










Serviços Personalizados
Journal

artigo
 Inglês (pdf)
Inglês (pdf)
 Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
Indicadores
Compartilhar

 Permalink
PermalinkJournal of Human Growth and Development
versão impressa ISSN 0104-1282versão On-line ISSN 2175-3598
J. Hum. Growth Dev. vol.31 no.2 Santo André maio/ago. 2021
https://doi.org/10.36311/jhgd.v31.11279
ORIGINAL ARTICLE
Foot rotation asymmetry in Down syndrome and the relationship with crawling and walking onset: a cross-sectional study
Camila ValeroI; Zan MustacchiII, III; Patrícia M. BezerraI; Francisco W. S. FigueiredoIV; Patricia Merly MartinelliIV; Alzira A. S. CarvalhoV; David FederVI
ICentro Universitário FMABC - Santo André/SP, Brazil;
IISetor de Genética do Hospital Infantil Darcy Vargas, São Paulo/SP, Brazil;
IIICentro de Estudos e Pesquisas Clínicas (CEPEC) - São Paulo (SP), Brazil;
IVDepartamento de Epidemiologia e Análise de Dados do Centro Universitário FMABC, Santo André/ SP, Brazil;
VDepartamento de Neurologia do Centro Universitário FMABC, Santo André/SP, Brazil;
VIDepartamento de Farmacologia do Centro Universitário FMABC, Santo André/SP, Brazil
ABSTRACT
INTRODUCTION: Down syndrome individuals have different gait patterns, which include specific characteristics such as foot rotation asymmetry
OBJECTIVE: The aim of this study was to analyze the relationship between this asymmetry and the hands-and-knees crawling pattern before gait acquisition in Down syndrome children, as well as the possible association of this gait to gender, ethnicity, comorbidities, physiotherapy, and occupational therapy interventions
METHODS: In this cross-sectional study, 361 children with or without foot rotation asymmetry were selected. An online questionnaire was administered to the parents or guardians of those children
RESULTS: Hands-and-knees crawling decreased the prevalence of foot rotation asymmetry in Down syndrome children. The longer it took for walking onset, the higher the prevalence of this asymmetry. Indeed, for each month of delay, there was a 7% increase in prevalence. There was a significant relationship between orthopedic alterations in knees or flat feet and foot rotation asymmetry. There was no significance related to gender, ethnicity, other comorbidities, physiotherapy, or occupational therapy interventions
CONCLUSION: The findings in this study revealed that foot rotation asymmetry might be related to the acquisition of motor skills, hands-and-knees crawling and the walking onset
Keywords: Down syndrome, gait, locomotion, motor skills, posture.
Authors summary
Why was this study done?
Down syndrome (DS) involves specific characteristics in motor development that require an intervention early. The gait becomes an important developmental milestone. Indeed, DS individuals have different gait patterns, such as foot rotation asymmetry. This study investigated the possible relationship between hands-and-knees crawling and this gait pattern, as well as the association of foot rotation asymmetry and others comorbidities and specific intervention.
What did the researchers do and find?
We elaborated an online questionnaire for parents and guardians of Down syndrome children with questions related to gender, ethnicity, neonatal complications, cardiac/orthopedic/visual/hearing/neurological alterations, physiotherapy and occupational therapy interventions, motor patterns, and motor acquisitions. From the analysis of this study, it is possible to perceive the relationship between foot rotation asymmetry and the previous acquisition of hands-and-knees crawling in Down syndrome. There was an association between walking onset and this asymmetry. Orthopedic alterations in knees or flat feet demonstrated a relationship with foot rotation asymmetry.
What do these findings mean?
The therapists should prioritize these acquisitions to prevent future gait alterations. Parents/guardians, in turn, should also stimulate the child to go through all motor skill development stages.
INTRODUCTION
In Brazil, Down syndrome (DS), also known as trisomy 21 (T21), is one of the major causes of birth deficiencies, with a prevalence of 1 in 600-800 births1. The presence of an extra copy of chromosome 21 is associated with easily identifiable physical and anatomical characteristics, which are accompanied by cardiac, orthopedic, visual, hearing, and neurological alterations that trigger a delay in motor development2-4.
Many researchers aim to find motor development parameters that manifest later in DS compared with ordinary children. These alterations occur due to dendritic growth deficiencies and abnormal myelination of cortical and subcortical structures of the brain, changes that lead to overall generalized synaptic dysfunction5. Thus, motor development differences occur by the fourth month of age. These differences amplify as motor demands become more complex, especially when muscle coactivation against gravity is required; this action is also hampered by muscular hypotonia and ligament laxity4,6,7.
A study that included the Test of Infant Motor Performance (TIMP) and Bayley Scales of Infant and Toddler Development (Bayley-III) showed that DS children present difficulty in early postural control and activities that require speed, postural control and balance8. Palisano et al.9. used the Gross Motor Function Measure (GMFM) to study the motor development of children between 1 and 6 years old. They concluded that it takes the DS population longer to learn the movements: the probability of reciprocal hands-and-knees crawling at 18 months old is 34%, and at 24 months old, it is over 50%.
Tudella et al.7 compared the motor development rate in 3-to-12-month-old DS infants using the Alberta Infant Motor Scale (AIMS). They concluded that the DS motor development sequence is the same with regards to typical infants. Still, it takes the DS group more time to acquire skills, especially anti-gravitational skills such as prone, sitting, and standing positions. Another study comparing typical and DS infants revealed the difficulty of the DS group regarding the prone (including crawling, acquired by only 33%), sitting, and standing positions due to the fact these positions require greater postural control 6.
These studies describe motor development landmarks in the DS population; however, they do not relate some motor acquisitions, such as crawling and foot rotation asymmetry, to factors including gender, ethnicity, specific comorbidities, and treatment length. Therefore, in the current study, a questionnaire was developed and administered to parents and/or guardians of DS children in order to relate foot rotation asymmetry and crawling to the hypothesis that crawling would bring about fewer risks to the development of this asymmetry. This study also analyzed whether foot rotation asymmetry is related to gender, ethnicity, cardiac, orthopedic, visual, and/or hearing impairments and specific comorbidities associated with birth. Besides, it included other motor acquisitions and physiotherapy and occupational therapy interventions.
METHODS
Study design
This cross-sectional study was performed according to the recommendations of the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) statement guidelines.
Scenario
Data were collected as part of a large DS cross-sectional study. It was conducted in Brazil over 2016 and 2017 (218 days total) and was approved by the Institution's Ethics Committee under file number 1.684.429.
Regarding legal requirements, the study was discussed and approved by the Center for Studies and Clinical Research of São Paulo (CEPEC-SP), owner of the website www.sindromededown.com.br, which hosted the data collection questionnaire.
On the CEPEC website, a short presentation informed parents and/or guardians of the DS children about the aim of the study and how they could voluntarily participate. In order to ensure anonymity, the names of the participants were not requested, which allowed for a closer approach to sensitive topics10 and enabled them to express themselves more freely in terms of feelings, experiences, and actions when dealing with their children. The Free and Informed Consent Form was on the website, and when starting to fill out the questionnaire, participants automatically authorized the analysis and publication of results.
The online questionnaire was titled "Pesquisa sobre o Desenvolvimento Motor em Crianças com Síndrome de Down" ("Research on Motor Development of Down Syndrome Children"). It was in Portuguese, added to the content of the website www.sindromededown.com.br, and promoted on Facebook using the web link www.survio.com/survey/d/B9P8H5G1U1X9Z1F5N. A member of the research team supervised the website until all the data were collected. Those individuals who answered the questions on the presence or absence of foot rotation asymmetry in the online questionnaire were screened and included in the study.
Instrument
Due to the lack of tools to evaluate the studied topic, such as an instrument specifically elaborated for DS individuals, a semi-structured questionnaire was designed by the authors of this study. Some research team members specialized in DS discussed the main topics that should be included, and many pre-tests were designed before the final approval.
Information including date, start time, and length of time for questionnaire completion was required. There were open- and closed-ended questions to which parents and/or guardians had to choose an alternative related to gender, apgar score, neonatal complications, ethnicity, cardiac/orthopedic/visual/hearing/neurological alterations, physiotherapy and occupational therapy interventions, motor patterns (on all fours and standing positions), and motor acquisitions (crawling, walking and foot rotation asymmetry). However, whenever necessary, questions related to age and/or other specific information were asked. With regards to questions specifically related to crawling, a figure showing a "child on all fours" position7 was included to avoid misinterpretations of hands-and-knees crawling.
The online access enabled parents and/or guardians to provide information more comprehensively and efficiently in a very economical way. Additionally, those individuals who were previously neglected in this kind of study, due to the long distances they had to travel to participate, could also be included11.
Participants
The intentional sample consisted of parents and/or guardians of DS children. The confirmation of a clinical diagnosis for DS was not required since their phenotypic alterations were quite clear. The children included were those who could crawl, and when they could walk, those with or without asymmetric foot rotation were identified.
Variables
The independent variables were those related to the motor development of the DS children. In order to obtain these variables, the following information was considered: gender, ethnicity, apgar score, neonatal complications, cardiac/respiratory/neurological/visual/hearing/orthopedic alterations, hospitalization, physiotherapy and occupational therapy interventions, ages at which specific motor development stages were attained (e.g., crawling, standing position with and without assistance), walking onset (three independent steps12) and independent gait. The above variables, particularly hands-and-knees crawling were related to the dependent variable foot rotation asymmetry.
Statistical methods
Standard descriptive statistics were performed. The chi-squared test was applied to analyze the association between the studied characteristics and the presence of asymmetric foot rotation in DS children. Poisson regression with robust variance was used to estimate the magnitude of this association.
With regards to quantitative variables, data normality was assessed with Shapiro-Wilk's test. Since the data were not normally distributed (p < 0.05), median and 95% confidence intervals (CI) were used for descriptive analysis. Interquartile range regression was used to analyze median differences with their respective 95% CI (significance level of 5%). Stata Student Lab Sciences 11.0 software (StataCorp LCC) was used for analysis.
RESULTS
Participants
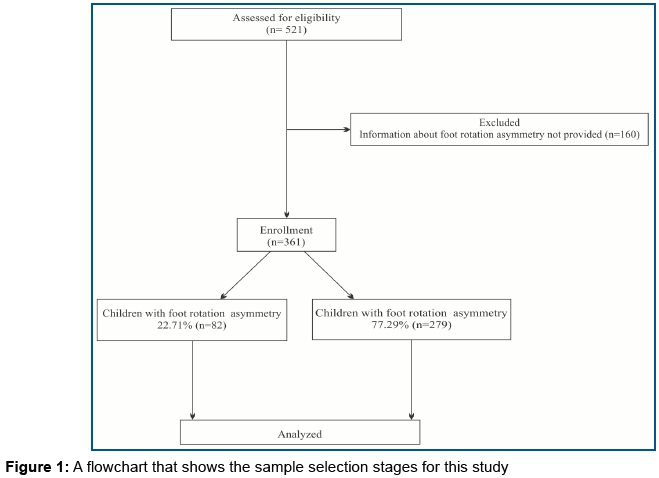
A total of 521 questionnaires were filled out by parents and/or guardians of DS children. Within this total, 160 questionnaires were excluded because the respondents did not provide any information concerning foot rotation asymmetry; this exclusion left 361 participants for analysis. From the 361 studied participants, foot rotation asymmetry was reported in 22.7% (n = 82) of the cases (figure 1).
Data description
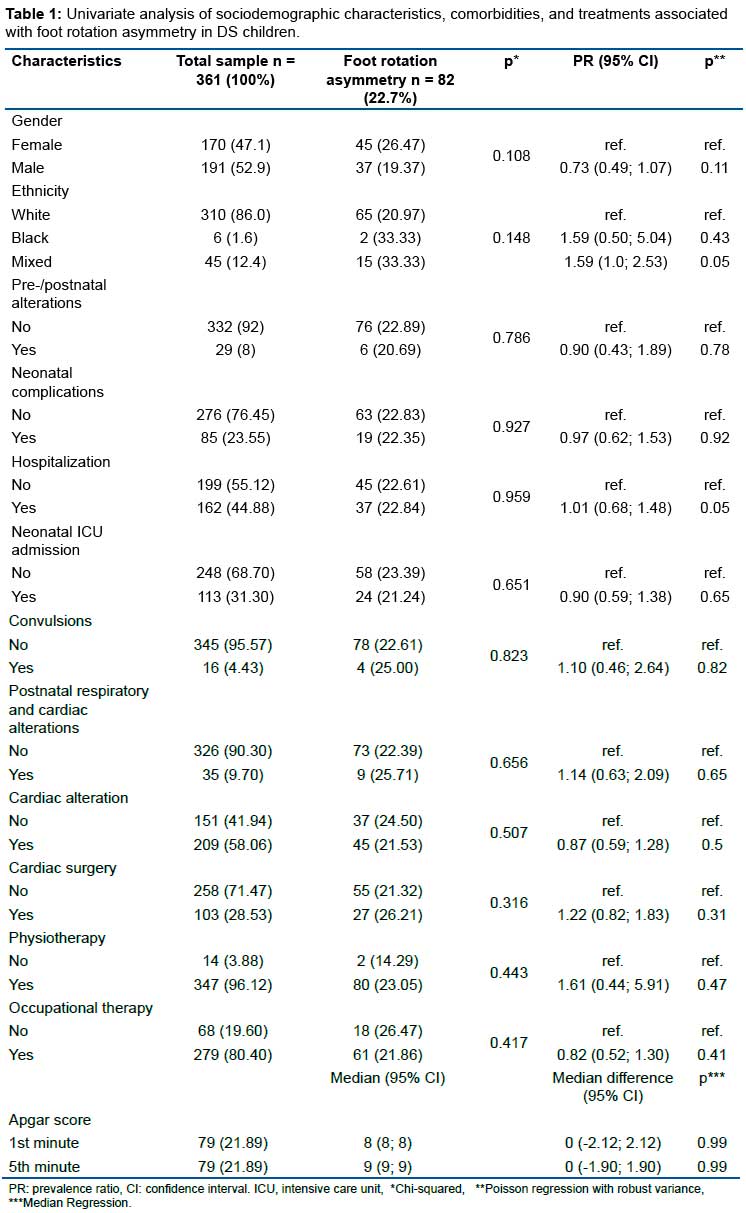
According to the characteristics shown in table 1, most of the children were male (52.9%; n = 191) and white (86%; n = 310). Cardiac and visual alterations (58% and 43%, respectively) were the most evident issues. With regards to reported treatments, the physiotherapy intervention rate (96%) was higher than in the occupational therapy intervention (80%). There were no statistically significant differences between sociodemographic characteristics, comorbidities, or treatments with the prevalence of foot rotation asymmetry in the studied population (table 1).
There were statistically significant associations between knee dysfunctions (p=0.002) and flat feet (p=0.019) with regards to foot rotation asymmetry (table 2). The presence of foot rotation asymmetry increased the appearance of knee alterations by 2% (p=0.002 indicates statistical significance). Flat feet, on the other hand, increased the prevalence of foot rotation asymmetry by approximately 1.5% (p=0.01 shows significance between variables (table 2).
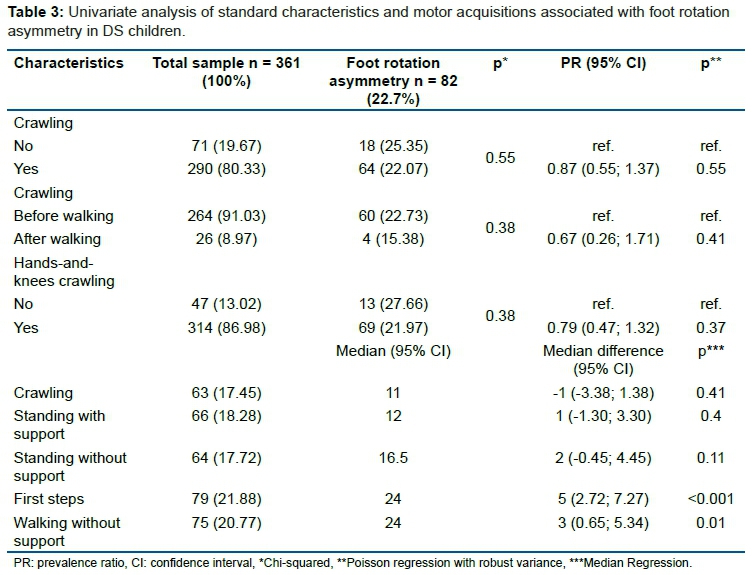
Among the studied motor development skills, crawling was acquired by 80.33% of the respondents (only 19.67% of the children did not acquire crawling skills). Hands-and-knees crawling, before or after the acquisition of walking, was not significantly different. However, the relationship between the first steps and foot rotation asymmetry was significant (p < 0.001) (table 3).
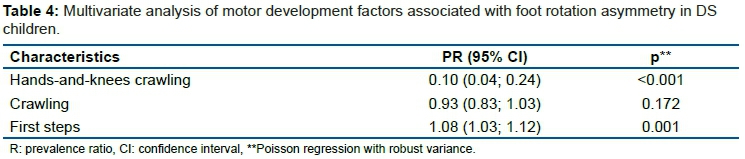
Table 4 presents multivariate analysis results regarding motor development factors. There was a significant association between hands-and-knees crawling and foot rotation asymmetry (p < 0.001).
Main results
Multivariate analysis revealed that hands-and-knees crawling reduced the appearance of foot rotation asymmetry in DS children by 10% (95% CI: 4-24%). On the other hand, the longer it took the child (in months) to take the first steps, the higher was the prevalence of asymmetric foot rotation (table 3).
DISCUSSION
Interpretation
Foot rotation asymmetry in Down syndrome has been studied and shown as one of the different walking patterns in these individuals13,14. However, studies on the relationship between foot rotation asymmetry and the specific acquisition of hands-and-knees crawling cannot be found in the literature. The importance of this investigation is paramount in this population since recent studies with ordinary children have revealed that hands-and-knees crawling is associated with not only the increase in muscular strength but also the coactivation of leg muscles, which boosts the developmental progression from crawling to erect walking15.
One of the proposals of this study was to associate foot rotation asymmetry with crawling. The results here found reveal that the prevalence of foot rotation asymmetry decreased due to the acquisition of hands-and-knees crawling, which confirms the hypothesis that crawling reduces the risk for the development of foot rotation asymmetry.
Angulo-Barroso et al.13 reached the conclusion that in DS the decrease in cases of foot rotation asymmetry was not related to treatments on treadmills at high or low intensities; however, another investigation confirms that the base width decreases according to age in this population, but this base is still wider when compared with control group14.
The current study also analyzed if foot rotation asymmetry is associated with other motor acquisitions, and significance in relation to first steps could be observed. The results showed that the longer it takes a child to take the first steps (in months), the higher the prevalence of a wider base of support. For each month of delay to take the first steps, this prevalence increases by 7%. Lloyd et al.16 showed that intense physical activity for the legs is related to the first steps. Interestingly, another study revealed that in this population, the intensity levels of leg activity were irrelevant for the first steps at the beginning of the interventions but significant at the end17.
This study did not show any association of foot rotation asymmetry with gender, ethnicity, other comorbidities, physiotherapy, or occupational therapy interventions. Rihtman et al.18 did not observe any association between gender and motor integration; however, some other previous studies on DS reported that girls have better motor development, and boys who were underweight and/or presented cardiac alterations had a slower development19. Malak et al.20 carried out a study with DS children in which the researchers confirmed that the upstanding and gait skills were delayed even when physiotherapy was performed. Other studies on the first months of DS children, however, revealed the vital importance of interventional treatments in the multiple areas of motor development21,22.
The results found in the current study showed significance between the comorbidity, knee alterations and foot rotation asymmetry. They confirm the findings of previous studies that report that patellar instability affects the motor function of SD individuals, compromising their gait and reducing the power generation and absorption in these joints. However, this kind of alteration is seldom found in the literature14,23.
Additionally, the current study also observed an association between flat feet and foot rotation asymmetry in DS, which was confirmed in researches where flat feet caused a greater outer foot rotation resulting in the worsening of the function. On the other hand, other studies did not report the relationship between flat feet with specific limitations to activities or overweight in this population24-26. Flat feet were present in 58% of the sample. Through clinical observation, Perotti et al.27 also found flat feet cases in 46% of SD children in their work. Some other studies found flat feet cases in 88% and 76% among the participants24-26.
From a clinical point of view, foot rotation asymmetry in DS was often observed in children who had not gone through the crawling phase, which aroused the interest to investigate if the data found were related to this fact. The results confirmed this observation, and surprisingly showed the relationship with the first steps and not with the treatment applied after the onset of the gait pattern expected in DS. Therefore, there should be more studies that focus on the skills acquired before the onset of gait.
The use of a movement capture system specific for the acquisition of crawling and not for the acquisition of gait alone16,17,28, a topic that has recently been studied among typical children15, would provide a broader view of which muscles are recruited at this stage as well as the strength of these muscles in DS children.
The findings reflect the need to prioritize all motor skill development stages, especially hands-and-knees crawling and first steps to prevent future gait alterations, including foot rotation asymmetry. The results suggest that therapists should then direct special attention to these acquisitions in order to prevent future gait alterations. At the same time, parents/guardians should stimulate their children to experience all the stages of motor development.
Methodological considerations
This online retrospective data collection reached a large number of people with DS. On the other hand, despite the importance, the researcher could not be present at the moment all the answers were provided for obvious reasons. Therefore, occasional doubts concerning the understanding of some questions, or even recall biases of the respondents when answering the questionnaire, may have led them to omit some information10,11. The ages of the participants were not collected due to the interest in the retrospective stages of motor development.
Author Contributions
CV: She had substantial contributions to the conception and design of the research, acquisition, interpretation of data for the work, and she contributed to drafting the work. ZM: He had substantial contributions to the conception and design of the research, acquisition of data for the work; he revised the article after the conclusion giving some suggestions. PMB and PMM: She contributed to the acquisition of data for the work, revising the article during the elaboration with new suggestions. FWSF: He contributed to making all statistical analysis, interpretation of data. He revised the article during the elaboration for important intellectual content. AASC: She contributed to the design of the work, revising it critically for important intellectual content. DF: He oriented all the research with substantial contributions to the conception and design of the work, revising it critically for important intellectual content. All the authors approved the final version to be published and agreed to be responsible for all aspects of the work, ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Funding
This research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors.
Acknowledgments
We would like to thank the Center for Studies and Clinical Research of São Paulo (CEPEC) and Doctor Zan Mustacchi, in particular, for all the trust and support provided. We would also like to thank all the parents and/or guardians of the Down syndrome patients for their participation in this study.
The financial viability of the article is due to the Acre - Health Project in the Western Amazon (multi-institutional agreement process no. 007/2015 SESACRE-UFAC-FMABC).
Conflicts of Interest
No author reported any conflict of interest.
REFERENCES
1.Ministério da Saúde, Secretaria de Atenção à Saúde, Departamento de Ações Programáticas Estratégicas. - 1. ed., 1. reimp. - Brasília: Ministério da Saúde, 2013. 60 p.: il. [ Links ]
2.Bull MJ, the Committee on Genetics. Health supervision for children with down syndrome. PEDIATRICS. 1o de agosto de 2011; 128(2): 393-406. [ Links ]
3.Roizen NJ, Patterson D. Down's syndrome. The Lancet. abril de 2003; 361(9365): 1281-9. [ Links ]
4.Lott IT. Neurological phenotypes for Down syndrome across the life span. In: Progress in Brain Research [Internet]. Elsevier; 2012 p. 101-21. Disponível em: https://linkinghub.elsevier.com/retrieve/pii/B9780444542991000066 [ Links ]
5.Wisniewski KE. Down syndrome children often have brain with maturation delay, retardation of growth, and cortical dysgenesis. Am J Med Genet. 6 de junho de 2005; 37(S7):274-81. [ Links ]
6.Pereira K, Basso RP, Lindquist ARR, Silva LGP da, Tudella E. Infants with Down syndrome: Percentage and age for acquisition of gross motor skills. Research in Developmental Disabilities. Março de 2013; 34(3): 894-901. [ Links ]
7.Tudella E, Pereira K, Basso RP, Savelsbergh GJP. Description of the motor development of 3-12 month old infants with Down syndrome: The influence of the postural body position. Research in Developmental Disabilities. setembro de 2011; 32(5): 1514-20. [ Links ]
8.Cardoso AC das N, de Campos AC, dos Santos MM, Santos DCC, Rocha NACF. Motor performance of children with down syndrome and typical development at 2 to 4 and 26 months. Pediatric Physical Therapy. 2015; 27(2): 135-41. [ Links ]
9.Palisano RJ, Walter SD, Russell DJ, Rosenbaum PL, Gémus M, Galuppi BE, et al. Gross motor function of children with down syndrome: Creation of motor growth curves. Archives of Physical Medicine and Rehabilitation. abril de 2001; 82(4): 494-500. [ Links ]
10.Walker D-M. The internet as a medium for health services research. Part 2. Nurse Researcher. Maio de 2013; 20(5): 33-7. [ Links ]
11.Meho LI. E-mail interviewing in qualitative research: A methodological discussion. J Am Soc Inf Sci. agosto de 2006; 57(10): 1284-95. [ Links ]
12.Wu J, Ulrich DA, Looper J, Tiernan CW, Angulo-Barroso RM. Strategy adoption and locomotor adjustment in obstacle clearance of newly walking toddlers with down syndrome after different treadmill interventions. Exp Brain Res. março de 2008; 186(2): 261-72. [ Links ]
13.Angulo-Barroso RM, Wu J, Ulrich DA. Long-term effect of different treadmill interventions on gait development in new walkers with Down syndrome. Gait & Posture. Fevereiro de 2008; 27(2): 231-8. [ Links ]
14.Rigoldi C, Galli M, Albertini G. Gait development during lifespan in subjects with Down syndrome. Research in Developmental Disabilities. Janeiro de 2011; 32(1): 158-63. [ Links ]
15.Xiong QL, Hou WS, Xiao N, Chen YX, Yao J, Zheng XL, et al. Motor skill development alters kinematics and co-activation between flexors and extensors of limbs in human infant crawling. IEEE Trans Neural Syst Rehabil Eng. Abril de 2018; 26(4): 780-7. [ Links ]
16.Lloyd M, Burghardt A, Ulrich DA, Angulo-Barroso R. Physical activity and walking onset in infants with down syndrome. Adapted Physical Activity Quarterly. Janeiro de 2010; 27(1): 1-16. [ Links ]
17.Angulo-Barroso R, Burghardt AR, Lloyd M, Ulrich DA. Physical activity in infants with Down syndrome receiving a treadmill intervention. Infant Behavior and Development. Abril de 2008; 31(2): 255-69. [ Links ]
18.Rihtman T, Tekuzener E, Parush S, Tenenbaum A, Bachrach SJ, Ornoy A. Are the cognitive functions of children with Down syndrome related to their participation? Developmental Medicine & Child Neurology. Janeiro de 2010; 52(1): 72-8. [ Links ]
19.Aoki S, Yamauchi Y, Hashimoto K. Developmental trend of children with Down's syndrome - How do sex and neonatal conditions influence their developmental patterns? Brain and Development. Março de 2018; 40(3): 181-7. [ Links ]
20. Malak R, Kostiukow A, Krawczyk-Wasielewska A, Mojs E, Samborski W. Delays in motor development in children with down syndrome. Med Sci Monit. 2015; 21: 1904-10. [ Links ]
21.Kloze A, Brzuszkiewicz-Kuzmicka G, Czyzewski P. Use of the timp in assessment of motor development of infants with down syndrome. Pediatric Physical Therapy. 2016; 28(1): 40-5. [ Links ]
22. Wentz EE. Importance of initiating a "tummy time" intervention early in infants with down syndrome. Pediatric Physical Therapy. Janeiro de 2017; 29(1): 68-75. [ Links ]
23. Kocon H, Kabacyj M, Zgoda M. The results of the operative treatment of patellar instability in children with Down's syndrome. Journal of Pediatric Orthopaedics B. setembro de 2012; 21(5): 407-10. [ Links ]
24.Galli M, Cimolin V, Rigoldi C, Pau M, Costici P, Albertini G. The effects of low arched feet on foot rotation during gait in children with Down syndrome: Low arched feet and foot rotation. J Intellect Disabil Res. Agosto de 2014; 58(8): 758-64. [ Links ]
25.Concolino D, Pasquzzi A, Capalbo G, Sinopoli S, Strisciuglio P. Early detection of podiatric anomalies in children with Down syndrome. Acta Paediatrica. 1o de janeiro de 2006; 95(1): 17-20. [ Links ]
26.Lim PQ, Shields N, Nikolopoulos N, Barrett JT, Evans AM, Taylor NF, et al. The association of foot structure and footwear fit with disability in children and adolescents with Down syndrome. J Foot Ankle Res. dezembro de 2015; 8(1): 4. [ Links ]
27.Perotti LR, Abousamra O, del Pilar Duque Orozco M, Rogers KJ, Sees JP, Miller F. Foot and ankle deformities in children with Down syndrome. J Child Orthop. junho de 2018; 12(3): 218-26. [ Links ]
28.Gontijo APB, Mancini MC, Silva PLP, Chagas PSC, Sampaio RF, Luz RE, et al. Changes in lower limb co-contraction and stiffness by toddlers with Down syndrome and toddlers with typical development during the acquisition of independent gait. Human Movement Science. agosto de 2008; 27(4): 610-21. [ Links ]
 Correspondence:
Correspondence:
Camila Valero
cavalero25@gmail.com
Manuscript received: January 2021
Manuscript accepted: June 2021
Version of record online: July 2021


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}