










Serviços Personalizados
Journal

artigo
 Inglês (pdf)
Inglês (pdf)
 Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
Indicadores
Compartilhar

 Permalink
PermalinkJournal of Human Growth and Development
versão impressa ISSN 0104-1282versão On-line ISSN 2175-3598
J. Hum. Growth Dev. vol.29 no.2 São Paulo maio/ago. 2019
https://doi.org/10.7322/jhgd.v29.9415
ORIGINAL ARTICLE
Neonatal mortality in Luanda, Angola: what can be done to reduce it?
Ema Cunha RodriguesI; Beatriz da Costa Aguiar AlvesI; Glaucia Luciano da VeigaI; Fernando AdamiII; Juliana Spat CarlessoIII; Francisco Winter dos Santos FigueiredoII; Ligia Ajaime AzzalisIV; Virginia Berlanga Campos JunqueiraIV; Alexandre Luiz Affonso FonsecaI; Fernando Luiz Affonso Fonseca.I, IV, *
ILaboratório de Análises Clínicas da Faculdade de Medicina do ABC, Santo André, SP, Brazil
IILaboratório de Epidemiologia da Faculdade de Medicina do ABC, Santo André, SP, Brazil
IIILaboratório de Delineamento e Escrita Científica, Centro Universitário Saúde ABC (FMABC) - Santo André (SP), Brasil
IVDepartamento de Ciências Farmacêuticas da Universidade Federal de São Paulo, UNIFESP - Diadema, Sao Paulo, Brazil
ABSTRACT
INTRODUCTION: One of the main health indicators is infant mortality rate, which is a metric of living conditions and population development. The goal of reducing neonatal mortality requires an adequate knowledge of the real factors at each level of health care so that maternal and human resources are efficiently channeled to the constraint. Countries that have paid special attention to improving health services for the entire pregnancy-puerperal cycle have attained the reduction of infant mortality, especially early neonatal mortality.
OBJECTIVE: The present study aims to describe the profile and analyze the risk factors associated with neonatal mortality in the Angolan context at a tertiary level public maternity hospital, located in Luanda.
METHODS: This is a retrospective cross-sectional study with a quantitative approach, using secondary data, of provincial base in hospital and ministerial registry instruments from January to December 2012.
RESULTS: The results show that the neonatal deaths are not mere occurrences, since they indicate failures of the political powers, professionals of the health system and of the families.
CONCLUSIONS: This study suggests that the major risk factor for birth mortality in Luanda is the type of delivery (c-section) and that this data is not related to the age of the mother or to premature birth. We also found that there was higher mortality between May and July, during the period of lower rainfall index in the region. However, further studies are needed that may provide a logical framework and arguments for realistic policies to mitigate neonatal mortality.
Keywords: neonatal death, low birth weight newborn, maternal age.
Authors summary
Why was this study done?
We aimed to provide a framework of subsidies that could help understand the risk factors associated with neonatal mortality and to suggest more favorable theoretical and professional positions to drastically reduce the very high rates of neonatal mortality in Angola.
What did the researchers do and find?
Our results suggest the neonatal deaths are not mere occurrences, since they indicate failures of the political powers, professionals of the health system and of the families.
What do these findings mean?
Our findings suggest that public policies to mitigate neonatal mortality should be improved, deployed, and observed.
INTRODUCTION
One of the main health indicators is infant mortality rate, which is a metric of living conditions and population development. The neonatal mortality rate, also known as the neonatal mortality coefficient1, is defined as the total number of deaths in infants under 27 days of age in a given year divided by the total number of live births in the same year and reflects the socioeconomic and health conditions of the mother, the quality of prenatal care, delivery and assistance to the newborn2. Countries that have paid special attention to improving health services for the entire pregnancy-puerperium cycle have attained the reduction of infant mortality, especially early neonatal mortality (up to the 7th day after birth). In 2015, the estimated worldwide neonatal mortality rate was 19 deaths per 1000 live births. In developed countries, mortality rates range from around 3 deaths per 1000 live births, while in developing countries this rate ranges from 6 (East Asia) to 29 (sub-Saharan Africa) deaths / 1000 live births1.
One of the great advances associated with health services in the world context during the twentieth century was the vigorous reduction of infant mortality rates, initially recorded in developed countries and now extended to many developing countries. Indeed, in 2013 it was verified an estimated 6.6 million (6.3-7.0) children under-5 died worldwide. On the other hand, between 1990 and 2013 the under-5 mortality rate declined 47% and between the same period the neonatal mortality rate declined 37% being that one child dies every 20 seconds. Being that most deaths can be attributable to preventable diseases3.
In the 2009 United Nations Children's Fund (UNICEF) Report, an estimated 4 million newborns die each year before they reach 28 days4. From 1990 to 2011, global child mortality fell from almost 12 million to 6.9 million in absolute terms, representing an over 40% decrease in deaths among children under 5 years of age5.
From UNICEF's perspective, the drop was a "significant success" and the results qualified as "dramatic gains" indicate the work of governments, donors, agencies and families. The hypothesis here is that there has been progress in nations across the globe, which shows that economic status is not necessarily a barrier to decreasing these rates, and that mortality can be significantly reduced in two decades. The published data also confirm the improvement of care for mothers and babies in prenatal care, delivery and the first moments after childbirth6. The decline is not homogeneously confirmed in all regions of the world, with very high levels remaining in sub-Saharan Africa. Of the 62 countries that have not made progress or whose progress have been insufficient to achieve the Millennium Development Goal related to reducing child mortality, about 75% are in Africa.
The goal of reducing neonatal mortality and its components requires an adequate knowledge of the real factors at each level of health care so that maternal and human resources can be efficiently channeled to the constraint. For example, in their study Soares and Menezes2 identified low educational level, gestational age and multiple gestations, less than 6 medical consultations, low birth weight and vaginal delivery as the factors that most influenced the outcome in precocious neonatal mortality; Schoeps et al.7, in turn, found that mortality was mainly related to low birth weight, recently married mothers and single mothers and the presence of complications during pregnancy. These data demonstrate that a significant number of factors associated with mortality can be prevented with adequate attention toward pregnancy2. Likewise, there seems to be an association with multiple pregnancy, probably due to low birth weight and prematurity8.
In the category of developing countries is Angola, a country with a population of 24.4 million inhabitants with a fertility rate of 5.7% and life expectancy of 57.2 for men and 63.0 for women. In the recent years Angola has recorded good macroeconomic performances and significant improvements in sanitary infrastructures and public health policies for families, pregnant women and children9. However, between 2011 and 2015, it is estimated that the neonatal infant mortality rate in Angola was 44 deaths per 1000 live births10.
Although several factors such as prenatal medical consultations, prematurity, multiple pregnancies, the male sex and the type of delivery contribute in a combined way to neonatal mortality, knowledge of the weight that each of these factors exerts on the general balance cannot be underestimated; in this way, their identification becomes important to define health measures and policies aimed at reducing mortality. Thus, neonatal mortality being seen as an indicator of quality of life and health services as well as an avoidable event with better prenatal care, delivery and newborn care, besides there being no known Angolan studies, investing in research that provides indicators at the national level to aid decision making is justified. The present study aims to describe the profile and analyze the risk factors associated with neonatal mortality in a tertiary level public maternity hospital, located in Luanda.
METHODS
This is a retrospective cross-sectional study11 with a quantitative approach, using secondary data, of provincial base in hospital and ministerial registry instruments from January to December 2012, at a public maternity from Luanda Province - Angola. This work was approved by Faculdade de Medicina do ABC Ethics Committee (protocol number 2016/308).
The variables studied were parity, gestational age, mother's age, mother's level of education, location of residence (geographical area), socioeconomic conditions, type of delivery, Apgar evaluated at the 1st and 5th minutes, weight, comorbidities, gender, use of legal and illicit drugs, newborn maturity, time of birth of the newborn and time of discharge.
To describe the qualitative variables, we used absolute and relative frequency; for the quantitative variables, median and 25th and 75th percentiles. To analyze the association between child death during childbirth, infant mortality and socio-demographic variables, a chi-square test was used; the Mann-Whitney test and the median confidence intervals were used to analyze the difference in quantitative variables and death of the neonate during delivery. The risk of death of the infant during childbirth and risk of death of the infant according to type of delivery were estimated by means of Poisson regression with robust variance. The level of significance was set at 95%. The statistical program used was Data Analysis and Statistical Software for Professionals (Stata) version 11.0®.
RESULTS
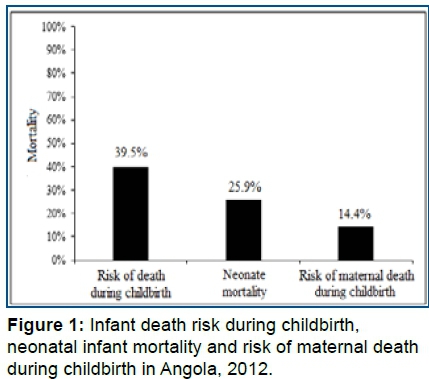
Table 1 describes newborn survival data (up to 27 days) in 2012. Of the 10,989 newborns analyzed, 4,341 (39.5%) died; of these, 1,295 died before the first 27 days (neonatal). Of the neonates with neonatal death, 336 died early (before the 7th day of life) (Figure 1) and Table 1.
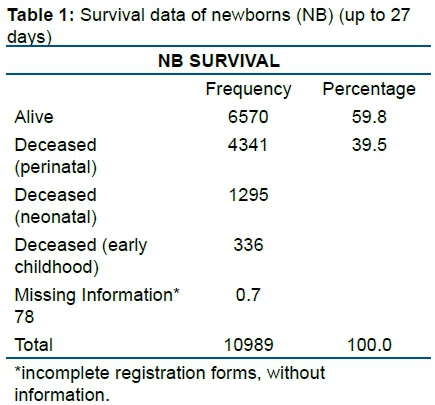
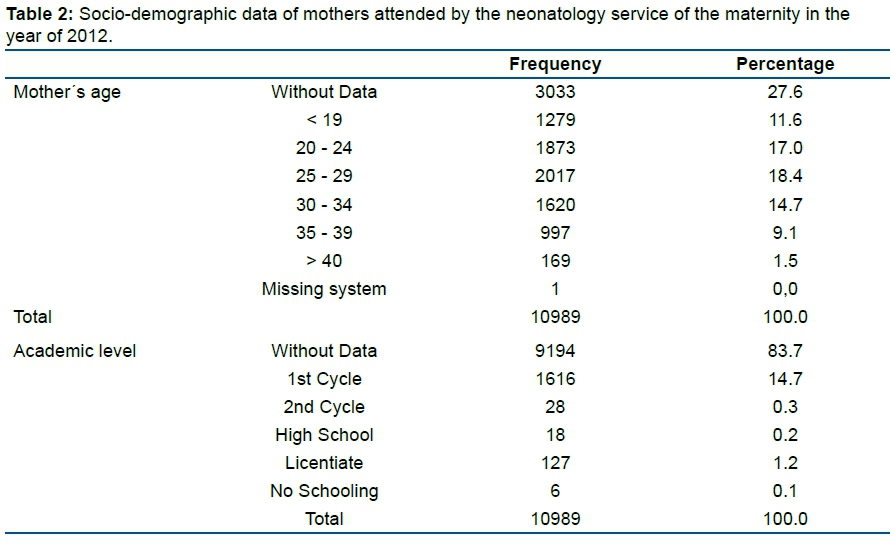
The global death rate for the year 2012 was 21/1000 live births (The World Bank). In 2012, the neonatal mortality rate in Angola was 51.1% (World Data Atlas); Analyzing the data presented above, it is observed that in 2012, in the neonatology service of this maternity, of every 10 infants hospitalized, 4 died before completing the first month of life, of which approximately 30% died in the first week of life. These numbers show the importance of assessing risk factors for neonatal death. The variables found in this study are described in Table 2.
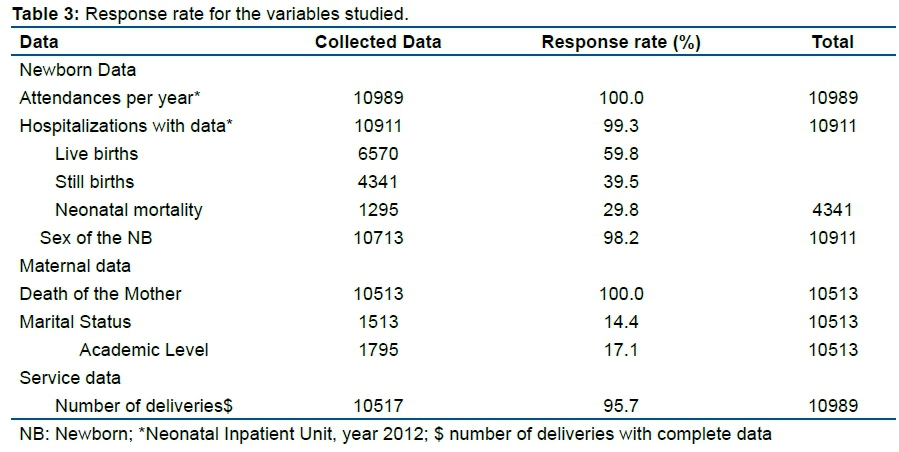
Table 3 shows the response rate of the variables on newborns, mothers and on the service. A low response rate was observed for the variables neonatal infant death (29.8%), marital status (14.4%) and academic level (17.1%) of the mothers, and therefore the results related to these variables should be seen with caution (Table 3).
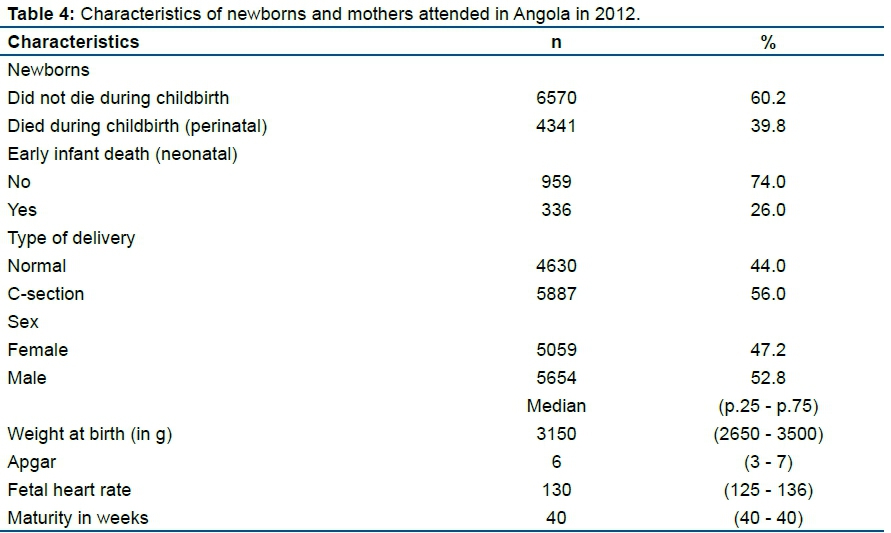
Table 4 presents the profile of newborns and mothers attended in Angola in 2012. Of the newborns, 60.2% survived childbirth and 26% died in the early childhood period (up to the 27th day); 56% were delivered by caesarean section and 52.8% were male. It is claimed that in females the maturation of the fetal lung occurs earlier than in males, increasing in the latter the probability of the occurrence of asphyxia12 (Table 4).
The median (25% and 75% percentiles) of birth weight in grams was 3150 (2650 - 3500), Apgar score was 6 (3-7), fetal heart rate was 130 (125- 136), and 40 (40-40) weeks of maturity (Table 5).
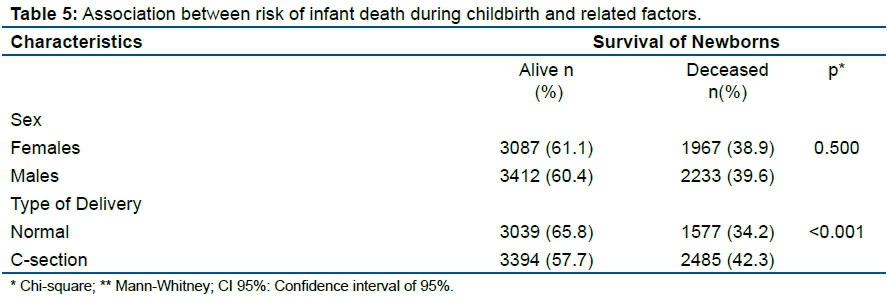
There was no association between risk of neonatal death and sex (p= 0.500), birth weight in g (p= 0.760), fetal heart rate (p= 0.635) and neonatal maturity in weeks (p= 0.543).
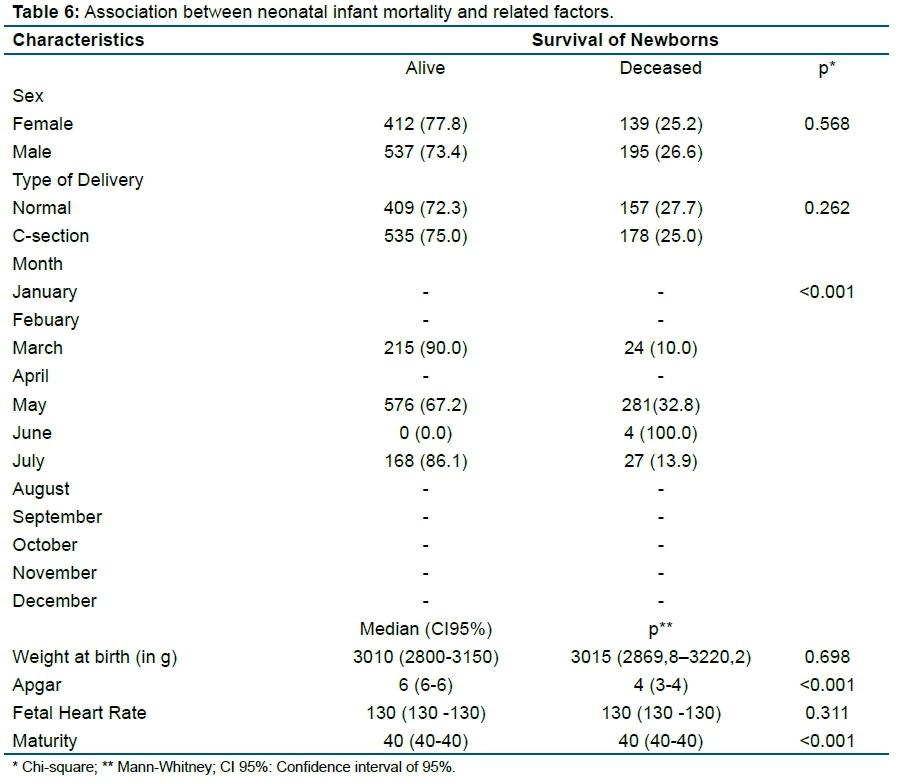
For the factors related to the risk of neonatal infant death, the month of May was observed to present a higher risk of death during childbirth (281 deaths, 32.8% of the total born in this month) (Table 6). It was observed that neonatal deaths are related to Apgar score (p<0.001) and maturity (p<0.001), and those who died presented a median Apgar of 3 to 4 when compared to those who survived, with an Apgar of 6 (Table 6).
DISCUSSION
This Angolan study was carried out with the objective of analyzing the factors associated with mortality in the neonatal period, based on a public health policy focused on neonatal infant mortality, and it is possible to identify mother and newborn variables that increase the risk of death in this period. In 2012, 31,626 deliveries were performed at the maternity where data were collected. Of this total, 10,989 births were included in this study, representing the babies admitted to the Neonatology Unit.
As can be seen, the majority of the mothers assisted in this service live in matrimony (7.1%). Ribeiro et al.13 suggest that the presence of a partner is an important psychosocial factor attributed to lower neonatal mortality due to the financial participation of the partner, as well as in the social acceptance of the mother and the newborn, bringing more support and encouraging the care needed for both.
According to Abuqamar et al.14, the mother's academic level is one of the variables that influence the neonatal mortality rate, since it is an indirect indicator of the socioeconomic status of the family and a predictor of risk for infant mortality. This data corroborates with the results of our study showing 14.7% of mothers with only first cycle education.
Considering maternal age, the results presented here show that the majority of the mothers (18.4%) who lost their children in the first month of life during the study period were between 25-29 years of age. However, according to Ribeiro et al.15, the maternal high-risk age groups for the neonate is below 15 or above 35 years. Data from the neonatology service from this maternity indicate that pregnant women aged 25 -29 have a high rate of eclampsia, a condition that can lead to the death of the newborn. Arterial hypertension and eclampsia are among the complaints reported by mothers upon entering the Emergency service.
Among the factors related to the risk of death of the infant during delivery, it is observed that the caesarean section delivery type (p <0.001) is associated with neonatal death (Table 5). In a study of caesarean sections and maternal and neonatal mortality rates, a statistically significant association between caesarean births and neonatal deaths (p <0.0001) in developing countries was also found16. According to the authors, this relationship was not found in developed countries. Analyzes regarding the type of delivery have generated controversy, but most of the literature indicates that in developing countries where the neonatal mortality rate is high, caesarean section results from conditions that predispose the fetus to fetal distress and infections, and consequently, to death17.
In May 2012 there were many hospitals in Angola without operative blocks, which resulted in all municipalities in Luanda transferring women in complicated labor (eg. bleeding, retroplacental hematoma, placenta praevia, eclampsia, prolonged labor, uterine atony). Many of these women came from the province of Bengo, passing through Catete, Viana, to Luanda where they finally found an operative block; in many cases, the product of conception was lost. With efforts made by the government, it was possible to reverse the situation. Currently, the municipality with the largest number of births in the study already has an operative block, as well as the re-opening of some hospitals, improvement in access, construction and equipping of new hospitals, including this one, which gained one more operating block and another yet to be inaugurated. Considering the Apgar, Li et al.18 also found a significant association between low Apgar scores (1-3) and neonatal mortality.
One of the limitations of this study was the use of data from medical records and death and birth records, which depend on the quality of their completion by professionals, entailing in the absence of data (ignored).
Other authors address the problem in terms of infant mortality and avoidability, reflections of health policies on infant mortality trends, prenatal care, impact of family health strategy on infant mortality rate and the identification of preventable causes that led to fetal and under-one mortalities. For its part, the World Health Organization also draws attention to the keys to neonatal survival19-22.
In the year 2000, the United Nations (UN), in analyzing the major world problems, established eight millennium development goals (MDGs), with MDG four being the reduction of child mortality, which aims to reduce by two thirds the child mortality rate between 1990 and 2015. To achieve MDG four, rapid expansion of child health interventions in various countries is required. To support this process, in addition to increasing frequent monitoring, it is important to promote correct registration of death certificates, as well as to improve the root cause, strengthening national health information systems, allowing improvement in future estimates of infant mortality.
With these data, it will be possible to provide a framework of subsidies that help understand the risk factors associated with neonatal mortality and to suggest more favorable theoretical and professional positions to drastically reduce the very high rates of neonatal mortality in Angola.
We emphasize the importance of studies focused on public health since it has the capacity to identify the sensitive points related to health policies and aim to incorporate viable solutions for the reduction of infant mortality in low income populations.
The present study had as limitations the studied period, which could have been greater, as well as the underreported data (missing information).
CONCLUSION
This study suggests that the major risk factor for birth mortality in Luanda is the type of delivery (c-section) and that this data is not related to the age of the mother or to premature birth. We also found that there was higher mortality between May and July, during the period of lower rainfall index in the region. However, further studies are needed that may provide a logical framework and arguments for realistic policies to mitigate neonatal mortality.
REFERENCES
1.United Nations Children's Fund (UNICEF). World Health Organization (WHO). Levels & Trends in Child Mortality. Estimates Developed by the UN Inter-agency Group for Child Mortality Estimation. [cited 2017 Feb 21]. Available from: https://www.unicef.org/publications/files/Child_Mortality_Report_2015_Web_9_Sept_15.pdf [ Links ]
2.Soares ES, Menezes GMS. Fatores associados à mortalidade neonatal precoce: análise de situação no nível local. Epidemiol Serv Saúde. 2010;19(1):51-60. DOI: http://dx.doi.org/10.5123/S1679-49742010000100007 [ Links ]
3.Guerrera G. Neonatal and pediatric healthcare worldwide: A report from UNICEF. Clin Chim Acta. 2015; 451(Pt A):4-8. DOI: http://doi.org/10.1016/j.cca.2015.03.004 [ Links ]
4.United Nations Children's Fund (UNICEF). Situação Mundial da Infância 2008: sobrevivência infantil. [cited 2017 May 04]. Available from: http://www.crianca.mppr.mp.br/arquivos/File/publi/unicef_sowc/sit_mund_inf_2008_sobrevivencia.pdf. [ Links ]
5.World Health Organization (WHO). Infant mortality: Situation and trends. [cited 2017 March 31]. Available from: http://www.who.int/gho/child_health/mortality/neonatal_infant_text/en/. [ Links ]
6.United Nations Children's Fund (UNICEF). Committing to child survival: a promise renewed. Progress report, 2014. [cited 2014 Aug 25]. Available from: http://passthrough.fw-notify.net/download/561427/http://files.unicef.org/publications/files/APR_2014_web_15Sept14.pdf. [ Links ]
7.Schoeps D, Almeida MF, Alencar GP, França Jr I, Novaes HMD, Siqueira AAF, et al. Fatores de risco para mortalidade neonatal precoce. Rev Saúde Pública. 2007;41(6):1013-22. DOI: http://dx.doi.org/10.1590/S0034-89102007000600017 [ Links ]
8.Bernabé JV, Soriano T, Albaladejo R, Juarranz M, Calle ME, Martı́nez D, et al. Risk factors for low birth weight: a review. Eur J Obstet Gynecol Reprod Biol. 2004;116(1):3-15. DOI: http://doi.org/10.1016/j.ejogrb.2004.03.007 [ Links ]
9.Instituto Nacuional de Estatística (INE): Resultados definitivos do recenseamento geral da população e da habitação de Angola. Censo 2014. [cited 2017 Feb 21]. Available from: http://www.info-angola.com/index.php?option=com_content&view=article&id=4654:resultados-definitivos-do-censo-2014&catid=736&Itemid=1816. [ Links ]
10.Instituto Nacional de Estatística (INE). Ministério da Saúde (MINSA). Ministério do Planeamento e do Desenvolvimento Territorial (MINPLAN) e ICF International. Inquérito de Indicadores Múltiplos e de Saúde em Angola 2015-2016. [cited 2017 Feb 21]. Available from: https://dhsprogram.com/pubs/pdf/PR76/PR76.pdf. [ Links ]
11.Zangirolami-Raimundo J, Echeimberg JO, Leone C. Research methodology topics: Cross-sectional studies. J Hum Growth Dev. 2018; 28(3):356-60. DOI: http://dx.doi.org/10.7322/jhgd.152198 [ Links ]
12.Fottrell E, Osrin D, Alcock G, Azad K, Bapat U, Beard J, et al. Cause-specific neonatal mortality: analysis of 3772 neonatal deaths in Nepal, Bangladesh, Malawi and India. Arch Dis Child Fetal Neonatal Ed. 2015;100:F439-447. DOI: http://dx.doi.org/10.1136/archdischild-2014-307636 [ Links ]
13.Ribeiro AM, Guimarães MJ, Lima MC, Sarinho SW, Coutinho SB. Risk factors for neonatal mortality among children with low birth weight. Rev Saúde Pública. 2009;43(2):246-55. http://dx.doi.org/10.1590/S0034-89102009005000004 [ Links ]
14.Abuqamar M, Coomans D, Louckx F. The impact of parental education on infant mortality in Gaza strip, Palestine. J Public Health Epidemiol. 2011;3(1):28-33. [ Links ]
15.Ribeiro FD, Ferrari RAP, Sant'Anna FL, Dalmas JC, Girotto E. Extremos de idade materna e mortalidade infantil: análise entre 2000 e 2009. Rev Paul Pediatr. 2014;32(4):381-8. DOI: http://dx.doi.org/10.1590/S0103-05822014000400015 [ Links ]
16.Althabe F, Sosa C, Beliza´N JM, Gibbons L, Jacquerio ZF, Bergel E. Cesarean Section Rates and Maternal and Neonatal Mortality in Low-, Medium-, and High-Income Countries : an ecological study. Birth. 2006;33(4):270-7. DOI: http://doi.org/10.1111/j.1523-536X.2006.00118.x [ Links ]
17.Lansky S, Friche AAL, Silva AAM, Campos D, Bittencourt SDA, Carvalho ML, et al. Pesquisa Nascer no Brasil: perfil da mortalidade neonatal e avaliação da assistência à gestante e ao recém-nascido. Cad Saúde Pública. 2014;30(Supl 1):S192-207. DOI: http://dx.doi.org/10.1590/0102-311X00133213 [ Links ]
18. Li F, Wu T, Lei X, Zhang H, Mao M, Zhang J. The apgar score and infant mortality. PloS One. 2013;8(7):e69072. DOI: http://doi.org/10.1371/journal.pone.0069072 [ Links ]
19.Andrade KFS, Bringel AL, Frois JC, Pereira MA, Cruz SS, Oliveira TT. Mortalidade infantil no município de Feira de Santana, Bahia. Sanare. 2015;14(Supl 1):153. [ Links ]
20.Ceccon RF, Bueno ALM, Hesler LZ, Kirsten KS, Portes VM , Viecili PRV. Mortalidade infantil e Saúde da Família nas unidades da Federação brasileira, 1998-2008. Cad Saúde Coletiva. 2014;22(2):177-83. DOI: http://dx.doi.org/10.1590/1414-462X201400020011 [ Links ]
21.Jobim R, Aerts D. Mortalidade infantil evitável e factores associados em Porto Alegre, Rio Grande do Sul, Brasil, 2000-2003. Cad Saúde Colet. 2008;24(1):179-87. DOI: http://dx.doi.org/10.1590/S0102-311X2008000100018 [ Links ]
22.Nobre LC, Victora CG, Barros FC, Lombardi C, Teixeira AMB, Fuchs SC. Avaliação da qualidade da informação sobre a causa básica de óbitos infantis no Rio Grande do Sul (Brasil). Rev Saúde Pública. 1989;23(3):207-13. DOI: http://dx.doi.org/10.1590/S0034-89101989000300005 [ Links ]
 Correspondence:
Correspondence:
profferfonseca@gmail.com
Manuscript received: December 2018
Manuscript accepted: September 2019
Version of record online: October 2019


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}