










Serviços Personalizados
Journal

artigo
 Inglês (pdf)
Inglês (pdf)
 Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
Indicadores
Compartilhar

 Permalink
PermalinkJournal of Human Growth and Development
versão impressa ISSN 0104-1282versão On-line ISSN 2175-3598
J. Hum. Growth Dev. vol.29 no.2 São Paulo maio/ago. 2019
https://doi.org/10.7322/jhgd.v29.9416
ORIGINAL ARTICLE
Spatial and Spatio-temporal Analysis of Congenital Malformations of Nervous System in the State of Paraíba from 2010 to 2016
Luciana Moura Mendes de LimaI; Rodrigo Pinheiro de Toledo ViannaII; Ronei Marcos de MoraesII
IMestre e Doutoranda do Programa de Pós-Graduação em Modelos de Decisão e Saúde, Universidade Federal da Paraíba, João Pessoa, Paraíba, Brasil
IIProfessor permanente do Programa de Pós-Graduação em Modelos de Decisão e Saúde, Universidade Federal da Paraíba, João Pessoa, Paraíba, Brasil
ABSTRACT
INTRODUCTION: In Brazil, congenital malformation anomaly of the nervous system has been the most frequent among the anomalies. Knowledge of your geographical distribution both in space as throughout the time, can assist public managers in the decision-making process about the areas that must be prioritized for the monitoring of this disease.
OBJECTIVE: Detecting spatial and spatio-temporal clusters of congenital malformations of nervous system.
METHODS: An ecological study based on secondary data from the National Information System on Live Births in the period from 2010 to 2016 in the state of Paraíba. We estimated the spatial incidence ratios and applied circular and spatio-temporal Scan statistics to detect clusters with of abovementioned malformations.
RESULTS: The spatial pattern was different throughout the years of the occurrence of these malformations, since the spatial clusters were detected on different regions of the state, except in the years 2013 and 2015, which revealed a higher concentration in the central-west and northwest regions of the state. The retrospective spatio-temporal analysis revealed three clusters that persisted during the years of 2015 and 2016.
CONCLUSION: The findings indicated the regions that must be prioritized for the monitoring of congenital malformations of nervous system in the state of Paraíba in time and space.
Keywords: spatial analysis, spatiotemporal analysis, cluster analysis, congenital defects.
Authors summary
Why was this study done?
This study was performed due to a paucity of research related to spatial and spatio-temporal analysis for congenital malformation of nervous system.
What did the researchers do and find?
The researchers developed an ecological study using secondary data from National Information System on Live Births. Spatial Incidence Ratio, circular spatial Scan and spatio-temporal Scan Statistics for detecting spatial clusters were used on congenital malformation of nervous system data. The spatial patterns of the clusters were different throughout the years, except 2013 and 2015, in which was verified a higher concentration in the central-west and northwest regions of the state. Three spatial clusters persisted throughout the years 2015 and 2016.
What do these findings mean?
They suggest a methodology able to indicate areas which prioritized for their monitoring of congenital malformations of nervous system in the state of Paraíba in time and space. This methodology can support decision making process regarding this subject by public health managers.
INTRODUCTION
A congenital malformation (CM) is an internal or external structural defect in genesis, which is usually identified at birth1. Most happens between the third and eighth week of gestation2. The large anomaly is a defect that requires significant surgical or aesthetic interventions, but in the case of a small, this type of intervention may not be necessary1.
The etiology may be due to genetic, environmental or multifactorial causes. The multifactorial causes include the gene-teratogen interactions and malformations of unknown origin and correspond to 55% of cases. The genetic causes include the chromosomal malformations and single gene mutations and represent 30% of occurrences. The environmental causes involve drugs/medication, environmental pollutants, infectious diseases and maternal diseases, they constitute 15% of cases2. The literature highlights that pregnancies of women younger than 20 years or older than 35 years have an increased risk for CM3,4. However, in addition to age, other factors may increase the likelihood of the occurrence of malformations, including: family history, acute diseases in the first quarter and exposure to physical factors3,5.
It is a condition that has a great impact on society, especially in the family context. Since they face difficulties in understanding the diagnosis, in dealing with prejudices, in addition as well as obstacles in the search for proper care that the child will depend for years to have a better quality of life6.
The most frequent CM in Brazil is the malformation of nervous system7,8. In 2016, there were 4,820 cases this type, with the Northeast region ranking second in the number of occurrences, with only the Southeastern region in front of it9. A study conducted in Brazil using data from the National Census of Isolated Populations on Brazilian populations with a high frequency of genetic diseases or congenital anomalies or environmental, identified CM in the Sertão Paraibano region10.
When one takes spatial and spatio-temporal (ST) information into consideration in the decision-making process, it is important to know its geographic distribution. The spatial analysis enables the identification of characteristics related to these events in the territory in order to plan prevention and control measures11 that can contribute to a better organization of health care management. In a study on the occurrence of congenital anomalies in space and time, their geographical distributions are used to support public managers in the care given to these children and families. No studies associating CM of nervous system and their geographical distributions in the state of Paraíba were found in the literature. Therefore the main goal of this study is detecting spatial and ST clusters of CM of nervous system in the state of Paraíba in the period from 2010 to 2016.
METHODS
This study is exploratory, quantitative and ecological in nature, using secondary data from the National Information System on Live Births (SINASC). All live births with CM of nervous system in the state of Paraíba, in the period from 2010 to 2016, were included. The state of Paraíba is composed of 223 municipalities and is situated in the Northeast of Brazil.
The Spatial Incidence Ratio (SIR) were calculated for all municipalities (geo-objects) and circular and ST Scan statistics were applied to analyze the data in order to detect spatial and ST clusters of malformations above mentioned. Understanding the concepts of geographical region and geo-object is crucial for the analysis of the SIR.
The region is a geographic area in which the events of interest occur. While the geo-object is manifested by distinct entities and detected geographically in the geographical region12. Formally, therefore, SIR are represented by a geographical region R composed by a set of n geo-objects represented as r1, r2, ..., rn. Where C(ri), i=1,..., n, is a random variable representing the number of cases of an epidemiological event in a given interval of time for each geo-object ri and is expressed by c1, c2, ..., cn. Where P(ri) is the population at risk for that epidemiological event in each geo-object ri, denoted as p1, p2, ..., pn13. The SIR in each geo-object ri is presented in the following equation:
The explanation of the SIR(ri) can be performed according to the following categories: if the geo-object ri under study has no epidemiological incidence, the SIR will be equal to 0; if 0<SIR(ri)<0.5; , then the SIR is less than half of the total incidence of the geographical region in that geo-object ri; if 0.5≤SIR(ri)<1.0 then SIR is more than half of the total incidence, but is less than the epidemiological incidence of the geographical region; 1.0≤SIR(ri)<1.5 then SIR is higher than the overall incidence of the geographical region by less than 50%; if 1.5≤SIR(ri)<2.0 then SIR is higher than the overall incidence of the geographical region by more than 50%; and if SIR(ri)≥2.0 then it is two or more times higher than the total incidence of the geographical region13. So, the SIR of the geo-object ri is given by the incidence ratios of the occurrence of CM of nervous system in that geo-object (municipality) with respect to the geographic region (the state of Paraíba).
Circular scan statistics were used for the detection of the spatial clusters of the CM14. The method searches the entire geographical region of study for geo-object clusters (composed by at least one geo-object), which are defined as clusters where the likelihood of case occurrence is significantly higher inside it than outside it. To this end, the information of the geo-object must be concentrated in a single point within it, called the centroid, which representes the center of mass of each region's area14.
To identify these spatial clusters, the likelihood ratio test is used, which checks whether the observed number of cases in a geo-object exceeds the expected number of cases. If this does not occur, a circle centered around the centroid of that geo-object is increased so as to encompass its neighbors. The radius of the circle can vary from zero to a maximum percentage of 50% of the population under risk14. The radius of each circle created by the scan statistics is based on the total number of cases and the population size in the geographic region15.
The ST scan was used for the detection of clusters that occur simultaneously in space and time. The method can be defined by a window with a cylindrical shape with its circular base representing the geographical dimension and its height the interval of time. As such, the cylindrical window is moved in space and time for each possible location and size of the circle as well as for each possible time interval. Although an infinite number of cylinder overlays is obtained, the epidemiological data contains a finite number of individuals, which means some of these cylinders will contain exactly the same number of people. This circumstance therefore leads to a finite number of cylinders for which the probability really has to be calculated. It is recommended that the size of the geographical dimension (circular base) and the time interval should be limited to half the number of expected cases and half of the total period, respectively16.
That method can be used both retrospectively or prospectively. The prospective use seeks to detect clusters that are still active, i.e., those that are still present during the last time period for which data is available. It is repeated periodically in time, for example, every day, week, month or year16. The retrospective study, meanwhile, detects clusters that began and ended before the beginning of the study. It is used in a single analysis, using historical data, for example17. The retrospective ST scan was used with historical data from SINASC with a persistence time of one, two and three years.
The discrete Poisson model was the most appropriate for the study since it uses occurrence count data15. It was used a significance level of 5% for the Monte Carlo simulations hypothesis tests with 999 random replications of the data with a null hypothesis of both spatial and ST randomness14,16. This study analyzed, 0.1%, 0.3%, 0.5%, 0.7%, and the values between 1.0 and 10% of the population at risk, and for the ST analysis persistence times of one, two and three years were used. Next, the scan statistics maps were analyzed for each year and ST scan, using the SIR maps as reference.
The data were stored in a electronic spreadsheet and analyzed in the SaTScanTM and R software. The project was approved by the Brazil Platforma under protocol number 082/17.
RESULTS
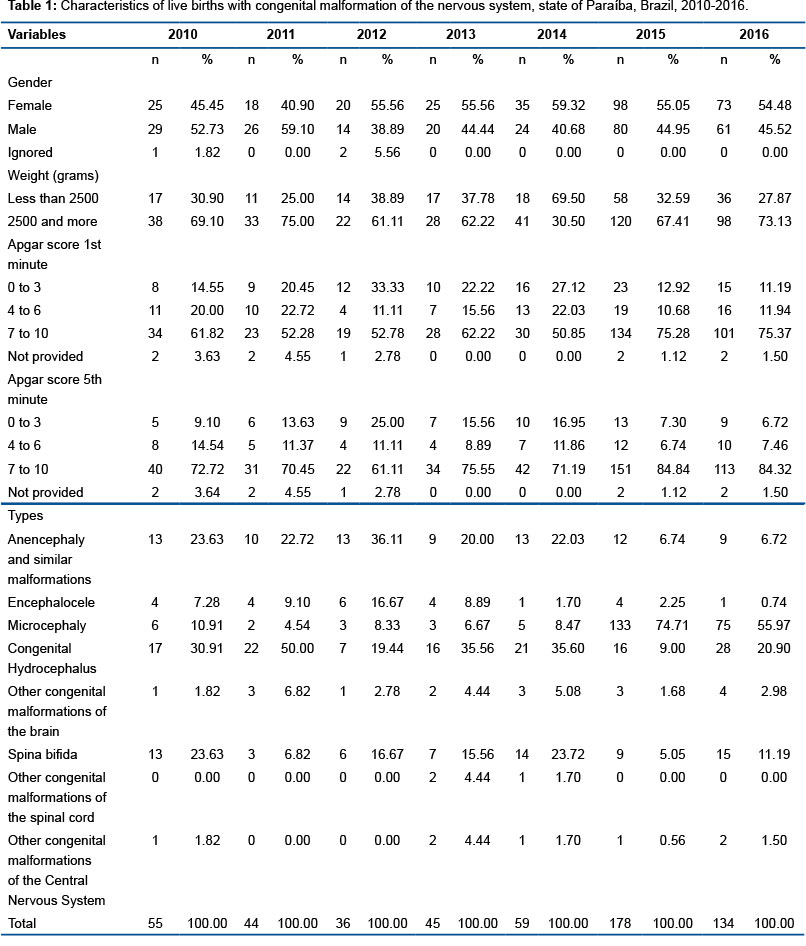
In the period from 2010 to 2016, 551 cases of CM of nervous system were reported in the state of Paraíba. Of these, 53.3% were females, with a mean weight of 2757 grams. Approximately 70% of live births had an Apgar score greater than or equal to seven in the first minute and 78.5% in the fifth minute. The malformations with a higher frequency included microcephaly, hydrocephalus, anencephaly and similar malformations, representing 76.5% of the sample, as can be seen in Table 1.
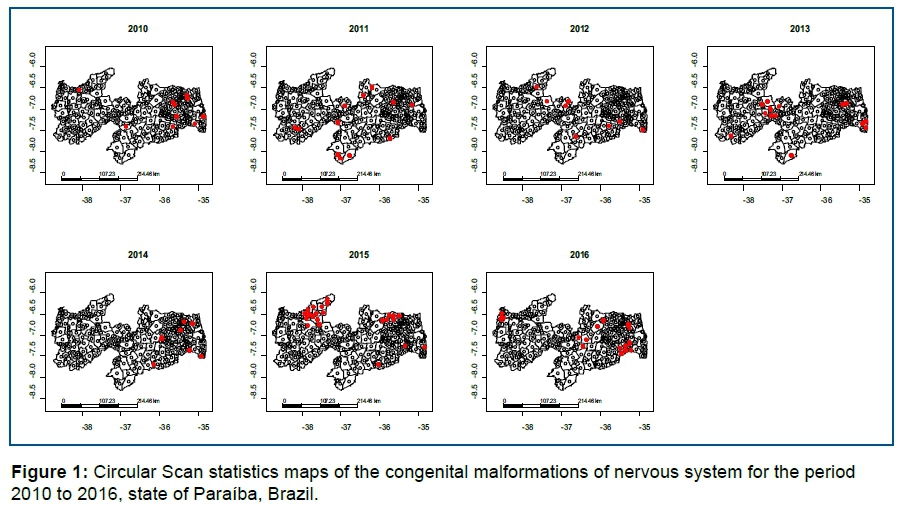
In relation to the detection of spatial clusters through the circular Scan statistic, 0.3% of the at-risk population was listed for the years 2010, 2011, 2012 and 2014, obtaining 10, 12, 8 and 8 spatial clusters, respectively, distributed throughout the state. 14 spatial clusters were identified in the year 2013 with a higher number in the center-west region of the state, under na at-risk population of 1%. With an at-risk population of 7% in the year 2015, 23 were detected with a greater concentration in the northwest of the state. In the year of 2016, 16 spatial clusters were detected with an at-risk population of 1% (Figure 1).
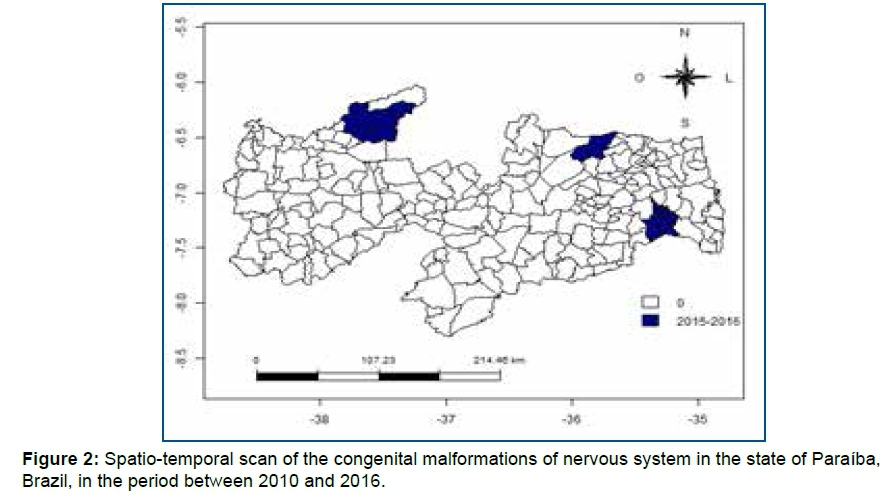
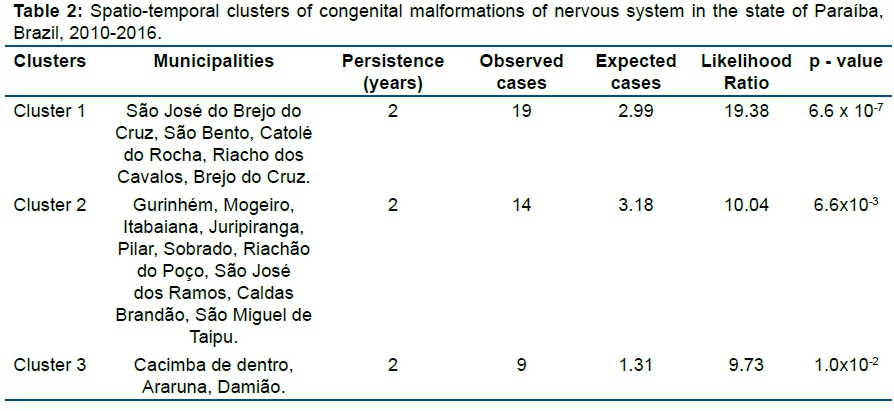
A retrospective approach was used in the ST scan for the period from 2010 to 2016, with an at-risk population of 2% and a persistence time of two years, using the SIR maps as reference, obtaining three clusters that persisted simultaneously in space and time (Figure 2).
Table 2 shows the information related to the ST clusters, such as the, the municipalities making up the clusters, persistence time, the expected and observed number of cases, the likelihood ratio and the p-value.
DISCUSSION
The spatial analysis revealed that the clusters were dispersed in different regions of the state, except in the years 2013 and 2015, which showed a higher concentration in the central-west and northwest regions of the state, respectively, representing the Sertão Paraibano. Cardoso et al.10 mapped genetic diseases and CM in Brazil and observed a high percentage of CM in the region of the Sertão Paraibano, albeit not in the same locations as in the present study.
In the year of 2010, ten spatial clusters scattered throughout the state were identified, but most were located in the eastern region near the capital of the state. In 2011, the spatial clusters present were not in the same regions as in the previous year. The eight identified in 2012 were well dispersed. In the following year of 2013, meanwhile, there was a greater concentration in the center-west portion of the state, in the region of the Sertão. In 2014, the spatial clusters were detected near the major cities of the state. It is worth mentioning that this is the only year in which they were not identified in the central-west and western regions of the state. In the year 2015, the Sertão Paraibano region had a larger numbers, which were in different locations than in the year 2013. The 15 spatial clusters observed in the year of 2016 were mostly between the northeast and southeast of the state. It is worth noting that when referring to the purely spatial analysis, the spatial clusters cannot be compared in relation to years, so one could not say that a change or displacement between them occurred.
With respect to the ST analysis, a approach was used in which clusters that began and ended before the beginning of the study were pointed out, detecting three, which are concentrated in the northeast, southeast and northwest of the state, which persisted during the years of 2015 and 2016. Cluster 1, located to the northwest of the state, is far from the state capital (more than 350 kilometers). This negatively affects the access to the main reference centers, especially the hospitals and maternity units specialized in high-risk pregnancies. Cluster 2 is located to the southeast of the state, close to the capital and major cities in the state, which offer more adequate care support. Finally, cluster ST 3 is located about 200 kilometers from the capital city near the border with the state of Rio Grande do Norte, being composed of small-sized municipalities.
Only two of the seven years under study showed the occurrence of persistent cases for these CM, which were the years of 2015 and 2016. This period was marked by a change in the historical series of microcephaly at the SINASC. Since the year 2000, the prevalence of microcephaly in newborns was 5.5/100,000 live births, with this frequency holding steady until 2010 (5.7/100,000 live births). At the end of 2015, the incidence increased to 99.7/100,000 live births, corresponding to a 20-fold increase in comparison with the rate observed in previous years18. According to Barreto et al.19, issues related with the magnitude of this problem project new health care patterns, needs and demands into the following years that should be investigated. Adequate resources, training and qualifications will have to be defined to deal with this current situation. The increase in these cases of microcephaly has been attributed to the probable intrauterine exposure to the Zika virus20.
Groisman et al.21 highlight the importance of studying clusters by stating that the maps used in conjunction with statistical tests may be useful for researchers in the health care sector by focusing attention on areas for further research. They further state that, because these maps show general disease patterns, they generate hypotheses about the role of environmental, genetic or life style factors in the etiology of a disease.
Circular scan statistics have been used in different studies on CM22-24. ST scan in the health care sector have been employed to identify clusters for tuberculosis25, hand-foot-mouth disease26, breast cancer27,28 and CM21. These methods can be used in geographic patterns with different types of diseases, demonstrating their legitimacy. The studies showed a clustering analysis using the circular or ST scan statistics, but did not use both methods at the same time, as in the present study, which therefore reinforces its relevance. The limitation of this study is similar to all the studies that work with secondary data and depend on the good and accurate recording of information. In addition, no studies were found involving all CM of nervous system in the context of spatial and ST analysis.
The findings contributed to the field of public health by revealing the patterns of spatial and ST distribution of CM of nervous system in state of Paraíba, and especially by indicating the regions that must be prioritized for their monitoring. This information can assist public managers in maintaining or expanding the access to health services for this population and may support public policy actions involving maternal and child health.
Among the malformations present in this study, anencephaly and similar malformations stand out for being part of the neural tube defects that are responsible for the greatest proportion of CM of nervous system. However, the incidence of these defects can be reduced with the supplementation of folic acid in the periconceptional period and during pregnancy, mainly in the first quarter. It should be noted that neural tube defects may also be due to other factors, including genetic or multifactoral ones29.
CONCLUSION
This study enabled the detection of the spatial and ST clusters of CM of nervous system in the state of Paraíba, in the period from 2010 to 2016. In addition, it demonstrated the use of a suitable and useful methodology in the analysis of health information in this territory. The findings presented in the study indicate areas that should be prioritized for monitoring of congenital anomalies of nervous system cases, supporting public managers in the decision making process regarding this subject.
Acknowledgments
The authors would like to thank the financial support of Coordination of Superior Level Staff Improvement(CAPES)/Foundation for Research Support of the State of Paraíba (FAPESQ/PB).
REFERENCES
1.Martin RJ, Fanaroff AA, Walsh MC. Medicina neonatal e perinatal: doenças do feto e do neonato. 10 ed. Elsevier, 2016. [ Links ]
2.Sadler TW. Langman: embriologia médica. 13 ed. Rio de Janeiro: Guanabara Koogan, 2016. [ Links ]
3.Silva HMC, Almeida KN, Braga MB, Lago EA, Pessoa LT, Silva IP. Aspectos fisiológicos e sociais associados às alterações cromossômicas e malformações congênitas em gestações perimenopáusicas. Rev Enferm UFPI. 2015;4(1):61-7. [ Links ]
4.Andrade AM, Ramalho AA, Opitz SP, Martins FA, Koifman RJ. Anomalias congênitas em nascidos vivos. Rev Bras Promoç Saúde. 2017;30(3):1-11. DOI: http://dx.doi.org/10.5020/18061230.2017.6309 [ Links ]
5.Canals A, Cavada G, Nazer J. Factores de riesgo de ocurrencia y gravedad de malformaciones congénitas. Rev Med Chile. 2014;142(11):1431-9. DOI: http://dx.doi.org/10.4067/S0034-98872014001100010 [ Links ]
6.Bolla BA, Fulconi SN, Baltor MRR, Dupas G. Cuidado da criança com anomalia congênita: a experiência da família. Esc Anna Nery. 2013;17(2):284-90. DOI: http://dx.doi.org/10.1590/S1414-81452013000200012 [ Links ]
7.Reis LV, Araújo Júnior E, Guazzelli CAF, Cernach MCSP, Torloni MR, Moron AF. Anomalias congénitas identificadas ao nascimento em recém-nascidos de mulheres adolescentes. Acta Med Port. 2015;28(6):708-14. [ Links ]
8.Westphal F, Fustinoni SM, Pinto VL, Melo PS, Abrahão AR. Associação da idade gestacional com a opção pela interrupção da gravidez de fetos com anomalias incompatíveis com a sobrevida neonatal. Einstein. 2016;14(3):311-6. DOI: http://dx.doi.org/10.1590/S1679-45082016AO3721 [ Links ]
9.Departamento de Informática do Sistema Único de Saúde (DATASUS). Informações de saúde (Tabnet). Estatísticas vitais. Nascidos vivos [cited 2018 oct 28] Available from: http://tabnet.datasus.gov.br/cgi/deftohtm.exe?sinasc/cnv/nvuf.def. [ Links ]
10.Cardoso GC, Oliveira MZ, Paixão-Côrtes VR, Castilla EE, Schuler-Faccini L. Clusters of genetic diseases in Brazil. J Community Genet. 2019;10(1):121-8. DOI: http://doi.org/10.1007/s12687-018-0369-1 [ Links ]
11.Magalhães GB. O uso do geoprocessamento e da estatística nos estudos ecológicos em epidemiologia: o caso da dengue em 2008 na região metropolitana de Fortaleza. Rev Bras Geografia Médica Saúde. 2012;8(15):63-77. [ Links ]
12.Goodchild MF. Geographical data modeling. Comput Geosci. 1992;8(4):401-8. DOI: https://doi.org/10.1016/0098-3004(92)90069-4 [ Links ]
13.Lima LMM, Melo ACO, Vianna RPT, Moraes RM. Análise espacial das anomalias congênitas do sistema nervoso. Cad saúde colet.2019;27(3):257-63.http://dx.doi.org/10.1590/1414462x201900030313 [ Links ]
14.Kulldorff M, Nagarwalla N. Spatial disease clusters: detection and inference. Stat Med. 1995;14(8):799-810. DOI: https://doi.org/10.1002/sim.4780140809 [ Links ]
15.Kulldorff M. A spatial scan statistic. Commun Stat Theory Meth. 1997;26(6):1481-96. DOI:https://doi.org/10.1080/03610929708831995 [ Links ]
16.Kulldorff M, Athas WF, Feurer EJ, Miller BA, Key CR. Evaluating cluster alarms: a space-time Scan statistic and brain cancer in Los Alamos, New Mexico. Am J Public Health. 1998;88(9):1377-80. DOI: https://doi.org/10.2105/ajph.88.9.1377 [ Links ]
17.Kulldorff M. Prospective time periodic geographical disease surveillance using a scan statistic. J R Stat Soc Ser A Stat Soc. 2001;164(1):61-72. DOI: https://doi.org/10.1111/1467-985X.00186 [ Links ]
18.World Health Organization (WHO). Epidemiological Alert. Neurological syndrome, congenital malformations, and Zika virus infection. Implications for public health in the Americas. Geneva: 2015. [ Links ]
19.Barreto ML, Barral-Netto M, Stabeli R, Almeida-Filho N, Vasconcelos PFC, Teixeira M, et al. Zika virus and microcephaly in Brazil: a scientific agenda. Lancet. 2016;387(10022):919-21. DOI: https://doi.org/10.1016/S0140-6736(16)00545-6 [ Links ]
20.Schuler-Faccini L, Ribeiro EM, Feitosa IML, Horovitz DDG, Cavalcanti DPC, Pessoa A, et al. Possible Association Between Zika Virus Infection and Microcephaly - Brazil, 2015. MMWR Morb Mortal Wkly Rep. 2016;65(3):59-62. DOI: http://dx.doi.org/10.15585/mmwr.mm6503e2 [ Links ]
21.Groisman B, Gili J, Giménez L, Poletta F, Bidondo MP, Barbero P, et al. Geographic clusters of congenital anomalies in Argentina. J Community Genet. 2017;8(1):1-7. DOI: https://doi.org/10.1007/s12687-016-0276-2 [ Links ]
22.Gili JA, Poletta FA, Pawluk M, Gimenez LG, Campaña H, Castilla E, et al. High birth prevalence rates for congenital anomalies in South American regions. Epidemiology. 2015;26(5):e53-5. DOI: https://doi.org/10.1097/EDE.0000000000000345 [ Links ]
23.Orioli IM, Camelo JSL, Rittler M, Castilla EE. Sentinel phenotype for rubella embryopathy: time-space distribution in Brazil. Cad Saude Publica. 2011;27(10):1961-8. http://dx.doi.org/10.1590/S0102-311X2011001000009 [ Links ]
24.Poletta FA, Castilla EE, Orioli IM, Lopez-Camelo JS. Regional analysis on the occurrence of oral clefts in South America. Am J Med Genet A. 2007;143A(24):3216-27. DOI: https://doi.org/10.1002/ajmg.a.32076 [ Links ]
25.Arroyo LH, Yamamura M, Protti-Zanatta ST, Fusco AP, Palha PF, Ramos AC, et al. Identificação de áreas de risco para a transmissão da tuberculose no município de São Carlos, São Paulo, 2008 a 2013.Epidemiol Serv Saúde. 2017;26(3):525-34. DOI: http://dx.doi.org/10.5123/s1679-49742017000300010 [ Links ]
26.Deng T, Huang Y, Yu S, Gu J, Huang C, Xiao G, et al. Spatial-temporal clusters and risk factors of hand, foot, and mouth disease at the district level in Guangdong Province, China. PloS one. 2013;8(2):e56943. DOI: https://doi.org/10.1371/journal.pone.0056943 [ Links ]
27.Roche LM, Niu X, Stroup AM, Henry KA. Disparities in Female Breast Cancer Stage at Diagnosis in New Jersey: A Spatial-Temporal Analysis. J Public Health Manag Pract. 2017; 23(5):477-86. DOI: https://doi.org/10.1097/PHH.0000000000000524. [ Links ]
28.Olfatifar M, Karami M, Hosseini SM, Parvin M, Moghimbeigi A, Kousha A, et al. Space-time Analysis of Breast Cancer and Its Late-stage Cases among Iranian Women. Iran J Public Health. 2017;46(10):1413-21. [ Links ]
29.Kliegman R, Stanton BMD, Geme JS, Schor NF. Nelson: tratado de pediatria. 20 ed. Elsevier, 2017. [ Links ]
 Correspondence:
Correspondence:
lucianamm_@hotmail.com
Manuscript received: November 2018
Manuscript accepted: March 2019
Version of record online: October 2019


{kind=link}
{kind=link}
{kind=link}
{kind=link}