










Serviços Personalizados
Journal

artigo
 Inglês (pdf)
Inglês (pdf)
 Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
 Curriculum ScienTI
Curriculum ScienTIIndicadores
Compartilhar

 Permalink
PermalinkTemas em Psicologia
versão impressa ISSN 1413-389X
Temas psicol. vol.24 no.1 Ribeirão Preto mar. 2016
https://doi.org/10.9788/TP2016.1-25
ARTIGOS
Factor structure, reliability, and item parameters of the brazilian-portuguese version of the GAD-7 questionnaire
Estrutura fatorial, fidedignidade e parâmetros de itens da versão em português brasileiro do questionário GAD-7
Estructura factorial, confiabilidad, y ítems parámetros de la versión de portugués brasileño del cuestionario GAD-7
André Luiz MorenoI; Diogo Araújo DeSousaII; Ana Maria Frota Lisbôa Pereira de SouzaIII; Gisele Gus ManfroIV; Giovanni Abrahão SalumIV; Silvia Helena KollerV; Flávia de Lima OsórioVI; José Alexandre de Souza CrippaVI
IPost-Graduate Program in Mental Health, Ribeirão Preto Medical School, University of São Paulo, Ribeirão Preto, SP, Brazil
IICenter of Psychological Studies on At Risk Populations (CEP-Rua), Post-Graduate Program in Psychology, Institute of Psychology, Federal University of Rio Grande do Sul, Porto Alegre, RS, Brazil. Anxiety Disorders Outpatient Program for Child and Adolescent Psychiatry (PROTAIA), Post-Graduate Program in Medical Sciences: Psychiatry, Hospital de Clínicas de Porto Alegre, Federal University of Rio Grande do Sul, Porto Alegre, RS, Brazil
IIICEP-Rua, Post-Graduate Program in Psychology, Institute of Psychology, Federal University of Rio Grande do Sul, Porto Alegre, RS, Brazil
IVPROTAIA, Post-Graduate Program in Medical Sciences: Psychiatry, Hospital de Clínicas de Porto Alegre, Federal University of Rio Grande do Sul, Porto Alegre, RS, Brazil
VCEP-Rua, Post-Graduate Program in Psychology, Institute of Psychology, Federal University of Rio Grande do Sul, Porto Alegre, RS, Brazil
VIPost-Graduate Program in Mental Health, Ribeirão Preto Medical School, University of São Paulo, Ribeirão Preto, SP, Brazil
ABSTRACT
This study examined the psychometric properties of the Brazilian-Portuguese version of the Generalized Anxiety Disorder GAD-7 questionnaire in a community sample (n = 206) of Brazilian adults. The sample was 41% female, with a mean age of 21.10 (SD = 4.49),75.6% from colleges/universities. Results of a confirmatory factor analysis provided support to the original unidimensional model of the GAD-7 in the Brazilian context. Analyses of Variance (ANOVA) showed that the GAD-7 scores were significantly different between males and females, with females scoring higher than males. The scale demonstrated good reliability evidence; both Cronbach's alpha coefficient (α = .916) and rho composite reliability coefficient (ρ= .909) were adequate. Item parameter analysis showed items 5 and 7 presented the highest severity thresholds for the generalized anxiety latent trait, whereas item 1 presented the lowest ones. Our findings suggest that the Brazilian-Portuguese version of the GAD-7 is suitable for assessing Generalized Anxiety Disorder symptoms in Brazilian adults in community settings.
Keywords: GAD-7, Generalized Anxiety Disorder, anxiety, psychometrics.
RESUMO
Este estudo analisou as propriedades psicométricas da versão em Português Brasileiro do questionário de "Transtorno de Ansiedade Generalizada - GAD-7 em uma amostra de comunidade (n = 206) da população adulta brasileira. A amostra foi composta por de 41% de participantes do sexo feminino, com idade média de 21,10 (DP = 4,49), e 75,6% em instituições de ensino superior. Os resultados da análise fatorial confirmatória forneceram apoio para o modelo unidimensional original do GAD-7 no contexto brasileiro. As análises de variância (ANOVA) mostraram que os escores do GAD-7 foram significativamente diferentes entre homens e mulheres, com as mulheres apresentando maiores escores que os homens. A escala demonstrou uma boa fidedignidade; sendo que tanto o coeficiente de Cronbach alfa (α = 0,916) e rho coeficiente de confiabilidade composta (ρ = 0,909) foram adequados. A análise dos parâmetros dos itens mostrou itens 5 e 7 apresentaram os limiares mais elevados de severidade para o traço-latente de ansiedade generalizada, enquanto que o item 1 apresentou as menores. Nossos resultados sugerem que a versão Português Brasileiro do GAD-7 é adequada para avaliar os sintomas do transtorno de ansiedade generalizada em adultos brasileiros em ambientes comunitários.
Palavras-chave: GAD-7, Transtorno de Ansiedade Generalizada, ansiedade, psicometria.
RESUMEN
Este estudio examinó las propiedades psicométricas de la versión de portugués brasileño del cuestionario de Desorden de Ansiedad Generalizada GAD-7, en una muestra comunitaria (n = 206) de adultos brasileños. La muestra se compone de 41% de mujeres, con una edad media de 21,10 (SD = 4,49), y 75,6% estudiantes universitarios. El análisis factorial confirmatorio proporcionó evidencias que soportan el modelo unidimensional original del GAD-7 en el contexto brasileño. El análisis de variancia (ANOVA) mostró que las puntuaciones fueron significativamente diferentes entre hombres y mujeres, siendo que las mujeres obtuvieron puntuaciones más altas que los hombres. La escala demostró tener una buena confiabilidad; el coeficiente de alpha de Cronbach (α= .916) y el coeficiente rho de fiabilidad (ρ = .909) fueron adecuados. El análisis de datos mostró los ítems 5 y 7 tuvieron los umbrales de gravedad más altos en el trazo de ansiedad generalizada, mientras el ítem 1 tuvo el más bajo. Nuestros hallazgos sugieren que la versión en portugués brasileño de GAD-7 es adecuado para la evaluación de síntomas de trastorno de ansiedad generalizada en adultos brasileños en contextos comunitarios.
Palabras clave: GAD-7, Desorden Generalizado de Ansiedad, ansiedad, psicometría.
The Generalized Anxiety Disorder (GAD) is characterized by the presence of exaggerated anxiety and worries, which the individual has difficulties to control, related to a variety of contexts and situations, along with physiological symptoms (American Psychiatric Association, 2013). GAD is one of the most common mental disorders and the most prevalent disorder in the anxiety disorders group (Wittchen, 2002). GAD is highly comorbid with other mental disorders (Jacobi et al., 2004) and other non-psychiatric problems (Hoyer, Hofler, Jacobi, & Wittchen, 2003) and associated with a variety of negative outcomes. Valid instruments to measure GAD symptoms are essential for both clinicians and researchers.
Professionals and practitioners use a variety of instruments to diagnose GAD, such as general diagnostic interviews (e.g., the Structured Clinical Interview for the DSM-IV; Del-Ben et al., 2001) or even self-report measures of worry (e.g., the Penn State Worry Questionnaire; Castillo, Macrini, Cheniaux, & Landeira-Fernandez, 2010). Nevertheless, the straight-forward assessment of GAD symptoms can favor the screening of this specific mental disorder, which can influence the prognosis and treatment possibilities.
In this context, the Generalized Anxiety Disorder 7-item scale (GAD-7; Spitzer, Kroenke, Williams, & Löwe, 2006) is a self-report measure specifically developed to assess GAD symptoms. The GAD-7 items were developed based on the DSM-IV criteria and other anxiety assessment instruments. The short amount of time required to its application and the objectivity of the items make it an easy-to-administer alternative measure of GAD symptoms in clinical and research contexts. Because of these advantages, the GAD-7 has already been adapted to different countries (e.g., Spain; García-Campayo et al., 2010); Germany (Donker, Straten, Marks, & Cuijpers, 2011); Malaysia (Sidik, Arroll, & Goodyear-Smith, 2012) and to different clinical contexts (e.g., Delgadillo et al., 2012; Ruiz et al., 2011), being also used in many experimental studies (Robinson et al., 2010; Stoop, Spek, Pop, & Pouwer, 2011; Titov et al., 2009) and considered the best-performing test do assess GAD (Herr, Williams, Benjamin, & McDuffie, 2014).
However, to our knowledge, although there is a Brazilian-Portuguese version of the GAD-7 available online (Pfizer, 2013), no psychometric study has investigated the adequacy of the Brazilian version of the GAD-7. Moreover, according to a recent systematic review of the literature, none of the self-report scales available in Brazil to the assessment of anxiety symptoms was specifically designed to assess GAD symptoms (DeSousa, Moreno, Manfro, Gauer, & Koller, 2013). The aim of this study was therefore to investigate psychometric properties of a Brazilian-Portuguese version of the GAD-7. The specific aims were: (a) to examine the factor structure of the Brazilian version of the GAD-7 questionnaire; (b) to assess item performance of the GAD-7 items (i.e., item characteristic curves and thresholds); and (c) to evaluate the internal consistency and reliability of the Brazilian version of the GAD-7 score.
Method
Participants and Procedures
We recruited 206 Brazilian young adults and adults from universities, colleges, and preparation courses to university enrollment in the states of Rio Grande do Sul (n = 114) and Minas Gerais (n = 92). Participants were asked to complete a sociodemographic sheet and the GAD-7 questionnaire during their classroom period. One protocol presented missing values in the GAD-7 questionnaire items and was therefore excluded from analyses. The analytic sample consisted of 205 participants. Institutional approval was obtained before participation and all participants signed informed consent forms which explained the research objectives, risks, benefits, procedure, and their rights as participants. The study design was approved by the local Ethics Committee (project number 25298). The demographic characterization of the sample is depicted in Table 1.
Instrument
The Generalized Anxiety Disorder 7-item scale (GAD-7; Spitzer et al., 2006) is a 7-item self-report measure of generalized anxiety symptoms grouped into one factor of generalized anxiety. Respondents score each item in a 4-point scale based on how often they have been bothered by the described symptoms over the last two weeks (not at all = 0; several days = 1; more than half the days = 2; nearly every day = 3). Total scores range from 0 to 21, with higher scores reflecting higher severity levels of GAD symptomatology. The original items and instructions in the GAD7 were translated to Brazilian-Portuguese by two independent translators followed by an evaluation of the revised translated version by a group of experts and focus groups.
Data Analysis
A Confirmatory Factor Analysis (CFA) was conducted to evaluate whether the unidimensional model of the GAD-7 proposed by studies from other cultures (Donker et al., 2011; García-Campayo et al., 2010; Sidik et al., 2012, Spitzer et al., 2006) fits to the Brazilian context. We conducted the CFA using the Weighted Least Squares Means and Variance Adjusted (WLSMV) estimation method to account for the categorical nature of the items, in the Mplus software version 7.11. For fit indices, we cal-culated the Comparative Fit Index (Cfi), the Tucker-Lewis Index (TLI), and the Root Mean Square Error of Approximation (RMSEA) with a 90% confidence interval. Values of the Cfiand TLI higher than .90 represent an acceptable fit, and higher than .95 represent a good fit. Values of the RMSEA lower than .08 represent an acceptable fit, and lower than .05 represent a good fit (Brown; 2006; Hu & Bentler, 1999).
Standardized regression weights as factor loadings of the items were calculated in the CFA. Furthermore, item performance analyses were also calculated. Three thresholds were computed for each item (T1, T2, T3), representing the latent trait level at which there is a 50% probability of endorsing a given response option or higher in the scale (in this case, T1 = transition from endorsing "not at all" to endorsing "several days" or higher; T2 = transition from endorsing "several days" to endorsing "more than half the days" or higher; and T3 = transition from endorsing "more than half the days" to "nearly every day"). The mean of these three thresholds was also calculated to provide a single estimate of each item's difficulty (i.e., the item location in the severity continuum represented by the latent trait). Item characteristic curves were plotted for each item representing a function of the probability of endorsing each of the response option categories along the latent trait estimated by the GAD-7 factor scores.
Multigroup CFA was conducted to evaluate the measurement invariance of the model across genders (male vs. female participants). We tested an unconstrained model to assess configural invariance (i.e., whether the scale configuration; number of factors and items per factor) was acceptable for both males and females; and two constrained models to assess metric invariance (constraining the factor loadings to be equal across groups) and scalar invariance (constraining the factor loadings and intercepts/thresholds to be equal across groups). The χ2 difference test and the Cfidifference test (ΔCfi) evaluated measurement invariance between the models (configural vs. metric; and metric vs. scalar). If the difference between indices was not significant (i.e., χ2 p > .05; and ΔCfi< .01), the difference tests indicate factorial invariance for the evaluated parameter (Brown, 2006).
The Cronbach's alpha coefficient was calculated to evaluate the internal consistency of the GAD-7 score. Alpha values higher than .70 are deemed adequate. We also calculated Raykov's reliability rho coefficient to have a measure of composite reliability of the instrument, which presents advantages over Cronbach's alpha coefficient (Raykov, 1998). Values of the rho coefficient higher than .80 indicate good reliability.
Results
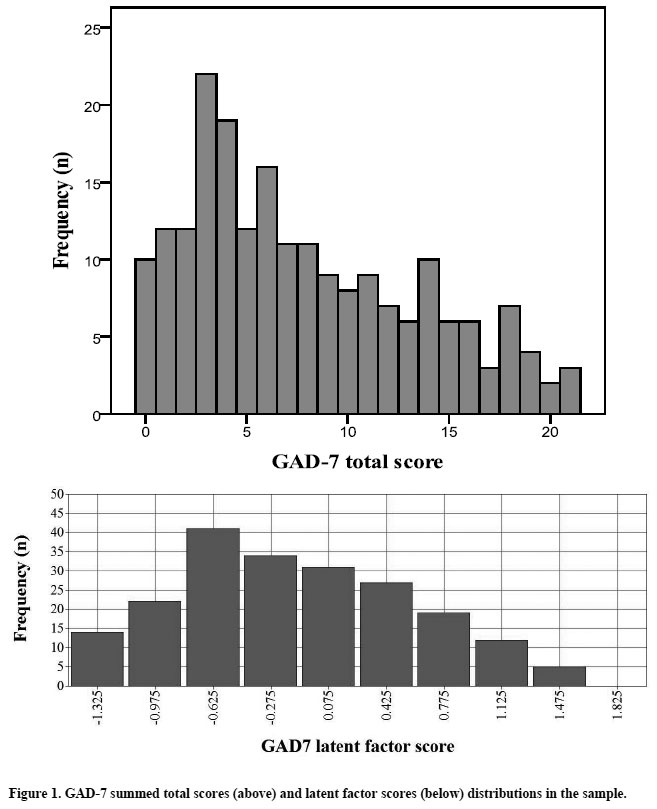
Table 1 depicts the descriptive analyses of the mean GAD-7 scores for the total sample and demographic subsamples. Analyses of Variance (ANOVAs) showed that the GAD-7 scores were significantly different between males and females, with females scoring higher than males, but not significantly different between high school participants and college/university participants. Figure 1 shows the histograms with the distributions of the GAD-7 summed total scores (raw sum of scores) and latent factor scores (estimated scores from the CFA) in the total sample.
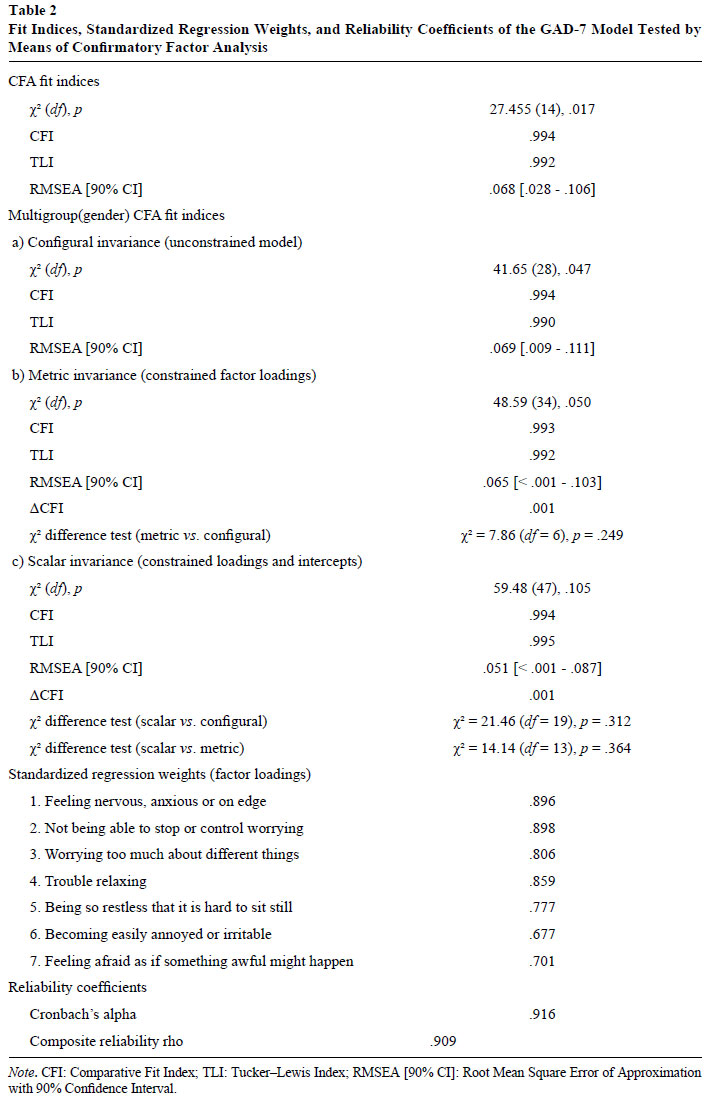
Table 2 depicts the results for the CFA fit indices, standardized regression weights, and reliability coefficients. The fit indices demonstrated that the unidimensional model had acceptable (RMSEA) to good fit (Cfi, TLI) to the sample. The multigroup CFA results showed that the unconstrained model (configural invariance) provided acceptable fit indices, supporting that the one-factor model is plausible for both boys and girls. The constrained models (metric and scalar) also presented acceptable fit indices and non-significant χ2 difference tests and ΔCfi. Since constraining the factor loadings and the intercepts/thresholds to be equal across genders did not significantly change the fit indices of the model, our results indicate that the GAD-7 presented similar patterns of these parameters for boys and girls. Standardized regression weights of the 7 items were all above .60, ranging from .677 to .898 with a mean of .802 (SD = .089). The Cronbach's alpha coefficient and the composite reliability rho coefficient were also adequate.
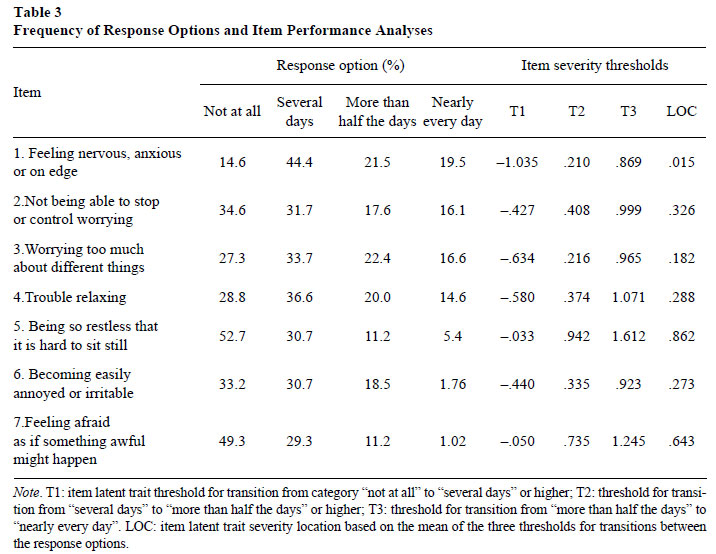
The frequency of response options for each item and item performance analyses are shown in Table 3. Severity thresholds estimates demonstrated that item 1 ("feeling nervous, anxious or on edge") presented the lowest severity estimates whereas item 7 ("feeling afraid as if something awful might happen") and even more item 5 ("being so restless that it is hard to sit still") presented high severity estimates. These results indicate that subjects who endorse higher categories of items 5 and 7 have relatively higher levels of the generalized anxiety latent trait than those who endorse higher categories of the remaining items in the GAD-7 questionnaire, especially item 1. Figure 2 depicts graphic information on the item parameter analyses, representing all item characteristic curves (ICC) of the scale. Overall the ICC showed good evidence of the functioning of the four response options of each item in the scale along the estimated latent trait of generalized anxiety. Only item 7 presented a problem considering the third option ("more than half the days") since there was no range in the latent trait in which this option had a higher probability of being endorsed than the other three response options.
Discussion
This study evaluated the adequacy of the Brazilian-Portuguese version of the GAD-7, an instrument designed to assess symptoms of GAD. Our results support the original unidimensional structure of the instrument and demonstrate evidence of reliability in terms of internal consistency and composite reliability. Furthermore item parameter results highlight severity differences among the seven items in the scale in identifying pathological states of generalized anxiety.
The unidimensional factor structure fit our Brazilian data well, supporting the original conceptualization of the GAD-7 (Spitzer et al., 2006). The one-factor model has been supported by several cross-cultural adaptations of the GAD-7 instrument, suggesting that this is a good model to assess GAD symptoms worldwide (Donker et al., 2011; García-Campayo et al., 2010; Sidik et al., 2012).
All seven items in the GAD-7 questionnaire presented high factor loadings, and the GAD-7 total score demonstrated high internal consistency, in line with previous research (Donker et al., 2011; García-Campayo et al., 2010), as well as high composite reliability. Significant differences were found between genders in our sample, with females scoring higher in the questionnaire. Higher scores in generalized anxiety measures among females is an expected result; for instance, the fifth edition of the Diagnostic and Statistical Manual of Mental Disorders (DSM-5; American Psychiatric Association, 2013) points that females are twice as likely to experience GAD than males. In this case, discriminative validity between genders is another important property of GAD-7. Also, as could be hypothesized, the histogram of the distribution of the GAD-7 scores was positively skewed, which is an expected distribution when dealing with psychopathological symptoms in community samples, especially when the prevalence rates of GAD in community samples are considered (DSM5; American Psychiatric Association, 2013).
Our findings from the item parameters analyses showed that items 7 ("feeling afraid as if something awful might happen") and 5 ("being so restless that it is hard to sit still") were the most severe. To endorse such description in their self-report, individuals are therefore expected to present a relatively high level of the generalized anxiety latent trait. This suggests that these items may be the best ones in the GAD-7 questionnaire for differentiating subjects with high levels of the GAD latent trait. The first item in the scale ("feeling nervous, anxious or on edge"), on the other hand, presented a quite low severity estimate. This suggests that this item might be a good candidate for differentiating GAD patients from subjects without anxiety problems. This could be discussed based on the description of these items. The items 5 and 7 describe sensations that are considered specifically to GAD diagnosis (DSM-5; American Psychiatric Association, 2013), while item 1 describe a sensation that fits in every anxiety disorder or even in non-clinical descriptions of stressful situations. Therefore, the high specificity demonstrated in items 5 and 7 of this paper endorses that the Brazilian-Portuguese version of GAD-7 is useful for screen GAD in community samples.
Future research focusing on the psychometric properties of the Brazilian-Portuguese version of the GAD-7 should investigate further psychometric properties of the instrument such as convergent and divergent validity, test-retest reliability, and discriminative validity for clinical samples. Studies testing these properties could account for some of the limitations of the present study, such as the fact that we did not have clinical data to assess the utility of the GAD-7 measure for helping in diagnostic procedures and sensitivity to treatment response.
In conclusion, our results suggest that the GAD-7 is a reliable instrument to assess GAD symptoms in Brazilian samples as a unidimensional measure. The Brazilian-Portuguese version of the GAD-7 is very similar to the original version of the instrument, which encourages cross-cultural studies to use this questionnaire. Nonetheless, researchers and clinicians that use the GAD-7 questionnaire to assess GAD symptoms in their practice should be aware of the specificities of the items in the scale, such as the different severity levels of each item.
References
American Psychiatric Association. (2013). Diagnostic and statistical manual of mental disorders. Fifth edition (DSM-5). Arlington, VA: Author. [ Links ]
Brown, T. A. (2006). Confirmatory factor analysis for applied research. New York: The Guilford Press. [ Links ]
Castillo, C., Macrini, L., Cheniaux, E., & Landeira-Fernandez, J. (2010). Psychometric properties and latent structure of the Portuguese version of the Penn State Worry Questionnaire. The Spanish Journal of Psychology, 13(1),431-443. doi:10.1017/S113874160000398X [ Links ]
Del-Ben, C. M., Vilela, J. A. A., Crippa, J. A. S., Hallak, J. E. C., Labate, C. M., & Zuardi, A. W. (2001). Confiabilidade da "Entrevista Clínica Estruturada para o DSM-IV - Versão Clínica" traduzida para o português. Revista Brasileira de Psiquiatria, 23(3),156-159. doi:10.1590/S1516-44462001000300008 [ Links ]
Delgadillo, J., Payne, S., Gilbody, S., Godfrey, C., Gore, S., Jessop, D., & Dale, V. (2012). Brief case finding tools for anxiety disorders: Validation of GAD-7 and GAD-2 in addictions treatment. Drug and Alcohol Dependence, 125,37-42. doi:10.1016/j.drugalcdep.2012.03.011 [ Links ]
DeSousa, D. A., Moreno, A. L., Manfro, G. G., Gauer, G., & Koller, S. H. (2013). Revisão sistemática de instrumentos para avaliação de ansiedade na população brasileira. Avaliação Psicológica, 12(3),397-410. [ Links ]
Donker, T., Straten, A. V., Marks, I., & Cuijpers, P. (2011). Quick and easy self-rating of Generalized Anxiety Disorder: Validity of the Dutch web-based GAD-7, GAD-2 and GAD-SI. Psychiatry Research, 188,58-64. doi:10.1016/j.psychres.2011.01.01 [ Links ]
García-Campayo, J., Zamorano, E., Ruiz, M. A., Pardo, A., Pérez-Páramo, M., López-Gómez, V., ...Rejas, J. (2010). Cultural adaptation into Spanish of the Generalized Anxiety Disorder-7 (GAD-7) scale as a screening tool. Health and Quality of Life Outcomes, 8,8. doi:10.1186/1477-7525-8-8 [ Links ]
Herr, N. R., Williams, J. W., Benjamin, S., & McDuffie, J. (2014). Does this patient have generalized anxiety or panic disorder?: The Rational Clinical Examination systematic review. The Journal of the American Medical Association, 312(1),78-84. doi:10.1001/jama.2014.5950 [ Links ]
Hoyer, J., Hofler, M., Jacobi, F., & Wittchen, H.U. (2003). Physical illnesses and generalized anxiety disorder. Psychosomatic Medicine Psychological, 53(2),112. [ Links ]
Hu, L., & Bentler, P. M. (1999). Cutoff criteria for fit indexes in covariance structure analysis: Conventional criteria versus new alternatives. Structural Equation Modeling: A Multidisciplinary Journal, 6,1-55. doi:10.1080/10705519909540118 [ Links ]
Jacobi, F., Wittchen, H. U., Holting, M., Hofler, M., Pfister, H., Muller, N., & Lieb, R. (2004). Prevalence, co-morbidity and correlates of mental disorders in the general population: Results from the German Health Interview and Examination Survey (GHS). Psychological Medicine, 34,1-15. doi:10.1017/S0033291703001399 [ Links ]
Pfizer Inc. (2013). Portuguese for Brazil version of the GAD-7 Screener. Retrieved from http://www.phqscreeners.com/pdfs/03_GAD-7/GAD7_Portuguese%20for%20Brazil.pdf [ Links ]
Raykov, T. (1998). Coefficient alpha and composite reliability with interrelated nonhomogeneous items. Applied Psychological Measurement, 22(4),375-385. doi:10.1177/014662169802200407 [ Links ]
Robinson, E., Titov, N., Andrews, G., McIntyre, K., Schwencke, G., & Solley, K. (2010). Internet treatment for Generalized Anxiety Disorder: A randomized controlled trial comparing clinician vs. technician assistance. PlosOne, 5(6),e10942. doi:10.1371/journal.pone.0010942 [ Links ]
Ruiz, M. A., Zamorano, E., García-Campayo, J., Pardo, A., Freire, O., & Rejas, J. (2011). Validity of the GAD-7 scale as an outcome measure of disability in patients with generalized anxiety disorders in primary care. Journal of Affective Disorders, 128,277-286. doi:10.1016/j.jad.2010.07.010 [ Links ]
Sidik, S. M., Arroll, B., & Goodyear-Smith, F. (2012). Validation of the GAD-7 (Malay version) among women attending a primary care clinic in Malaysia. Journal of Primary Health Care, 4(1),5-11. [ Links ]
Spitzer, R. L., Kroenke, K., Williams, J. B., & Löwe, B. (2006). A brief measure for assessing generalized anxiety disorder: The GAD-7. JAMA Internal Medicine, 166,1092-1097. doi:10.1001/archinte.166.10.1092 [ Links ]
Stoop, C. H., Spek, V. R. M., Pop, V. J. M., & Pouwer, F. (2011). Disease management for co-morbid depression and anxiety in diabetes mellitus: Design of a randomised controlled trial in primary care. BMC Family Practice, 12,139. doi:10.1186/1471-2296-12-139 [ Links ]
Wittchen, H. U. (2002). Generalized anxiety disorder: Prevalence, burden, and cost to society. Depression and Anxiety, 16,162-171. doi:10.1002/da.10065 [ Links ]
Titov, N., Andrews, G., Robinson, E., Schwencke, G., Johnston, L., Solley, K., & Choi, I. (2009). Clinician-assisted internet-based treatment is effective for Generalized Anxiety Disorder: Randomized controlled trial. Australian & New Zealand Journal of Psychiatry, 43(10),905-912. doi:10.1080/00048670903179269 [ Links ]
 Mailing address:
Mailing address:
André Luiz Moreno
Av. Dr. João Severiano Rodrigues da Cunha, 101
Uberaba, MG, Brazil 14048-900
Phone: (34) 9198-3998
E-mail: moreno.andreluiz@gmail.com, diogo.a.sousa@gmail.com, anamariaflps@gmail.com, gmanfro@gmail.com, gsallumjr@gmail.com, silvia.koller@gmail.com, flaviaosorio@ig.com.br and jcrippa@fmrp.usp.br
Recebido: 12/11/2014
1ª revisão: 15/12/2014
Aceite final: 17/03/2015


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}