










Serviços Personalizados
Journal

artigo
 Inglês (pdf)
Inglês (pdf)
 Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
Indicadores
Compartilhar

 Permalink
PermalinkJournal of Human Growth and Development
versão impressa ISSN 0104-1282versão On-line ISSN 2175-3598
J. Hum. Growth Dev. vol.26 no.1 São Paulo 2016
https://doi.org/10.7322/jhgd.110421
ORIGINAL RESEARCH
Concurrent validation of the MABC-2 and Developmental Coordination Disorder Questionnaire-BR
Ana Paula Pietro Nobre MontoroI; Renata CapistranoI, * ; Elisa Pinheiro FerrariII; Monalisa da Silva ReisI; Fernando Luiz CardosoII; Thais Silva BeltrameI
IUniversity of the State of Santa Catarina-UDESC / Graduate Program in Human Movement Sciences - PPGCMH Laboratory of / Learning and Development Disorders - LADADE
IIUniversity of the State of Santa Catarina -UDESC / Graduate Program in Human Movement Sciences - PPGCMH Graduate Program in Education - PPGE / Laboratory of Gender and Sexuality - LAGESC
ABSTRACT
INTRODUCTION: The Movement Assessment Battery for Children, Second Edition (MABC-2) has been widely used in national literature for the diagnosis of Developmental Coordination Disorder (DCD). The relationship of MABC-2 with the scientific gold standard instrument for DCD, the Brazilian version of the Developmental Coordination Disorder Questionnaire (DCDQ-BR), is not well established and is rather controversial.
OBJECTIVE: The aim of this study was to verify the concurrent validity of the MABC-2 motor battery and the DCDQ-BR, controlled for sex and age group.
METHODS: The concurrent validation process took place with the participation of 350 schoolchildren aged 7-11 years from the cities of Florianopolis-SC and Manaus-AM and their parents or guardians. The agreement between instruments was assessed with the Spearman correlation test and simple linear regression using SPSS software version 20.0.
RESULTS: Positive correlation between instruments´ scales was found.
CONCLUSION: This study showed evidence of concurrent validity between MABC-2 and DCDQ-BR, suggesting that MABC-2 can be used as an indicator for developmental coordination disorder.
Keywords: validation; MABC-2; DCDQ-BR; motor performance.
INTRODUCTION
The study of motor development is a prerequisite for the full understanding of children's evolution, in which movement is an integral part of life1. Therefore, motor assessment is important and necessary in preschool individuals2 and has been explored in several national3-7 and international studies8-10.
One of the test protocols most widely used in this area to evaluate motor performance is the Movement Assessment Battery for Children - Second Edition (MABC-2), developed in the UK to identify motor difficulties in children aged 3-16 years through the following skills: manual dexterity, ball skills, and static and dynamic balance, organized according to each age group11. MABC-2 is a widely used tool in both national3-5 and international studies8-10.
In Brazil, MABC-2 has been used for the diagnosis of developmental coordination disorder (DCD)3-5. However, this is not a unique tool for assessment of this disorder, but rather of motor problems as a whole. One of the instruments considered the gold standard for diagnosis of DCD is the Developmental Coordination Disorder Questionnaire (DCDQ), developed in Canada12 for children aged 5-15 years. It is a questionnaire for parents composed of 15 items related to a child's performance in various everyday activities. Questions are designed to assess three categories: motor control during movement, fine/written motor skills, and general coordination. The instrument has been validated in various countries, such as Australia13, China14, Germany15, Israel16, Japan17, and Brazil18. However, the fact that the instrument uses replies provided by parents or guardians, who may not always have the availability or even knowledge to fill out the questionnaire, compels the researcher to use other tools for diagnosis of DCD that do not require active parental participation. Thus, the increasing use of the MABC-2 motor battery for diagnosis of DCD has been observed.
In light of this information, some studies have verified the concordance between the MABC-2 motor battery and the gold standard, DCDQ19. In the Netherlands, authors found a high correlation between DCDQ and MABC-2 in children aged 6-11 years20. In China, researchers evaluated 1.823 children and found that the MABC-2 motor battery and DCDQ were correlated, concluding that MABC has good reliability and validity. In Brazil, a pioneer study developed by Capistrano et al.19 did not reveal significant congruence between the MABC-2 motor battery and DCDQ-BR. Given this lack of consensus, the present study seeks to provide a basis for growth and assessment consolidation in motor performance. Thus, the aim of the present investigation was to analyze the concurrent validity of the MABC-2 motor battery with DCDQ-BR according to sex and age group.
METHODS
Study characterization
This study was conducted as part of a project entitled "Concurrent validation of the MABC-2, according to the Developmental Coordination Disorder Questionnaire Brazil," which was approved by the protocol number 38772214.3.0000.0118.
Participants
The study included 350 children (175 girls and 176 boys) aged 7-10 years enrolled in public and private elementary schools of Florianópolis - SC and Manaus - AM and their parents or guardians.
Inclusion criteria were age between 7 and 10 years; agreeing to participate in the study; not presenting physical problems that prevented evaluation of the motor performance; returning the free and informed consent form signed by parents or guardians.
Characterization of different environments
Florianopolis/SC and Manaus/AM were chosen because of their contextual differences. These cities differ in their physical structure and therefore in the academic structure among schools. For example, in the schools of Florianópolis/SC, students have courtyards, playgrounds, indoor courts, swimming pools, and physical education classes three times a week taught by teachers. This set of elements could provide new and diversified motor experiences. In the schools of Manaus/AM, students have only courtyards and twice weekly physical education classes taught by teachers.
Tools
To evaluate motor performance, the MABC-2, and the Developmental Coordination Disorder Questionnaire-Brazil (DCDQ-BR) were used and presented as follows:
Movement Assessment Battery for Children, 2nd edition
The MABC-2 is a motor test protocol developed by Henderson21 for intervention in children aged 3-16 years with DCD and other motor problems. It consists of a movement battery, a checklist, and a manual. The MABC-2 is organized into three age-specific sections: 3-6 years, 7-10 years, and 11-16 years. The test refers to a series of tasks (manual dexterity, ball skill, and static and dynamic balance), assigned to a value as number of attempts, hits and misses, or time spent to perform the tasks. The test categorizes children according to their level of motor difficulty. The score varies from 1 to 19, and for each value, there is a corresponding percentage that may vary from 0.1% to 99.9%. A score at or below the fifth percentile is the cutoff point for severe motor difficulties, such as DCD; values between the sixth and fifteenth percentile are considered to indicate risk for the development of motor difficulties; performance at or above the sixteenth percentile indicates that there are no motor difficulties21. For this study, only the motor battery with tasks specific for the age group 7-10 years was used, and children were categorized into two categories: defined motor problem (risk for the development of difficulties and motor problems) and normal motor performance (no motor difficulties).
Developmental Coordination Disorder Questionnaire
DCDQ is a questionnaire for parents, designed to detect DCD in children aged 5-15 years. Created by Wilson12, it consists of 15 items divided into 3 categories: motor control, fine/written motor skills, and general coordination. According to the standard protocol for DCDQ administration, parents are instructed to fill out the questionnaire and mark the answers on a Likert scale from 1 to 5 points, which describes the child's performance on that task. The final score is the sum of the scores of each item, which varies from 15 to 75 points. The total score indicates whether the child is in the group with indicative or suspected DCD or probably no DCD, according to the three cutoffs across age groups. In the group aged 5-7 years and 11 months, a score of 0-46 indicates that the child has DCD or suspected DCD while a score of 47-75 indicates that the child probably does not have DCD. From the age of 8 to 9 years and 11 months, a score 0-55 identifies children who have, or are suspected of having, DCD. In the oldest group, 10-13 years and 11 months, a score of 0-57 indicates that a child has or is suspected of having DCD. In this study, children who have, or are suspected of having DCD, were considered to have a defined motor problem and those who did not were considered to have normal motor performance.
Procedures
Motor assessments were individually performed during physical education classes in the period from September to November 2014 in educational institutions. Students were assessed in a large room with free space, which allowed researchers to conduct the whole test protocol in the same place; this was designed to reduce potential interference. After application of the battery, parents or guardians received a printed copy of the DCDQ-BR questionnaire with a letter explaining how to fill out the instrument and how to contact the researchers in case of further questions.
Statistical analysis
Data were tabulated in the Statistical Package for Social Sciences (SPSS) ® software, version 20.0. To characterize data, descriptive statistics were used to compare means of relative and absolute frequencies.
The concurrent validity of MABC-2 and DCDQ-BR by sex and age group was assessed using the Spearman correlation test. The reference values for this analysis were as follows: below 0.40, weak correlation; between 0.40 and 0.59, moderate correlation; between 0.60 and 0.80, good correlation; and above 0.80, very good correlation.
In order to check the predictive power of MABC-2 for identifying the DCD in children, a simple linear regression analysis was performed. The independent variable was the total score on the MABC-2 test and the dependent variable was DCDQ-BR scores, the gold standard for identification of DCD. A p value <0.05 was considered statistically significant.
RESULTS
A total of 155 schoolchildren from the city of Manaus, including 81 girls with a mean age of 8.77 (± 1.22) years and 74 boys with a mean age of 8.74 (± 1.12) years, and 195 schoolchildren from the city Florianópolis, including 94 girls with a mean age of 9.09 (± 1.08) years and 101 boys with a mean age of 8.87 (± 1.06) years, were assessed.
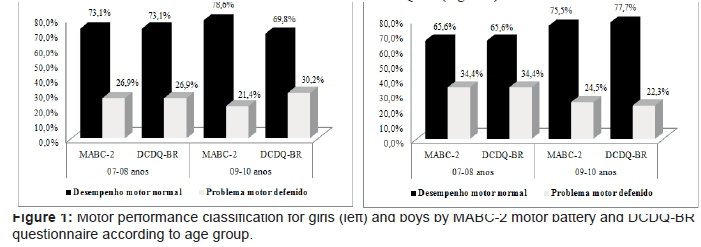
Figure 1 shows the motor performance classification assessed using MABC-2 and DCDQ-BR according to sex and age group. In the assessment of the MABC-2 motor battery in the age group of 7-8 years, 26.9% of girls and 34.4% of boys were classified as having a defined motor problem; the DCDQ -BR questionnaire yielded similar findings.
For the age group of 9-10 years, 21.4% of girls and 24.5% of boys were classified as having a defined motor problem according to MABC-2 and 30.2% of girls and 22.3% of boys were classified as such according to DCDQ-BR (Figure 1).
When comparing the MABC-2 motor battery and DCDQ-BR for girls in the age groups 7-8 years and 9-10 years, positive correlations between total score and the standard score of MABC-2 according to the DCDQ-BR for the age group of 7-8 years (total, r = 0.47; p = 0.01; standard, r = 0.45; p = 0.01) and 9-10 years (total, r = 0.32; p = 0.01; standard, r = 0.35; p = 0.01) was observed, respectively (Table 1).
Table 2 shows the correlations between MABC-2 motor battery (total score and standard score) and DCDQ-BR for men aged 7-8 years and 9-10 years. The results show a significant positive correlation between total score and the standard score of MABC-2 according to the DCDQ-BR for the age group of 7-8 years (total, r = 0.62; p = 0.01; standard, r = 0.61; p = 0.01) and 9-10 years (total, r = 0.35; p = 0.01; standard, r = 0.37; p = 0.01) (Table 2).
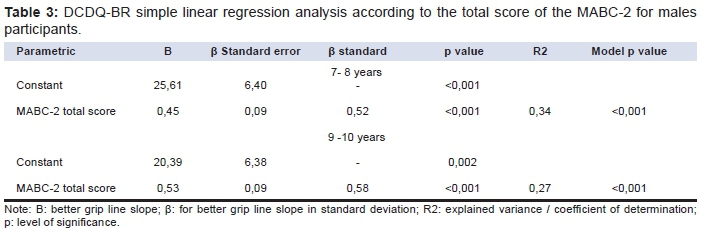
From the simple linear regression analysis, it was possible to infer the predictive ability of MABC-2 to identify the presence or risk of the development of DCD in children. The regression model showed statistically significant results for boys between the ages of 7 and 8 years and 9 and 10 years (p < 0.05) (Table 3), with the largest coefficient of determination observed for the newest (R2 = 0.34) compared to older participants (R2 = 0.27) (Table 3).
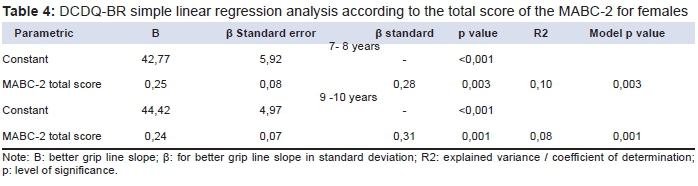
In females, the regression model yielded statistically signifi cant results for ages 7–8 years and 9–10 years (p < 0.05). However, when compared to the coeffi cient of determination (R2) similar values were observed for ages 7–8 years and 9-10 years (R2 = 0.10 and R2 = 0.08, respectively) (Table 4).
DISCUSSION
This study contributes to knowledge in this field by demonstrating that there is a positive and significant correlation between MABC-2 and DCDQ-BR total scores, regardless of sex or age group. This suggests that DCDQ-BR provides a useful validity criterion, since motor performance is part of its construct, overall development disorders. This result is consistent with findings of other studies conducted in children aged 5-15 years13,22 that generated similar results ( p = 0.01). Schoemaker et al.20 assessed children aged 5-8 years and found smaller albeit a significant correlation between MABC and DCDQ (r= 0.36; p < 0.001). A smaller study of Brazilian children conducted by Capistrano et al.19 found no association between the instruments. These discrepancies may be related to methodological aspects, such as small group sizes. The present research, which includes a much larger sample of children, provides strong evidence for the concurrent validity between MABC-2 and DCDQ-BR in children from two Brazilian states.
The regression between the total punctuationof MABC-2 and DCDQ-BR scores showed evidence that general coordinative disorders in children can be in part explained by the MABC-2 motor test performance. That is, MABC-2 may explain and also predict which children can have or will have some general developmental coordination disorders, mainly between boys that presented higher determination coefficient with regards to girls. Therefore, this study provides evidence that MABC-2 can be used as an indicator for DCD. Furthermore, owing to its association with the DCDQ-Br, the MABC-2 serves as a good indicator for children with general coordinative disorders, providing a preliminary diagnosis that can be used to identify specific Brazilian children who may need specific clinical or pedagogical approaches. By using MABC-2 to identify the children with the highest risk early on, we can create opportunities for the development of appropriate intervention strategies.
Given that our results confirm findings in national and international literature, we can say with confidence that the compared instruments in this study have a good reliability. Regarding the prevalence of motor disorders according to biological sex, the results indicate agreement with global estimates of higher prevalence of motor disorders among boys23. These data are consistent with those from other studies24 showing higher incidence of DCD among boys. Data from the World Health Organization (WHO) indicate that motor difficulty occurs more frequently in boys (four or five boys for every girl). Confirming this predisposition in boys3 an evaluation of 380 scholars in Florianópolis/SC showed that the boys showed lower performance than girls. Green et al.25 assessed 4,331 English children, among whom 173 were considered to have motor difficulty; of these students, 60.6% were boys and 40.4% were girls.
There is no clear explanation for this higher prevalence of motor difficulty among boys in the current literature. However, Zwicker et al.23 found some evidence that low motor performance may be more common in children born with low birth weight or premature children. In addition, this study showed an increased risk of neurological damage among boys born with these conditions. As such, a higher prevalence of motor difficulty in boys may be attributable to effects in early life and infancy.
We observed that children's maturation process decreased the association between MABC-2 and DCDQ-BR. That is, the MABC-2 had better predictive power in younger children than in older children who participated in this study. With regard to motor performance classification by applying the MABC-2 motor battery and DCDQ-BR questionnaire, the prevalence found was the same for the age group of 7-8 years in both sexes, suggesting that, despite the methodological differences between instruments, MABC-2 is a good indicator for the diagnosis of DCD in children aged 7-8 years. These results are surprising, given that DCDQ is considered the gold standard for evaluation of DCD in this population. In males aged 9-10 years, MABC-2 classified more children with motor problem than DCDQ-BR; however, the difference was small: < 10 percentage points.
Cardoso, Magalhães, and Rezende26 assessed 793 Brazilian children aged 7-8 years and found no differences in the DCD classification between DCDQ and MABC-2; 34 children were considered to have DCD by both instruments. However, other studies have shown larger differences regarding the prevalence of motor problems among children between the two instruments. Pannekoek et al.22 and Capistrano et al.19 suggested that this discrepancy can be explained due to methodological aspects used in the construction of the research tools27 as well as varying cutoff points used to identify problems in different motor tests.
With regard to the fact that differences between instruments were only observed in the 9-10-year-old group, we suggest two possible explanations. The natural course of child development may decrease the strength of the associations between motor performance and general motor disorder. Alternatively, increased independence in older children may decrease the amount of time that parents and guardians spend surveilling their behavior. The DCDQ is filled out by parents or guardians, who may not play an active role in the children's daily life by the age of 7-8 years.
The lack of sample representativeness is the main limitation of this study, which prevents extrapolation of data conclusions. Additional studies of a representative sample are required in order to confirm data obtained in the current research. Another limitation is the lack of longitudinal follow-up data to confirm the capability of MABC in predicting general developmental coordination disorders. This criterion validation can be conducted in two possible ways, either by accompanying children through their life until adolescence, or by transversely applying the same tests in children with a definitive clinical diagnosis of a developmental disorder.
ACKNOWLEDGEMENTS
Fundação de Amparo à Pesquisa e Inovação do Estado de Santa Catarina - FAPESC 2015 TR 390.
REFERENCES
1.King Dowling S, Rodriguez MC, Missiuna C, Cairney J. Validity of the Ages and Stages Questionnaire to detect risk of Developmental Coordination Disorder in preschoolers. Child: Care, Health Dev. 2015;1-7. DOI: http://dx.doi.org/10.1111/cch.12314 [ Links ]
2.Caçola P, Romero H, Ibana H, Chuang J. Effects of two distinct group motor skill interventions in psychological and motor skills of children with Developmental Coordination Disorder: A pilot study. Disabil Health J. 2015;9(1):172-8. http://dx.doi.org/10.1016/j.dhjo.2015.07.007 [ Links ]
3.Miranda TB, Beltrame TS, Cardoso FL. Desempenho motor e estado nutricional de escolares com e sem transtorno do desenvolvimento da coordenação. Rev Bras Cineantropom Desempenho Hum. 2011;13(1):59-66. DOI: http://doi.org/10.5007/1980-0037.2011v13n1p59 [ Links ]
4.Santos VAP, Vieria JLL. Prevalência de desordem coordenativa desenvolvimental em crianças com 7 a 10 anos de idade. Rev Bras Cineantropom Desempenho Hum. 2013;15(2):233-42. DOI: http://doi.org/10.5007/1980-0037.2013v15n2p233 [ Links ]
5.Silva J, Beltrame TS. Indicativo de transtorno do desenvolvimento da coordenação de escolares com idade entre 7 e 10 anos. Rev Bras Ciênc Esporte. 2013; 35(1):3-14. DOI: http://doi.org/10.1590/S0101-32892013000100002 [ Links ]
6.Nascimento EMF, Contreira AR, Silva EVA, Souza LPD, Beltrame TS. Desempenho motor e estado nutricional em escolares com transtorno do déficit de atenção e hiperatividade. J Hum Growth Dev. 2013;23(3):358-64. DOI: http://dx.doi.org/10.7322/jhgd.69514 [ Links ]
7.Silva J, Beltrame TS, Oliveira ADVPD, Sperandio FF. Dificuldade motoras e de aprendizagem em crianças com baixo desempenho escolar. J Hum Growth Dev. 2012; 22(1):41-46. [ Links ]
8.Engel-Yeger B, Hanna KA. The relationship between Developmental Co-ordination Disorders, child's perceived self-efficacy and preference to participate in daily activities. Child: Care, Health Dev. 2010; 6(5):670-7. DOI: http://doi.org/10.1111/j.1365-2214.2010.01073.x [ Links ]
9.Jarus T, Lourie-Gelberg Y, Engel-Yeger B, Bart O. Participation patterns of school-aged children with and without DCD. Res Dev Disabil. 2011;32(4): 1323-31. DOI: http://doi.org/10.1016/j.ridd.2011.01.033 [ Links ]
10.Liu T, Breslin CM. The Effect of a Picture Activity Schedule on Performance of the MABC-2 for Children With Autism Spectrum Disorder. Res Q Exerc Sport. 2013;84(2):206-12. DOI: http://doi.org/10.1080/02701367.2013.784725 [ Links ]
11.Henderson SE, Sugden DA, Barnett A. Moviment Assessment Battery for Children-2 (2nd ed). London: The Psychological Corporation; 2007. [ Links ]
12.Wilson B, Dewey D, Campbell A. Developmental coordination disorder questionnaire (DCDQ). Canada: Alberta Children's Hospital Research Center; 1998. [ Links ]
13.Civetta LR, Hillier SL. The developmental coordination disorder questionnaire and movement assessment battery for children as a diagnostic method in Australian children. Pediatr Phys Ther . 2008;20(1): 39-46. http://doi.org/10.1097/PEP.0b013e31815ccaeb [ Links ]
14.Tseng MH, Fu CP, Wilson BN, Hu FC. Psychometric properties of a Chinese version of the developmental coordination disorder questionnaire in community-based children. Res Dev Disabil. 2010;31(1):33-45. http://doi.org/10.1016/j.ridd.2009.07.018 [ Links ]
15.Kennedy-Behr A, Wilson BN, Rodger S, Mickan S. Cross-cultural adaptation of the Developmental Coordination Disorder Questionnaire for brazilian children. Neuropediatrics. 2013; 44(5): 245-51. DOI: http://doi.org/10.1055/s-0033-1347936 [ Links ]
16.Traub R, Levi A, Parush S. Validity and reliability of the developmental coordination disorder questionnaire for school-aged children in Israel. Isr J Occup Ther. 2005; 14(4): H175-91. [ Links ]
17.Nakai A, Miyachi T, Okada R, Tani I, Nakajima S, Onishi M, et al. Evaluation of the Japanese version of the Developmental Coordination Disorder Questionnaire as a screening tool for clumsiness of Japanese children. Res Dev Disabil. 2011;32(5):1615-22. DOI: http://doi.org/10.1016/j.ridd.2011.02.012 [ Links ]
18.Prado MS, Magalhães LC, Wilson BN. Cross-cultural adaptation of the Developmental Coordination Disorder Questionnaire for brazilian children. Rev Bras Fisioter. 2009;13(3):236-43. DOI: http://dx.doi.org/10.1590/S1413-35552009005000024 [ Links ]
19.Capistrano R, Ferrari EP, Souza LP, Beltrame TS, Cardoso FL. Concurrent validation of the MABC-2 Motor Tests and MABC-2 Checklist according to the Developmental Coordination Disorder Questionnaire-BR. Motriz: Rev Educ Fis. 2015;.21(1):100-106. DOI: http://dx.doi.org/10.1590/S1980-65742015000100013 [ Links ]
20.Schoemaker MM, Flapper B, Verheij NP, Wilson BN, Reinders-Messelink H, Kloet A. Evaluation of the Developmental Coordination Disorder Questionnaire as a screening instrument. Dev Med Child Neurol. 2006;48(8):668-73. DOI: http://doi.org/10.1017/S001216220600140X [ Links ]
21.Henderson S, Sugden D. Movement Assessment Battery for Children- MABC. London: The Psychological Corporation; 1992. [ Links ]
22.Pannekoek L, Rigoli D, Piek JB, Barret NC, Schoemaker M. The revised DCDQ: Is it a suitable screening measure for motor difficulties in adolescentes. Adap Phys Activ Q. 2012;29(1):81-97. [ Links ]
23.Zwicker JG, Missiuma C, Harris SR, Boyd LA. Developmental coordination disorder: a review and update. Eur J Paediatr Neurol. 2012; 16(6):573-81. DOI: http://doi.org/10.1016/j.ejpn.2012.05.005 [ Links ]
24.Gibbs J, Appleton J, Appleton R. Dyspraxia or developmental coordination disorder? Unravelling the enigma. Arch Dis Child. 2007;92(6):534-9. DOI: http://doi.org/10.1136/adc.2005.088054 [ Links ]
25.Green D, Lingam R, Mattocks C, Riddoch C, Ness A, Emond A. The risk of reduced physical activity in children with probable Developmental Coordination Disorder: a prospective longitudinal study. Res Dev Disabil. 2011;32(4):1332-42. DOI: http://dx.doi.org/10.1016/j.ridd.2011.01.040. [ Links ]
26.Cardoso AA, Magalhães LC, Rezende MB. Motor skills in Brazilian children with developmental coordination disorder versus children with motor typical development. Occup Ther Int. 2014;21(4):176-85. DOI: http://doi.org/10.1002/oti.1376 [ Links ]
27. Pasquali L. Psychometrics. Rev Esc Enferm USP. 2009;43(Spe): 992-9. DOI: http://dx.doi.org/10.1590/S0080-62342009000500002 [ Links ]
Manuscript submitted:Dec 09 2015
Accepted for publication Feb 03 2016.
* Corresponding author: Renata Capistrano. Email: recapis@gmail.com.


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}