










Serviços Personalizados
Journal

artigo
 Inglês (pdf)
Inglês (pdf)
 Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
Indicadores
Compartilhar

 Permalink
PermalinkJournal of Human Growth and Development
versão impressa ISSN 0104-1282
Rev. bras. crescimento desenvolv. hum. vol.24 no.1 São Paulo 2014
ORIGINAL RESEARCH
Auditory Late Responses in Asperger Syndrome: two case study
Ana Cláudia Bianco GuçãoI; Ana Carla Leite RomeroII; Vitor Engracia ValentiIII; Ana Cláudia Vieira CardosoIV; Andréa Regina Nunes MisquiattiV; Ana Claúdia Figueiredo FrizzoVI
IFonoaudióloga. Aluna regular do mestrado em Fonoaudiologia do Programa de Pós-Graduação da Faculdade de Filosofia e Ciências da Universidade Estadual Paulista - FFC/UNESP - Marília - SP/Brasil
IIFonoaudióloga. Aluna regular do mestrado em Fonoaudiologia do Programa de Pós-Graduação da Faculdade de Filosofia e Ciências da Universidade Estadual Paulista - FFC/UNESP - Marília - SP/Brasil
IIIFisioterapeuta. Docente do Departamento de Fonoaudiologia e do Programa de Pós-Graduação em Fonoaudiologia da Faculdade de Filosofia e Ciências da Universidade Estadual Paulista - FFC - UNESP - Marilia (SP), Brasil
IVFonoaudióloga. Docente do Departamento de Fonoaudiologia da Faculdade de Filosofia e Ciências da Universidade Estadual Paulista - FFC - UNESP - Marilia (SP), Brasil
VFonoaudióloga. Docente do Departamento de Fonoaudiologia da Faculdade de Filosofia e Ciências da Universidade Estadual Paulista - FFC - UNESP - Marilia (SP), Brasil
VIFonoaudióloga. Docente do Departamento de Fonoaudiologia e do Programa de Pós-Graduação em Fonoaudiologia da Faculdade de Filosofia e Ciências da Universidade Estadual Paulista - FFC - UNESP - Marilia (SP), Brasil
ABSTRACT
INTRODUCTION: Auditory Late Responses (ALR) assess central auditory processing by neuroelectric activity of the auditory pathway and analyse the activities involved in cortical abilities of discrimination, attention and integration of the brain. Individuals withAsperger Syndromeexperience changesinthese skills, so it is importanttoresearchthesepotentialthis population. The objective of this paper was to describe the auditory late responses of two patients with Asperger Syndrome.
METHODS: The study included two male patients with Asperger Syndrome, of 7 and 12 years of age, treated in a study centre. The patients did not present any auditory complaint detected by anamnesis. The external auditory canal was inspected and audiological and auditory late responses assessed. After evaluation the components P2, N2 and P3 were analysed.
RESULTS: In both patients, the latency of the components P2, N2 and P3 were elongated in both ears. Regarding the amplitude of the P2 component, reduced values were found for the left ear of patient 1 and the right ear of patient 2. The N2 amplitude was reduced for both ears of patient 1 and only the right ear of patient 2. The two patients showed a decrease in the amplitude of the P3 only in the right ear.
CONCLUSION: This study concludes that there were changes in the ALR results in both patients with Asperger Syndrome, suggesting alteration of the auditory function at the cortex level.
Key words: Asperger Syndrome, auditoryevoked responses, cognition.
INTRODUCTION
Auditory Late Responses (ALR) assess central auditory processing by neuroelectric activity of the auditory pathway in response to an acoustic stimulus or event. They analyse the activities involved in cortical abilities of discrimination, attention and integration of the brain,1 and disclose the integrity and ability of the central auditory nervous system.2
To generate these potentials it is necessary that the peripheral and central auditory system are intact, including the areas of the brain stem, sub-cortical routes, auditory cortex and corpus callosum, as well as areas of the frontal lobe and the temporo parieto occipital connection. The attention the individual gives to the stimulus is the main factor for definition of the potentials and it is useful in the investigation of cognitive functions and attention.1
ALR are recorded between 80 and 600 ms after stimulus presentation and are described as exogenous: N1 (negative wave with latency of approximately 80 to 150 ms and 5 to 10 µV of amplitude), P2 (positive wave with latency ranging from 145 to 200 ms and 3-6 µV of amplitude); and endogenous: N2 (negative wave range 180-250 ms and 3 to 6 µV of amplitude) and P3 (positive wave with latency of approximately 220-400 ms and the range of 8 to 15 µV of amplitude).1
ALR application has been conducted in individuals diagnosed with Asperger syndrome4-5 to confirm changes in attention and concentration tasks and solution of problems,6 support the diagnostic method and give focus to the encoding process of the sound characteristic.
Asperger Syndrome belongs to the Autism Spectrum Disorders (ASD)7 and individuals with it present failures in executive function,8 characterized as inflexible and rigid behaviour and difficulty in planning actions and controlling impulsive responses, which may interfere with the results of ALR. The frontal lobe, especially the prefrontal region, has been associated with these disorders.9
An ALR study5 performed in children with Asperger Syndrome has concluded that there are changes in the coding of a sound's transient characteristic, like sound discrimination. This indicates that the auditory sensory processing is impaired in these children and that such deficits may be related to perceptual problems presented by children with this syndrome.
ALR study is an objective method to assess hearing but is dependent on the attention and participation of the subject. Capturing the responses of central auditory processing in patients with Asperger Syndrome is a challenge to the evaluator, bearing in mind the changes in behaviour and attention span in these patients.
This study has hypothesized that individual with Asperger Syndrome show changes in attention and sound discrimination that justify consideration of an auditory processing impairment. Based on this hypothesis, the objective of this study was to investigate and describe the auditory late responses of two patients with Asperger Syndrome.
METHODS
This study was approved by the Ethics Committee of the Faculdade de Filosofia e Ciências - CEP / FFC / UNESP, process number 0486/2012.
The study was conducted at the Center for the Study of Education and Health (CEES) of the Faculdade de Filosofia e Ciências (FFC), Universidade Estadual Paulista (UNESP), Marilia.
The participants' legal guardians were informed about the methodological procedures and provided informed consent before the performance of any procedure.
Two patients with Asperger Syndrome participated in this study. They were diagnosed by an expert team composed of a neurologist, a psychiatrist, two psychologists and two speech therapists.
Characterization of the individuals in this study was performed by specialized professionals according to the diagnostic criteria established by DSM-IV10 and the Evaluation Scale of Autistic Traits (ATA) was applied.11 This instrument is composed of 23 subscales, each divided into different items. It was developed considering the diagnostic criteria of DSM-III, DSM-III-R and CID-10, and the authors' standardization also used the corrections of criteria that resulted from the publication of the DSM-IV. The Evaluation Scale of Autistic Traits11 is an easy tool to apply, the professional must know the clinical profile, not necessarily amedical professional, and however the physician is responsible for the answers ´evaluation according to each item11. It is not a diagnostic interview but a standardized test that indicates the profile of the child's behaviour, and it also assists in the drafting of a more reliable diagnosis.12 Its application is accomplished through interview with the parents, and the alternative answers are exemplified to facilitate their understanding, with an average time of scale application of 40 minutes.
The scale is scored based on the following criteria: each sub-scale test has a value from 0 to 2 and a score of zero is given if there is no presence of any items, 1 if there is only one item and 2 if there are more than one item. The points gained are added up and the cutoff is 23.11
The exclusion criteria were the presence of other associated impairments, such as biological, visual, and auditory complaints, audiological risk factors or hearing loss detected by specialized staff through anamneses with the legal guardian, inspection of the external ear canal, tympanometry and pure tone audiometry.
In both cases no audiological changes were detected. There were no auditory complaints in anamneses, tympanometry was normal and hearing sensitivity was within normal values.13
ALR investigation was carried out using Eclipse (Interacoustics), through software EP-25.
The patients were placed in a reclining chair and were asked to remain awake. The electrical impedance was below 5 kohms and the difference of the electrodes was 3 kohms.The acoustic stimulus used was the tone-burst at 80 dB HL at frequencies of 1000 Hz (frequent stimulus) and 2000Hz (rare stimulus), presented randomly by computer, with analysis window of 500ms, high-pass filters of 30Hz and low pass of 100 Hz, and a gain of 50000.The rare stimulus occurred in 20% of a total of 200 stimuli. Noninverting electrodes were placed on the vertex site (Fz), the inverting electrodes on the right and left mastoid (A1 and A2) and the ground electrode on the forehead, according to the 10-20 International System.
To obtain the ALR the individual was instructed to pay attention to rare stimuli (2000Hz) that appeared randomly within a series of frequent stimuli (1000Hz), and to lift the index finger every time the rare event occurred.
The individuals took a training session to ensure understanding of the test, and this training was monitored by two evaluators in order to avoid interference in the results. The evaluation was accompanied by the patient's therapist.
The latency and amplitude for the N2 and P3 components was analysed.
The normal parameters adopted for the analysis were based on studies that investigate the latency and amplitudeof the P2,14 N215 and P316 in typically developing children according to age. These studies found P2 component latencies of 157ms with a standard deviation of 47ms; the amplitude was in a range of 3-6mv. The N2 component latency was of 230ms with a standard deviation of 31ms; the amplitude was in a range of 5.77 mv with a standard deviation of 3.41mv. The P3 component latency was of 330ms with a standard deviation of 35ms; the amplitude was in a range of 10.35 mv and a standard deviation of 6.3mv.
RESULTS
Table 1 shows the characterization of the individuals related to age, sex, medical diagnosis, education and ATA scores.
It is observed that the two patients attend school and have a high enough ATA score to be diagnosed with autism spectrum disorder.
The following table shows the values of latency and amplitude of the P2, N2 and P3 components of the two individuals studied.
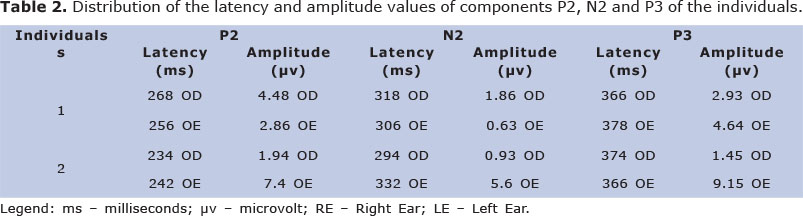
As can be seen, in both cases of Asperger Syndrome, the latency of the components P2, N2 and P3 was elongated in both ears when compared to literature values. The P2 amplitude was smaller for the left ear of individual number 1 and the right ear of individual number 2. The N2 amplitude observed was smaller for both ears of individual number 1 and the right ear of individual number 2. Both individuals had smaller P3 amplitude for the right ear.
DISCUSSION
The main finding of this study is the alteration of the auditory function at the cortex level in the two Asperger Syndrome individuals evaluated.
The literature emphasizes that there is controversy regarding the presence of abnormal cortical and subcortical trunks, consisting of known heterogeneity within and between diagnostic categories of autism spectrum disorder.17
The ALR reveal the functioning of the attention mechanism in the cortical portion, which justifies the significant number of studies in the literature on these mechanisms in children with Asperger Syndrome. The literature18 reports that the cognitive and attention deficits presented by these individuals are reflected in the P3 wave by elongated latency values, which indicate a possible deficit in cognitive processing; this characteristic was observed in this study.
The elongated latency values found in all components investigated in this study (P2, N2 and P3) infer changes in the auditory processing skills involving attention, discrimination and information storage.
Changes in the right ear are consistent with the idea that there is a deficit in neural transmission that causes abnormalities in auditory processing. These deficits are related to the recording and storage of information and to severe language alterations which these individuals can present in childhood.19
The elongation of the latency values found in the right and left ears, in both cases, may suggest a malfunction of the right20,21 and the left hemisphere.22,23
There is evidence that individuals with Asperger Syndrome have atypical brain development that results in changes in neural connections between the parts of the brain, which occur in a different way in the cerebral hemispheres.20
Other authors24 have observed significantly different activities in the cerebellar region, mesolimbic and temporal cortex in individuals with autism spectrum disorder and Asperger Syndrome through functional magnetic resonance, and have correlated this difference with neural development.Based on the observation made by the authors and the involvement of the temporal cortex in the auditory processing information, a possible correlation can be made between P300 alterations found and the abnormal brain activity displayed by the children with Asperger Syndrome.
The changes observed in this study are similar to the findings of other researchers4 who conducted ALR assessment in individuals with Asperger Syndrome and found a high occurrence of abnormal results in P3; the most common findings were elongated latency and decreased amplitude.
In this study it was observed that individuals showed abilateral decrease of the P3 amplitudes, confirming previous studies25,26 that infer abnormalities in the activation level of the cortex, which involves storage and information processing, in this population.
The analysis of the N2 component showed elongated latencies with decreased amplitudes in both patients,19,27 whichindicate a deficit in the stimulus discrimination and delayed time reaction to sound.
Regarding the P2 latency, it was elongated for both ears, and the amplitude was decreased for the left ear in individual number 1 and for the right ear in individual number 2.This component is often associated with the individual's attention to sound stimulus and inhibition of processing competitive stimuli. Thus, these findings indicate a possible central auditory processing dysfunction, suggesting deficits in attention and sound discrimination.Impairment in these skills could be observed in the necessity to repeat the instructions for the tests and in the difficulty that these individuals had in perceiving the rare stimulus.28-30
In addition, limitations and other important observations regarding the electrophysiological evaluation in children with Asperger Syndrome were noted.The presence of the child's therapist is required to favour a familiar environment, since the interaction between them is already established. The therapist favoured the patient interaction and collaboration in accomplishing the task proposed, the audiological and electrophysiological assessment. Schedule of a longer period of time for evaluations and the audiologist expertize were primordial to minimize the difficulty of the inter-personal relationship.
CONCLUSION
This study concludes that there were changes in the ALR in both individuals with Asperger Syndrome, suggesting alteration of the auditory function at the cortex level. However, further research in this area is necessary to provide more effective diagnosis and intervention in this population.
REFERENCES
1. Mcpherson DL. Late potentials of the auditory system. San Diego: Singular Publishing Group; 1996. [ Links ]
2. Schochat E, Matas CG, Sanches SGG, Carvallo RMM, Matas S. Central auditory evaluation in multiple sclerosis: case report.Arq Neuro-Psiquiatr. 2006; 64(3):872-76. [ Links ]
3. Pereira L, Cavadas M. Processamento auditivo central. In: Frota S. Fundamentos de fonoaudiologia: audiologia. Rio de Janeiro: Guanabara Koogan; 1998. p. 135-46. [ Links ]
4. Kujala T, Lepisto T, Nieminem-von Wendt T, Naatanen P, Naatanen R. Neurophysiological evidence for cortical discrimination impairment of prosody in Asperger syndrome. Neurosci Lett. 2005; 383(3):260-5. [ Links ]
5. Jansson-Verkasalo E, Ceponiene R, Kielinen M, Suominen K, Jantti V, Linna SL et al. Deficient auditory processing in children with Asperger Syndrome, as indexed by event-related potentials. Neurosci Lett. 2003; 338(3): 197-200. [ Links ]
6. Dias KZ. Processamento auditivo em indivíduos com síndrome de Asperger [tese]. São Paulo (SP): Universidade Federal de São Paulo; 2005. [ Links ]
7. Wing L. Asperger's Syndrome: a clinical account. Psychol Med. 1981; 11(1):115-29. [ Links ]
8. Barnard L, Muldoon K, Hasan R, O'Brien G, Stewart M. Profile executive dysfunction in adults with autism and comorbid learning disability. Autism. 2008; 12:125. [ Links ]
9. Rotta N, Ranzan J, Ohlweiler L, Soncini KN, Steiner S. Síndromes del hemisferio no dominante. Medicina. 2007; 67(6). [ Links ]
10. American Psychiatric Association. Diagnostic and statistical manual of mental disorders. Ed 4(DSM-IV). Washington DC, American Psychiatric Association; 1994. [ Links ]
11. Assumpção Jr FB, Baptista F, Gonçalves JDM, Cuccolichio S, Amorim LCD, Rego F et al. Escala de avaliação de traços autísticos (ATA): segundo estudo de validade. Med reabil. 2008; 27(2):41-4. [ Links ]
12. Brito MC, Misquiatti ARN. Iniciativas de comunicação na interação entre crianças com distúrbios do espectro autístico e suas mães: análise pragmática. Rev. CEFAC, São Paulo. 2011; 13(6). [ Links ]
13. Northen JL, Dows MP. Hearing in Children. Baltimore: Williams & Wilkins; 1984. [ Links ]
14. Kraus N, Mcgee, T. Potenciais auditivos de longa latência. In: Katz, J. Tratado de audiologia clínica. São Paulo: Manole; 1999. P. 403-20. [ Links ]
15. Duarte JL, Alvarenga KF, Banhara MR, Melo ADP, Sãs RM, Costa O. Potencial evocado auditivo de longa latência - P300 em indivíduos normais: valor do registro simultâneo em Fz e Cz. Rev. Bras. Otorrinolaringol. 2009; 75. [ Links ]
16. Brayner ICS. Aplicação do paradigma auditivo "oddball" no estudo do P300: normatização para faixa etária de 7-14 anos e avaliação de crianças com dificuldade de aprendizagem com e sem transtorno de déficit de atenção/hiperatividade. [Dissertação] Campinas (SP): Faculdade de Ciências Médicas, Universidade Estadual de Campinas; 2003. [ Links ]
17. Russo NM, Skoe E, Trommer B, Nicol T, Zecker S, Bradlow A, et al. Deficient brainstem encoding of pitch in children with autism spectrum disorders. Clin Neurophysiol. 2008; 119:1720-31. [ Links ]
18. Picton TW. The P300 wave of the human event-related potential. J Clin Neurophysiol. 1992; 9:456-79. [ Links ]
19. Novick B, Kurtzberg D, Vaughn HGJR. An Electrophysiologic indication of defective information storage in childhood autism. Psychiatr Res. 1979; 1:101-8. [ Links ]
20. Gage NM, Siegel B, Roberts TPL. Cortical auditory system maturational abnormalities in children with autism disorder: an MEG investigation. Dev Brain Res. 2003; 144: 201-9. [ Links ]
21. Herbert MR, Ziegler DA, Deutsch CK, O´Brien LM, Kennedy DN, Filipek PA, et al. Brain asymmetries in autism and developmental language disorder: a nested whole-brain analysis. Brain. 2005; 128(1):213-26. [ Links ]
22. Gomot M, Giard MH, Adrien JL, Barthelemy C, Bruneau N. Hypersensitivity to acoustic change in children with autism: electro-physiological evidence of left frontal cortex dysfunctioning. Psychophysiology. 2002; 39(5):577-84. [ Links ]
23. Escalante-Mead PR, Minshew NJ, Sweeney JA. Abnormal brain lateralization in highfunc-tioning autism. J Autism Dev Disord. 2003; 33(5):539-43. [ Links ]
24. Critchley HD, Daly EM, Phillips M, Brammer M, Bullmore E, Williams SC, et al. Explicit and implicit neural mechanisms for processing of social information from facial expressions. A functional magnetic resonance imaging study. Hum Brain Mapp. 2000; 9:93 - 105. [ Links ]
25. Lotspeich LJ, Ciaranello RD. The neurobiology and genetics of infantile autism. Int Rev Neurobiol. 1993; 35:87-129. [ Links ]
26. Courchesne E. A neurophysiological view of autism. In: Schopler E, Mesibov GB, editors. Neurological issues in autism. New York: Plenum Press; 1987. [ Links ]
27. Orekhova EV, Stroganova TA, Prokofyev AO, Nygren G, Gillberg C, Elam M. Sensorygating in young children with autism: relation to age, IQ, and EEG gammaoscillations. Neurosci Lett. 2008; 434:218 - 23. [ Links ]
28. Hansen JC, Hillyard SA. Temporal dynamics of human auditory selective attention. Psychophysiology. 1988; 25:316 - 29. [ Links ]
29. Oades RD, Dittmann-Balcar A, Schepker R, Eggers C, Zerbin D. Auditory event-related potentials (ERPs) and mismatch negativity (MMN) in healthy children and those with attention-deficit or tourette/tic symptoms. Biol psychol. 1996; 12:163-85. [ Links ]
30. Silva EB, Filipini R, Monteiro CB, Valenti VE, de Carvalho SM, Wajnsztejn R, de Farias Mdo C, Macedo CC, de Abreu LC. The biopsy-chosocial processes in autism spectrum disorder. Int Arch Med. 2013;6(1):22. [ Links ]
Manuscript submitted Aug 01 2013
Accepted for publication Dec 28 2013
Corresponding author: anafrizzo@marilia.unesp.br

{kind=link}