










Serviços Personalizados
Journal

artigo
 Inglês (pdf)
Inglês (pdf)
 Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
Indicadores
Compartilhar

 Permalink
PermalinkPsicologia: teoria e prática
versão impressa ISSN 1516-3687
Psicol. teor. prat. vol.23 no.3 São Paulo set./dez. 2021
https://doi.org/10.5935/1980-6906/ePTPSP13428
10.5935/1980-6906/ePTPSP13428 ARTICLES
SOCIAL PSYCHOLOGY
Care to the dependent older person: motivations of caregivers in Brazil and Portugal
O cuidado ao idoso dependente: motivações de cuidadores do Brasil e Portugal
Cuidando a los dependientes mayores: motivaciones de cuidadores en Brasil y Portugal
Elaine dos S. SantanaI ; Felismina Rosa P. MendesII; Nádia Cristina M. S. GobiraI; Alessandra S. de OliveiraI; Arianna O. S. LopesIII; Thaiza T. XavierIV; Layanne Christinne dos P. MiguensV; Luana A. dos ReisIII; Luciana A. dos ReisI
; Felismina Rosa P. MendesII; Nádia Cristina M. S. GobiraI; Alessandra S. de OliveiraI; Arianna O. S. LopesIII; Thaiza T. XavierIV; Layanne Christinne dos P. MiguensV; Luana A. dos ReisIII; Luciana A. dos ReisI
IState University of Southwest Bahia (UESB), Vitória da Conquista, BA, Brazil
IIÉvora University, Évora, Portugal
IIINortheast Independent College (Fainor), Vitória da Conquista, BA, Brazil
IVFederal University of Rio Grande do Norte (UFRN), Natal, RN, Brazil
VFederal Institute of Education, Science and Technology of Maranhão (IFET), São Luís, MA, Brazil
ABSTRACT
In an attempt to fulfill care needs to the elderly, the family usually assumes this function. In order to understand the social representations of informal caregivers of Brazilian and Portuguese elderly people about the motivations for care, a qualitative, exploratory-descriptive research was carried out, based on the Social Representations Theory, in which 21 informal Brazilian caregivers and 11 informal Portuguese caregivers of elderly dependents were interviewed. Thematic Content Analysis and QSR NVivo® software were used in the treatment of the data, and the results showed care as the main motivation: family relationships, in which marriage, parenting, and the affections resulting from these relationships led to the function; the negative representation of Portuguese caregivers on the home, as a place of abandonment and action contrary to the cultural norm; and the representation of the elderly as frail and dependent, who, like children, constantly need care and attention.
Keywords: caregivers; seniors; functional dependence; motivations; family.
RESUMO
Na tentativa de suprir as necessidades de cuidado destinado ao idoso, a família comumente é a instituição que assume tal função. Com o objetivo de compreender as representações sociais dos cuidadores informais de idosos brasileiros e portugueses acerca das motivações para o cuidado, realizou-se uma pesquisa qualitativa, exploratória e descritiva, fundamentada na Teoria das Representações Sociais, em que foram entrevistados 21 cuidadores informais brasileiros e 11 cuidadores informais portugueses de idosos dependentes. Utilizaram-se a análise de conteúdo temática e o software QSR NVivo® no tratamento dos dados, e os resultados evidenciaram como principais motivações o cuidado: as relações familiares, em que o matrimônio, a parentalidade e os afetos decorrentes dessas relações conduziram a função; a representação negativa dos cuidadores portugueses sobre o lar como local de abandono e ação contrária à norma cultural; e a representação da pessoa idosa como frágil e dependente, que, assim como as crianças, precisa constantemente de cuidados e atenção.
Palavras-chave: cuidadores; idosos; dependência funcional; motivações; família.
RESUMEN
En un intento por atender las necesidades de cuidado de las personas mayores, la familia suele ser la institución que asume esta función. Para comprender las representaciones sociales de los cuidadores informales de ancianos brasileños y portugueses sobre las motivaciones del cuidado, se realizó una investigación cualitativa, exploratoria-descriptiva, basada en la Teoría de las Representaciones Sociales, en la que 21 cuidadores informales brasileños y 11 informales portugueses Se entrevistó a los cuidadores de ancianos dependientes. En el tratamiento de los datos se utilizó el software de Análisis de Contenido Temático y QSR NVivo® y los resultados se mostraron como las principales motivaciones: las relaciones familiares, en las que el matrimonio, la paternidad y los afectos resultantes de estas relaciones condujeron a la función; la representación negativa de los cuidadores portugueses en el hogar, como lugar de abandono y acción contraria a la norma cultural; y la representación de los ancianos como frágiles y dependientes, quienes, como los niños, necesitan cuidados y atenciones constantes.
Palabras clave: cuidadores; mayores; dependencia funcional; motivaciones; familia.
1. Introduction
The family represents a requirement of the humanization process of great significance, which acts in the mediation of relationships and reproduction of values and customs (Petrini, 2009). According to Sarti (1995), family relationships are governed by an order that crosses the functionality context and is inserted in what the author calls symbolic order.
The existence of strange cultural heritage that characterizes the family as the main source of support to be resorted to in situations of difficulties or illnesses compels the family to act protective of their loved ones because it is expected a position of solidarity from the family institution (Sousa, Mesquita, Pereira, & Azeredo, 2014; Reis & Trad, 2016; Fernandes, 2008). Therefore, the family functions are established based on such properties and are mainly centered on the notion of parenting that involves its members (Passos, 2005; Petrini, 2009).
Thus, the decision to form a new family arrangement is not part of an affective and purely individual determination of the older person or the family but is intensely influenced by cultural, historical, political, and social factors (Melo, Ferreira, Santos, & Lima, 2017). The very shaping of this arrangement runs through complex issues involving family relationships, ties, and the inheritance of a responsibility to care for older family members (Santos, 2010).
Camarano, Kanso, Mello, & Pasinato (2004) indicate two types of family arrangements that are common in Brazilian society: elderly families, in which they exercise the role of head and, in most cases, are autonomous; and families with elderly people, where they are most vulnerable and in need of care. In both arrangements, the elderly's income contribution represents an important resource for the family budget. Data from the National Household Sample Survey conducted in 2010 confirm this reality and present what can be called the new role of the elderly in society.
Another frequent feature of this new family organization is related to the increasing trend towards multigenerational family arrangements (Herédia, Casara, & Cortelletti, 2007; Silva et al., 2014). Multigenerational homes are spaces for exchanging knowledge and experiences, but they also constitute an environment of divergences and overload, which can compromise both the relationships established between their members and the quality of care provided to the elderly (Pedreira & Oliveira, 2012).
Intergenerational relations in the family occur from three domains that function in a complementary way: the affective, normative, and instrumental domains (Santos et al., 2016). The affective domain corresponds to the affections given throughout life; the normative domain is related to the values, customs, and rules that its members share; and the instrumental domain refers to the support exercised by the family institution, whether as economic support or even in carrying out domestic chores and care waiver (Brito et al., 2017).
The family, seen as an organizational segment of human beings, also functions as an ideological object and stereotype that potentiates certain types of social control and subordination of its members. However, the existence of an organizational structure does not necessarily guarantee quality in relationships. It is possible to find families with the same composition but with different dispositions (Meira, Vilela, Casotti, Nascimento, & Andrade, 2015; Melo et al., 2017).
In Brazil, spouses and children are the main relatives to take care of their older relatives. The spouses are assigned the responsibilities for the closeness and the sealed alliance with the marriage, being for them an obligation to take care of his/her companion. In the relationship with the sons, and, in this case, mainly the daughters, who represent an expressive majority, the conventions of filial piety, gratitude, and obligation to return the care received in childhood prevail (Lima, 2018; Manoel et al., 2013).
In Portugal, the support offered by the family, called informal, represents the main affective and effective support of the elderly (Mocelin et al., 2019). In their work, Pimentel & Albuquerque (2010) and Paúl (1997) pointed out the role of the family when it comes to elderly care, especially in daily activities and in psychological and social support. This direction towards the family sphere is strongly influenced by the concept of provident society, a historical and cultural condition rooted in the social imagination, especially in rural communities, where the feeling of obligation and ethical imposition is commonly shared (Pimentel & Albuquerque, 2010).
The determination of family roles in social policies and in the legislation itself has been modified over the periods (Camarano & Barbosa, 2016). Despite an increase in formal support network services in European Union countries, the support offered by the family is still strongly pointed out by surveys (Dias, 2015).
José (2012) highlights a condition of "implicit familialism" in the Portuguese reality. This premise justifies the accountability of care, as "the family is [...] a guarantee of solidarity [...] between generations" (Xavier, 2010, p. 363). In this sense, Ramos (2005) defends the idea that taking on family care can be something learned, as he observed that, in families who took care of previous generations, this experience worked as an example to be followed. An example of influence in the universe of care is demonstrated by a popular saying transmitted in the communities: "you are children, father you will be, as you do, so you will find" (Ramos, 2005, p. 203).
In this sense, the investigations around home care help unveil an increasingly frequent reality that is not always evidenced by society. As a valuable tool for unveiling the reality of confrontations and circumstances that involve the experiences of informal caregivers, the results of research of this nature can help create alternative support for the elderly and caregivers and also construct social and health policies that meet their real needs.
Therefore, the present study aims to understand the motivations of informal caregivers of older adults with functional dependency in Brazil and Portugal to assume this care.
2. Method
This is an exploratory-descriptive study with a qualitative approach based on the Social Representations Theory of the social psychologist Serge Moscovici (2007). The study's scenario consisted of two programs of assistance to the elderly: the Municipal Home Care Program for the Elderly with Limitation (in Portuguese, Programa de Atendimento Municipal Domiciliar ao Idoso com Limitação - PAMDIL) in the municipality of Vitória da Conquista, in the state of Bahia, Brazil; and the Integrated Community Care Team (in Portuguse, Equipa de Cuidados na Comunidade Integrados - ECCI) in the municipality of Évora, in the Alentejo region, Portugal.
The city of Vitória da Conquista, the third-largest in the state, with about 306.866 inhabitants, corresponds to the health center of the southwest region, serving 72 municipalities in the state of Bahia and northern Minas Gerais (Instituto Brasileiro de Geografia e Estatística, 2010). Currently, the PAMDIL has two teams, formed by two doctors, two nursing techniques, and a driver, and benefits the population of seven health units in the municipality (Vitória da Conquista, 2018).
Of the seven units covered by the program, four Family Health Units were chosen to develop the research. The other units were excluded due to violence in the neighborhoods where they were, which could compromise the access and security of the researcher.
The city of Évora in the Alentejo region is also the capital of the district of Évora, composed of 14 municipalities and has 53,084 inhabitants. Alentejo is considered the oldest region in the country, and the proportion of older adults per 100 young people in the city of Évora is 161.6 (Pordata, 2018).
The Integrated Community Care Team (ICCT) works as a full-time follow-up service for patients, mostly elderly, and is composed of a multidisciplinary team that serves 25 patients and is formed by six nurses, a physical therapist, a nutritionist, an occupational therapist, a psychologist, a social worker, a speech therapist, an administrative assistant, and a driver. They all provide comprehensive medical and nursing care, rehabilitation, and social support in the home environment as needed by the patient and the necessary support to the family caregiver.
The full support provided by the ICCT has a 24-hour service, 12 hours for face-to-face assistance, and 12 hours for the support provided over the phone.
The participants in the study were informal caregivers of older adults with functional dependency in Brazil and Portugal, 21 were Brazilian family caregivers, and 11 were informal Portuguese caregivers. The inclusion of family caregivers was due to having some degree of kinship with the elderly, living in the same household, being over 18 years of age, without restriction as to gender or marital status, and that they were primarily responsible for caring for the elderly and not receiving remuneration for care.
The first stage began with identifying the elderly population registered in the program, and from the records, a database with 781 addresses was prepared. In the four units chosen, 251 addresses were registered, and 176 effective visits were identified. In 23 houses visited, the elderly had died and, therefore, were excluded from the research. Another 52 elderly individuals were excluded after visiting because they did not live at the indicated address, refused to participate in the study, or because they did not respond after three attempts, thus remaining 101 households.
The second phase of data collection took place between January and March 2018. After applying the inclusion and exclusion criteria, the 21 caregivers of the elderly were selected to follow up the research by applying the interview.
Stage two of the research was carried out in Évora. Initially, there was an approximation with the elderly population through an initiative proposed by the ICCT, and after monitoring the team's activities, visits were scheduled for the interview. The ICCT treated 25 patients in the period, of which 17 were seniors. At the end of the stage, the participants totaled 11 caregivers of the elderly, because, during the period, there was one death, two refusals, and three unsuccessful contact attempts.
Data collection was carried out through the open interview with guiding questions, based on a script composed of fourteen questions related to the routine of care and caregivers' conceptions regarding care. The questions sought to explore the daily activities developed by caregivers in providing care to the elderly and how this process was done.
To analyze the information collected, we used the Content Analysis proposed by Laurence Bardin with the help of QSR software NVivo® version 11. Content Analysis consists of a set of communication analysis techniques, and, according to Bardin (2009), through this technique, it is possible to deal with the information contained in the messages and thus achieve an exploration of both meanings and signifiers.
This technique comprises three phases and is organized in three chronological poles: pre-analysis, exploitation of the material and treatment of the results, and inference and interpretation. The Nvivo® QSR is a software that assists in the organization and structuring of the data. Through the organization of the information collected with the interviews, Nvivo® enables a kind of categorization, in which the descriptive information of the text is arranged from the identification of trends and, through this structuring, "nodes" and "subnodes" are created and, later on, the word clouds with the words most frequently cited by the participants. This feature enables better visualization of categories as well as representing modern tool that contributes to content analysis.
Both studies were submitted and approved by the Research Ethics Committees. The Brazilian Project was approved by the Research Ethics Committee of the State University of Southwest Bahia with the number 1.875.418 of 8/15/2016; and the Portuguese project was approved by the Health and Welfare Ethics Committee of the University of Évora with the number 16012 of 05/19/2016.
3. Results and Discussion
Figure 3.1 presents a profile of the research participants based on the sociodemographic data collected.
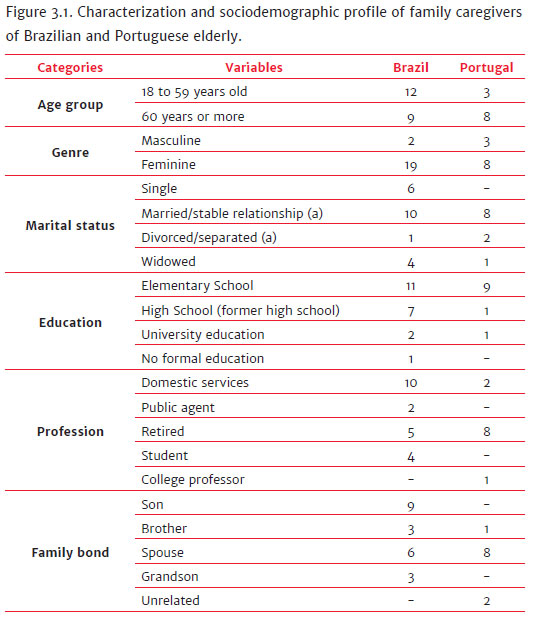
When asked about the process that led them to assume the role of caregivers, the participants demonstrated that affective ties represent one of the main motivations.
It is possible to notice words like "years", "married", "home", "house", and "husband" with great emphasis, which represents the high frequency of evocations by the Portuguese caregivers. The prominence of these words demonstrates once again the importance of bonds in the care process and, as in the case of Portuguese caregivers, who were mostly spouses, how this condition assumes a determining character.
According to Lage and Araújo (2014), the responsibility in the care process is given by the existence of a relationship of closeness built throughout life, which in most cases is based on material and moral reciprocity.
This reality is quite common in the Portuguese scenario, even where there are formal support networks available, because there is a cultural determination that gives generations the obligation to manage efforts and resources for the care of elderly members (Araújo, Paúl, & Martins, 2011; Wall, 1995). Martins (2013) and Andrade (2009) certify that the motivations of caregivers also vary according to the degree of the relationship, as it was possible to verify in their studies that the sentimental relationships and the sense of obligation were more present in the reasons assigned by children and spouses, while the supportive nature of the family justified the care of brothers.
It is noteworthy the elements "aged", "created", "reciprocating", "family", "child", among others. The words that emerged from this cloud are similar to the findings in the cloud of words of the Portuguese caregivers and confirm not only what the literature has pointed out regarding care and family relations, but also the approximation between the realities of the two countries.
In Brazil, the co-residence is a widely used alternative and is usually associated to financial issues and cases of health problems of the elderly or death of the spouse, in which adult children take responsibility for elderly parents and thus exercise a type of mutual assistance (Silva et al., 2014; Pedrazzi et al., 2010).
In a study with family caregivers of elderly dependents in the city of Londrina, Manoel et al. (2013) noted that the family was not always organized to assume the role of caregiver and as the difficulties were perceived, the integrated organization of the members took place. The study also concluded that lifelong relationships might be determinant in the quality of interactions after the establishment of the disease.
To better explore the representations pointed, three categories emerged: "Familiar relationship", "Social Representations about nursing homes", and "Social Representations about old age".
The discussion presented in this section is related to the cloud of words, already mentioned and also includes the speeches of caregivers of the elderly who were, from then on, named by the acronyms BC (Brazilian caregivers) and PC (Portuguese caregivers).
3.1 Familiar relationship
This category shows how care is permeated by relationships and affections. The sense attributed to care by many people is associated with the ability to develop relationships and awake this experience from such experience (Brito et al., 2017).
Care is an expression of the relationship with the other, in a significant and engaging way, guided by patience, by concern. Through the sense of value, the reciprocity, complementarity, and otherness necessary to exercise care arise (Almeida et al., 2012). However, this family solidarity is identified as a characteristic that allows for intergenerational exchanges of care based on the members' level of cohesion. Therefore, in some families, these aid transfers will work better than in others, as their performance approaches the quality of the networks that were built during life (Lemos, 2013; Guerra, Almeida, Souza, Minamisava, & Tobias, 2017).
That said, it reaffirms the social construction that determines the family as the source and main place of support, since it corresponds to the first socializing institution in which the individual is inserted, constituting a place of arrival, permanence, and departure of each human being (Manoel et al., 2013). In both the Brazilian and the Portuguese realities, the family takes care of elderly family members, both in providing basic needs such as housing, food, and personal care, as well as in providing care, love, and the possibilities of communicating and favoring the sense of belonging (Santos et al., 2016; Rodrigues & Martins, 2014).
Similar perceptions were also found in the research, as can be verified in the statements of caregivers who denote how responsibility occurs due to family ties:
We've been married for 53 years, right? People who don't get along don't last that long, right? (PC1)
And I will continue to do so. We have been married for forty years, and she has been incapacitated for 20 (PC3).
The statements of the Portuguese caregivers presented above reflect how marriage is a determining factor in their care. It is important to note that most of the Portuguese participants were spouses of the elderly who provided care, which justifies the expressiveness of this bond.
Many authors approach the existence of a responsibility that falls on the spouse (Lima, 2018; Melo et al., 2017). What these studies reveal is actually a sense of obligation to care determined by marriage, a culturally pre-established hierarchy (Manoel et al., 2013; Braz; Ciosak, 2009), which is ratified by the studies by Cattani and Girardon-Perlini (2004) and Mendes (1995) by pointing out the centrality of the designation of the caregiver based on four rules: kinship, gender, physical proximity, and affective proximity.
It is important to explore the gender element, considering that, although it is possible to observe a movement of change over the years, this has been an almost exclusively female reality. The characterization of caregivers evidenced by Brazilian and Portuguese research leaves no doubt that there is an expressive majority of female caregivers.
The femininization of care is the main characteristic pointed out in the literature. Several investigations with informal caregivers present this reality in their results (Almeida, Meneses, Freitas, & Pedreira, 2018; Fernandes, Margareth, & Martins, 2018; Vaz et al., 2018). Women represent an expressive majority in the responsibility of care, because of the inclination to attribute to them the role of caregiver that has been transmitted over time.
What many studies highlight is that thinking about the care of the female figure is not only associated with maternal love, but also with religious precepts of obedience and filial duty that direct interactions and meanings in relationships (Meira et al., 2015; Lima, 2018).
Thus, it is common that the decision of caring is influenced by the bonds (matrimonial or filial), but also by the feeling of gratitude, which is a way to repay what was received in childhood, for example, or because they judge that they have no alternatives, either because of lack of support or because they do not consider asylum an option, as can be confirmed by the following statement:
I don't have the guts... Sometimes they ask, "Why didn't you get him in a nursing home?" and I'm not able to do it, because he was a person who helped me so much in life, and was a father always present, he was in France for a long time, but was always very present, so as long as he needs me and I can do it, I will have him there in the nest. My husband keeps saying, "I give you a heart of pain... and you're the best thing for me" because he knows I've been the only person. To my husband I say that God put him in my way because maybe He knew he would need me so much. Because I'm already with him, I started dating him when I was 15 years old. Today I am 68 "you know?", we dated nine years and we've been married for 45. So I mean... sometimes he and my dad say, "If it was anyone else, she'd have left already". But then if God gave him to me, maybe it was because I was able to care for him (PC4).
Discourses like this confirm the notion defended by Halbwachs (2006) of how memories cannot be separated from social frameworks. The memories that emerged from the participants announce elements considered important for their subjective well-being, justifying the decision of care from the good feelings that were experienced and cultivated even before the condition of dependence.
This sense of value and subjective well-being can be observed in the words of the caregivers:
I feel extremely good. You know what it's like to be able to take care of your mother, who is an old person. So it's very rewarding (BC1).
She took care of me since I was born. Then when she started getting sick, it was already in routine... Ah, she is my mother (BC6).
These speeches allow us to recognize that, despite the difficulties in providing care, this experience becomes strongly motivated by gratitude, because caregivers find in this feeling a positive dimension to do so (Meira et al.; 2017; Brito et al., 2017).
The findings revealed in the research agree with a study which investigated the social representations of family caregivers of older adults and found that the act of caring was closely linked to the feeling of gratitude for the care received in childhood performed by the elderly (Floriano, Azevedo, Reiners, & Sudré, 2012).
Meira et al. (2017) highlight how this feeling of gratitude acts as a motivating element for care. It is also important to highlight that Christian traditions and values are esteemed and transmitted to generations as guiding principles of conduct in Portugal and Brazil. The very belief that responsibility for care is a design of God, as seen in the speech of one of the participants, demonstrates how there is a moral-religious influence around this process and how, at the same time, the function of caregiver constitutes a hope of future retribution and recognition (Reis & Trad, 2015):
Look, child, my life was a little complicated because my father was a baker, he had a bakery, my brother and I worked there and I left two years ago, but he continued working nights, used to come to my house in the middle of the night to see how my father was doing, and that's how I did it. And my life was like that, it wasn't easy, but I think I did my duty. God knows, but I think I did (PC10).
Thus, Lima (2018) points out that, by assuming responsibility in caring, there is an inclination to reciprocate the affections and the exercise of a practice that will serve as a good example to children, in an attempt that they will also be called upon to take care when requested, as can be verified in the speech below:
I think it's just an exchange of favors. We were taken care of by the elderly, it's more than an obligation to take care of our elders now. Now I'm taking care of my son, my son is one year old. But if you have love for your family and were raised with a solid upbringing to take care of each other, I don't think that's even necessary, because it's a matter of love anyways. I think that's how I had more awareness. Even awareness of the meaning of life. There are times when we are very superficial, when we think that life is only about taking care of you, that it's just a party. And actually, it's not. I think that's what life is. It's about taking care of each other, helping each other when necessary. Before, I had a more selfish vision, and today I don't, it is different (BC7).
Several studies developed with this theme corroborate this thought, pointing out that gratitude actually emerges in the speeches of individuals as an abstract form of moral and ethical experience (Santos et al., 2016; Lima, 2018). Among the representations that emerged from the participants' discourses, moral obligation was one of the main motivations for establishing care.
It is understood that the designation of the caregiver may result from the establishment of four factors that are organized according to the particularities of each situation: degree of kinship, gender, physical proximity, and emotional closeness (Rodrigues, 2014); but these elements are not always able to sufficiently express and represent the motivations of a caregiver, either because such factors do not occur in this way in their homes, or because the constructions of individuals do not enclose themselves in them.
3.2 Negative social representations about nursing homes1
The social representations evidenced in this category demonstrate how the social construction around institutionalization greatly influences the decision to care. For the participants, the meanings and memories evoked around this dynamic are often associated with abandonment and fall into the blaming process fueled by cultural, historical, and moral factors already mentioned in the previous category.
Only Portuguese caregivers expressed speeches related to this representation, which leads us to infer the paucity of such structures within the Brazilian reality.
Gil (2007) elucidates that, despite the encouragement of care in the family environment within the Portuguese scenario, there are still few policies that legitimize such practices, whether through financial support or other types of assistance such as flexible working hours and leaves for care. In addition, some responses provided by formal support networks are still limited considering the high demand in relation to the number of existing vacancies, the criteria established for service, and the value of services that cannot always be paid for by the family (José, 2012; Pimentel, 2012).
According to Meira et al. (2017), each culture has its vision of old age and how societies are organized to deal with the population's needs in this age group. Care circumstances permeate feelings, relationships, closeness, as previously discussed, and especially memories.
Halbwachs (2006) defends an idea of total reciprocity of memory, which is supported by the premise of the interaction between individual memory and collective memory. When the subject remembers, he/she is situated in the group's point of view, and the memory of a single person thus manifests the group memory.
Therefore, it is possible to verify how memories influence the constitution of representations. Although a certain fact has not been experienced directly, the representations anchored in the group's memories allow this individual to assign a sense of value and position.
The speeches raised in this category reveal how the participants' memories greatly influence their decision-making. Anchored in the memories and representations seized throughout life, the caregivers justify caring from a negative judgment attributed to institutionalization, as the statements:
My conscience hurts because we know what nursing homes are like. We know that every person is a person, working in these places there should only be people with real vocation, but people go to earn money. And it is not with vocation, and some have a heart of flesh while others have a heart of stone. And then it's not really seeing, because we're not there, but it's hearing the people who are there (PC4).
Now what we know is that the elderly go to homes and that there are homes that are more careful with their elderly than others, this is quite true. I even registered her in many homes, because each home is different. Home is the last stop, and I still have a lot to think about when it comes to homes (PC3)
Now, if you ask me, obviously, between her being here at home with me, or with someone I know, or with my parents or in a nursing home, the last place she would go is a nursing home, regardless of the professionalism of these people (PC7).
My son's wife wanted my husband to go to a home when he left the hospital, but I didn't want it. He won't go and when he goes I'll go with him because I want to see what they do to him. I know what it looks like, and I'm not into it and I don't want to see him mistreated (PC11).
Institutions for the elderly have undergone many changes over the years in societies, but some conceptions that are related to historical influences are still very present today.
The origin of homes for the elderly is linked to spaces for sheltering the elderly, people with mental illness, and marginalized people. Some authors point its genesis to the 16th century in Europe, others already draw attention to the 10th century in England in the Middle Ages, when some houses were built near the monasteries, named almshouse, to provide charity and hospitality to people, including the elderly (Fernandes, 1997; Christophe; Camarano, 2010). Due to this historical trait, institutionalization is often understood as something negative, commonly attributed to abandonment and poverty, a space where old age is sad and lonely.
In 2012 there were about 2,093 facilities with capacity to house 79,997 elderly people, which corresponded to 4% of the population over 65 years of age. According to data from the Social Report of the year 2018 there are, in the District of Lisbon, 393 facilities with 13,405 users and a total capacity of 15,320. Also according to the same report, the district of Évora has 99 equipment and 3.136 registered users (Social Charter, 2018).
Data from IPEA (2012) identified 3.548 institutions in the Brazilian territory with 83.870 elderly residents, corresponding to 0.5% of the Brazilian older people population. These institutions cover only 28,9% of the Brazilian municipalities, and, according to the IPEA survey, most institutions are philanthropic, although a considerable growth of private profit-making institutions has been observed in recent decades (Camarano & Barbosa, 2016).
It is possible to verify with the data presented of the two countries that, despite the increasing supply, institutionalization is a resource not always considered. As regards the Portuguese reality, studies justify that, like other countries in southern Europe, such as Italy and Spain, institutionalization in Portugal ranks third in the social responses sought, because the family is still very present in the care of the elderly (Sousa et al., 2014; Rodrigues & Martins, 2014).
This sense of rejection of institutions has been observed by many authors (Pinto, Barham, & Albuquerque, 2013; Mocelim et al., 2019). The negative view reported by the caregivers and confirmed in the studies is commonly associated with the stigmatization of nursing homes and the centrality of the family in care. Some authors highlight how these spaces can violate the individualities of the elderly, often in the removal of the autonomy of their belongings, their time and space being controlled by the institution's administrative decisions (Camarano & Barbosa, 2016; Reis and Trad, 2015).
The stigmatization attributed to the institutions reflects the historical influence of their purpose and target audience of origin, since these spaces were intended for marginalized poor people, who had no relatives to whom they could turn, and this is the idea that persists in the social imaginary until the present day. The studies and the caregivers' own statements demonstrate how old age in an institution is perceived as sad and abandoned, which generates in the elderly low self-esteem and feeling of isolation (Fernandes, 1997; Born & Boechat, 2002).
Thus, home care is valued, mainly by enabling and preserving the intimacy of the elderly in a space that is already known and which the elderly can identify, representing an emotional symbolism of great value (Meira et al., 2015; Mocelim et al., 2019). This symbolism means that the elderly commonly recognize their space as a bearer of stories, where the memories of a life are located, and therefore tend to refuse the idea of going to live in an institution if they are offered another possibility (Manoel et al., 2013).
Moreover, associated with this is the premise discussed in the previous category, which dealt with the family obligation to care for their loved ones, whether for charity, gratitude, or even moral obligation. There is a feeling of guilt and failure often revealed by family members who need to send the elderly to live in an institution that can be justified by the negative moral perception of the act or by negative experiences experienced by others that lead them to think the same way (Mocelim et al., 2019).
There is a family tendency to retain care, especially when it comes to older spouses. In her research, the author demonstrates how it is common for caregivers to manifest the desire to have health and conditions to keep the elderly under their care at home, which is also manifested by the statements of caregivers presented in this category (Almeida et al., 2012).
Therefore, the search for housing in an institution is mainly due to the difficulty of the elderly in ensuring self-care, either by the high degree of dependence or by the impossibility of help in the care of widowhood, disability of the family, or financial conditions that do not make it possible to hire formal home caregivers (Brito et al., 2017; Camarano; Barbosa, 2016).
It is important to highlight that the changes in family organization and the growing needs associated with the high number of elderly in the population, both Portuguese and Brazilian, constitute a movement for reflection of public policies and the devices made available to support the caring family and the elderly, since, although long-term institutions for the elderly are more present in the Portuguese reality, the representation of institutions as spaces of abandonment, violence and waiting for death is shared by both countries.
In addition, the different support needs (instrumental, financial, and psychoemotional) illustrate not only inequalities in supply and access to social responses between countries, but they mainly denounce the urgency of discouraging stigmata and prejudices around long-term institutions, expanding their access, as well as inciting critical thinking for the implementation of an effective care network and informal support.
3.3 Social representations about old age: "becoming a child"
This category explores the decision of caregivers based on the social representations of old age as a phase of dependence and care demands similar to the childhood. The discourse of the caregivers at this moment shows how old age is still a stage seen from many prejudices, and one of these is this sense of infantilization that tends to take away from the elderly their autonomy.
By revealing the meaning of old age and childhood as phases that require greater care, attention, supervision, and accountability, caregivers reproduce and nurture the representations that commonly result in negative consequences, but which, for them, assume the character of the main motivation for care.
Beauvoir (1990) presented in her work how old age was seen by various societies, primitive, and civilized, and found that, despite the eccentricities with which the collectives treated their elderly, there was a common tendency to approach old age from childhood, as an attempt to explain and deal with the extreme stages of life.
Halbwachs (2006) argues that it is not possible to think in collective memory without looking at the social plane that anchors such memories, and also points out that the representations built in the present are given by the organization of the sense of the past established from the social frameworks. That is, the cohesion guaranteed by the social frameworks of memory aggregates the groups, be they of class, religious or family, and imputes a system of values to the social ties formed by them.
In this sense, the contents of the memory are not limited to a reproduction of the past, but rather representations constructed from it and added to the exchanges and experiences established with other groups, allowing the memory not to be limited by what was lived, but accumulating from the sum and modifications of the experiences lived (Reis & Trad, 2015). Therefore, the meanings attributed by caregivers to care in the old age phase as a condition similar to childhood reveal how the past acts in the memories of individuals, while it is updated in the present as a function of social representations.
The premise exposed by the caregivers resumes the thought pointed out by Beauvoir (1990), and is anchored in the idea of unproductivity associated with the two phases. The older people and children are free from social pressures and can thus distance themselves from the issues and problems of an adult life, and this is where the similarities are centered, as noted in the following statements:
As children, it's the same thing because in Alentejo, ' any garlic peel hits a child' (CP8).
Elderly for me is like a child. That when you get old you go back to being a child, right? Then you have to be more careful still (BC2).
Especially elderly, who becomes a child again (BC8).
Elderly for me is like a child. When you get older, you really go back to being a child. That's why the person needs care because the child also needs it (BC16).
The perceptions revealed in the speeches of the caregivers are anchored in the memories of an intersubjective past, but also recalled and shared in the collective, since the origin of every individual memory is the social, and to remember his/her past every individual anchors it in the reminiscences and in the figures of others (Halbwachs, 2006).
Scientific productions involving the elderly have progressively discussed discrimination with old age and the circumstances surrounding this phenomenon. The elderly have been reserved a range of stereotypes that disqualify them, limit them and remove much of their autonomy (Sousa et al., 2014; Santos et al., 2016), and some studies have reported infantilization.
Almeida et al. (2012), seeking to know the dynamics of care provided by informal caregivers to older adults with functional dependency, found similar results to the findings of this research. The infantilized perception of the elderly by the caregiver was justified by the physical dependence of the elderly to perform basic daily activities, including the demonstration of feelings of resistance or stubbornness in the face of care.
What the literature discusses is how this trend assumes a harmful character in two ways, both in the performance of the caring function, when feeding the discourse of stigmatization of the elderly, and in the developments of this idea that can culminate in the practice of abuses, from the most subtle to the most flagrant (Meira et al., 2015; Santos et al., 2016).
One of the main negative implications of infantilization of the elderly in the development of care practices is the withdrawal of their autonomy. When comparing the elderly to children, caregivers disregard their intellectual capacity, and commonly insert in their treatment a paternalistic language, often with infant expressions, which are justified as a strategy to facilitate communication and, yet, they result in a depreciation of the elderly's ability to understand (Sousa et al., 2014; Lima, 2018). Thus, the real capacities of the elderly are devalued, which implies the commitment of their recovery potential and the promotion of effective social and health responses (Brito et al., 2017), in addition to undermining the principles established by the National Health Policy for the Elderly that guides the practice of care from the promotion of autonomy and independence of the elderly.
The second implication related to the discrimination against older people through this tendency to infantilize them is associated with signs of abuse and ill-treatment. Lima (2018) and Santos et al. (2016) show in their studies, as much in Portugal as in Brazil, that this practice is quite common, but not always recognized by caregivers as a form of abuse, since in both, the literature and society itself, the subtle forms of abuse tend to be undervalued.
Thus, it is possible to notice that there is a tendency to bring old age closer to childhood on the part of elderly caregivers, especially when referring to the meaning of care and the norms that govern this process.
4. Conclusion
In the analysis of the motivations for care revealed by the relatives of the elderly, it was possible to verify that the family relationship is one of the main reasons for individuals to take care of their elderly relatives. In response to the influence of historical, moral, and even religious factors, caregivers revealed a strong sense of responsibility for care as a continuation of a social tradition.
The circumstances surrounding this decision permeate the conception of the roles of members in the family and in social spaces, which have been built and assigned over the years. When assuming the role of caregiver, family members were also concerned with responding to expectations regarding the place and condition of the elderly in society, and the roles assigned to them by marriage or parenthood.
The social representations evidenced by the research also showed how the memories of individuals feed and reinforce such representations, whether in the moral, historical, religious convention that defines the family as an institution of care, or even in indirect circumstances, as in the case of the negative view around the homes for the elderly and the institutionalization process as an alternative for directing the same conduct and practice.
As a research limitation, the sample size stands out, which, despite expressing a concrete reality and which has been constantly confirmed by other studies, had a small number of participants.
However, studies of this nature constitute an important contribution to the understanding of practical points and subjectivities that surround the reality of elderly care. Knowing the position and coping strategies of the family in articulating this assistance is an increasingly accentuated need, considering the age profile of today's society.
Thus, when going through the care references and exploring the stimuli and circumstances of this context, it is noted how some assumptions conceived in the past still induce and inspire behaviors in the present and can favor the reproduction of stereotypes that affect both the quality of life of the elderly and their family caregivers, and also how much it hinders the strengthening of the support network, whether through informal or formal care agents.
References
Almeida, L., Azevedo, R. C. de S., Reiners, A. A. O., & Sudré, M. R. S. (2012). Cuidado realizado pelo cuidador familiar ao idoso dependente, em domicílio, no contexto da estratégia de Saúde da Família. Texto & Contexto - Enfermagem, 21(3),543-548. doi: 10.1590/S0104-07072012000300008 [ Links ]
Almeida, L. P. B., Meneses, T. M. O., Freitas, A. V. S., & Pedreira, L. C. (2018). Características sociais e demográficas de idosos cuidadores e motivos para cuidar da pessoa idosa em domicílio. REME Rev. Min. Enferm, 22,e-1074. doi: 10.5935/1415-2762.20180004 [ Links ]
Andrade, F. (2009). O cuidado informal à pessoa idosa dependente em contexto domiciliário: Necessidades educativas do cuidador principal (Dissertação de Mestrado não Publicada). Universidade do Minho, Braga. [ Links ]
Araújo, I., Paul, C., & Martins, M. (2010). Cuidar no paradigma da desinstitucionalização: A sustentabilidade do idoso dependente na família. Revista de Enfermagem Referência, 2,45-53. [ Links ]
Bardin, L. (2009). Análise de conteúdo. Lisboa: Edições 70. [ Links ]
Beauvoir, S. (1990). A velhice. Rio de Janeiro: Nova Fronteira. [ Links ]
Born, T., & Boechat, N. (2002). A qualidade dos cuidados ao idoso institucionalizado. In E. V. Freitas & F. Chaimowicz (Orgs.), Tratado de geriatria e gerontologia (pp. 768-777). Rio de Janeiro: Koogan. [ Links ]
Braz, E., & Ciosak, S. I. (2009). O tornar-se cuidadora na senescência. Esc. Anna Nery Rev. Enferm.; 13(2),372-377. [ Links ]
Brito, A. M. M., Camargo, B. V., Giacomozzi, A. I., & Berri, B. (2017). Representações sociais do cuidado ao idoso e mapas de rede social. Liberabit, 23(1),9-22. doi: 10.24265/liberabit.2017.v23n1.01 [ Links ]
Camarano, A. A., & Barbosa, P. (2016). Instituições de longa permanência para idosos no Brasil: do que se está falando? In A. O. Alcântara, A. A. Camarano, & K. C. Giacomin (Eds.), Política nacional do idoso: Velhas e novas questões (pp. 479-514). Rio de Janeiro: Ipea. [ Links ]
Camarano, A.A., Kanso, S., Mello, J. L., & Pasinato, M. T. (2004). Famílias: espaço de compartilhamento de recursos e vulnerabilidades. In A. A. Caramano (org.), Os Novos Brasileiros: muito além dos 60? (pp. 137-167). Rio de Janeiro: IPEA. [ Links ]
Cattani, R. B., & Girardon-Perlini, N. M. O. (2004). Cuidar do idoso doente no domicílio na voz de cuidadores familiares. Revista Eletrônica de Enfermagem, 6(2). [ Links ]
Christophe, M., & Camarano, A. A. (2010). Dos asilos às instituições de longa permanência: Uma história de mitos e preconceitos. In A. A. Camarano (Org.), Cuidados de longa duração para a população idosa: um novo risco social a ser assumido? Rio de Janeiro: Ipea. [ Links ]
Dias, I. (2015). Família e envelhecimento: O estatuto dos idosos. In I. Dias, Sociologia da família e do gênero. Lisboa: Pactor. [ Links ]
Fernandes, A. A. (1997). Velhice e Sociedade: Demografia, Família e Políticas Sociais em Portugal. Oeiras: Celta Editora. [ Links ]
Fernandes, P. M. (2008). O idoso e a assistência familiar: Uma abordagem da família cuidadora economicamente dependente do idoso. Revista Eletrônica Novo Enfoque, 7(7). Retrieved from http://castelobranco.br/sistema/novoenfoque/edicao/artigos/7 [ Links ]
Fernandes, C. S., Margareth, Â., & Martins, M. M. (2018). Cuidadores familiares de idosos dependentes: Mesmas necessidades, diferentes contextos-uma análise de grupo focal. Geriatr., Gerontol. Aging, 12(1),31-37. [ Links ]
Floriano, L. A., Azevedo, R. C. de S., Reiners, A. A. O., & Sudré, M. R. S. (2012). Cuidado realizado pelo cuidador familiar ao idoso dependente, em domicílio, no contexto da estratégia de Saúde da Família. Texto & Contexto Enfermagem, 21(3),543-548. doi: 10.1590/S0104-07072012000300008 [ Links ]
Gil, A. P. (2007). Envelhecimento activo: Complementariedades e contradições. Presented in Forum Sociológico. Série II. CESNOVA. [ Links ]
Guerra, H. S., Almeida, N. A. M., Souza, M. R., Minamisava, R., & Tobias, G. C. (2017). Qualidade de vida dos cuidadores de um serviço de atenção domiciliar. Rev. enferm. UFPE on line, 11(supl. 1),254-263. [ Links ]
Halbwachs, M. (2006). A memória coletiva. São Paulo: Centauro, 2006. [ Links ]
Herédia, V. B. M., Casara, M. B., & Cortelletti, I. A. (2007). Impactos da longevidade na família multigeracional. Revista Brasileira de Geriatria e Gerontologia, 10(1),7-28. doi: 10.1590/1809-9823.2007.10012 [ Links ]
Instituto Brasileiro de Geografia e Estatística. (2010). Cidades IBGE. Retrieved from https://cidades.ibge.gov.br/brasil/ba/vitoria-da-conquista/panorama [ Links ]
Instituto de Pesquisa Econômica Aplicada (2012). O Conselho Nacional dos Direitos do Idoso na visão de seus conselheiros. Relatório de pesquisa. Projeto Conselhos Nacionais: perfis e atuação dos conselheiros. Brasília: Ipea. Retrieved from http://www.ipea.gov.br/agencia/images/stories/PDFs/relatoriopesquisa/120409_relatorio_direitos_idoso.pdf [ Links ]
José, J. S. (2012). A divisão dos cuidados sociais prestados a pessoas idosas: Complexidades, desigualdades e preferências. Sociologia, Problemas e Práticas, 69,63-85. [ Links ]
Lage, M. I. G. S., & Araújo, O. (2014). A experiência de cuidar um idoso dependente em contexto familiar. Presented in the 3º Congresso Ibero-Americano em Investigação Qualitativa. Ludomedia-Conteúdos Didácticos e Lúdicos (pp. 238-244). [ Links ]
Lemos, C. E. S. (2013). Entre o Estado, as famílias e o mercado. Velhice, família, Estado e propostas políticas, 8(22),1-152. [ Links ]
Lima, A. A. (2018). Eu cuido de você... E você, cuida de mim? Um olhar sobre o cuidado por idosas que moram sozinhas (Tese de doutorado). Universidade Estadual Paulista "Júlio de Mesquita Filho", Botucatu, SP, Brasil. [ Links ]
Manoel, M. F., Teston, E. F., Waidman, M. A. P., Decesaro, M. N., & Marcon, S. S. (2013). As relações familiares e o nível de sobrecarga do cuidador familiar. Escola Anna Nery, 17(2),346-353. doi: 10.1590/S1414-81452013000200020 [ Links ]
Martins, E. (2013). Constituição e significação de família para idosos institucionalizados: uma visão histórico-cultural do envelhecimento. Estudos e Pesquisas em Psicologia, 13(1),215-236. [ Links ]
Meira, S. S., Vilela, A. B. A., Casotti, C. A., Nascimento, J. C. D., & Andrade, C. B. (2015). Idosos em estado de corresidência em um município do interior da Bahia. O Mundo da Saúde, 39(2),201-209. doi: 10.15343/0104-7809.20153902201209 [ Links ]
Melo, L. A., Ferreira, L. M. B. M., Santos, M. M., & Lima, K. C. (2017). Fatores socioeconômicos, demográficos e regionais associados ao envelhecimento populacional. Revista Brasileira de Geriatria e Gerontologia, 20(4),494-502. doi: 10.1590/1981-22562017020.170004 [ Links ]
Melo, N. C. V., Teixeira, K. M. D., Barbosa, T. L., Montoya, Á. J. A., & Silveira, M. B. (2009). Arranjo domiciliar de idosos no Brasil: Análises a partir da Pesquisa Nacional por Amostra de Domicílios. Revista Brasileira de Geriatria e Gerontologia, 19(1),139-151. [ Links ]
Mendes, P. M. T. (1995). Cuidadores: Heróis anônimos do cotidiano. (Unpublished Master's Dissertation), Pontifícia Universidade Católica de São Paulo, São Paulo. [ Links ]
Ministério do Trabalho, Solidariedade e Segurança Social (2018). Carta social: Rede de serviços e equipamentos 2018. Lisboa: MTSSS. Retrieved from http://www.cartasocial.pt/pdf/csocial2018.pdf [ Links ]
Mocelin, D., Aires, M., Fuhrmann, A. C., Pizzol, F. L. D., & Paskulin, L. M. G. (2019). Responsabilidade filial: Quais as atitudes dos filhos sobre a institucionalização dos pais idosos? Revista Gaúcha de Enfermagem, 40,e20180377. doi: 10.1590/1983-1447.2019.20180377 [ Links ]
Moscovici, S. (2007). Representações sociais: Investigações em psicologia social. Translated by Pedrinho A. Guareschi. (5th ed). Petrópolis, RJ: Vozes. [ Links ]
Oliveira, A. M. S., & Pedreira, L.C. (2012). Being elderly with functional dependence and their family caregivers. Acta Paul. Enferm., 25(spe1),143-149. [ Links ]
Passos, M. C. (2005). Nem tudo que muda, muda tudo: Um estudo sobre as funções da família. In Feres-Carneiro, T. (Ed.), Família e casal: Efeitos da contemporaneidade (pp. 11-23). Rio de Janeiro: Editora PUC-Rio. [ Links ]
Paúl, M. C. (1997). Lá para o fim da vida. Idosos, família e meio ambiente. Coimbra: Livraria Almedina. [ Links ]
Pedrazzi, E. C., Motta, T. T. D., Vendrúscolo, T. R. P., Fabrício-Wehbe, S. C. C., Cruz, I. R., & Rodrigues, R. A. P. (2013). Arranjo domiciliar dos idosos mais velhos. Revista latino-americana de enfermagem, 18(1). [ Links ]
Petrini, G. (2009). Significado social da família. Cadernos de Arquitetura e Urbanismo, 16(18+19),111-122. doi: 10.5752/P.2316-1752.2009v16n18/19p111 [ Links ]
Pimentel, L. (2012). Cuidar de pessoas idosas dependentes: As intersecções entre a esfera pública e a esfera privada. Revista Rediteia, (45),67-78. [ Links ]
Pimentel, L. G., & Albuquerque, C. P. (2010). Solidariedades familiares e o apoio a idosos: Limites e implicações. Textos & Contextos, 9(2),251-263. [ Links ]
Pinto, F. N. F. R., Barham, E. J., & Albuquerque, P. P. (2013). Idosos vítimas de violência: Fatores sociodemográficos e subsídios para futuras intervenções. Estudos e Pesquisas em Psicologia, 13(3),1159-1181. [ Links ]
Pordata (2018). BI de Portugal. Retrieved from http://www.pordata.pt [ Links ]
Ramos, N. (2005). Relações e solidariedades intergeracionais na família: Dos avós aos netos. Revista Portuguesa de Pedagogia, 39(1),195-216. [ Links ]
Reis, L. A., & Trad, L. A. B. (2016). Percepção de idosos com comprometimento da capacidade funcional acerca do suporte familiar. Revista Kairós: Gerontologia, 19(22),175-189. doi:0.23925/2176-901X.2016v19iEspecial22p175-189 [ Links ]
Rodrigues, T. F., & Martins, M. R. O. (2014). Envelhecimento e Saúde. Prioridades Políticas num Portugal em Mudança. Portugal: Instituto Hidrográfico. [ Links ]
Rodrigues, R. A. P., Silva, L. M., Santos, A. M. R., Pontes, M. L. F., Fhon, J. R., Bolina, A. F., ... Silva, L. M. (2017). Violência contra idosos em três municípios brasileiros. Revista Brasileira de Enfermagem, 70(4),783-791. doi: 10.1590/0034-7167-2017-0114 [ Links ]
Santos, S. M. A. (2010). Idosos, Família e Cultura: Um estudo sobre a construção do papel do cuidador (3rd ed). Campinas: Alínea. [ Links ]
Santos, R. A. A. S., Santos, R. A. A. S., Rolim, I. L. T. P., & Coutinho, N. P. S. (2016). Atenção no cuidado ao idoso: Infantilização e desrespeito à autonomia na assistência de enfermagem. Revista de Pesquisa em Saúde, 17(3),179-183. [ Links ]
Sarti, C. A. (1995). O valor da família para os pobres. In I. Ribeiro & A. C. T. Ribeiro (Org.), Família em processos contemporâneos: Inovações culturais na sociedade brasileira (pp. 131-150). São Paulo: Loyola. [ Links ]
Silva, I. T., Junior, E. P. P., & Vilela, A. B. A. (2014). Autopercepção de saúde de idosos que vivem em estado de corresidência. Revista Brasileira de Geriatria e Gerontologia, 17(2),275-287. [ Links ]
Silva, M. J., Victor, J. F., Mota, F. R. do N., Soares, E. S., Leite, B. M. B., & Oliveira, E. T. (2014). Análise das propriedades psicométricas do APGAR de família com idosos do nordeste brasileiro. Escola Anna Nery Revista de Enfermagem, 18(3),527-532. doi: 10.5935/1414-8145.20140075 [ Links ]
Sousa, K. T., Mesquita, L. A. S., Pereira, L. A., & Azeredo, C. M. (2014). Baixo peso e dependência funcional em idosos institucionalizados de Uberlândia (MG), Brasil. Ciência & Saúde Coletiva, 19,3513-3520. [ Links ]
Vitória da Conquista (2018). Programa municipal presta atendimento em saúde aos idosos com limitações. Retrieved from https://www.pmvc.ba.gov.br/programa-municipal-presta-atendimento-em-saude-aos-idosos-com-limitacoes/ [ Links ]
Xavier, R. L. (2010). Família, Direito e Lei. In R. L. Xavier, Léxico da Família: Temas Ambíguos e Controversos sobre Família, Vida e Aspectos Éticos, de Pontifício Conselho para a Família (pp. 363-376). Cascais: Princípia. [ Links ]
Wall, K. (1995). Apontamentos sobre a família na política social portuguesa. Análise Social, 431-458. [ Links ]
 Correspondence:
Correspondence:
Luciana Araújo dos Reis
Av. José Moreira Sobrinho, S/N, Jequiezinho
Jequié, BA, Brazil. CEP 45200-000
E-mail: lucianauesb@yahoo.com.br
Submission: May 28th, 2020
Acceptance: March 26th, 2021
Authors' notes: Elaine dos S. Santana, Program of Memory: Language and Society, State University of Southwest Bahia (UESB); Felismina Rosa P. Mendes, Department of Nursing, Évora University; Nádia Cristina M. S. Gobira, Technical Coordination of Environment (COTAM), UESB; Alessandra S. de Oliveira, Department of XX, UESB; Arianna O. S. Lopes, Nursing Collegiate, Northeast Independent College (Fainor); Thaiza T. Xavier, Department of XX, Federal University of Rio Grande do Norte (UFRN); Layanne Christinne dos P. Miguens, Department of Development and Teaching, Federal Institute of Education, Science and Technology of Maranhão (IFET); Luana A. dos Reis, Nursing Collegiate, Fainor; Luciana A. dos Reis, Department of Health, UESB.
1 Modified designation for Residential Structure for Older person in Portugal and Long-Stay Institutions for the Elderly in Brazil.

