










Serviços Personalizados
Journal

artigo
 Inglês (pdf)
Inglês (pdf)
 Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
Indicadores
Compartilhar

 Permalink
PermalinkPsicologia Clínica
versão impressa ISSN 0103-5665versão On-line ISSN 1980-5438
Psicol. clin. vol.34 no.1 Rio de Janeiro jan./abr. 2022
https://doi.org/10.33208/PC1980-5438v0034n01A01
THEMATIC SECTION - SOCIAL DYNAMICS AND PSYCHOLOGY: COGNITION, FAMILY, TRAUMA AND TECHNOLOGICAL INNOVATION IN RELATIONSHIPS AND TREATMENTS
Does self-compassion mediate the relation between perfectionism and psychopathological outcomes?
A autocompaixão medeia a relação entre perfeccionismo e desfechos psicopatológicos?
¿La autocompasión media la relación entre el perfeccionismo y los resultados psicopatológicos?
Luiz Fellipe Dias da RochaI; Eliane Mary de Oliveira FalconeII; José Augusto Evangelho HernandezIII
IMestre em Psicologia Social pela Universidade do Estado do Rio de Janeiro (UERJ), doutorando em Psicologia Social pela Universidade do Estado do Rio de Janeiro (PPGPS/UERJ), Rio de Janeiro, RJ, Brasil. email: luiz.rocha@uerj.br
IIDoutora em Psicologia Clínica pela Universidade de São Paulo (USP). Professora do Programa de Pós-Graduação em Psicologia Social da Universidade do Estado do Rio de Janeiro (PPGPS/UERJ), Rio de Janeiro, RJ, Brasil. email: elianefalcone@uol.com.br
IIIDoutor em Psicologia pela Universidade Federal do Rio Grande do Sul (UFRGS), Professor do Programa de Pós-Graduação em Psicologia Social da Universidade do Estado do Rio de Janeiro (PPGPS/UERJ), Rio de Janeiro, RJ, Brasil. email: hernandez.uerj@gmail.com
ABSTRACT
This research aims to investigate the mediating role of self-compassion in the relationship between perfectionism and psychopathological outcomes. The sample was composed of 175 Brazilian undergraduate students, aged from 18 to 59 years old (M=25.97, SD=8.2). The participants filled out three self-report psychometric instruments: Clinical Perfectionism Questionnaire with only positive items, Self-Compassion Scale - Short Form (SCS-SF), and Depression, Anxiety and Stress Scales - Short Form (DASS-21). Preliminary correlations confirmed that the investigated variables were significantly correlated with one another. Subsequently, two simple mediation model analyses were run, and results supported a partial mediation of self-compassion between the two dimensions of perfectionism (i.e., perfectionistic strivings and perfectionistic concerns) and the global factor of DASS-21 (i.e., negative affectivity), separately. A serial multiple mediator model was also performed, and results demonstrated that, together, self-compassion and perfectionistic concerns fully mediated the relationship between perfectionistic strivings and negative affectivity. These findings are consistent with the possibility that self-compassion and perfectionistic concerns are underlying processes through which perfectionistic strivings may result in psychopathological outcomes.
Keywords: perfectionism; self-compassion; psychopathology; path analysis; multiple regression.
RESUMO
Esta pesquisa tem como objetivo investigar o papel mediador da autocompaixão na relação entre perfeccionismo e desfechos psicopatológicos. A amostra foi composta por 175 estudantes brasileiros de graduação, com idades entre 18 e 59 anos (M=25,97; DP=8,2). Os participantes preencheram três instrumentos psicométricos de autorrelato: Clinical Perfectionism Questionnaire apenas com itens positivos, Self-Compassion Scale - Short Form (SCS-SF), e Depression, Anxiety and Stress Scales - Short Form (DASS-21). Correlações preliminares confirmaram que as variáveis investigadas estavam significativamente correlacionadas entre si. Posteriormente, duas análises de modelo de mediação simples foram executadas e os resultados apoiaram uma mediação parcial da autocompaixão entre as duas dimensões do perfeccionismo (i.e., esforços perfeccionistas e preocupações perfeccionistas) e o fator global de DASS-21 (i.e., afetividade negativa), separadamente. Um modelo serial de mediadores múltiplos também foi realizado e os resultados demonstraram que, juntas, a autocompaixão e as preocupações perfeccionistas mediaram totalmente a relação entre os esforços perfeccionistas e a afetividade negativa. Essas descobertas são consistentes com a possibilidade de que a autocompaixão e as preocupações perfeccionistas sejam processos por meio dos quais os esforços perfeccionistas resultam em desfechos psicopatológicos.
Palavras-chave: perfeccionismo; autocompaixão; psicopatologia; análise de caminhos; regressão múltipla.
RESUMEN
Esta investigación tiene como objetivo investigar el papel mediador de la autocompasión en la relación entre el perfeccionismo y los resultados psicopatológicos. La muestra estuvo constituida por 175 estudiantes brasileños de pregrado, con edades entre 18 y 59 años (M=25,97; DE=8,2). Los participantes completaron tres instrumentos psicométricos de autoinforme: Clinical Perfectionism Questionnaire solo con elementos positivos, Self-Compassion Scale - Short Form (SCS-SF), y Depression, Anxiety and Stress Scales - Short Form (DASS-21). Las correlaciones preliminares confirmaron que las variables investigadas se correlacionaron significativamente entre sí. Posteriormente, se realizaron dos análisis de modelos de mediación simple y los resultados apoyaron una mediación parcial de la autocompasión entre las dos dimensiones del perfeccionismo (i.e., esfuerzos perfeccionistas y preocupaciones perfeccionistas) y el factor global de DASS-21 (i.e., afectividad negativa), por separado. También se realizó un modelo serial de múltiples mediadores y los resultados mostraron que, en conjunto, la autocompasión y las preocupaciones perfeccionistas mediaron por completo la relación entre los esfuerzos perfeccionistas y la afectividad negativa. Estos hallazgos son consistentes con la posibilidad de que la autocompasión y las preocupaciones perfeccionistas sean procesos a través de los cuales los esfuerzos perfeccionistas dan como resultado consecuencias psicopatológicas.
Palabras clave: perfeccionismo; autocompasión; psicopatología; análisis de ruta; regresión múltiple.
Introduction
Perfectionism might be defined as a personality trait characterized by setting high personal demanding standards and striving for flawlessness (Stoeber, 2020). So, perfectionists have rigorous criteria to define their success, and strive to reach their high standards and to avoid failures - or what they deem to be failures.
Although initial conceptualizations considered perfectionism as unidimensional, studies that investigated the latent structure of different self-report measures have indicated the hegemonic presence of two correlated dimensions, frequently called Perfectionistic Strivings (PS) and Perfectionistic Concerns (PC) (see Stoeber, 2018a, for a review). PS dimension embraces cognitions and behaviors of setting high personal demanding standards and pursuing them, whereas PC dimension includes cognitions and behaviors related to imperfections and their feared consequences (Stoeber, 2018a, 2020).
From a behavioral perspective, the two dimensions of perfectionism can be differentiated based on their functions: PS would include perfectionist components due to positive reinforcement, while PC would include perfectionist components due to negative reinforcement (Terry-Short et al., 1995). In other words, the PS dimension is related to positive control (i.e., it involves cognitions and behaviors that aim to achieve positive consequences) and the PC dimension is more related to aversive control (i.e., it involves cognitions and behaviors that aim to avoid or to escape from adverse consequences). Therefore, it could be said that PS are driven by motivation for perfection and PC are driven by fear of failure (Slade & Owens, 1998).
The number of publications about perfectionism increased significantly in the last three decades (see Smith et al., 2022). The interest in perfectionism has grown mainly because this variable has been highlighted as a transdiagnostic process, that is, a set of cognitive or behavioral aspects that perform an important role in the etiology, maintenance, and course of several psychopathological states (Egan et al., 2011; Egan et al., 2014; Shafran et al., 2002). Generally, the two dimensions of perfectionism are positively associated with psychopathological indicators, although the PC dimension has a higher association, compared to the PS dimension, especially when the overlap between them is under control (Limburg et al., 2016; Smith et al., 2016).
A meta-analysis performed with 284 empirical studies - mostly cross-sectional ones - revealed that both perfectionistic dimensions were positively correlated to psychopathological outcomes (i.e., mental disorders, symptoms of mental disorders and outcomes related to psychopathology, as suicidal ideation and general psychological distress) (Limburg et al., 2016). It means that the higher the levels of PS and PC, the higher the levels of psychological maladjustment indicators. Nevertheless, single effect values of PC have shown to be superior to those of PS, after these dimensions' overlap control (b≤0.70 and b≤0.25, respectively).
Similar results have been found by another meta-analysis that investigated the longitudinal relation between perfectionism and depression symptoms in 10 studies with different samples (Smith et al., 2016). After the depression symptoms control at the baseline, both PS and PC revealed a little effect over depression symptoms throughout time. However, after the PC control at the baseline, the PS dimension no longer predicted depression symptoms longitudinally.
Aiming for a better understanding of this relationship, research has been conducted in order to verify mediators between perfectionism and psychopathological indicators. Research on mediators examines "how" or "why" a variable predicts an outcome variable (Frazier et al., 2004). So, mediator variables could partially or totally explain the relation between perfectionism and psychopathological outcomes, indicating the ways in which one predicts the other (Stoeber, 2018b).
As may be seen, the identification of mediators can provide a better understanding of the underlying processes between perfectionism and psychopathology. This information can enable the construction and testing of theories about the causal mechanisms responsible for change, as well as indicate the core components of treatment (Frazier et al., 2004).
Among the variables found as mediators of the relationship between perfectionism and psychopathology, self-compassion is highlighted. Self-compassion can be defined as a sensitivity to one's own pain, along with a commitment to relieve or prevent it (Irons & Beaumont, 2017). According to Neff (2003), self-compassion involves a kind and tender way to relate to oneself, especially under suffering and tough circumstances, involving the acceptance of hurtful emotional experiences, along with the comprehension that they are part of a bigger human experience.
As it may be observed, there are three components involved in the conceptualization of self-compassion: self-kindness (versus self-judgment), mindfulness (versus over-identification), and common humanity (versus isolation) (Neff & Germer, 2019; Souza & Hutz, 2016). Self-kindness refers to love, support, acceptance, and encouragement actions towards oneself, instead of judging or blaming, mainly when faced with feelings of personal inadequacy, failures, and painful life situations. Mindfulness, in self-compassion, involves awareness of one's own suffering, mistakes, flaws, or inadequacies, without being absorbed by it, exaggerating it, or dedicating the whole self to it. Common humanity refers to the sense of interconnectivity, perceiving problems and struggles as difficulties that occur in everyone's life, instead of being an isolated situation, as if the person was apart from the rest of the world. In a nutshell, self-compassion means a loving (self-kindness) and connected (common humanity) presence (mindfulness).
In general, perfectionism tends to be negatively associated with self-compassion, that is, the higher the level of perfectionist dimensions, especially PC, the lower the level of self-compassion (Barnett & Sharp, 2016; Mehr & Adams, 2016; Neff, 2003; Stoeber et al., 2020). Since the Self-Compassion Scale (Neff, 2003), used in these studies, measures both positive and negative components of self-compassion, it could be said that perfectionists are self-critical, feel isolated and easily become over-identified with negative emotions and thoughts, instead of being self-compassionate.
In turn, self-compassion showed a negative correlation with psychopathology outcomes; in other words, the lower the level of self-compassion, the higher the level of mental health symptoms (see MacBeth & Gumley, 2012, for a review). Thus, the criteria for investigating the mediating role are established, that is, all variables involved must be significantly correlated (Frazier et al., 2004). Namely, perfectionism (predictor or antecedent) is positively associated with psychopathology (outcome or consequent) and self-compassion (mediator), while self-compassion is inversely associated with psychopathology. Lastly, to affirm that self-compassion is a mediating variable, it is necessary to show that, when it is added to the model, the strength of the relation between the perfectionism and psychopathology is significantly reduced. Some studies have investigated this.
In a sample of 358 undergraduate students from the United States, the association between PC, measured by Almost Perfect Scale - Revised (APS-R), and depressive symptom reduced from b=.423 (p<.001) to b=.324 (p<.001) after controlling for the mediator of self-compassion (Mehr & Adams, 2016). Since the strength of the association between predictor and outcome was reduced after the introduction of self-compassion, but was not zero or non-significant, there was support for the hypothesis that self-compassion partially mediated the effect of PC dimension on depressive symptoms. In a different study, using a sample composed of 77 undergraduate students from Ireland, the association between PC measured by APS-R and anxiety symptoms was no longer significant after controlling for self-compassion, indicating a full mediation effect (Murtagh, 2018).
In a third study, with a sample of the general population, mostly undergraduate students from Canada and the USA, the scores of self-compassion were merged with the scores of other variables (e.g., rumination and mindfulness) through principal components analysis, and a global factor emerged, which was called self-criticism by the authors (James et al., 2015). Self-criticism partially mediated the association between PC dimension, measured by Frost multidimensional perfectionism (FMPS), and the global factor of Depression, Anxiety and Stress Scales (DASS-21). After controlling for the mediator of self-compassion, the association between PC and the global factor of DASS-21 was b=.38 (p<.01).
Gilbert (2009, 2016), inspired by the affective neuroscience of evolution, describes three types of primary systems of emotional regulation (also called motivational systems) that operate in humankind and might help in understanding the relation between perfectionism, self-compassion and psychopathological outcomes. The drive, seeking and acquisition focused system (or just drive system) has as its function to motivate the pursuit of resources and rewards, guiding the development of desires and goals. The threat and self-protection focused system (or just threat system) enables the individual to be alert and to quickly respond to threats, motivating security response in the face of real or imaginary danger stimuli. The contentment, soothing focused system (or just soothing system) enables a state of contentment, peacefulness, and safeness when the individual is not seeking resources or threat-focused.
It is possible to observe similarities between the drive system and the PS dimension, since these could denote a mindset oriented to objectives that motivate people to pursue their high standards. On the other hand, PC is similar to the threat system, since this dimension may be seen as a mindset that tries to avoid failures or imperfections and their negative consequences. Thus, it would be possible to hypothesize that the PS dimension is related to the activation of the drive system, while the PC dimension is related to the activation of the threat system.
Even though the threat system has a primordially adaptive function, a lot of problems connected to mental health are related to it, especially if it is overdeveloped, sensitive, biased, or confused (Gilbert, 2009). In general, the threat system is more related to psychopathology due to the processes involved in its activation, such as neurohormonal mechanisms (e.g., cortisol response), negative emotions or emotional states (e.g., stress, fear, anxiety, and anger), biased cognitive processing (e.g., hypervigilance and worry) and often dysfunctional security strategies (e.g., avoidance) (Gilbert, 2016; Irons & Beaumont, 2017). This may explain why the PC dimension has a higher association with psychopathological indicators compared to the PS dimension.
Nevertheless, the drive and threat systems interact in a way that the search for resources might be connected to the attempt to fight against threats or to avoid them, designing a safety-seeking strategy to negative events (e.g., pursuing high standards to avoid inferiority feelings) (Gilbert, 2016). At the same time, thwarting the drive system (e.g., when the goals are not reached) tends to trigger the activation of the threat system, creating a negative emotional response (Gilbert, 2009). This may partially explain why the association between PS and psychopathological outcomes is reduced when PC is under control.
The soothing system, in its turn, helps to balance the other two systems through the activation of the parasympathetic system, being a source of well-being, peacefulness and contentment. This system was shaped by evolution to be activated by attachment behaviors (e.g., nutrition, validation, empathy, and compassion), since it brought benefits for the species, such as offspring survival and developing helpful alliances and friendships (Gilbert, 2009). One way to boost the activation of the soothing system is through self-compassion, a way of caring directed at oneself.
As can be seen, (low) self-compassion may be one of the mechanisms through which perfectionism affects psychopathology (James et al., 2015; Mehr & Adams, 2016; Murtagh, 2018), and this is coherent from a theoretical point of view on primary systems of emotional regulation (Gilbert, 2009, 2016). However, empirical studies of mediation tend to focus on the PC dimension and neglect the PS dimension. Moreover, no studies with that aim were found with Brazilian samples. Therefore, this study aims to investigate the mediating role of self-compassion in the relationship between perfectionism, including its two dimensions, and psychopathological outcomes among Brazilians.
The hypothesis to be tested is that self-compassion is a significant mediator in this relationship, at least partially explaining the negative effect of perfectionism. If this is corroborated, the results will indicate that individuals with high levels of perfectionism (especially PC) tend to treat themselves with little (or no) self-compassion, and this partially explains the level of psychopathological symptoms experienced by them. Thus, interventions aimed at reducing perfectionism, in order to reduce psychopathology, must take into account the promotion of self-compassion.
Another hypothesis to be tested is that PC also mediates the relations between PS and psychopathology, since the individual may pursue high personal demanding standards, trying to prevent or stop the feared consequences related to imperfections and that not reaching high standards can evoke the threat system. In other words, PS predicts psychopathological outcomes due to high levels of PC (combined with low levels of self-compassion). If this is corroborated, PS cognitions and behaviors may, in some cases, configure safety-seeking strategies and must be faced by interventions within that context. Besides that, interventions could also help perfectionists to develop more functional ways to manage failures and mistakes (i.e., by thwarting PS).
Method
Participants
In this study, 175 Brazilian undergraduate students took part, with ages from 18 to 59 years old (M=25.97, SD=8.2), 86.3% being female (n=151) and 13.4%, male (n=23). One participant did not report sex, but gender (non-binary). Regarding marital status, 76% declared to be single (n=133), 20.57% married or in common-law marriage (n=36), and 3.4% divorced or separated (n=6).
Instruments
Clinical Perfectionism Questionnaire with only positive items (CPQ+), adapted by Rocha, Hernandez, and Falcone (in press), based on CPQ of Fairburn et al. (2003), was applied. CPQ+ is composed of 12 items that examine the frequency of some behaviors and cognitions related to perfectionism in the previous 30 days. The respondent must indicate the answer through a Likert-type scale from 1 (not at all) to 4 (all of the time). Items 1, 3, 6, 7, 9, 10, and 11 measure PS, and items 2, 4, 5, and 12 measure PC. Item 8 is removed due to simultaneous saturation in both factors of CPQ+. Composite reliability of PS was .78 and that of PC, .75; Cronbach's alpha were .79 and .74, respectively (Rocha et al., in press).
To measure self-compassion, the Self-Compassion Scale - Short Form (SCS-SF), devised by Raes et al. (2011), was applied. SCS-SF is made up of 12 items out of 26 in the long form SCS (items 6*, 26, 14, 13*, 15, 12, 9, 25*, 2*, 10, 1*, and 11* - items followed by * are reversed), in which the participants are instructed to indicate, in a scale from 1 (almost never) to 5 (almost always), how often they act in the given manner. In this study, SCS-SF was applied using the wording of the items in the long form SCS adapted for Brazilian samples by Souza and Hutz (2016). The items measure the six components of self-compassion construct (self-kindness, mindfulness, common humanity, self-judgment, over-identification, and isolation); however, the global factor is predominant. In the validity study, SCS-SF demonstrated adequate internal consistency (Cronbach's alpha ≥0.86) and a near-perfect correlation with the long form SCS (r≥0.97).
To measure psychopathological outcomes, the Depression, Anxiety and Stress Scales - Short Form (DASS-21) by Lovibond and Lovibond (1995), adapted to Brazilian population by Vignola and Tucci (2014), were applied. This self-report instrument is composed of 21 items that measure depression, anxiety, and stress symptoms. The respondents must indicate how much each item was related to their reality in the previous week. Answers are given in Likert-type scale, from "Did not apply at all" (0) to "Applied a lot or most of the time" (3). Although specific factors (e.g., depression, anxiety, and stress) are present, the measure is predominantly unidimensional (Zanon et al., 2020). In a Brazilian sample, the Cronbach's alpha of the global factor was .94, and composite reliability was .96 (Rocha et al., 2021). The global factor of DASS-21 will be named negative affectivity here, but it is also called general distress, general affective distress, negative affective distress, and general negative affectivity in other studies.
Procedures
After approval of the project by the Ethics in Research Committee of the institution to which this study is attached, an online questionnaire was created through Google Forms, containing the Written Informed Consent Form (WICF) and the research instruments. The invitation to participate in the project was made through social media (e.g., Facebook) and e-mails to university professors, requesting them to forward the form link to their students. The form was available for completion between August 2020 and September 2020. The mandatory responses feature was used for all items, which prevented the form being returned with missing values.
Data analysis
All data collected in this study were recorded on a computer and processed using the statistical software SPSS (version 23). Firstly, descriptive statistical analysis was performed to understand how the collected data was distributed. Internal consistency indicators for the instruments were also generated.
Since studies investigating the factorial structure of SCS-SF with Brazilian samples were not found, the Factor software (version 10.10.03) was employed, in order to perform an Exploratory Factor Analysis (EFA). A Robust Diagonally Weighted Least Squares (RDWLS) extraction method was applied, with Robust Promin rotation over a polychoric correlation matrix. The decision about the number of factors to be retained was made through Parallel Analysis, with random permutation of observed data (Timmerman & Lorenzo-Seva, 2011).
The relationship between all variables was examined by computing the Pearson's product moment correlation coefficient. To meet the assumptions necessary for mediation analysis, it is necessary for the antecedents (PS and PC) to be associated with the consequent (negative affectivity) and mediator (self-compassion), while the mediator is associated with the consequent (Frazier et al., 2004).
To test our hypothesis concerning the mediating role of self-compassion in the relationship between perfectionism and negative affectivity, mediator models were used. For this, multiple regression analysis was applied through the PROCESS macro for SPSS, according to procedures described by Hayes (2018). Standardized coefficients were used. The Bias-Corrected and Accelerated confidence interval (BCa) was estimated using the Bootstrapping technique (5000 resampling), and a 95% bias-corrected bootstrap confidence interval (CI) for the indirect effect was also reported.
Results
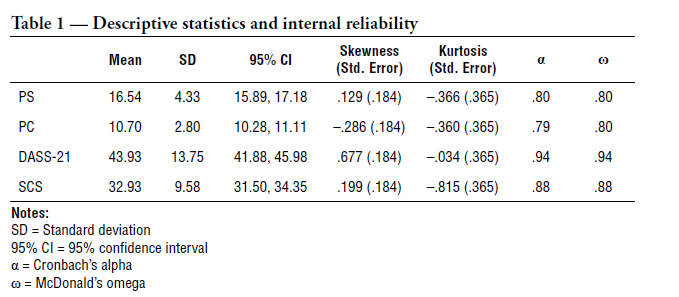
Results related to data distribution, as well as internal reliability indicators, can be found in Table 1. Regarding the factor analysis of SCS-SF, Kaiser-Meyer-Olkin (KMO) measure exhibited an index of .87 and Bartlett's sphericity test of χ2 (66)=1035.7, p<.001, both indicating the suitability of the data for structure detection. Parallel Analysis recommended an extraction of one factor, in which all 12 items loaded substantially (loading ≥.53).
Regarding the correlations, all variables presented a statically significant association with each other. According to Evans' (1996) guide for interpreting the strength of correlation coefficients, PS dimension presented a weak positive correlation with negative affectivity (r=.33) and a weak negative correlation with self-compassion (r=-.31). PC dimension presented a moderate positive correlation with negative affectivity (r=.53) and a moderate negative correlation with self-compassion (r=-.57). Self-compassion, in its turn, presented a strong negative correlation with negative affectivity (r=-.65). Lastly, PS dimension presented a moderate positive correlation with PC dimension (r=.53). All the correlations were significant at the .01 level. Therefore, the assumptions for mediation analysis were met.
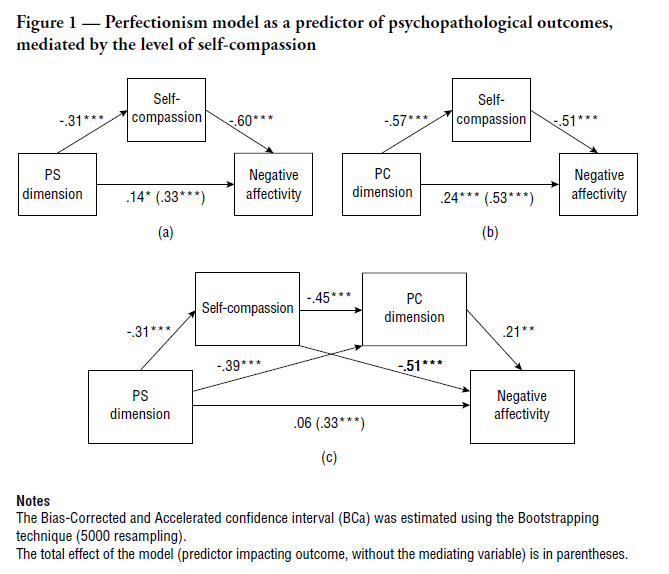
Regarding mediation analyses, we firstly sought to investigate the extent to which self-compassion (M) mediated the relationship between PS (X) and negative affectivity (Y), though a simple mediation model. As can be seen in Figure 1(a), the impact of PS was significant for self-compassion (b=-.31, t=-4.3345, SE=.1597, p<.0001, R2=.098). Self-compassion (the mediating variable) had a statistically significant effect on negative affectivity (b=-.60, t=-9.9769, SE=.0865, p<.001). PS impacted negative affectivity, controlled by self-compassion (b=.14, t=2.3972, SE=.1914, p<.05). The total effect of the model (PS impacting negative affectivity, without the mediating variable) was b=.33, t=4.6390, SE=.2277, p<.001, R2=.11 (11%). The mediation effect (i.e., indirect effect) was significant (b=.19 [95% BCa CI=.10, .27]). Self-compassion mediated approximately 57.6% of the relationship between PS and negative affectivity. Therefore, it can be said that self-compassion partially mediates the relationship between PS and negative affectivity.
Then, we sought to investigate the extent to which self-compassion (M) mediated the relationship between PC (X) and negative affectivity (Y), through another simple mediation model. As can be seen in Figure 1(b), the impact of PC was significant for self-compassion (b=-.57, t=-9.1629, SE=.2139, p<.0001, R2=.33). Self-compassion had a statistically significant effect on negative affectivity (b=-.51, t=-7.4281, SE=.0983, p<.001). PC impacted negative affectivity, controlled by self-compassion (b=.24, t=3.5176, SE=.3372, p<.001). The total effect of the model (PC impacting negative affectivity, without the mediating variable) was b=.53, t=8.2567, SE=.3171, p<.001, R2=.28 (28%). The mediation effect (i.e., indirect effect) was significant (b=.29 [95% BCa CI=.21, .38]). Self-compassion mediated approximately 54.7% of the relationship between PC and negative affectivity. Therefore, it can be said that self-compassion partially mediates the relationship between PC and negative affectivity.
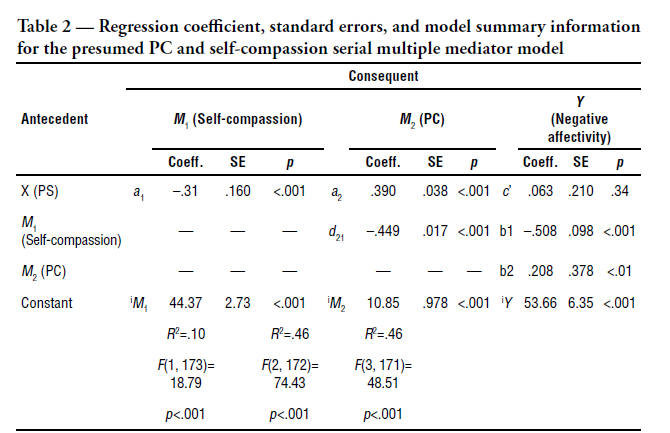
Whereas self-compassion partially mediates the relations between PS and negative affectivity, and the strength of the association between PS and psychopathological outcomes tends to decrease after controlling for PC, a serial multiple mediator model was performed, with PS (X) as a predictor, and self-compassion (M1) and PC (M2) as mediating variables (Table 2). As can be seen in Figure 1(c), PS ceased to significantly impact negative affectivity, after controlling for self-compassion and PC (b=.06, t=9.564, SE=.2103, p>.05). The mediation effect (i.e., indirect effect) was significant (b=.27 [95% BCa CI=.16, .37]). Therefore, it can be said that, together, self-compassion and PC fully mediate the relationship between PS and negative affectivity.
Discussion
The present study aimed to investigate the mediating role of self-compassion in the relation between perfectionism and psychopathological outcomes. The results of the correlations are consistent with previous research demonstrating that higher levels of the two dimensions of perfectionism, especially PC, are related to higher levels of psychopathology (Limburg et al., 2016; Smith et al., 2016), and consistent with previous findings on self-compassion, which suggest that it is negatively correlated with psychopathological symptoms (MacBeth & Gumley, 2012). Moreover, the higher the levels of perfectionist dimensions, the lower the level of self-compassion, corroborating the results found by other studies (Barnett & Sharp, 2016; Mehr & Adams, 2016; Neff, 2003; Stoeber et al., 2020).
In addition to providing additional evidence for these previously identified relations, the current study examined self-compassion as a mediator of the two dimensions of perfectionism and negative affectivity. Our hypothesis that self-compassion would mediate the relationship between PS and negative affectivity was supported by the results, which indicated partial mediation, that is, self-compassion explained approximately 57.6% of the relationship. Self-compassion also partially mediated the relationship between PC and negative affectivity, which explained approximately 54.7% of the relationship.
Other studies had already indicated that self-compassion might be one mechanism through which PC affect psychopathological outcomes (James et al., 2015; Mehr & Adams, 2016; Murtagh, 2018). The present study adds evidence in this regard using a Brazilian sample, in addition to demonstrating that self-compassion is also one of the mechanisms through which PS predicts psychopathological outcomes. Thus, it could be said that individuals with high levels of perfectionist dimensions tend to treat themselves with little self-compassion and this partially explains the level of psychopathological symptoms experienced by them.
As proposed by Gilbert (2009), seeking resources and rewards (e.g., high standards) and responding to threats (e.g., fear of failure) generate psychopathological symptoms partially due to low activation of the soothing system (i.e., low levels of self-compassion). Distress arises when drive and threat systems get out of balance with the soothing system and it is not working or accessible. So, the soothing system could help to regulate the excessive need/want feelings and the threat-based emotions (Gilbert, 2009).
In practical terms, these results may indicate that interventions aimed at reducing perfectionism, in order to reduce psychopathology, must consider the promotion of self-compassion, in addition to helping the subject to establish more flexible goals, and to have a more realistic view of the consequences of failures (Egan et al., 2014; Shafran et al., 2018). In other words, it is important that interventions help perfectionists to increase a loving (self-kindness) and connected (common humanity) presence (mindfulness), instead of being self-critical, feeling isolated and becoming over-identified with negative emotions and thoughts.
Besides assessing the two simple mediation models (i.e., self-compassion mediating the effect of PS and PC, separately, on psychopathological outcomes), this study also checked whether self-compassion and PC together mediate the relationship between PS and negative affectivity, through a serial multiple-mediator model. The results of this analysis indicated that after controlling the levels of self-compassion and PC, PS no longer predicted the level of negative affectivity.
Theoretically, it could be said that the drive system, when balanced with threat and soothing systems, does not present a risk for the development of psychopathological symptoms (Gilbert, 2009; Irons & Beaumont, 2017). Thus, pursuing high standards (i.e., PS) is dangerous when individuals do that to prevent or stop the feared consequences related to imperfections, as a safety-seeking strategy, and because thwarting the search for high standards can provoke the activation of the threat system (e.g., through PC).
Additionally, perfectionists may become obsessed with pursuing their high standards, blocking the activation of the soothing system (e.g., through self-compassion). That is, an over-stimulated drive system makes it difficult to reduce the rhythm a little, through the parasympathetic system activation, to be present in the moment (i.e., mindfulness), to offer unconditional acceptance to oneself (i.e., self-kindness) and to be connected with other people (i.e., common humanity). In summary, "[…] what desires we have, the purpose of them, how we set about trying to satisfy them and how we feel and treat ourselves if we don't get what we want or think we need - are all important to our well-being" (Gilbert, 2009, p. 159).
These results may have some practical implications. Firstly, interventions should probe whether cognitions and behaviors related to pursuing high personal demanding standards are being used as a form of protection against feared consequences (i.e., as safety-seeking strategies). Cognitive models have pointed to the trap of such strategies, since, although it reduces fear or anxiety in the short term, it also prevents longer-term cognitive change and an accurate perception of the threat (Irons & Beaumont, 2017; Thwaites & Freeston, 2005). In the case of PS as a safety strategy, perfectionists will continue to believe, for example, that they are not a failure as a person just because they reached extremely high standards. Therefore, treatments should focus on gradually dismantling these strategies and helping perfectionists to create opportunities to test their beliefs.
Furthermore, it is important that interventions help perfectionists to develop functional strategies to use when things do not go according to plan, since the thwarting of the drive system tends to provoke the activation of the threat system, generally focused on the self, creating a negative emotional response (Gilbert, 2009). For instance, not reaching high standards tends to awaken negative beliefs, such as 'I am inadequate', which, in its turn, will lead to the experience of negative affectivity (Neff & Germer, 2019). So, it is important that perfectionists learn to identify and correct cognitive distortions as one of the possible strategies to cope with life's setbacks (Shafran et al., 2018).
Finally, another practical implication is the possibility of helping the perfectionist to slow down, offering self-compassion to themselves and providing moments of relaxation, so that they can continue the search for high standards in a healthy way. Pursuing high standards can become somewhat addictive, and self-compassion can help perfectionists find a more balanced life regarding the search of pleasures through the activation of the drive system versus experiencing contentment through the activation of the soothing system (Gilbert, 2009).
Although the present study may contribute to a better understanding of the underlying processes between perfectionism and psychopathology, it has limitations regarding to representativeness and generalizability. The sample employed does not represent the Brazilian population, making it difficult to extrapolate results. Moreover, this study used a sample of undergraduates, as do most related studies, making it important to have further research done with clinical samples. Lastly, the cross-sectional design prevents inference regarding causes, as it fails to address directionality or temporal precedence. Future studies may adopt multi-wave longitudinal design, with, at least, three measurement points (i.e., predictor in the first time, mediators in the second, and outcomes in the third), and experimental design, comparing the effectiveness of interventions that include the promotion of self-compassion, those that do not include such promotion, and of no intervention (as a control group) on the reduction of perfectionism and psychopathological outcomes.
References
Barnett, M. D.; Sharp, K. J. (2016). Maladaptive perfectionism, body image satisfaction, and disordered eating behaviors among U.S. college women: The mediating role of self-compassion. Personality and Individual Differences, 99, 225-234. https://doi.org/10.1016/j.paid.2016.05.004 [ Links ]
Egan, S. J.; Wade, T. D.; Shafran, R. (2011). Perfectionism as a transdiagnostic process: A clinical review. Clinical Psychology Review, 31(2), 203-212. https://doi.org/10.1016/j.cpr.2010.04.009 [ Links ]
Egan, S. J.; Wade, T. D.; Shafran, R.; Antony, M. M. (2014). Cognitive-behavioral treatment of perfectionism. New York: Guilford. [ Links ]
Evans, J. D. (1996). Straightforward statistics for the behavioral sciences. Pacific Grove: Brooks/Cole. [ Links ]
Fairburn, C. G.; Cooper, Z.; Shafran, R. (2003). The clinical perfectionism questionnaire (unpublished manuscript). Department of Psychiatry, University of Oxford, UK. [ Links ]
Frazier, P. A.; Tix, A. P.; Barron, K. E. (2004). Testing moderator and mediator effects in counseling psychology research. Journal of Counseling Psychology, 51(1), 115-134. https://doi.org/10.1037/0022-0167.51.1.115 [ Links ]
Gilbert, P. (2009). The compassionate mind: A new approach to life's challenges. London: Robinson. [ Links ]
Gilbert, P. (2016). Human nature and suffering. London: Routledge. [ Links ]
Hayes, A. F. (2018). Introduction to mediation, moderation, and conditional process analysis: A regression-based approach. New York: Guilford. [ Links ]
Irons, C.; Beaumont, E. (2017). The compassionate mind workbook: A step-by-step guide to developing your compassionate self. London: Robinson. [ Links ]
James, K.; Verplanken, B.; Rimes, K. A. (2015). Self-criticism as a mediator in the relationship between unhealthy perfectionism and distress. Personality and Individual Differences, 79, 123-128. http://doi.org/10.1016/j.paid.2015.01.030 [ Links ]
Limburg, K.; Watson, H. J.; Hagger, M. S.; Egan, S. J. (2016). The relationship between perfectionism and psychopathology: A meta-analysis. Journal of Clinical Psychology, 73(10), 1301-1326. https://doi.org/10.1002/jclp.22435 [ Links ]
Lovibond, P. F.; Lovibond, S. H. (1995). The structure of negative emotional states: Comparison of the Depression Anxiety Stress Scales (DASS) with the Beck Depression and Anxiety Inventories. Behaviour Research and Therapy, 33(3), 335-343. https://doi.org/10.1016/0005-7967(94)00075-u [ Links ]
MacBeth, A.; Gumley, A. (2012). Exploring compassion: A meta-analysis of the association between self-compassion and psychopathology. Clinical Psychology Review, 32(6), 545-552. https://doi.org/10.1016/j.cpr.2012.06.003 [ Links ]
Mehr, K. E.; Adams, A. C. (2016). Self-compassion as a mediator of maladaptive perfectionism and depressive symptoms in college students. Journal of College Student Psychotherapy, 30(2), 132-145. https://doi.org/10.1080/87568225.2016.1140991 [ Links ]
Murtagh, S. (2018). Self-compassion as a mediator between maladaptive perfectionism and anxiety in college students (undergraduate thesis). The National College of Ireland, Dublin, Irlanda. http://norma.ncirl.ie/3282/ [ Links ]
Neff, K. D. (2003). The development and validation of a scale to measure self-compassion. Self and Identity, 2(3), 223-250. https://doi.org/10.1080/15298860309027 [ Links ]
Neff, K. D.; Germer, C. K. (2019). Manual de mindfulness e autocompaixão: Um guia prático para construir forças internas e prosperar na arte de ser seu melhor amigo. Porto Alegre: Artmed. [ Links ]
Raes, F.; Pommier, E.; Neff, K. D.; Van Gucht, D. (2011). Construction and factorial validation of a short form of the self-compassion scale. Clinical Psychology & Psychotherapy, 18(3), 250-255. https://doi.org/10.1002/cpp.702 [ Links ]
Rocha, L. F. D.; Hernandez, J. A. E.; Falcone, E. M. O. (2021). Latent structure evidence of the Depression, Anxiety and Stress Scales - Short Form. Estudos de Psicologia (Campinas), 38, 1-13. https://doi.org/10.1590/1982-0275202138e190103 [ Links ]
Rocha, L. F. D.; Hernandez, J. A. E.; Falcone, E. M. O. (in press). Psychometric properties of the Brazilian version of Clinical Perfectionism Questionnaire after rewording negatively keyed items. [Manuscript submitted in 2019 for publication in Análise Psicológica]. [ Links ]
Shafran, R.; Cooper, Z.; Fairburn, C. G. (2002). Clinical perfectionism: A cognitive-behavioural analysis. Behaviour Research and Therapy, 40(7), 773-791. https://doi.org/10.1016/S0005-7967(01)00059-6 [ Links ]
Shafran, R.; Egan, S.; Wade, T. (2018). Overcoming perfectionism: A self-help guide using scientifically supported cognitive behavioural techniques (2nd ed.). London: Robinson. [ Links ]
Slade, P. D.; Owens, R. G. (1998). A dual process model of perfectionism based on reinforcement theory. Behavior Modification, 22(3), 372-390. https://doi.org/10.1177/01454455980223010 [ Links ]
Smith, M. M.; Sherry, S. B.; Ge, S. Y. J.; Hewitt, P. L.; Flett, G. L.; Baggley, D. L. (2022). Multidimensional perfectionism turns 30: A review of known knowns and known unknowns. Canadian Psychology / Psychologie Canadienne, 63(1), 16-31. https://doi.org/10.1037/cap0000288 [ Links ]
Smith, M. M.; Sherry, S. B.; Rnic, K.; Saklofske, D. H.; Enns, M.; Gralnick, T. (2016). Are perfectionism dimensions vulnerability factors for depressive symptoms after controlling for neuroticism? A meta-analysis of 10 longitudinal studies. European Journal of Personality, 30(2), 201-212. https://doi.org/10.1002/per.2053 [ Links ]
Souza, L. K.; Hutz, C. S. (2016). Adaptation of the self-compassion scale for use in Brazil: Evidences of construct validity. Temas em Psicologia, 24(1), 159-172. https://doi.org/10.9788/TP2016.1-11 [ Links ]
Stoeber, J. (2018a). The psychology of perfectionism: An introduction. In: J. Stoeber (Ed.), The psychology of perfectionism: Theory, research, applications, p. 3-16. London: Routledge. [ Links ]
Stoeber, J. (2018b). The psychology of perfectionism: Critical issues, open questions, and future directions. In: J. Stoeber (Ed.), The psychology of perfectionism: Theory, research, applications, p. 333-352. London: Routledge. [ Links ]
Stoeber, J. (2020). Perfectionism. In: V. Zeigler-Hill; T. K. Shackelford (Eds.), Encyclopedia of personality and individual differences. New York: Springer. [ Links ]
Stoeber, J.; Lalova, A. V.; Lumley, E. J. (2020). Perfectionism, (self-)compassion, and subjective well-being: A mediation model. Personality and Individual Differences, 154, 1-4. https://doi.org/10.1016/j.paid.2019.109708 [ Links ]
Terry-Short, L. A.; Owens, R. Glynn; Slade, P. D.; Dewey, M. E. (1995). Positive and negative perfectionism. Personality and Individual Differences, 18(5), 663-668. https://doi.org/10.1016/0191-8869(94)00192-U [ Links ]
Thwaites, R.; Freeston, M. H. (2005). Safety-seeking behaviours: Fact or function? How can we clinically differentiate between safety behaviours and adaptive coping strategies across anxiety disorders?. Behavioural and Cognitive Psychotherapy, 33(2), 177-188. https://doi.org/10.1017/S1352465804001985 [ Links ]
Timmerman, M. E.; Lorenzo-Seva, U. (2011). Dimensionality assessment of ordered polytomous items with parallel analysis. Psychological Methods, 16(2), 209-220. https://doi.org/10.1037/a0023353 [ Links ]
Vignola, R. C. B.; Tucci, A. M. (2014). Adaptation and validation of the Depression, Anxiety and Stress Scale (DASS) to Brazilian Portuguese. Journal of Affective Disorders, 155, 104-109. https://doi.org/10.1016/j.jad.2013.10.031 [ Links ]
Zanon, C.; Brenner, R. E.; Baptista, M. N.; Vogel, D. L.; Rubin, M.; Al-Darmaki, F. R.; Gonçalves, M.; Heath, P. J.; Liao, H.; Mackenzie, C. S.; Topkaya, N.; Wade, N. G.; Zlati, A. (2020). Examining the dimensionality, reliability, and invariance of the Depression, Anxiety, and Stress Scale - 21 (DASS-21) across eight countries. Assessment, 28(6), 1531-1544. https://doi.org/10.1177/1073191119887449 [ Links ]
Recebido em 17 de fevereiro de 2021
Aceito para publicação em 02 de junho de 2021
Não se declararam fontes de financiamento.


{kind=link}
{kind=link}
{kind=link}