










Serviços Personalizados
Journal

artigo
 Inglês (pdf)
Inglês (pdf)
 Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
Indicadores
Compartilhar

 Permalink
PermalinkPsicologia: teoria e prática
versão impressa ISSN 1516-3687
Psicol. teor. prat. vol.23 no.1 São Paulo jan./abr. 2021
https://doi.org/10.5935/1980-6906/ePTPC1913554
10.5935/1980-6906/ePTPC1913554 COVID-19
Healthcare professionals in COVID-19: safety, fear, and intention to leave
Profissionais de saúde na COVID-19: segurança, medo e intenção de se afastar
Profesionales de la salud en COVID-19: seguridad, miedo e intención de alejarse
Ricardo N. CoutoI ; Emerson Diógenes de MedeirosI; Ana Beatriz de C. SouzaI; Paulo Gregório N. da SilvaII; Clara Lohana C. GuimarãesII; Patrícia N. da FonsecaII
; Emerson Diógenes de MedeirosI; Ana Beatriz de C. SouzaI; Paulo Gregório N. da SilvaII; Clara Lohana C. GuimarãesII; Patrícia N. da FonsecaII
IFederal University of Delta do Parnaíba (UFDPar), Parnaíba, PI, Brazil
IIFederal University of Paraíba (UFPB), João Pessoa, PB, Brazil
ABSTRACT
The objective was to verify the fear of COVID-19 mediating role between the perception of safety at work and the intention of professionals on the frontline of COVID-19 to distance themselves from work. For this intent, 227 professionals (Mage = 33.01; SD = 7.67), mostly female (67.8%), answered the Safety Climate Scale in Hospital Work, the Intentional Behavior to Take a Leave of Absence Scale adapted to the COVID-19 context, the Fear of COVID-19 Scale, and a sociodemographic questionnaire. The safety perception in places of fight against the COVID-19 minimizes the fear of infection, consequently reducing health professionals' intention to take leaves of absence when in hospitals in the pandemic. Thus, ensuring the professionals' safety in their workplace is a protective factor of fear, so it may collaborate for the development of relevant strategies that minimize the intention to take a leave of absence.
Keywords: COVID-19; job safety; fear; absence; professionals.
RESUMO
O objetivo deste trabalho foi verificar o papel mediador do medo da COVID-19 na relação entre a percepção de segurança no trabalho e a intenção de profissionais atuantes no combate da COVID-19 de se afastarem do serviço. Para tanto, 227 profissionais (Midade = 33,01; DP = 7,67), maioria do gênero feminino (67,8%), responderam à Escala de Clima de Segurança no Trabalho Hospitalar, à Escala de Intenção Comportamental de Afastamento dos Serviços, adaptadas para o contexto da COVID-19, a Fear of COVID-19 Scale e a um questionário sociodemográfico. A percepção de segurança nos locais de combate à COVID-19 minimiza o medo da infecção, consequentemente diminuindo a intenção dos profissionais atuantes em hospitais na pandemia de se afastarem do serviço. Assim, assegurar segurança dos profissionais no local de trabalho é um fator protetivo do medo, que pode então colaborar para o desenvolvimento de estratégias pertinentes que minimizem a intenção de afastamento do trabalho.
Palavras-chave: COVID-19; segurança do trabalho; medo; afastar; profissionais.
RESUMEN
El objetivo del presente trabajo fue verificar el papel mediador del miedo de la COVID-19 en la relación entre percepción de seguridad en el trabajo y la intención de apartarse de los servicios de profesionales actuantes en el combate el COVID-19. Por lo tanto, 227profesionales (Medad = 33.01 años; DE= 7.67), la mayoría mujeres (67.8%), respondieran la Escala de Clima de Seguridad en el Trabajo Hospitalario, la Escala de Intención Comportamental de Alejarse de los Servicios, adaptadas para el contexto de la COVID-19, Fear of COVID-19 Scale y cuestionario sociodemográfico. La percepción de seguridad en los lugares de combate al COVID-19 minimiza el miedo a la enfermedad, reduciendo en consecuencia la intención de alejarse de los profesionales de los hospitales durante la pandemia. Así, velar por la seguridad de los profesionales en el trabajo es un factor protector del miedo, por lo que es posible colaborar en el desarrollo de estrategias relevantes que minimicen la intención de alejarse del trabajo.
Palabras clave: COVID-19; seguridad del trabajo; miedo; retirada; profesionales.
Introduction
With the first case of viral pneumonia detected in Wuhan, China, and its rapid spread, other territories beyond the Chinese borders were affected and dominated by a virus capable of paralyzing the world: the new coronavirus, which, in a short time, has transformed itself into the COVID-19 pandemic. Like other countries, Brazil was hit by an increasing number of COVID-19 cases, with the alarming data and rapid transmission causing the World Health Organization (WHO) to issue a pandemic alert. On October 04th, 2020, Brazil had 4,880,523 confirmed cases and 145,388 deaths, apart from the 34,804,348 confirmed cases and 1,030,738 deaths worldwide, distributed several in areas, territories, and countries (WHO, 2020).
In addition, frequent circulations of dubious news and fake information increased the population's fear, aggravating a state of insecurity motivated by the absence of control measures and effective therapeutic mechanisms. In some situations, the psychosocial impacts of outbreaks are more widespread than the disease itself, a fact that causes concern about the psychosocial impact of the disease in the entire population (Asmundson & Taylor, 2020).
In infectious diseases' outbreaks, the feeling of fear is an assiduous characteristic, and it is directly associated with transmission and mortality rates, in addition to the uncertainty in the face of the unknown, being characterized as a fundamental variable in the assessment of mental health, leading to challenges beyond the physical dimensions. When the level of fear is high, individuals may not think clearly and rationally when reacting to COVID-19, which is enhanced in professionals who continue to work in centers of excellence to combat this disease (Mertens, Gerritsen, Salemink, & Egelhard, 2020).
Faced with this scenario, it is evident that health professionals are the most vulnerable professional group, suffering negative psychological consequences, which can cause feelings of loneliness and helplessness, mainly because they have to leave their families, or sensing a series of dysphoric emotional states such as stress, irritability, mental fatigue, and despair. Such conditions, in addition to hindering the development of normal activities, can contribute to their intention to take leaves of absence, a decision that, when implemented, makes it difficult to meet the demand of patients infected due to the lack of skilled professionals (Ornell, Halpern, Kessler, & Narvaez, 2020).
The whole scenario that involves professionals working to combat the disease and the possible leave of absence can hinder the functioning and provision of healthcare services in Brazil. Thus, in order to overcome the daily challenges in these places, there is a need for professionals to feel safe in their work environment. Facts such as the provision of personal protective equipment (PPE) and the performance of specific activities/training for each job performed maximize their perception of work safety, directly influencing their confidence in themselves and their interpersonal relationships (Andrade, Silva, & Netto, 2015; Ornell et al., 2020).
Thus, in the fight against COVID-19, the perception of work safety is presented as a protective factor. Given that the "safe environment" construct comprises shared perceptions of norms, beliefs, values, and practices about occupational risk and safety, it is an important indicator in preventing accidents and promoting worker's health. However, in some situations, working conditions may not promote good health, leading workers to report malaise and discomfort episodes. Mental and behavioral disorders are frequent causes of sickness absence, specifically in Brazil (Andrade et al., 2015).
Given the importance of the topic and the emergence of actions towards professionals' mental health, this research aims to answer, "What is the relationship pattern of the perception of work safety in hospitals, the fear of COVID-19, and the intention to take a leave of absence?" In order to answer this question, the objective was to verify the mediating role of the fear of COVID-19 in the relationship between the perception of safety at work and the intention of professionals working to combat COVID-19 to distance themselves from the work. The objective was to verify the relationship between the three variables and to propose versions of the Escala de Clima de Segurança no Trabalho Hospitalar (ClimaSeg-H - Safety Climate Scale in Hospital Work) and the Escala de Intenção Comportamental de Afastamento dos Serviços (EICAS - Intentional Behavior to Take a Leave of Absence Scale), adapted to the COVID-19 context, gathering psychometric evidence. The research starts from the following hypotheses: 1) the ClimaSeg-H and the EICAS Scales, adapted to the COVID-19 context, will present acceptable psychometric evidence; 2) the perception of work safety will have an indirect effect on the intention to take a leave of absence, mediated by the fear of COVID-19.
The need for special attention to this class of workers, who perform an essential role with patients, seems essential. It is increasingly urgent to understand these professionals' work environments and their psychological status to develop appropriate guidelines on work safety, clinical and mental health interventions. Therefore, to carry out this research and obtain evidence that can demonstrate the contribution of work safety practices in explaining the intention to take a leave of absence, mediated by the fear of infection with the new coronavirus, it is necessary to have instruments that have adequate psychometric measuring qualities. Therefore, the psychometric instruments - and their adaptations - used in this research will be described before demonstrating the results obtained.
Escala de Clima de Segurança no Trabalho Hospitalar (ClimaSeg-H, Safety Climate Scale in Hospital Work): developed by Gershon et al. (2000) in the American context, in order to assess the perception of employees about the commitment of their hospital organization to work safety. They point out that safety climate includes cognitive and affective aspects about a given organization, related to the different perceptions and shared practices about risk and safety in the hospital environment.
The scale has a multifactorial approach, through 45 items theoretically subdivided into nine dimensions (engineering and safety equipment, support from safety managers, obstacles to safety, communication and feedback on safety, organization and cleanliness of the environment, safety programs and standards, support for safety programs and standards, responsibility management, and training and education; Gershon et al., 2000). This measure was adapted to the Brazilian context by Andrade et al. (2015), with 278 workers from public and private hospitals in the country's Southeastern region, providing a measure of 32 items.
The final structure was distributed in four dimensions: 1) safety program and standards: it assesses aspects related to the inspection standards and documents, in addition to the conduct of managers and staff; 2) safety equipment and environmental organization: it considers the structure, the maintenance of the work environment, and the provision of personal protective equipment; 3) support for work and safety practices: it gauges interpersonal aspects of the work environment, the communication and practices of managers to control unsafe conditions; 4) safety training and education: it alludes to organizational behaviors linked to general training, improvement, and education actions on topics related to safety (Andrade et al., 2015). In general, the scale assesses these dimensions as a set of shared perceptions and practices on work risk and safety.
Escala de Intenção Comportamental de Afastamento dos Serviços (EICAS - Intentional Behavior to Take a Leave of Absence Scale): initially elaborated by Brasileiro (2014) as the Escala de Intenção Comportamental de Adotar (EICA - Behavioral Intention of Adopting Scale), it indicates how much people intend to adopt this behavior, being composed of five items. Its items were adapted to the hospital work context to assess the professional's intention to take a leave of absence (e.g., item 2: I have clear goals of taking a leave of absence).
Thus, behavioral intention can be defined as the subjective probability of an individual to perform a certain behavior. Bearing in mind that knowing an individual's intention regarding a certain behavior is the best way to predict its occurrence, such adaptation to the hospital context is justified, as the behavioral intention has been studied to understand behaviors in the work environment (Steil, Floriani, Zilli, & Rubio, 2019).
Fear of COVID 19 Scale: conceptually, fear refers to an emotional response to an external factor. In the pandemic's specific case, situations of excessive fear have been frequently reported, especially the fear of community transmission of COVID-19, which can harm individuals' rational behavior and mental health, especially in health professionals working on the frontline (Ahorsu et al., 2020).
Regarding the Brazilian situation, it is understood that the country emerges as one of the pandemic epicenters. According to the bulletin released by the Brazilian Ministry of Health, on September 26th, 2020, 1,301,066 cases of suspected COVID-19 were reported in health professionals. Of these, 322,178 (24.8%) were confirmed, with the highest numbers being among nursing technicians/assistants (109,955; 34.1%), followed by nurses (47,339; 14.7%), doctors (33,032; 10.3%), community health workers (16,546; 5.1%), and health center receptionists (14,024; 4.4%). Of these numbers, 315 confirmed cases of COVID-19 resulted in death, in which the most frequent professional categories were nursing technicians/assistants (107; 34%), doctors (62; 19.7%), and nurses (36; 11.4%).
Thus, it is understood that the moment requires caution, especially regarding the adaptation of protocols and specificities associated with the Brazilian health structure. All of the above seem to clarify the importance of conducting this research, which aims to contribute with evidence that will support the execution of specific actions with professionals to avoid taking a leave of absence. The methodological path to obtain the results and the discussion from the specialized literature are presented below.
2. Method
2.1 Participants
The sample consisted of professionals (e.g., doctors, nurses, psychologists, physiotherapists) working to combat COVID-19, mostly in public institutions (82%), all with PPE available. Altogether, 227 professionals answered the survey, mostly single (55.7%), without children (56.2%), female (67.8%), and with a mean age of 33.01 years (SD = 7.84). Furthermore, most of them came from states in the Northeastern region of Brazil: Piauí (36.7%), Ceará (20.8%), and Maranhão (7.3%).
2. 2 Instruments
• Intentional Behavior to Take a Leave of Absence Scale (EICAS): a version composed of five items that assess whether health professionals, due to COVID-19, intended to ask to leave their functions (e.g., item 5: I plan to take a leave of absence). For this, it was necessary to adapt the Behavioral Intention of Adopting Scale elaborated by Brasileiro (2014), which presents a Cronbach's alpha equal to 0.86, with its items answered on a Likert scale that varies from 1 (totally disagree) to 7 (totally agree).
• Safety Climate Scale in Hospital Work (ClimaSeg-H): composed of 32 items, it assesses the perception of safety climate in the hospital context from a response scale that varies from 1 (strongly disagree) to 5 (strongly agree). For the correct usage, some items have undergone content adaptation to refer to COVID-19 (e.g., item 21: I have all the necessary equipment to protect myself from possible exposure to COVID-19). Andrade et al. (2015) adapted and gathered psychometric evidence for Brazil from the original scale proposed by Gershon et al. (2000). Once that was done, an instrument with four dimensions and Cronbach alphas ranging from 0.82 to 0.91 was made available.
• Fear of COVID-19 Scale (FCV-19S): composed of seven items, it assesses the fear of COVID-19 (e.g., item 4: I am afraid of losing my life because of COVID-19). It was answered on a five-point scale ranging from 1 (strongly disagree) to 5 (strongly agree) and, in its elaboration, acceptable psychometric evidence was gathered (single-factor structure and Cronbach's alpha equal to 0.82; Ahorsu et al., 2020). In this research, the Brazilian version for health professionals was used, adapted, and validated by Couto, Medeiros, Sousa, Medeiros, & Carvalho (in press).
• Sociodemographic questionnaire: for the characterization of the sample, it was composed of questions related to age, sex, and work-related aspects in the fight against COVID-19.
2. 3 Procedure
The research was approved by the Human Research Ethics Committee of the Universidade Federal do Piauí (UFPI, Federal University of Piauí), process no. 4.062.796, considering all the ethical requirements of Resolution 510/16 of the Conselho Nacional de Saúde (CNS, National Health Council/Ministry of Health, Brazil). Initially, the ClimaSeg-H and the EICAS scales were translated using the back-translation technique, assisted by two bilingual psychologists. After this stage, a semantic validation was performed (Pasquali, 2016) with the participation of 20 professionals, equally distributed regardless of sex and occupation (e.g., doctors, nurses, psychologists, physiotherapists), who analyzed the version of instruments and suggested no changes.
Subsequently, the Qualtrics platform (www.qualtrics.com) applied the instruments, providing an access link via e-mail and various social networks (e.g., Facebook, WhatsApp, and Instagram). People were invited to participate in the survey, whose home page contained information about the general objective of the study, voluntary nature, anonymity, and the possibility of quitting at any time, free of penalties. Before responding to the instruments, they were asked to confirm their participation by agreeing with the Informed Consent Term (ICT). The average time taken to complete the survey was 10 minutes.
2. 4 Data analysis
With the Factor 10.10.03 software, the dimensionality of the scales (ClimaSeg-H and EICAS) was investigated, using the Hull Comparative Fit Index (CFI) method as a criterion for deciding how many factors to retain, taking into account a categorical Exploratory Factor Analysis (EFA), a robust Diagonally Weighted Least Squares (DWLS) implemented in the matrix of polychoric correlations, because the scales cannot be considered continuous, as they are Likert-type, composed of ordered categories (Lara, 2014). In addition, Cronbach's alpha and McDonald's omega were calculated to gather evidence of accuracy. The SPSS software was used to characterize the participants through descriptive statistics and dispersion, in addition to correlations between measures. With the Process extension (Hayes, 2013), a mediation model was tested, with the perception of work safety as an independent variable, fear of COVID-19 as a mediating variable, and the intention to take a leave of absence as a dependent variable.
3. Results
In order to gather evidence validity regarding the internal structure of the ClimaSeg-H and the EICAS scales, robust categorical analyzes were performed (500 bootstrap resamplings), with the adaptation of the polychrome matrices to the EFA of the ClimaSeg-H [KMO = 0.94 and Bartlettχ2 (496) = 2481.1; p < 0.001] and of the EICAS [KMO = 0.78 and Bartlettχ2 (10) = 914.1; p < 0.001]. From a categorical EFA of the DWLS, both scales resulted in a single factor that explains 54% and 70% of the total variance, respectively. The unidimensionality of the aforementioned measures was suggested by the Hull method and the unidimensionality indicators for the ClimaSeg-H [UniCo (Unidimensional Congruence), with mean correlations at the item level equal to 0.98, ranging from 0.94 to 1.00; Explained Common Variance (ECV), mean = 0.90, ranging from 0.75 to 1.00; Mean of Item Residual Absolute Loadings (MIREAL) = 0.21, ranging from 0.01 to 0.44]; and the EICAS (single, with mean correlations at the item level equal to 0.97, ranging from 0.89 to 1.00); ECV, mean= 0.89, ranging from 0.66 to 0.97; and MIREAL= 0, 27, ranging from 0.15 to 0.30.
It is noteworthy that the factorial loads of the ClimaSeg-H items ranged from 0.53 (item 20) to 0.83 (item 17); the EICAS loads ranged from 0.40 (item 04) to 0.93 (item 01). In addition, internal consistency was measured using Cronbach's alpha and McDonald's omega, with results that indicated equally satisfactory evidence. These details and the relationship pattern, based on the total scores of the measures between the intention to take a leave of absence, the perception of work safety, and the fear of COVID-19, are shown in Table 3.1.

From the data in Figure 3.1, the intention to leave services is negatively correlated with the perception of work safety and positively correlated with the fear of COVID-19. In addition, fear is negatively correlated with the perception of work safety in hospitals. Based on these results and the proposed theoretical relationship, a mediation model is investigated, which perceives safety as an independent variable. The mediator variable is the fear of COVID-19. The dependent variable is the intention to take a leave of absence. Readers must consider that data collection was carried out using an online platform with all questions answered by the participants, so there was no missing information, and the data were calculated from the sum of the items. To this end, this simple mediation model was tested, with a method of 5000 bootstraps resamples (Hayes, 2013), whose results are detailed below.
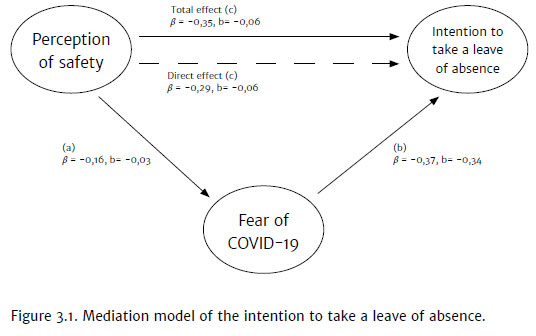
The direct effect of perceived safety on the intention to take a leave of absence was statistically significant [β = -0.35, b = -0.06, 95% CI (-0.08; -0.04), t = - 5.55, p < 0.001; R2 = 0.12 (12%)]. With the inclusion of the mediating variable in the model, the direct effect of perceived safety impacting on the intention to take a leave of absence, controlled by the fear of COVID-19, decreases the coefficient, but remains statistically significant [β = -0.29, b = - 0.06, 95% CI (-0.07; -0.03), t = -4.94, p < 0.001]. It also happened with the impact of fear (m) on the intention to take a leave of absence (y) [β = 0.37, b = 0.34, 95% CI (0.24; 0.45), t = 6, 25, p < 0.001] and with the impact of perceived safety (x) on fear (m) [β = -0.16, b = -0.03, 95% CI (-0.06; -0.01 ), t = -2.41, p = 0.02].
It is noteworthy that this model, illustrated in Figure 3.1, the perception of safety mediated by the fear of COVID-19, explaining the intention to take a leave of absence, presented an R2 = 0.25. Furthermore, it had an indirect effect that was considered statistically significant according to the bootstrap method (5000 samples), since the coefficients and their confidence intervals do not reach zero and do not change the direction of the relationship [β = -0.06, 95% CI (- 0.10; -0.01); b = -0.01, 95% CI (-0.02; -0.01)]. Thus, it can be observed that the model explained 25% of the variance, a little more than twice the explanation, without the presence of the mediating variable (the fear of COVID-19). Such partial mediation is considered, therefore, even in the presence of a mediator variable, and the independent variable (perception of safety) continues to influence the intention to take a leave of absence.
4. Discussion
The present research was successful regarding its proposed objectives, which, in general, was to test a mediation model with the perception of work safety in hospitals as an independent variable, the fear of COVID-19 as a mediator, and the intention to take a leave of absence as a dependent variable. Specifically, it was intended to verify the relationship between the three variables and propose versions of the Safety Climate Scale in Hospital Work (ClimaSeg-H) and the Intentional Behavior to Take a Leave of Absence Scale (EICAS) adapted to the context of COVID-19, gathering psychometric evidence.
To this end, initially, evidence was gathered that attested to the metric quality of the ClimaSeg-H and the EICAS scales, with rates higher than those indicated in the literature (Pasquali, 2016). Thus, the aforementioned measures presented a unidimensional structure for the Brazilian context, with good precision indices, assessed by Cronbach's alpha and McDonald's omega indicators, the latter being considered more robust (Cohen, Swerdlik, & Sturman, 2014). Such evidence corroborates hypothesis 1 and suggests that both the work safety climate and the intention to take a leave of absence can be assessed globally.
Considering the measures in a separate way, it is emphasized that for the safety work measure (despite being initially considered multidimensional, in which, in the American context, structures of nine and six factors were verified (Gershon et al., 2000)), in different countries, different versions and structures of ClimaSeg-H can be verified (Smith, Zhao, Wang, & Ho, 2013), including in the Brazilian context, in which four factors were found (Andrade et al., 2015). Thus, despite the unified structure presented in this study, diverging from previous studies, such results can be justified by the theoretical bias, assessing the climate as a set of perceptions and shared practices about risk and safety at work, so all aspects of the safety climate are assessed in an objective and general way, and in an empirical bias, which were assessed by the UniCo, ECV, and MIREAL indicators, which suggested the possibility of the sets of items being represented by a single-factor model, given that a weighted interpretation of the results reinforces the unidimensionality indicated by the Hull method (Ferrando & Lorenzo-Seva, 2017).
A result that corroborates international studies that relied on samples from hospitals, Blegen, Pepper, and Rosse (2005) assert that joining the dimensions to assess the safety climate makes conceptual sense. Hahn and Murphy (2008) provide a short scale of six items from the gather items already existing in the literature that belonged to multidimensional measures. Therefore, they suggest a more objective assessment of the phenomenon in a general and parsimonious way. The intention to take a leave of absence corroborates the structure previously found by Brasileiro (2014), who verified the behavioral intention to adopt a scale, an instrument that was adapted to the context of the present research.
Furthermore, correlations followed by a mediation model demonstrate that the relationship between fear and the desire to take a leave of absence was positive. The increase in this intention is related to the many challenges faced by health professionals in combating COVID-19. Stressful events are recurrent in the context of a pandemic, which demands more effort and dedication from professionals, causing and intensifying the fear of self-contamination, as well as the fear of contaminating family members; fear of dying, verbal, psychological, and even physical violence by those who seek medical care; taking care when handling PPE to avoid contamination, requiring more time and caution from the professional; distancing from family and social life. All of this can be an exhaustion factor for professionals, causing symptoms of anxiety, stress, depression, and loneliness (Ornell et al., 2020; Zhang et al., 2020).
Corroborating hypothesis 2, the perception of work safety presented itself as a protective factor in environments to combat COVID-19, with a negative relationship with fear and the intention to take a leave of absence, which also remained with a significant direct effect, even with the inclusion of the fear of COVID 19 as a mediator variable. Data that emphasize the importance of the topic and procedures that should be adopted when professionals have close contact with confirmed or suspected cases at work or elsewhere are applied (given that, in different places, the focus on safety measures is a priority, for example, in a study conducted at a university hospital in Bari, Italy, which presents possible measures for the prevention and protection of health professionals exposed to coronavirus), such as the implementation of a reporting system to record situations and the correct measures in order to prevent the spread of this infection, showing effective results in the correct management of the protocol (Vimercati et al., 2020).
Another study, this time at a university hospital in Seoul, Korea, reported that the admission of 13 people who were infected with COVID-19 (a priori without confirmation) meant that 184 hospital professionals had direct contact with these patients. To avoid and contain virus contamination, the hospital management sector classified patients into four risk levels and defined appropriate care and protection measures for each professional according to the level of contact they had. Obeying such measures, the results showed that, after 31 days of the protocol implementation, test results were negative for COVID-19, and no symptoms of infection were reported by these professionals, which is evidence of the effectiveness of the adopted management model (Jeon et al., 2020). In summary, it must be said that the local administration of the work environment is fundamental to contain contamination among health professionals, and the speed in the implementation of certain measures is necessary to ensure work safety and motivation.
The COVID-19 pandemic has had a strong impact on public health worldwide, and health professionals compose the group most prone to the disease since they are directly exposed to the risk of contamination. The importance of having efficient instruments to assess related constructs is also emphasized, in addition to being concerned with the work safety and mental health of these professionals in order to collaborate with findings that facilitate the development of relevant strategies that minimize the intention to take a leave of absence and, consequently, the deficit in health services.
However, some limitations need to be considered, such as the research participants are predominantly health professionals from the Northeastern region of Brazil; the nature of the self-report instrument cannot exclude the possibility that the participants' answers were affected by factors of social desirability and convenience sampling weakens the generalization of the findings in the present study. Thus, studies with more diversified samples (e.g., health professionals from other Brazilian states, contaminated or not with COVID-19, elderly and young individuals, length of service, etc.) and with a greater number of participants are suggested, as well as highlighting the importance of future research to consider other variables that may be related to aspects experienced by health professionals in this COVID-19 pandemic period, such as stress, anxiety, depression, Burnout syndrome, and life satisfaction, for example. It is also suggested to conduct a longitudinal study to assess resilience and post-traumatic stress in health professionals after the pandemic.
The findings reported here are expected to assist professionals in coping with this atypical period; to serve as a guide for the city, state, and federal administrations in creating efficient strategies that guarantee the minimum necessary work safety and the alleviation of the psychological consequences caused by the pandemic to the professionals who fight daily against the COVID-19, with actions such as conducting progressive training with professionals to promote spaces for clarification and appreciation of better measures that can boost levels of confidence, safety, and the willingness to continue working. Thus, balanced mental health can favor a better performance of the functions and the motivation to continue in the work, facilitating health professionals' commitment fighting against COVID-19.
References
Andrade, A. L., Silva, M. Z., & Netto, M. T, (2015). Clima de Segurança no Trabalho Hospitalar: Adaptação de medida (ClimaSeg-H). Avaliação Psicológica, 14(2),161-171. doi:10.15689/ap.2015.1402.11 [ Links ]
Ahorsu, D. K., Lin, C.-Y., Imani, D., Saffari, M., Griffiths, M. D., & Pakpour, A. H. (2020). The Fear of COVID-19 Scale: Development and initial validation. International Journal of Mental Health and Addiction. doi:10.1007/s11469-020-00270-8 [ Links ]
Asmundson, G. J., & Taylor, S. (2020). Coronaphobia: Fear and the 2019-nCoV outbreak. Journal of Anxiety Disorders, 70, 102-196. doi:10.1016/j.janxdis.2020.102196 [ Links ]
Blegen, M. A., Pepper, G. A., & Rosse, J. (2005). Safety Climateon Hospital Units: A New Measure. In: Henriksen K., Battles J. B., Marks E. S., & Lewin, D. I. Advances in patientsafety: From research to implementation (Vol. 4: Programs, Tools, and Products). Rockville (MD): Agency for Healthcare Research and Quality (US). Retrieved from https://pubmed.ncbi.nlm.nih.gov/21250019/ [ Links ]
Brasileiro, T. N. (2014). Medidas Explícitas e Implícitas de Atitudes Frente à Adoção e seus correlatos valorativos. (Master's Dissertation in Social Psychology). Federal University of Paraíba, Departament of Psychology, João Pessoa-PB. [ Links ]
Cohen, R. J., Swerdlik, M. E., & Sturman, E. D. (2014). Testagem e avaliação psicológica: Introdução a testes e medidas (8 ed.) São Paulo: AMGH. [ Links ]
Couto, R. N., Medeiros, E. D., Sousa, I. M., Medeiros, P. B. C., & Carvalho, T. A. (in press). Medo e ansiedade frente ao COVID-19 em profissionais atuantes: Parâmetros psicométricos medidas. [ Links ]
Ferrando, P. J., & Lorenzo-Seva, U. (2017). Assessing the quality and appropriateness of factor solutions and factor score estimates in exploratory item factor analysis. Educational and Psychological Measurement, 78,762-780. doi:10.1177/0013164417719308 [ Links ]
Gershon, R. R., Karkashian, C. D., Grosch, J. W., Murphy, L. R., Escamilla-Cejudo, A., Flanagan, P. A., ... Martin, L. (2000). Hospital safety climate and its relationship with safe work practices and workplace exposure incidents. American Journal of Infection Control, 28(3),211-221. doi:10.1067/mic.2000.105288 [ Links ]
Hahn, S. E., & Murphy, L. A. (2008). A short scale for measuring safety climate. Safety Science, 46,1047-1066. doi:10.1016/j.ssci.2007.06.002 [ Links ]
Hayes, A. F. (2013). Introduction to mediation, moderation, and conditional process analysis. New York: The Guilford Press. [ Links ]
Jeon, Y. W., Park, E. S., Jung, S. J., Kim, Y., Choi, J. Y., & Kim, H. C. (2020). Yonsei Medical Journal, 61(7),631-634. doi:10.3349/ymj.2020.61.7.631 [ Links ]
Lara, S. A. D. (2014). ¿Matrices Policóricas/Tetracóricas o Matrices Pearson? Un studio metodológico. Revista Argentina de Ciencias del Comportamiento, 6(1),39-48. Retrieved from http://www.redalyc.org/articulo.oa?id=333430869006 [ Links ]
Ministry of Health (2020). Special epidemiological bulletin - Coronavirus disease - COVID 19. Retrieved from http://portalarquivos2.saude.gov.br/images/pdf/2020/October/01/Boletim-epidemiologico-COVID-33-final.pdf [ Links ]
Mertens, G., Gerritsen, L., Salemink, E., & Egelhard, M. (2020). Fear of the coronavirus (COVID-19): Predictors in an online study conducted in March 2020. Journal of Anxiety Disorders, 74,102258. doi:10.1016/j.janxdis.2020.102258 [ Links ]
Ornell, F., Halpern, S. C., Kessler, F. H. P., & Narvaez, J. C. M. (2020). The impact of the COVID-19 pandemic on the mental health of healthcare professionals. Cadernos de Saúde Pública, 36(4),e00063520. doi:10.1590/0102-311X00063520 [ Links ]
Pasquali, L. (2016). TEP - Técnicas de Exame Psicológico: Os Fundamentos. (2 ed.). São Paulo, SP: Vetor Editora. [ Links ]
Smith, D. R., Zhao, I., Wang, L., & Ho, A. (2013). Dimensions and reliability of a hospital safety climate questionnaire in Chinese health-care practice. International Journal of Nursing Practice, 19(2),156-162. doi:10.1111/ijn.12046 [ Links ]
Steil, A. V., Floriani, E. V., Zilli, M. B., & Rubio, M. A. (2019). Intenção de sair da organização: Definições, métodos e citações nas publicações nacionais. Revista Psicologia: Organizações e Trabalho, 19(2),580-587. doi:10.17652/rpot/2019.2.14080 [ Links ]
Vimercati, L., Dell'Erba. A., Migliore. G., De Maria, L., Caputi, A., Quarato, M., ... Tafuri, S. (2020). Prevention and protection measures of healthcare workers exposed to SARS-CoV-2 in a university hospital in Bari, Apulia, Southern Italy. Journal of Hospital Infection, 105,454-458. doi:10.1016/j.jhin.2020.05.024 [ Links ]
World Health Organization (2020). Coronavirus disease (COVID-2019): Data as received by WHO from national authorities, as of 04 October 2020, 10 am CEST. Retrieved from https://www.who.int/docs/default-source/coronaviruse/situation-reports/20201005-weekly-epi-update-8.pdf [ Links ]
Zhang, C., Yang, L., Liu, S., Ma, S., Wang, Y., Cai, Z., ... Zhang, B. (2020). Survey of insomnia and related social psychological factors among medical staff involved in the 2019 novel coronavirus disease outbreak. Frontiers in Psychiatry, 11(306),1-9. doi:10.3389/fpsyt.2020.00306 [ Links ]
 Correspondence:
Correspondence:
Ricardo Neves Couto
Rua Caiapós, n. 107
Parnaíba, PI, Brazil. CEP 64215-470
E-mail: r.nevescouto@gmail.com
Submission: 11/08/2020
Acceptance: 30/10/2020
The authors would like to thank the Conselho Nacional de Desenvolvimento Científico e Tecnológico for the productivity grant; The authors would like to thank the Coordenação de Aperfeiçoamento de Pessoal de Nível Superior for the doctoral grant.
Authors' notes:
Ricardo N. Couto, Department of Psychology, Federal University of Delta do Parnaíba (UFDPar); Emerson Diógenes de Medeiros, Department of Psychology, Federal University of Delta do Parnaíba (UFDPar); Ana Beatriz de C. Souza, Department of Psychology, IBRA University; Paulo Gregório N. da Silva, Department of Psychology, Federal University of Paraíba (UFPB); Clara Lohana C. Guimarães, Department of Psychology, Federal University of Paraíba (UFPB); Patrícia N. da Fonseca, Department of Psychology, Federal University of Paraíba (UFPB).
This study is part of a Post Doctoral Internship project presented to the Programa de Pós-Graduação em Psicologia of the Universidade Federal do Piauí.

