










Serviços Personalizados
Journal

artigo
 Inglês (pdf)
Inglês (pdf)
 Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
 Curriculum ScienTI
Curriculum ScienTIIndicadores
Compartilhar

 Permalink
PermalinkJournal of Human Growth and Development
versão impressa ISSN 0104-1282versão On-line ISSN 2175-3598
J. Hum. Growth Dev. vol.26 no.3 São Paulo 2016
https://doi.org/10.7322/jhgd.122816
ORIGINAL RESEARCH
doi: http://dx.doi.org/10.7322/jhgd.122816
How to monitor children with feeding difficulties in a multidisciplinary scope? Multidisciplinary care protocol for children and adolescents
Priscila MaximinoI; Rachel Helena Vieira MachadoI; Patrícia JunqueiraII; Maici CiariIII; Abykeila Melisse TosattiI; Cláudia de Cássia RamosII; Mauro FisbergIII
IDepartamento de Nutrição, Instituto PENSI/Hospital Infantil Sabará/Fundação José Luiz Egídio Setúbal - Av Angélica 1968 cj 71 - Higienópolis/SP - CEP 01228-200
IIDepartamento de Fonoaudiologia, Instituto PENSI/Hospital Infantil Sabará/Fundação José Luiz Egídio Setúbal - Av Angélica 1968 cj 71 - Higienópolis/SP - CEP 01228-200
IIIDepartamento de Nutrologia pediátrica, Instituto PENSI/Hospital Infantil Sabará/Fundação José Luiz Egídio Setúbal - Av Angélica 1968 cj 71 - Higienópolis/SP - CEP 01228-200
ABSTRACT
OBJECTIVES: To present the results of the implementation of a multidisciplinary approach to feeding difficulties in childhood and adolescence in a reference service
METHODS: The protocol was designed for outpatient patients aged from zero to 19 years old, with complaints of feeding difficulties and without psychiatric diagnoses, with signed parental consent. The protocol consists of paediatrician, speech therapist and nutritionist assessment in the same appointment, with common observation of evaluations and following multidisciplinary discussion. Diagnoses were categorized according Kerzner et al , and parenting styles according to Hughes20. Statistical analysis was conducted via SPSS v21 through frequency distribution (%), mean ± standard deviation, Chi-square test and ANOVA. Significance level was considered at 5%
RESULTS: Sample consisted of 56 children, 67.9% of males, most (75%) younger than 5 years old. The most frequent diagnosis was selectivity (30%). There was association between diagnoses and organic diseases in 30%. Start of complaints occurred at 18 months old. Speech-therapy alterations were detected mostly in speech (29%) and oral-motor skills (32%). Anthropometric assessment showed average normal growth patterns and average dietary assessment of protein intake derived from dairy products was above recommendations (18g/day
CONCLUSIONS: Results herein justify the presence of the multidisciplinary team in monitoring feeding difficulties in childhood and adolescence, and highlight the importance of longitudinal research nationwide
Keywords: children, feeding difficulties, selectivity, service protocols, multi-disciplinary.
INTRODUCTION
Feeding problems like refusal to eat, neophobia, picky eating or aversion are usually identified among children and teenagers heterogeneously. Although the studies on the topic are scarce, there are results which present different terminologies showing from 5,6% in Dutch children1 up to 30%, in a Canadian study2. Mascola et al.3, have described a prevalence between 13% and 22% in the American population.
One of the terminologies proposed to classify this condition is "feeding difficulties", suggested by Kezner et al.4 as a way of standardizing and incorporating several eating complaints that are common during childhood, such as low appetite, refusal to eat, disinterest for food, tantrums, the demand for rituals at the table, long lasting meals, excessive agitation, distractions, negotiations, blackmail and motherly dissatisfaction4,5. In the absence of specialized follow-up, feeding difficulties can become a lasting disorder6, having an impact in the child's cognitive, nutritional and emotional development, besides favoring both low weight and growth as well as obesity in the coming years7-9. Moreover, parents feel more and more dissatisfied and insecure with the quality and/or quantity of different kinds of food their children consume.
Given the complex, dynamic and sensorial nature of the feeding process, which requires the integration of organic, emotional and environmental actions10-12, interventions in problems related to refusing to eat demand a multi-disciplinary approach, regardless of the origin of the problem13,14. A multi-disciplinary team, different from a traditional one, works together and collaboratively in different contexts, resulting in the reduction of the time between medical appointments, the increase in the effectiveness in the evaluation and comprehension of the problem15. By using this interdisciplinary model, the doctor is responsible for the organic issues, the speech therapist is essential during the evaluation of the oral and motor conditions in order to enable healthy patterns of suction, chewing and swallowing, and the nutritionist follows up on the nutritional and anthropometric status of the patients16.
There are several protocols with a multidisciplinary approach when dealing with pediatric issues17,18, including overweight, obesity, dysphagia and organic alterations. However, there are gaps in the publications guided towards feeding difficulties. In Brazil, besides the scarce studies on this theme, there is also the lack of specialized interdisciplinary ambulatory teams of professionals that publish their results. Hence, the objective of this article is to present the results of the implementation of an outpatient service focused on exclusive multidisciplinary follow up for feeding difficulties during childhood and adolescence.
METHODS
Multidisciplinary service structure and sampling
The protocol was conceived by the multidisciplinary team at the Center of Feeding Difficulties, an outpatient clinic which is part of the PENSI Institute - Sabará Children's Hospital, supported by the José Luiz Egydio Setúbal Foundation and located in São Paulo, Brazil. The service helps children and teenagers between the ages of zero up to 19 years old who present complaints of feeding difficulties, excluding psychiatric diagnosis of eating disorders, according to official guidelines19.
Recruitment and sampling of patients were possible due to the promotion in the media and the referral of patients from other health care professionals. Given the fact that it was a pilot study, sampling was made through a convenience process. All patients assisted in the service were included in the study (after parents signed written consent forms), adding up to 56 patients in total. The assistance protocol was implemented as of July 2014 up to October 2015, after the approval of the ethics and research committee from PENSI Institute, under the registration number 32939314.0.0000.5567.
Service dynamics
The multidisciplinary service was structured in a triple flow, so that in the same appointment the patient is assessed by a pediatrician, a speech therapist and a nutritionist. By the first contact with the patient to schedule the appointment, families were advised to bring foods usually consumed by the children, as well as the utensils commonly used (plate, glass, baby bottle, spoon, fork, etc.). As one professional assessed the patient, the two remaining (from each specialty) accompanied the assessment inside an adjacent observation room with mirrors, audio and video (Gesell room), so that the patients did not notice the observation. After the appointment, the multidisciplinary team discussed each case in order to define the diagnosis and joint efforts to be made.
During a second appointment, the diagnosis put together by the team was presented to the family, as well as the therapeutic plan designed by each specialty. From then on, new appointments were scheduled - according to necessity - in order to apply the suggested treatment. Generally, plans for treatment consisted of diet plans and activities directed towards nutritional education (by a nutritionist), medications (by a doctor), stimulation and reestablishment of oral functions (by a speech therapist) or even referral to other professionals from other areas.
Service protocol
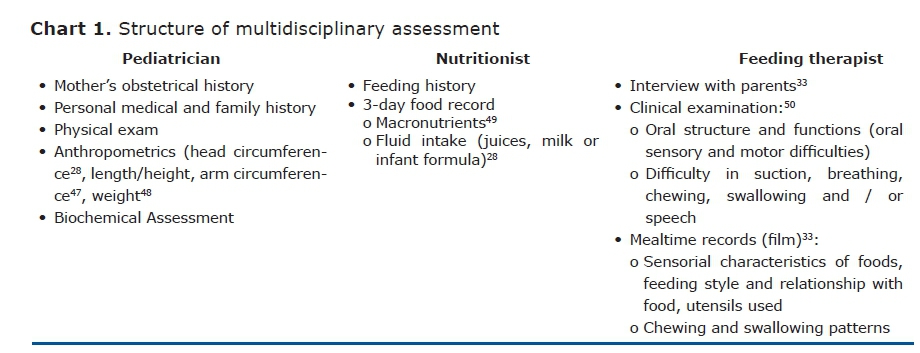
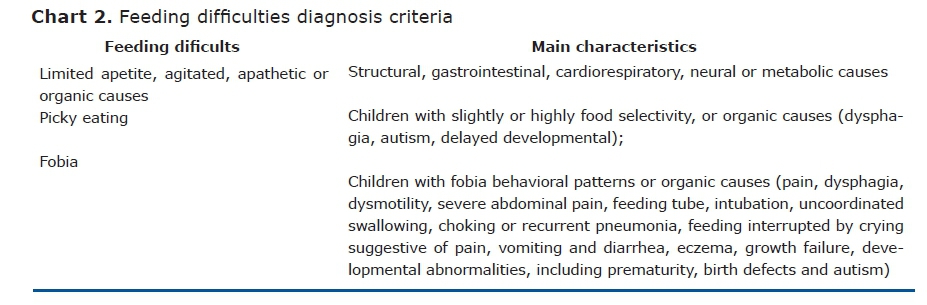
Guidelines for the service from each specialty are described in Chart 1. According to the information obtained by all the members from the multidisciplinary team, cases were categorized according to Kerzner et al.4, as described in Chart 2.
Diagnosis of feeding difficulties may vary as to its intensity, from lighter to severe, and may be associated to parental feeding styles, identified by the team according to clinical and observational history, besides the use of the instrument proposed by Hughes el al20; resulting in the classification of "Responsive Families", "Families with a controlling behavior", "Families with an indulgent behavior" and "Families with a negligent or third-partied behavior".
Statistical analysis
Data collected regarding the profile of the patients was transcribed in an Excel platform and evaluated according to its consistence. Statistical analysis was conducted by the software SPSS v21. Descriptive analysis was conducted through frequency of distribution (%) to the categorical variables and average ± standard deviation to the continuous variables. For comparisons between data on food intake, diagnosis and age, ANOVA test (or nonparametric equivalents) and Chi-squared tests were performed, respectively. A significance level of 5% was considered.
RESULTS
Multidisciplinary service structure
The flow of service is described in Figure 1.
Descriptive Analysis of the pilot sample
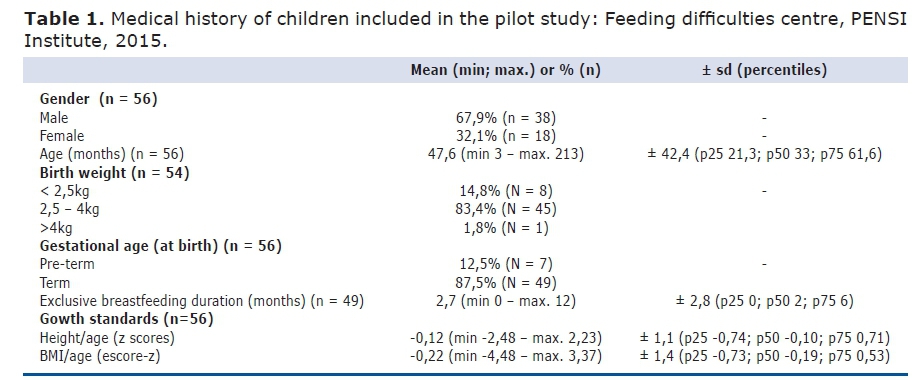
Characteristics of the clinical history of the population are described in Table 1. The sample consisted of children, majorly boys (67,9%) and at the approximate age of 2,7 years old (33 months; p25% 21,3 months; p75% 61,6 months), while 75% of the population assessed in this period was less than 5 years old. Low birth weight and preterm birth was present in approximately 15% and 13% of the cases, respectively. Children were breastfed exclusively for 2 months in average (p75% 6 months), while 25% of the population in the sample were never breastfed on an exclusive basis.
Regarding types of feeding difficulties, the main complaint reported by the caregivers was that children presented "decreased appetite and picky eating" (46,4%), followed by "They don't eat much and lose weight" (34%). The most frequent diagnosis conducted by the multidisciplinary team after the evaluation was picky eating (30%), followed by parent's misinterpretation (20%), while in 30% of total of cases the diagnosis was associated to organic alterations (such as gastric, neurologic, syndromic and allergic causes, among others). Around 75% of the population had the start of the complaints before 2 years of age, with a median of age at beginning of this process of 8 months (p25% 6 months, p75% 23 months). The average of the parent's age varied between 36 and 38 years (± 5,7 years) and nearly half of the approached families (49%) had also presented history of feeding difficulties during one or both parents' childhood. The feeding difficulties complete characteristics can be found in Table 2.
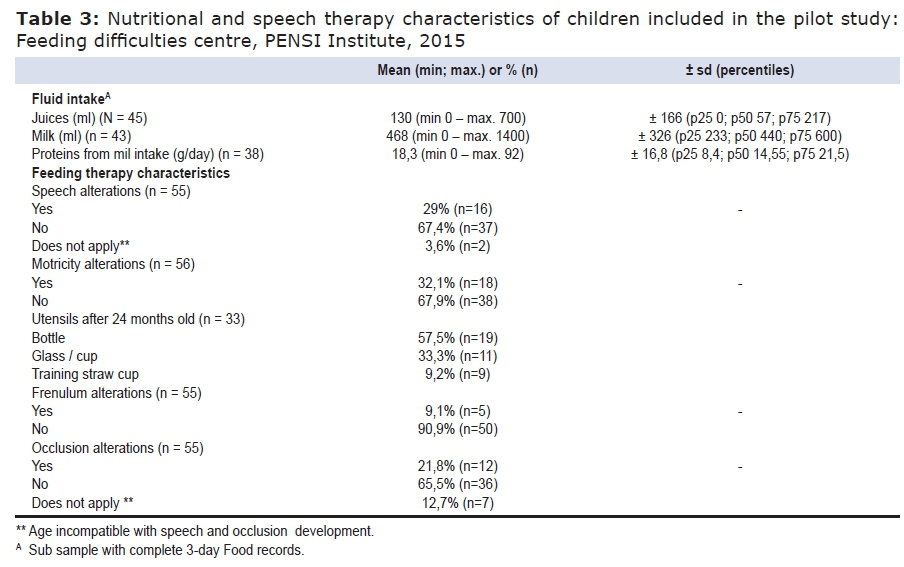
Data from the speech therapist evaluation can be found in Table 3. Assessment showed alterations in speech (29%), oral motor skills (32%), frenulum (9%) and occlusion (22%). Regarding nutritional status, population was majorly healthy, although quartiles suggest a trend of growth patterns in the inferior percentiles, with average values of Height/Age (HAZ) of -0,12sd (p25 -0,74; p75 0,71) and of BMI/Age of -0,22sd (p25 -0,73; p75 0,53). Regarding the fluid intake, there was a median volume of daily consumption of juices (natural or artificial) of 57ml (p75% 217ml, while 25% of the children didn't consume juice at all) and 440ml of milk (p25% 233ml, p75% 600ml). When comparing data across age groups, the ANOVA independent test showed a significant difference in the consumption of milk between children older than 8 years old and the ones between 1 and 3 years old (-336ml; IC95% -630; -42; p = 0,020), and 4 to 8 years old (-387ml; IC95% -705; -69; p = 0,012). It should be highlighted that 25% of the population drink more than 600ml of milk daily. There was no significant association between the volume of juice intake and age. The consumption of proteins derived from milk was around 18g/day. Consumption was also evaluated according to age, as demonstrated in Figure 2, showing protein inadequacy in children between 1 and 3 years old (median intake of 15,8g/day, above recommendations for age at 13g/day)21. This data considers only daily milk intake, disregarding the rest of the diet. These comparisons, however, did not present significant associations (p = 0,22).
With the exception of the variable age, types of feeding difficulties diagnosed in this pilot study were not tested for comparison with variables given to the limited N in each group. In a preliminary analysis, only the variable 'age' was related to diagnosis, while picky eating behavior was present more often in the age group of 4 to 8 years old (average of 48,5 months, ± 26,5sd) and the weight deviation in children who were above 8 years old (average of 142 months, ± 44,8sd) (p = 0,000).
DISCUSSION
Multidisciplinary service structure
This study describes the evaluation of children with feeding difficulties performed by a pediatrician, a nutritionist and a speech therapist in an integrated and collaborative approach, regardless of the origin of the complaint about the feeding process or the cause of the problem. In comparison with traditional methods of follow-up with a single professional, data from Australian and Canadian protocols show positive results after multidisciplinary treatments in 40% of the feeding problems, and 85% of the parents are favorable to this type of approach during the first evaluation visit, feeling more welcomed15,21. Marshall et al.14 highlight, in an Australian study, that the inclusion of occupational therapists and psychologists in the routine of the treatment also aids the enhancement of the evaluation and therapy methods, as well as Brazilian protocols22 that use this approach successfully to other feeding problems, such as overweight and obesity.
Pilot sample
Demographic characteristics of the population included in this pilot study show a higher prevalence of feeding difficulties in males (67,9%), with an average of 4 years of age (47,6 months, ± 42,4 months), while 75% of the population is below 5 years old. The beginning of the feeding problem was observed by the families, in average, at the age of 18 months. Mascola et al.3, in a longitudinal study with 120 children over the period of 9 years, didn't find any significant difference related to gender. Regarding age, Dubois et al.23 observed a higher incidence of picky eating in children between 2 years and a half and 4 years and a half (30 to 54 months old), with a slow decline up to 6 years old (72 months). The average of age in patients that presented picky eating in the present study was of 48 months ± 26,5sd, similar to these findings.
Regarding parents' perception of the problem, the main complaint reported in this study was "Low appetite and picky eating" (46,4%), followed by "They don't eat much and lose weight" (34%). However, the use of different definitions and methodologies makes it more difficult to compare with other studies. Family history of feeding difficulties was observed in 48,6% in parents during this study. Family environment, represented by the parents, influences and plays a determinant role in the development of preferences and feeding practices in children4,20,23,24. Hughes25, studying 639 families of 3 to 5-year-old children, concluded that positive motherly emotions also influence in food choices, including fruits and vegetables. Curtin et al.26 reinforce the need for the parents' presence in order for them to establish the behavior the child will assume regarding feeding patterns.
The multidisciplinary team's main diagnosis was the one related to picky eating (30%), and in 30% of all cases of difficulties there was an association with organic alterations, which can act as a triggering factor for food refusal (including gastric, neurological, syndromic and allergic reasons among others). According to Almeida et al.27 and the Brazilian Pediatrics Society28, reduction of appetite is a frequent condition and prodrome of any clinical disease, being usually a symptom that can persist until after its cure. Therefore, it is necessary to distinguish local conditions and those with a quick solution (such as canker sores, stomatitis and cheilitis) from those of difficult initial diagnosis, due poor clinical manifestations (such as gastroesophageal reflux, eosinophilic esophagitis and some food allergies). Gastroesophageal reflux, for example, has already been associated to a higher prevalence of behavioral or stomatognatic feeding problems, besides oral motor disorders (suction, chewing and swallowing disorders)29. Kerzner et al.4, differentiate feeding difficulties caused by organic causes (dysphagia, inhalation, apparent pain when feeding, vomiting and diarrhea, delay in development, chronical cardiorespiratory symptoms and growth deficit), from the behavioral ones (fixation on foods - extremely monotonous ingestion of foods, forced feeding, abrupt interruption of feeding after a traumatic event, anticipated choking and growth deficit), being necessary to refer the patient to specialists in order to conduct the correct treatment for each case.
Under the nutritional perspective, picky eating can be considered a threat to nutritional status due to the poor variety and limitation in quantity of foods ingested, altough few papers demonstrate this relationship9,30. In a prospective study with 120 children followed from 2 to 11 years of age3, there was no association between the selective behavior and loss of weight or growth. Xue et al.8, evaluated 793 Chinese healthy children and found that picky eaters had a lower ingestion of energy, proteins and carbohydrates when compared to the non picky eaters(p <0,05), besides lower values of HAZ in 0,184sd (IC 95%, -0,332, 0,036; p=0,015), lower in 0,385sd of Weight/Age (W/A) (IC 95%: -0,533, -0,237; p <0,001), and in 0,383sd of BMI/age (IC 95%: -0,563, -0,203; p <0,001). In the present study, although children were mostly healthy, there are more children in lower percentiles. Concern with low weight and growth during childhood is the main reason that makes parents go after specialized professional help for feeding difficulties4-6,25. They feel afraid of the consequences of poor nutrition, hence making the presence of a nutritionist in this multidisciplinary model beneficial to parents due to the reassurance of a thorough nutritional and anthropometric evaluation. Many mistakes in eating patterns can be corrected after this assessment, in order to establish an adequate eating behavior, aimed at solving the problem16.
As to macronutrient intake, there was a tendency to excessive protein ingestion and to the option of protein coming from dairy as a main feeding source. There was also the trend of reducing the consumption of milk, as they grew older. There are evidences of these associations31,32 in literature, just as of the association between unbalanced proportion of consumption of dairy proteins in children and enhancement of body fat, overweight and obesity. Hence, this shows the necessity for strategies to stimulate the ingestion of vegetable-originated proteins in children's diet, as well. Regarding juice consumption, the Brazilian Society of Pediatrics28 recommends the ingestion of 150ml for children between 2 and 6 years old, and 240ml for those older than 8. Although the average of daily ingestion (166ml) of juice in the present sample is coherent with the recommendations, it is noted that 25% of children consume a volume higher than recommended, which can contribute to the disinterest in the consumption of fruit in their solid form. Data available in the literature which relates the nutritional status and picky eating is focused on the refusal to eat in children with an autistic disorder, mostly, impairing comparisons with data here presented.
Under the speech therapist perspective, this pilot study showed 29% of speech alterations and 32% of alterations in the orofacial motor skills. Relationship between eating, speech and orofacial motor skills has been reason for discussion and studying among several authors33,34, and there is no convergence of opinion regarding this topic. There are scholars 35-37, who defend that the development is a sequential and predictable process that evolves around the maturation of the central nervous system. On the other hand, there are lines of research38-40 that suggest there are different mechanisms of motor control of speech, independent of oral functions involved in feeding. Regardless of that, feeding and speech development happen in parallel33. However, it is not possible to affirm that the skills related to feeding are pre-requisites in order for the child to speak. If that was the case, a child fed by tube would not have any possibility to develop speech. Motor development is a complex process that depends on the interaction among the child's biology, environment and culture in which one is inserted. This means the oral functions, as well as their development, are influenced by several variables and do not depend exclusively on neural maturation predicted for human beings. Despite this casual relation not being deeply established yet, literature mentions that picky eating may be related to a delayed development in motor-oral skills, while children with organic picky eating due to motor disorders present a higher difficulty with fluids or solid textures4. Therefore, the presence of a speech therapist in the team is essential for the diagnosis and the treatment of the feeding difficulty.
Another finding in the present pilot study showed 9% of alterations related to short frenulum or ankyloglossia. The effects of this anatomic limitation of the tongue have been the objective of frequent studies, and well-defined criteria and protocol have been published with the purpose of facilitating the diagnosis and prevalence in the population41. Literature shows an incidence of frenulum alterations between 0,2 and 12% of the population42, and the most frequent problems caused by ankyloglossia mentioned are related to speech, followed by the ones related to feeding mainly during the breast feeding phase43-45, and the alterations in swallowing and chewing, development of the skeleton structures of the face, teeth alteration, occlusion and the periodontal tissue46. Therefore, this kind of alteration has an impact in feeding and speech, highlighting the necessity for an intervention in order to improve the general situation of the feeding difficulty47-50.
The study has limitations, such as the lack of a control group, restricted sample size (which limits the association tests between the variables) and the absence of a model of follow-up to verify possible correlations. However, it opens room for discussion about this model of service (using the classification proposed by Kezner et al.4 for feeding difficulties), still poorly used in Brazil, as well as epidemiological data, which can foment new researches around this topic.
CONCLUSION
The outpatient service assessed picky eating children and teenagers, in most of the cases, with the minority of the cases related to organic causes. The complaint appeared, in average, before 2 years of age. The nutritional evaluation of the patients showed a healthy profile of the population, with inadequate protein intake. Speech and motor skills alterations were also detected. The results justify the necessity for a multidisciplinary team to follow up on the feeding difficulties in childhood and adolescence, and evidence the importance of the continuity of this topic as longitudinal research nationwide.
ACKNOWLEDGEMENTS
To "PENSI Institute-Hospital Infantil Sabará-Fundação José Luiz Egydio Setúbal", for the support given to the "Center of Feeding difficulties".
REFERENCES
1. Tharner A, Jansen PW, Kiefte-de Jong JC, Moll HA, van der Ende J, Jaddoe VW, et al. Toward an operative diagnosis of fussy/picky eating: a latent profile approach in a population-based cohort. Int J Behav Nutr Phys Act. 2014;11:14. DOI: http://dx.doi.org/10.1186/1479-5868-11-14 [ Links ]
2. Dubois L, Farmer A, Girard M, Peterson K, Tatone-Tokuda F. Problem eating behaviors related to social factors and body weight in preschool children: A longitudinal study. Int J Behav Nutr Phys Act. 2007;4:9. DOI: http://dx.doi.org/110.1186/1479-5868-4-9 [ Links ]
3. Mascola AJ, Bryson SW, Agras SW. Picky eating during childhood: A longitudinal study to age 11years. Eat Behav. 2010;11(4):253-7. DOI: http://dx.doi.org/10.1016/j.eatbeh.2010.05.006 [ Links ]
4. Kerzner B, Milano K, MacLean Jr WC, Berall G, Stuart S, Chatoor I. A practical approach to classifying and managing feeding difficulties. Pediatrics. 2015;135(2): 344-53. DOI: http://dx.doi.org/10.1542/peds.2014-1630 [ Links ]
5. Sampaio AB, Nogueira TL, Grigolon RB, Roma AM, Pereira LE, Dunker KL. Seletividade Alimentar: uma abordagem nutricional. J Bras Psiquiatr. 2013;62(2):164-70. DOI: http://dx.doi.org/10.1590/S0047-20852013000200011 [ Links ]
6. Ostberg M, Hagelin E. Feeding and sleeping problems in infancy - a follow up at early school age. Child Care Health Dev. 2011;37(1):11-25. DOI: http://dx.doi.org/10.1111/j.1365-2214.2010.01141.x [ Links ]
7. Jansen PW, Roza SJ, Jaddoe VW, Mackenbach JD, Raat H, Hofman A, et al. Children's eating behavior, feeding practices of parents and weight problems in early childhood: results from the population-based Generation R Study. Int J Behav Nutr Phys Act. 2012; 9:130. DOI: http://dx.doi.org/10.1186/1479-5868-9-130 [ Links ]
8. Xue Y, Lee E, Ning K, Zheng Y, Ma D, Gao H, et al. Prevalence of picky eating behaviour in Chinese school-age children and associations with anthropometric parameters and intelligence quotient. A cross-sectional study. Appetite. 2015;91:248-55. DOI: http://dx.doi.org/10.1016/j.appet.2015.04.065 [ Links ]
9. Dovey TM, Farrow CV, Martin CI, Isherwood E, Halford JC. When does food refusal require professional intervention? Current Nutr Food Sci. 2009;5(3):160-71. DOI: http://dx.doi.org/10.2174/157340109789007162 [ Links ]
10. Story M, Neumark-Sztainer D, French S. Individual and environmental influences on adolescent eating behaviors. J Am Diet Assoc. 2002;102(3):S40-51. [ Links ]
11. Schwartz C, Scholtens PA, Lalanne A, Weenen H, Nicklaus S. Development of healthy eating habits early in life. Review of recent evidence and selected guidelines. Appetite. 2011;57(3):796-807. DOI: http://dx.doi.org/10.1016/j.appet.2011.05.316 [ Links ]
12. Dovey TM, Aldridge VK, Dignan W, Staples PA, Gibson EL, Halford JC. Developmental differences in sensory decision making involved in deciding to try a novel fruit. Br J Health Psychol. 2012;17(2):258-72. DOI: http://dx.doi.org/10.1111/j.2044-8287.2011.02036.x [ Links ]
13. Rommel N, De Meyer AM, Feenstra L, Veereman-Wauters G. The complexity of feeding problems in 700 infants and young children presenting to a tertiary care institution. J Pediatr Gastroenterol Nutr. 2003; 37(1):75-84. [ Links ]
14. Marshall J, Hill RJ, Ware RS, Ziviani J, Dodrill P. Multidisciplinary intervention for childhood feeding difficulties. J Pediatr Gastroenterol Nutr. 2015;60(5):680-7. DOI: http://dx.doi.org/10.1097/MPG.0000000000000669 [ Links ]
15. Owen C, Ziebell L, Lessard C, Chuercher E, Bourget V, Villenueve H. Interprofessional group intervention for parents of children age 3 and younger with feeding difficulties: pilot program evaluation. Nutr Clin Pract. 2012;27(1):129-35. DOI: http://dx.doi.org/10.1177/0884533611430231 [ Links ]
16. Edwards S, Davis AM, Ernst L, Sitzmann B, Bruce A, Keeler D, et al. Interdisciplinary Strategies for Treating Oral Aversions in Children. JPEN J Parenter Enteral Nutr. 2015;39(8):899-909. DOI: http://dx.doi.org/10.1177/0148607115609311 [ Links ]
17. Arvedson JC. Assessment of pediatric dysphagia and feeding disorders: clinical and instrumental approaches. Dev Disabil Res Rev. 2008;14(2):118-27. DOI: http://dx.doi.org/10.1002/ddrr.17 [ Links ]
18. Conroy C, Logan DDE. Pediatric multidisciplinary and interdisciplinary teams and interventions. Clinical Practice of Pediatric Psychology. 2014; p.93. [ Links ]
19. American Psychiatric Association. Manual diagnóstico e estatístico de transtornos mentais. 4th ed. Artmed; 2002. [ Links ]
20. Hughes SO, Power TG, Orlet Fisher J, Mueller S, Nicklas TA. Revisiting a neglected construct: parenting styles in a child-feeding context. Appetite. 200544(1):83-92. DOI: http://dx.doi.org/10.1016/j.appet.2004.08.007 [ Links ]
21. Krom H, Otten MAGM, Veer L van der S, Zundert SMC van, Khawaja FK, Benninga MA, et al. Multidisciplinary approach in young children with severe feeding disorders. 2013;81:72. DOI: http://dx.doi.org/10.1007/s12456-013-0070-6 [ Links ]
22. Poeta LS, Duarte MFS, Giuliano ICB, Mota J. Interdisciplinary intervention in obese children and impact on health and quality of life. J Pediatr (Rio J). 2013;89(5):499-504. DOI: http://dx.doi.org/10.1016/j.jped.2013.01.007 [ Links ]
23. Dubois L, Farmer AP, Girard M, Peterson K. Preschool children's eating behaviours are related to dietary adequacy and body weight. Eur J Clin Nutr. 2007;61(7):846-55. DOI: : http://dx.doi.org/10.1038/sj.ejcn.1602586 [ Links ]
24. Bento IC, Esteves JMM, França TE. Alimentação saudável e dificuldades para torná-la uma realidade: percepções de pais/responsáveis por pré-escolares de uma creche em Belo Horizonte/MG, Brasil. Ciênc Saúde Coletiva. 2015;20(8):2389-2400. DOI: http://dx.doi.org/10.1590/1413-81232015208.16052014 [ Links ]
25. Hughes SO, Shewchuk RM. Child temperament, parent emotions, and perceptions of the child's feeding experience. Int J Behav Nutr Phys Act. 2012;29:9:64. DOI: http://dx.doi.org/10.1186/1479-5868-9-64 [ Links ]
26. Curtin C, Hubbard K, Anderson SE, Mick E, Must A, Bandini LG. Food Selectivity, Mealtime Behavior Problems, Spousal Stress, and Family Food Choices in Children with and without Autism Spectrum Disorder. J Autism Dev Disord. 2015;45(10):3308-15. DOI: http://dx.doi.org/10.1007/s10803-015-2490-x [ Links ]
27. Almeida CAN, Mello ED, Maranhão HS, Vieira MC, Barros R, Fisberg M, et al. Dificuldades alimentares na infância: revisão da literatura com foco nas repercussões à saúde. Pediatr Mod. 2012;48(9):24-26. [ Links ]
28. Sociedade Brasileira de Pediatria (SBP). Manual de orientação para a alimentação do lactente, do pré-escolar, do escolar, do adolescente e na escola. 3rd ed. Rio de Janeiro: SBP; 2012. [ Links ]
29. Drent LV, Pinto EALC. Problemas de alimentação em crianças com doença do refluxo gastroesofágico. Pró-Fono R Atual Cient. 2007;19(1):59-66. DOI: http://dx.doi.org/10.1590/S0104-56872007000100007 [ Links ]
30. Taylor CM, Wernimont SM, Northstone K, Emmett PM. Picky/fussy eating in children: Review of definitions, assessment, prevalence and dietary intakes. Appetite. 2015; 1(95):349-59. DOI: http://dx.doi.org/10.1016/j.appet.2015.07.026 [ Links ]
31. Bigornia SJ, LaValley MP, Moore LL, Northstone K, Emmett P, Ness AR, et al. Dairy intakes at age 10 years do not adversely affect risk of excess adiposity at 13 years. J Nutr. 2014;144(7):1081-90. DOI: http://dx.doi.org/10.3945/jn.113.183640 [ Links ]
32. Günther AL, Remer T, Kroke A, Buyken AE. Early protein intake and later obesity risk: which protein sources at which time points throughout infancy and childhood are important for body mass index and body fat percentage at 7 y of age? Am J Clin Nutr. 2007;86(6):1765-72. [ Links ]
33. Morris SE, Klein MD. Pre-feeding skills: a comprehensive resource for feeding development. Tucson: Therapy Skill Builders; 1987. [ Links ]
34. Ruscello DN. Nonspeech Oral Motor Treatment Issues Related to ChildrenWith Developmental Speech Sound Disorders. Language, Speech and Hearing Services in Schools. Am Speech Language Hearing Association. 2008;39: 380-91. [ Links ]
35. Neistadt ME, Crepeau EB. Willard and Spackman's occupational therapy. 9th ed. New York: Lippincott; 1998. [ Links ]
36. Ferriolli BHVM. Associação entre as alterações de alimentação infantil e distúrbios de fala e linguagem. CEFACS. 2010;12(6):990-7. DOI: http://dx.doi.org/10.1590/S1516-18462010005000037 [ Links ]
37. Felício CM, Ferreira-Jeronymo RR, Ferriolli BHVM, Freitas RLRG. Análise da associaçäo entre sucçäo, condiçöes miofuncionais orais e fala. Pró-Fono. 2003;15(1): 31-40. [ Links ]
38. Connaghan KP, Moore CA, Higashakawa M. Respiratory kinematics during vocalization and nonspeech respiration in children from 9 to 48 months. J Speech Lang Hear Res. 2004;47(1):70-84. DOI: http://dx.doi.org/10.1044/1092-4388(2004/007 [ Links ]
39. Moore CA, Caulfield TJ, Green JR. Relative kinematics of the rib cage and abdomen during speech and nonspeech behaviors of 15-month-old children. J Speech Lang Hear Res. 2001;44(1):80-94. [ Links ]
40. Moore CA, Ruark JL. Does speech emerge from earlier appearing oral motor behaviors? J Speech Hear Res. 1996;39(5):1034-47. [ Links ]
41. Martinelli RLC, Marchesan IQ, Berretin-Felix G. Lingual frenulum evaluation protocol for infants: relationship between anatomic and functional aspects. Rev CEFAC. 2013;15(3):599-610. [ Links ]
42. Marchesan IQ, Oliveira LR, Costa ML, Araujo RL. Análise comparativa da mastigação em pacientes com e sem alteração do frênulo lingual. In XV Congresso Brasileiro de Fonoaudiologia e VII Congresso Internacional de Fonoaudiologia. Gramado: 2007. [ Links ]
43. Lalakea ML, Messner AH. Ankyloglossia: the adolescent and adult perspective. Otolaryngol Head Neck Surg. 2003;128(5):746-52. [ Links ]
44. Messner AH, Lalakea ML, Aby J, Macmahon J, Bair E. Ankyloglossia: incidence and associated feeding difficulties. Arch Otolaryngol Head Neck Surg. 2000;126(1): 36-9. [ Links ]
45. Ballard L, Auer E, Khoury C. Ankyloglossia: Assessment, Incidence, and Effect of Frenuloplasty on the Breastfeeding Dyad. Pediatrics. 2002 nov; 110(5):e63. [ Links ]
46. Marchesan IQ. Protocolo de avaliação do frênulo da língua. Rev CEFAC. 2010; 12(6):977-89. [ Links ]
47. World Health Organization (WHO). Child growth standards and the identification of severe acute malnutrition in infants and children. Switzerland: WHO; 2009. [ Links ]
48. Sociedade Brasileira de Pediatria (SBP). Obesidade na infância e adolescência: manual de orientação. Rio de Janeiro: Departamento de nutrologia; 2008. [ Links ]
49. Junqueira P, Maximino P, Ramos CC, Machado RHV, Assumpção I, Fisberg M. O papel do fonoaudiólogo no diagnóstico e tratamento multiprofissional da criança com dificuldade alimentar: uma nova visão. CEFACS. 2015;17(3):1004-11. DOI: http://dx.doi.org/10.1590/1982-021620151614 [ Links ]
50. Institute of Medicine (IM). Dietary Reference Intakes for Energy, Carbohydrate, Fiber, Fat, Fatty Acids, Cholesterol, Protein, and amino acids. Washington: The National Academies Press. 2002/2005. [ Links ]
Manuscript Submitted Mai 25 2016,
Accepted for publication 10 Jun 2016
Corresponding author: Mauro Fisberg. mauro.fisberg@gmail.com


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}