










Serviços Personalizados
Journal

artigo
 Inglês (pdf)
Inglês (pdf)
 Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
 Curriculum ScienTI
Curriculum ScienTIIndicadores
Compartilhar

 Permalink
PermalinkJournal of Human Growth and Development
versão impressa ISSN 0104-1282
Rev. bras. crescimento desenvolv. hum. vol.22 no.2 São Paulo 2012
ORIGINAL RESEARCH
Impact of domestic and sexual violence on women's health
Sandra Dircinha Teixeira de Araujo MoraesI, III; Angela Maggio da FonsecaI, III; Vicente Renato BagnoliI; José Maria Soares JúniorI; Eli Mendes de MoraesI, III; Erika Mendonça das NevesI, III; Marina de Araújo RosaIII; Caio Fabio Schlechta PortellaIII; Edmundo Chada BaracatI, II
ISchool of Medicine-General Hospital - University of São Paulo
IIHead professor of Department of Gynecology-School of Medicine-General Hospital - University of São Paulo
IIINucleo de Estudos sobre Violência e Humanização da Assistência à Saúde - NEVHAS
ABSTRACT
INTRODUCTION: domestic violence and, particularly, sex can result in higher incidence of comorbidities in the climacteric.
OBJECTIVE: to assess the effects of menopause on sexual and domestic violence.
METHODS: sectional study in 124 postmenopausal women between 40 and 65, who suffered domestic violence and / or sexual, and a control group (124) composed (climacteric women who did not suffer violence) (N=120). Those who exposed to violence were divided into three groups 1 violence experienced in childhood and adolescence 2- adult phase 3- both phases. Subsequently a questionnaire on domestic and sexual violence was applied.Correlation was established for the intensity of climacteric symptoms measured with Menopausal Kupperman Index (MKI), type of violence experienced, stage of life exposesd to violence comorbidities during menopause, and women's perceptions about the quality of assistance received from the various professionals after the traumatic events. In the control group MKI and number of comorbidities were evaluated.
RESULTS: those who have experienced violence in childhood/adolescence have average of 5.1 comorbidities; adulthood 4.6, and 4.4 in both phases, with a median of 5.0 in all phases, without violence (control) 2.8. The victims of sexual violence have more comorbidities compared those who underwent other types of violence. There were significant associations between having suffered any kind of violence in both phases and MKI serious and have suffered sexual violence at any stage of life, and MKI at least moderate.
CONCLUSION: women who have experienced domestic and sexual violence have more comorbidities and MKI high compared to the control group.
Key words: domestic violence; sexual violence; menopause; climacteric co morbidities; menopausal Kupperman Index.
INTRODUCTION
Knowledge of the occurrence of violence committed against women and its impact on their health in the climacteric phase in national and international context, is still scarce and constitute a major problem in public heath. The issue seldom surfaces in diagnostics and in conducts carried out in health services due to the difficulty of the actors in expressing the experienced violence and limitations on the part of the health team in providing the adequate health assistance to the integral women's health, especially in the climacteric phase , among other reasons1-4.
Domestic violence and particularly sexual violence can lead to a greater occurrence of several physical, reproductive and mental health problems, and also leads to greater use of the various health services by women. 1,5,6,7
Although existing research8,9,10 has contributed to improving the quality of the investigation of the violence suffered by women, many instruments are still limited by a variety of methodological shortcomings1,4,5,7,11. Such probing tools concerning violence suffered in childhood/adolescence ignore the dimensional features of traumatic events12,13. These are the frequency, severity or duration that may play a crucial role in both the physical and psychological impact of the person victimized14. Many instruments focus solely on only the physical or sexual abuse and, underestimating other forms of victimization such as emotional abuse and emotional neglect1,15,16. In the literature review13,17, those contemplating such dimensions have directed the focus more to the child/adolescent and reproductive phase adult life of women3,15, yet not quantifying the impact of violence on the health of these women.
Women in climacteric arena lack satisfactory instruments to quantify the consequences of domestic violence and/or sexual assessed in this stage of life. Woks found employing questionnaires6,16,18 to evaluate the quality of life of adult women do not address some traumas like emotional neglect.
So this study enabled the assessment o the impact of domestic and sexual violence on women's health in the climacteric phase.
METHODS
Sectional study carried out with women sought assistance in Department of Endocrine Gynecology and Climacteric of the General Hospital of the Medical School USP-SP-Brazil between March and September 2010 During pre consultation the subjects were informed about the research objectives, when it was emphasized that if any of them at some point in life had undergone any type of domestic or sexual violence they should seek the researcher, research assistant or one of the volunteers in that oupatient clinic. They were explained the most common types of violence and clarified on the importance of due care to abused people, in view of better quality of life. The clinic gynecologists were coached into inquiring individually and privately during the consultation if they had suffered any kind of violence. If so , the outpatient was invited to participate in the study (124women) . A control group of women who had not experienced violence assisted in the same service was formed (120) The subjects who suffered violence were also invited to participate in group activities and/or individual psychotherapy with a psychologist experienced in post trauma stress assistance in the same institution.
Elegibility Criteria
Inclusion criteria were: women with one year of amenorrhea, FSH levels < 45U/mL and estradiol levels < 20pg/ml who had suffered domestic and/or sexual violence at any phase of their lives. Exclusion criteria: women who suffered hysterectomies, women with current cancer in treatment, using antidepressant hormonal or herbal drugs as well as patients with psycho disturbances, non compensated endocrine diseases (diabetes and thyroid disorders), cardiovascular disease in treatment.
The survey consisted of the use of the 'Questionnaire to evaluate impactcs on climacteric women health that were victims of domestic and/or sexual violence' for the record of each patient's past or current history of aggression signs and of gynecological clinical symptoms (anamnesis and clinical and gynecological exams) at consultation time, seeking to identify associations between the variables of the history of aggression and climacteric comorbidities diagnosed up to a year before the visit / interview.
Some questions address experience in adulthood and in both phases - childhood/adolescence and adulthood and were also scored by a Likert scale with possible responses ranging from 1 - never, 2-seldom, 3 sometimes 4 - often, 5 - always or 1 -full agreement 2 - partial agreement, 3 in doubt, 4 partial disagreement, 5 total disagreement. There were multiple choice questions, yes or no questions and questions in which they could choose more than one alternative.
During the attendance the Menopausal Kupperman Index2 (MKI) was measured. It suffered a twofold analysis: total score and categorized score: light (d"19 points), moderate (20 to 35 points) and severe (>35 points). These women were classified as analyzed in two ways: considering the total score and categorized as mild (<= 19 points), moderate (20-35) and severe> 35 points. These women were classified by type of violence suffered (physical, sexual, psychological and physical neglect) according to the OMS15 trauma classification and emotional neglect1 detected through the aforementioned already validated questionnaire.
The questionnaire consists of 13 key and 21 sub-key questions, totaling 34 The questions are divided into five groups, which assess: Location where you live (rural or urban area) and with whom (physiological parents, stepfather, etc.), beginning of violence (life stage), frequency, type, and author of violence, if health care is sought and/or denounced the violence, comorbidities and their relationship to the violence, Menopausal Kuppermann Index, women perception regarding violence suffered and current state of health, sex life and state of mind , along with their perceptions about the performance of health professionals regarding their contribution for the breaking of the silence covenant and comprehensive care towards them.
Statistical analysis
For the data analysis descriptive statistics, frequencies and percentages of occurrence of each alternative issues were used. For the variables: type of violence, age suffered, agent perpetrator of violence, we used proportions. The Chi-square test and the Odds Ratio were used to establish the comparison between the groups and a few factors like place of residence and health service seeking.
The t test was also used for determination of independent samples, in order to search for significant differences between the study variable averages for the women who suffered domestic and/or sexual violence at a 5% (p<0,05) significance level. Descriptive statistics for the Menopausal Kupperman Index, the number of comorbidities and BMI category in each phase of life were conducted. The Kruskal - Wallis or Mann-Whitney tests were used to investigate possible associations between the distributions of the Menopausal Kupperman Index, number of comorbidities, BMI, and characteristics of current sexual life.
Ethics Approval
The study protocol was approved by the Ethics Committee of the Faculty of Medicine, USP according to the recommendations of Resolution 196/96 National Health (protocol number: 180/09). The research guaranteed the anonymity of patients, assuring them the right to give up the participation at any time. For emerging and/or hazardous situations there were intervention mechanisms for those victims, such as immediate care dispensed by a psychologist and /or referral to a psychiatrist.
RESULTS
Population: women between 40 and 65 years old, - average age 55.8 years - (± 6.6), 62.1% Caucasian, 37.1% Afro descents and 0.8% Asian that suffered domestic violence and / or sexual violence at any stage of life. The average menarche age was 13.1 years (± 2), first intercourse 19.5 years (± 5.8), menopause 45.4 years (± 7) and body mass index 28.5 (± 5, 7).
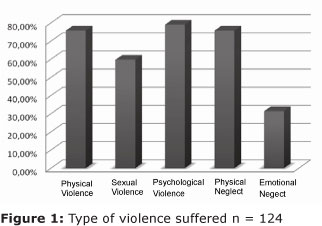
Figure 1 describes the types and frequency of violence suffered. Figures 2 and 3 describe tthe findings of the impacts of domestic and/or sexual violence on climacteric women health.
DISCUSSÃO
In this studied sample, only 20 women (16.12%) experienced violence in childhood / adolescence , 52 (41.9%) only in adulthood and 52 (41.9%) experienced violence throughout their lives (in both phases . 74 (59.7%) women suffered sexual violence at some stage of life . Regarding the type of violence suffered at any stage of life: Physical Violence 94 (75.8%), Sexual Violence 74 (59.7%) Psychological Violence 98 (79.03%) Physical Neglect 94 (75.8%); Emotional Neglect 39 (31.41%)
In adulthood in 88.00% the offender was the husband/partner.86.3% of those suffering violence in childhood had as aggressors biological parents.2.4%stepfather/stepmother, 7.3%, employers and 3.0% other.36 are sexually active (29.0%) and of these 20 (72.30%) consider it as satisfactory. 19 were smokers (15.0%) and 4 (3.1%) alcoholics.
These women have at least three comorbidities in climacteric: those with violence experienced in childhood/adolescence present average of 5.1 comorbidities; in adulthood 4.6, and 4.4 in both phases, with a median of 5.0 in all phases. The control group (without violence) presented 2.8 comorbidities.
Those who have suffered domestic violence and/or sexual presented: osteoporosis: 15.5%, depression/mental disorders: 69.4%; Hypertension: 54.0%; rheumatic disease and joint diseases: 47.7%, allergic disorders: 37.9%; fibromyalgia: 33.1%; varicose veins of the lower limbs: 29.8%; labyrinthitis: 29.8%, diabetes: 15.3%; disc herniation: 14.5%, cancer of the uterus / ovaries / breast: 13.7%, and the breast represents 47.05% of these cancers, other cancers: 2.4%.
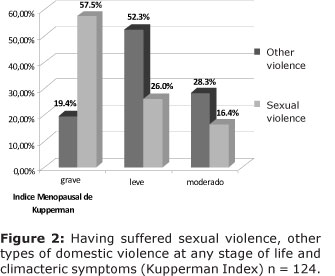
With reference to the intensity of climacteric symptoms: 53.2% of the women have moderate MKI ,25.8% light and 21% severe. Higher percentages in the Menopausal Kupermann Index (MKI) were determined by serious violence inflicted in both phases of life (29.3%), moderate in childhood / adolescence (75%) and adulthood mild (33%) (figure 2).
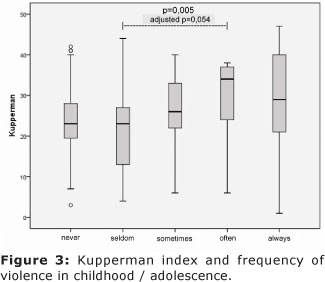
For those who suffered domestic and/or sexual violence in development phase (childhood and adolescence) the climacteric symptoms (measured by the Menopausal Kupperman Index) were associated with frequency of the violence suffered (figure 3).
As for the mood of women at the time of interview, 51.6% of the sample was moderately and sad / depressed, 17.7% a little sad / depressed, 20.9% were moderately joyful/happy , 7.3% felt indifferent and 2.5% could not answer.
The violence suffered showed negative influence on the way of life and behavior of 90.3% of the studied women .
Among the various episodes of violence that women suffered the one that most severely affected their physical and psychological health was the category "being battered/abused by a man who is the father of my child" (38.7%), followed by "Having suffered multiple trauma/violence by someone who brought me up or adopted me."(33.1%), "Having suffered humiliation, verbal abuse, slander". (25%),"Being battered by/suffered for a person whom I loved and / or still love" (24.2%), and "Having been abused/raped by someone close by someone close, known and/or family" (17.7%). 80.6% of the sample did not seek health services when they suffer violence.
As for the action of health professionals in addressing violence, 75% of women reported that they would have asked for help if the professional had discussed violence during attendance and 17.7% said they would not tell about the violence, even if questioned. These women suggested that: 58.1% "professionals need to be more open for people to talk; they need to show more assurance," 20.2% "The professionals must encourage women not to accept violence and denounce this violence."
The Chi-square test showed no association between having suffered sexual violence and presenting moderate and mild, Menopausal Kuppermann Index but those who have suffered sexual violence displayed a stronger association with severe Kupperman Index(p=0,001)
As for smoking, there is no difference between the distributions of the number of comorbidities and Menopausal Kupermann Index in smokers and nonsmokers (p = 0.094) and (p = 0.181) respectively.
Among those who had only physical violence, the most frequent disease was depression and chronic immunological background (39.5%). The same was observed in those who only suffered sexual violence, with the levels of depression and fibromyalgia significantly higher (p <0.001) in this group.
Worldwide, the power of the stronger over the weaker, has always made clear its degree of importance, whether in the universal capital, in society, policies and family. That is, power and the search for excesses in the attitudes of the human being may go beyond the limits considered as normal for ourselves, which adds to the little importance given to children, adolescents and women, and the consequent impact of these attitudes especially of adults on the health of their victims.
Gender-based violence within the family environment and outside it, leads women to several physical , psychological, social disorders, out of shame of being exposed or fear of rupture of family bond, or caused by threat, which makes the abused person keep silence. Such panorama unfortunately suggests that millions of women are suffering from this type of violence and living with its consequences.
The results of this study reflect not only differences between the types and consequences of violence on women's health during menopause, which are being evaluated, but also underscores the magnificence of sexual violence occurring at any stage of life. The sexual practice, that deserves significant attention, can present itself in various forms of relationships, such as excessive search for selfish pleasure, creating new situations and experiences, irrespective of it going beyond respect to ethics and morality in relation to others, whether or not within family bond. Some women experience sexual violence by their husbands/partners once they are made to have sexual intercourse under threat or physical violence , not rarely yielding to undesired sexual practices.
The interference of the health professional at 'windows of opportunity' are essential for the rupture of the process of violence. The emotional neglect reported by approximately one third of the studied women can be easily seen in medical visits, especially gynecology, when the professional during the interview, on the finding of the patient being divorced or separated, questions the reasons for this separation. Depending on the doctor-patient bond the woman opens her heart and then she may be asked : nowadays, how is the heart, your sexuality, feelings? What would you change in your life if you could?
By taking down the woman's age, the professional can probe feedback by asking, for example, as she and her partner celebrate your birthday, and may have as an answer that the partner routinely forgets the event and other important events for the patient, which would enable the detection of emotional neglect, that just like sexual violence, continues unnoticed by many health professionals, leading to serious implications for women's health. In addressing the process of violence, one should take into account social determinants such as access to health services and security, marital status, home environment, extra-domestic activities carried out and others. Health services therefore become privileged spaces where professionals can break the covenant of silence and the cycle of violence.
The quest for understanding the relationship of trauma/violence occurring throughout life and the genesis/exacerbation of certain comorbidities, may assist in directing the training, both initial and continued under the various categories/specialties professionals interact in the treatment of women in any stage of life1. Academic training does not prioritize discussions on this subject and the improvement and capacity building are dependent mainly on the needs and interests of the professional. The lack of knowledge to suspect the existence of problem or make the diagnosis, does not generate the notification, and without notification there is no adequate treatment and monitoring, and it is neither possible to intervene or to prevent violence.
It was possible to observe that he women who suffered domestic or sexual violence at any point of life display higher number of comorbidities during the climacteric and higher MKI than those who were not exposed to violence.The instrument of measurement/evaluation of the consequences of violence on women's quality of life must involve processes and steps that need to be well structured and reasoned so that there be no loss in data analysis. The questionnaire used in this work proved to be consistent on being able to propose several complementary lines of reasoning and show how those are jointly present in the thought of the respondents. After the application of the questionnaire many women expressed relief and some comfort, for having had the opportunity and confidence to open up to someone about this trauma, even if they cried during the application. From this stage on feel more secure and confident in the proposed therapy.
CONCLUSION
Among the types of violence the sexual, is the one that entails the worst consequences for climacteric women's health. The frequency of domestic and or sexual violence in the development phase, is associate to higher scores in the MKI. Women who suffered domestic violence at any point of their lives display a higher number of comorbidities such as: depression, psychiatric disorders, unsatisfactory sexual life, fibromyalgia, rheumatic disease, artramialgy, persistence of sleep disorders, arterial hypertension, allergic affection, labyrinthitis, uterus, ovaries, breath cancer, an comparison with those that those did not experience violence.
The present study did not aim at proving causal relation between violence and the development of comorbidities by climaretic women. Nevertheless, it raises important hypothesis for the development of further work that contemplate better understanding of violence and genesis of the associate of comorbidities, including the implications for the quality of life of these women.
ACKNOWLEDGEMENTS
CNPq for the Service of Endocrine Gynecology and Climacteric of the Hospital das Clinicas, Medical School of USP,Maria Elisa Lippe C de Oliveira , Eli Mendes de Moraes and Eleonora Menegutti, which greatly contributed in different ways for this research.
REFERENCES
1. Moraes SD, Fonseca AM, Júnior JMS, VICENTE AP, Souza MA, Arie WMY, et al. Construction and Validation of an instrument that breaks the silence: The impact of domestic and/or sexual violence on women's health, as show during climaterium. Menopause (New York, N.Y.). v.1, p.75, 2011. DOI: 10.1097/gme.0b013e 3182214e12 [ Links ]
2. Sousa RL, Sousa ESS, Silva JCB. Fidedignidade do teste-reteste na aplicação do Índice Menopausal de Blatt e Kupperman. Rev Bras Ginecol Obstet. 2000, 22(8):481-7. DOI: 10.1590/S0100-72032000000800003 [ Links ]
3. Garcia-Moreno C, Jansen HA, Ellsberg M, Heise L, Watts CH et al. Prevalence of intimate partner violence: findings from the WHO multi-country study on women's health and domestic violence. Lancet;368(9543):1260-9, 2006. DOI: 10.1016/S0140-6736(06)69523-8 [ Links ]
4. Silva Filho CR, Baracat EC, Conterno LO, Haidar MA, Ferraz MB. Climacteric symptoms and quality of life: validity of Women's Health Questionnaire. Rev Saúde Pública; 39(3):333-9, 2005. DOI: 10.1590/S0034-89102005000300002 [ Links ]
5. Campbell JC, Health consequences of intimate partner violence. The Lancet, Vol 359, April 13, 2002. DOI: 10.1016/S0140-6736(02)08336-8 [ Links ]
6. Mouton CP, Rodabough RJ, Rovi SLD, Brzyski RG, Katerndahl DA. Psychosocial Effects of Physical and Verbal Abuse in Postmenopausal Women. Annals of Family Medicine, vol. 8, no. 3, 2010. DOI: 10.1370/afm.1095 [ Links ]
7. Walker R, Shannon L, Logan TK. Sleep Loss and Partner Violence Victimization. J Interpers Violence. 2010. DOI: 10.1177/0886260510372932 [ Links ]
8. Ellsberg M, Jansen HAFM, Heise L, Watts CH, Moreno CG. Intimate partner violence and women's physical and mental health in the WHO multi-country study on women's health and domestic violence: an observational study, Lancet; 371: 1165 - 72, 2008 DOI: 10.1016/S0140-6736(08)60522-X [ Links ]
9. Reed E. Intimate partner violence: a gender-based issue? Am J Public Health; 98(2): 197-8; author reply 198-9, 2008. DOI: 10.2105/AJPH.2007.125765 [ Links ]
10. Greenfield EA, Marks NF. Profiles of physical and psychological violence in childhood as a risk factor for poorer adult health: evidence from the 1995-2005 National Survey of Midlife in the United States. J Aging Health; 21(7): 943-66, 2009. DOI: 10.1177/0898264309343905 [ Links ]
11. Albers G, Echteld MA, de Vet HC, Onwuteaka-Philipsen BD, van der Linden MH, Deliens L. Evaluation of quality-of-life measures for use in palliative care: a systematic review. Palliat Med 24: 17-37, 2010. DOI: 10.1177/0269216309346593 [ Links ]
12. Durrant JE, Trocmé N, Fallon Barbara, Milne C, Black T, Knoke D. Punitive Violence Against Children in Canada. Public Health Agency of Canada - Technical Paper Series, 2006. [ Links ]
13. Finkelhor D, Ormrod RK, Turner HA. Re-victimization patterns in a national longitudinal sample of children and youth. Crimes against Children Research Center, University of New Hampshire, 2006. DOI: 10.1016/j.chiabu.2006.03.012 [ Links ]
14. Wolfe DA. , Crooks CV, Lee V, McIntyre-Smith A, Jaffe PG. The Effects of Children's Exposure to Domestic Violence: A Meta-Analysis and Critique. Clinical Child and Family Psychology Review 6 (3): 171-187, 2003. DOI: 10.1023/A:1024910416164 [ Links ]
15. Schraiber L B, D'Oliveira AFPL, França-Junior I, Diniz S, Portella AP, Ludermir AB et al. Prevalence of intimate partner violence against women in regions of Brazil. Rev. Saúde Pública. Oct; 41(5): 797-807, 2007. DOI: 10.1590/S0034-89102007000500014 [ Links ]
16. Pérez IR, Castanõ JP, Lozano MR. Physical health consequences of intimate partner violence in Spanish women. European Journal of Public Health, Vol. 17, No. 5, 437 - 443, 2007. DOI: 10.1093/eurpub/ckl280 [ Links ]
17. Grassi-Oliveira R, Stein LM, Pezzi JC. Tradução e validação de conteúdo da versão em português do Childhood Trauma Questionnaire/ Translation and content validation of the Childhood Trauma Questionnaire into Portuguese language. Rev Saude Publica; 40(2): 249-255, abr. 2006. DOI: 10.1590/S0034-89102006000200010. [ Links ]
18. Dhakal S. Nepalese women under the shadow of domestic violence. The Lancet Vol 371 February 16, 2008. DOI: 10.1016/S0140-6736(08)60254-8 [ Links ]
19. Bossarte RM; Swahn MH; Choudhary E. The associations between area of residence, sexual violence victimization, and asthma episodes among US adult women in 14 states and territories, 2005-2007. J Urban Health; 86(2): 242-9, 2009. DOI: 10.1007/s11524-008-9340-5 [ Links ]
20. Bernstein DP, Stein JA, Newcomb MD, Walker E, Pogge D, Ahluvalia T, et al. Development and validation of a brief screening version of the childhood trauma questionnaire. Child Abuse Negl.27(2):169-90, 2003. DOI: 10.1016/S0145-2134(02)00541-0 [ Links ]
21. Moraes, SDTA et al. Acolhendo o acolhedor: o caminho mais curto para a humanização da assistência. Rev Bras Crescimento Desenvolv Hum. 2009; 19(3): 393-402. ISSN: 0104-1282 [ Links ]
 Corresponding author:
Corresponding author:
sandradi@usp.br
Manuscript submitted Jan 02 2011
Accepted for publication Apr 30 2012
