): 823-9. DOI: 10.1111/aogs.13867 [ Links ]
5.Dong L, Tian J, He S, Zhu C, Wang J, Liu C, et al. Possible Vertical Transmission of SARS-CoV-2 From an Infected Mother to Her Newborn. JAMA. 2020; DOI: 10.1001/jama.2020.4621 [ Links ]
6.Alzamora MC, Paredes T, Caceres D, Webb CM, Valdez LM, La Rosa M. Severe COVID-19 during Pregnancy and Possible Vertical Transmission. Am J Perinatol. 2020; 37(8): 861-5. DOI: 10.1055/s-0040-1710050 [ Links ]
7.Ashokka B, Loh M-H, Tan CH, Su LL, Young BE, Lye DC, et al. Care of the pregnant woman with coronavirus disease 2019 in labor and delivery: anesthesia, emergency cesarean delivery, differential diagnosis in the acutely ill parturient, care of the newborn, and protection of the healthcare personnel. American Journal of Obstetrics & Gynecology. 2020; 223(1): 66-74.e3. DOI: 10.1016/j.ajog.2020.04.005 [ Links ]
8.Yu N, Li W, Kang Q, Xiong Z, Wang S, Lin X, et al. Clinical features and obstetric and neonatal outcomes of pregnant patients with COVID-19 in Wuhan, China: a retrospective, single-centre, descriptive study. The Lancet Infectious Diseases. 2020; 20(5): 559-64. DOI: 10.1016/S1473-3099(20)30176-6 [ Links ]
9.Moriguchi T, Harii N, Goto J, Harada D, Sugawara H, Takamino J, et al. A first case of meningitis/encephalitis associated with SARS-Coronavirus-2. Int J Infect Dis. 2020; 94: 55-8. DOI: 10.1016/j.ijid.2020.03.062 [ Links ]
10.Poyiadji N, Shahin G, Noujaim D, Stone M, Patel S, Griffith B. COVID-19-associated acute hemorrhagic necrotizing encephalopathy: imaging features. Radiology. 2020; 296(2): E119-20. DOI: 10.1148/radiol.2020201187 [ Links ]
11.André V, Henry S, Lemasson A, Hausberger M, Durier V. The human newborn's umwelt: Unexplored pathways and perspectives. Psychon Bull Rev. 2018; 25(1): 350-69. DOI: 10.3758/s13423-017-1293-9 [ Links ]
12.Bartocci M, Winberg J, Ruggiero C, Bergqvist LL, Serra G, Lagercrantz H. Activation of olfactory cortex in newborn infants after odor stimulation: a functional near-infrared spectroscopy study. Pediatr Res. 2000; 48(1): 18-23. DOI: 10.1203/00006450-200007000-00006 [ Links ]
13.Bingham PM, Churchill D, Ashikaga T. Breast milk odor via olfactometer for tube-fed, premature infants. Behavior Research Methods. 2007; 39(3): 630-4. DOI: 10.3758/BF03193035 [ Links ]
14.Marlier L, Schaal B, Soussignan R. Neonatal responsiveness to the odor of amniotic and lacteal fluids: a test of perinatal chemosensory continuity. Child Dev. 1998; 69(3): 611-23. [ Links ]
15.Moura RGF, Cunha DA, Gomes AC de LG, Silva HJ da. Quantitative instruments used to assess children's sense of smell: a review article. CoDAS. 2014; 26(1): 96-101. DOI: 10.1590/s2317-17822014000100014 [ Links ]
16.Sarnat HB, Flores-Sarnat L, Wei X-C. Olfactory Development, Part 1: Function, From Fetal Perception to Adult Wine-Tasting. J Child Neurol. 2017; 32(6): 566-78. DOI: 10.1177/0883073817690867 [ Links ]
17.Schaal B, Marlier L, Soussignan R. Human Foetuses Learn Odours from their Pregnant Mother's Diet. Chemical Senses. 2000; 25(6): 729-37. DOI: 10.1093/chemse/25.6.729 [ Links ]
18.Schaal B, Marlier L, Soussignan R. Olfactory function in the human fetus: evidence from selective neonatal responsiveness to the odor of amniotic fluid. Behav Neurosci. 1998; 112(6): 1438-49. DOI: 10.1037//0735-7044.112.6.1438 [ Links ]
19.Albers CA, Grieve AJ. Test Review: Bayley, N. (2006). «Bayley Scales of Infant and Toddler Development--Third Edition». San Antonio, TX--Harcourt Assessment. Journal of Psychoeducational Assessment. 2007; 25(2): 180-90. DOI: 10.1177/0734282906297199 [ Links ]
20.Pizer J, ElBassiouny A. Wechsler Preschool and Primary Scale of Intelligence (WPPSI). Dans: The Wiley Encyclopedia of Personality and Individual Differences. John Wiley & Sons, Ltd; 2020. DOI: 10.1002/9781118970843.ch148 [ Links ]
21.Brazelton TB, Nugent JK. Neonatal behavioral assessment scale. London: Mac Keith Press; 2011. [ Links ]
22.Bunyavanich S, Do A, Vicencio A. Nasal Gene Expression of Angiotensin-Converting Enzyme 2 in Children and Adults. JAMA. 2020; 323(23): 2427. DOI: 10.1001/jama.2020.8707 [ Links ]
23.Yan CH, Faraji F, Prajapati DP, Boone CE, DeConde AS. Association of chemosensory dysfunction and COVID-19 in patients presenting with influenza-like symptoms. Int Forum Allergy Rhinol. 2020; 10(7): 806-13. DOI: 10.1002/alr.22579 [ Links ]
24.Somekh E, Gleyzer A, Heller E, Lopian M, Kashani-Ligumski L, Czeiger S, et al. The role of children in the dynamics of intra family coronavirus 2019 spread in densely populated area. Pediatr Infect Dis J. 2020; 39(8): e202-4. DOI: 10.1097/INF.0000000000002783 [ Links ]
 Correspondence:
Correspondence:
Kassandra Silva Falcão Costa
kassandrafcosta@gmail.com
Manuscript received: April 2021
Manuscript accepted: May 2021
Version of record online: July 2021


{kind=link}