










Serviços Personalizados
Journal

artigo
 Inglês (pdf)
Inglês (pdf)
 Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
Indicadores
Compartilhar

 Permalink
PermalinkJournal of Human Growth and Development
versão impressa ISSN 0104-1282versão On-line ISSN 2175-3598
J. Hum. Growth Dev. vol.30 no.3 São Paulo set./dez. 2020
https://doi.org/10.7322/jhgd.v30.11069
ORIGINAL ARTICLE
Stage to Change Eating behavior and physical activity among adolescents with an excess body mass: impact on metabolic profile
Prontidão para a mudança do comportamento alimentar e atividade física entre adolescentes com excesso de peso: impacto no perfil metabólico
Marciele Alves BologneseI; Danilo Fernandes da SilvaI, II; Josiane Aparecida Alves BianchiniI, III; Rose Mari BenemmammI, IV; Nelson Nardo JuniorI
IUniversidade Estadual de Maringá, Núcleo de Estudos Multiprofissional da Obesidade (NEMO/UEM)/Núcleo de Pesquisa Clínica do Hospital Universitário de Maringá, Maringá, Paraná, Brasil
IISchool of Human Kinetics, Faculty of Health Sciences, University of Ottawa, Ottawa, Ontario, Canada
IIIDepartamento de Educação Física, Faculdade de Filosofia, Ciência e Letras de Mandaguari (FAFIMAN), Mandaguari, Paraná, Brasil
IVDepartamento de Nutrição, Universidade Cesumar (UNICESUMAR), Maringá, Paraná, Brasil
ABSTRACT
INTRODUCTION: Obesity in children and adolescents is usuallyrelated to metabolic alterations, and intervention programs are one of the strategies for the treatment of obesity and associated comorbidities. At the beginning of the intervention, the stages of readiness to change behavior indicate specific habits that the teenager plans to modify or not, and how long he or she intends to make the alterations
OBJECTIVE: To assess the metabolic profile and their association with the stages of readiness to change eating habits and exercise behaviors in adolescents with overweight
METHODS: Eighty-three adolescents with excess body weight underwent an assessment of anthropometric variables and metabolic profile (glucose, total cholesterol, LDL-c, HDL-c, non-HDL-c, VLDL, triglycerides, insulin). Besides, the stages of readiness to change behaviors for "size and amount of portions," "amount of fat in the diet," fruits and vegetable consumption," and "physical activity practice," anthropometric variables and metabolic profile were compared according to the stages of change
RESULTS: About "fruits and vegetable consumption," adolescents in the Maintenance group presented lower body weight than those from Action and Preparation groups. The Action group presented higher body weight than group "Contemplation" and it showed higher non-HDL-cholesterol than the groups "Pre-contemplation" and "Preparation." In "physical activity practice," the Maintenance group presented lower body weight, Body Mass Index, and body fat (in kg) than Action, Preparation, and Contemplation groups. The alterations in HDL-cholesterol reduced as the stages of change progressed in the "physical activity practice" domain
CONCLUSION: The stages of readiness to change behaviors impact anthropometric and metabolic variables in adolescents with excess body weight, and it is a recommended instrument to monitor intervention programs
Keywords: adolescent behavior, eating habits, pediatric obesity, metabolic syndrome.
RESUMO
INTRODUÇÃO: A obesidade em crianças e adolescentes geralmente está relacionada com alterações metabólicas, sendo os programas de intervenção uma das estratégias para o tratamento da obesidade e das comorbidades associadas. Ao iniciar a intervenção, os estágios de prontidão para mudança do comportamento indicam hábitos específicos que o adolescente planeja ou não mudar e em quanto tempo ele pretende realizar a mudança
OBJETIVO: Avaliar o perfil metabólico e sua associação com os estágios de prontidão para mudança do comportamento alimentar e atividade física em adolescentes com excesso de peso
MÉTODO: Foram avaliados 83 adolescentes com excesso de peso. Os adolescentes foram avaliados em relação à variáveis antropométricas e perfil metabólico (glicemia, colesterol total, colesterol LDL, HDL, não-HDL, VLDL, triglicerídeos, insulina). Além disso, foram avaliados os estágios de prontidão para mudança do comportamento para os domínios "tamanho e quantidade das porções", "quantidade de gordura na dieta", "consumo de frutas e vegetais" e "prática de atividade física". Foi feita comparação das variáveis antropométricas e perfil metabólico de acordo com os estágios de prontidão
RESULTADOS: Em relação ao domínio "Consumo de Frutas e Vegetais", os adolescentes do grupo Manutenção apresentaram peso menor que os do grupo Ação e Preparação. O grupo Ação apresentou peso maior que o Contemplação, e o grupo Contemplação apresentou colesterol não-HDL maior que os grupos Pré-contemplação e Preparação. No domínio "Prática de Atividade Física", o grupo Manutenção apresentou peso, IMC e gordura corporal (em kg) menores que os grupos Ação, Preparação e Contemplação. A prevalência de alteração do colesterol HDL foi progressivamente menor conforme progrediram os estágios de prontidão para mudança do comportamento para o domínio "prática de atividade física"
CONCLUSÃO: Os estágios de prontidão para mudança do comportamento têm impacto sobre variáveis antropométricas e perfil metabólico de adolescentes com excesso de peso, sendo um instrumento recomendado para o monitoramento de programas de intervenção
Palavras-chave: comportamento do adolescente, hábitos alimentares, obesidade pediátrica, síndrome metabólica.
Authors summary
Why was this study done?
Adolescents with overweight enrolled in a multidisciplinary treatment program commonly present alterations in their metabolic parameters. However, so far, it is not clear if these metabolic impairments are associated with the stage of readiness for eating and physical activity behavioral change. Hence, this information can help the multidisciplinary team understand how the readiness to change can be associated with a more or less favorable metabolic profile.
What did the researchers do and find?
When engaging in the multidisciplinary treatment program, adolescents underwent an assessment of their metabolic profile (i.e., glucose levels, lipid profile, and insulin) and the stage of readiness for eating behavior changes (amount of fat in the diet, fruits and vegetable intake, and size of portions) and physical activity practice. Our study identified that adolescents with lower readiness to adhering to physical activity practice also presented more significant HDL cholesterol impairment.
What do these findings mean?
The stages of behavioral change readiness are essential assessment tools before beginning an intervention program to modify eating habits and physical activity practice. Adolescents in lower stages of readiness for behavioral change need to receive more considerable attention from the multidisciplinary team because these adolescents also have a higher metabolic risk profile.
INTRODUCTION
The relationship between metabolic alterations and obesity during childhood and adolescence has been widely demonstrated1,2, as well as a pro-inflammatory profile that seems to be more common in children and adolescents with excess body weight3,4. Several studies have indicated that the prevalence of metabolic syndrome in adolescents with obesity varies from 6 to 52% and is higher than the overall pediatric population, ranging from 2.6 to 10%5-9.
However, in the clinical setting, overweight and obesity treatment programs manage adolescents with different degrees of excess body weight10,11. Studies10,12,13 that compare alterations of metabolic syndrome risk factors in adolescents with different degrees of excess body weight (e.g., overweight, obesity, and severe obesity) are scarce and present conflicting results regarding having or not greater metabolic impairments10,12,13.
Additionally, it is unknown if, when engaging in an intervention program with a multidisciplinary team, adolescents who present metabolic impairments are in different stages of readiness to change eating behaviors.
The stages of readiness to change behaviors when embarking on an intervention program provide relevant information. They can contribute with the intervention team indicating specific behaviors that the adolescent is planning not to modify, and when he/she intends to change14,15.
To the best of our knowledge, it is unknown if stages of readiness to change behaviors are related to the metabolic profile (e.g., metabolic syndrome risk factors) in adolescents with excess body weight who engage in a multidisciplinary program for obesity treatment (MPOT).
Thus, this study's objective is to assess the metabolic profile and its association with the readiness stages to change eating habits and physical activity behaviors in adolescents with excess body weight.
METHODS
Experimental design and study participants
It is a cross-sectional study with comparative and associative analysis. The study was promoted in the local media to recruit adolescents aged 16 to 18 years interested in participating in the MPOT. The MPOT lasted 16 weeks, carried out twice a year, and had a multidisciplinary team composed of physical exercise professionals, nutritionists, a psychologist, and a pediatrician.
The multidisciplinary team's main goal was to contribute to positive changes in body weight and composition, in the medium-term, by encouraging physical activity practices and recommending healthy eating habits based on cognitive behavioral therapy.
Adolescents took part in the MPOT three times per week, on Mondays, Wednesdays, and Fridays, from 4 to 6 pm. From 4 to 5 pm discussed physical exercise behaviors. At this same time, adolescents participated in the nutritional group intervention on Wednesdays and the psychological group intervention on Fridays. The second hour of intervention (from 5 to 6 pm) of all the three days was designated for the exercise practices. The intervention protocol can be found in Da Silva et al.16.
Eighty-three adolescents selected on the following inclusion criteria:
- Having body mass index (BMI) in the overweight and obesity category according to the cut-off points described by Cole and Lobstein17;
- Being residents in Maringá city or surrounding areas;
- Availability to participate in the intervention program fully.
The adolescents engaged in other types of overweight (e.g., pharmacological or surgical), consumed alcohol during long-term, or used glucocorticoids or other appetite-related drugs were excluded.
The adolescent's parents attended a presentation on the study scope during the recruiting process. Those who agreed with the protocol signed the study consent form, previously approved by the local ethics board, based on document #466/2012 from the National Council of Health.
Evaluations
The week before the intervention, adolescents went through a battery of evaluations, including body weight, height, and BMI. Bodyweight calculated by a Welmy scale, measuring up to 300 kg and a precision of 0.05 kg, with adolescents wearing light clothes. A stadiometer with a scale of up to 2 meters and a precision of 0.1 cm measured the height. BMI was calculated by dividing body weight by squared height.
Body fat (absolute and relative to body mass) was assessed by an octapolar multifrequency bioelectrical impedance (InBody, model 520). Participants wore light clothes with no metallic objects, following the protocol: fasting for a minimum of 2 h including water; urinate about 30 min before the assessment; avoid consuming caffeinated beverages in the last 48 hours; avoid vigorous exercises in the last 24 hours; do not use diuretics in the last seven days, and not being in the menstrual period for girls.
Metabolic profile was assessed by a blood test to determine glucose levels, total cholesterol, LDL cholesterol, HDL cholesterol, non-HDL cholesterol, VLDL cholesterol, triglycerides, and insulin following the protocol of a specialized laboratory after 12 h fasting during the morning (Carlos Chagas, Parana, Brazil). Total cholesterol, HDL cholesterol, and triglycerides were classified as altered according to the cut-off points recommended by Back et al.18: total cholesterol ≥170 mg/dL, HDL cholesterol <45 mg/dL, LDL cholesterol ≥130 mg/dL, and triglycerides ≥130 mg/dL. Blood glucose of ≥100 mg/dL was considered altered19.
The questionnaire Stage of Change (SOC) was applied to determine the stages of readiness for eating and exercise behavior change, proposed by Sutton et al.15, validated for the Brazilian context by Cattai et al.20, who rigorously followed an international methodology for the translation and cultural adaptation with a sample of adolescents living with obesity. These authors concluded that the instrument is appropriate for the target population since it presented adequate scores of reliability and internal validity.
The main advantages of the SOC instrument are that it can be self-administered and contemplate the stages of readiness for behavior change, based on a list of items related to weight management15,20.
The instrument composed by 38 sentences distributed in four domains denominated: "size and amount of portions" (nine sentences); "amount of fat in diet" (11 sentences); "consumption of fruits and vegetables" (nine items); and "physical activity practice" (nine sentences). The answers for each sentence vary as a Likert scale from 1 to 5, with 1 being pre-contemplation, 2. contemplation, 3 preparation; 4 actions; and 5. maintenance.
A mean score was calculated to classify the stages for each of the four domains. For analysis purpose, data was classified as: 1 to 1.4 - pre-contemplation; 1.5 to 2.4 - contemplation; 2.5 to 3.4 - preparation; 3.5 to 4.4 - action; 4.5 to 5 - maintenance16,20.
Statistical Analysis
Descriptive and inferential statistics analyzed data, and the Shapiro-Wilk test assessed normality. Data presented as median (interquartile range). Comparisons of different readiness stages of behavior change (4 domains) for the metabolic variables (continuous data) were performed using the non-parametric tests of Kruskal-Wallis and Mann-Whitney when needed (as a post hoc). The Chi-square test showed the associations between categorical variables. Significance was set at P<0.05.
RESULTS
Of the 83 adolescents engaged in the MPOT, three (3.6%) presented incomplete data and were excluded. From the 80 adolescents included in the analysis, four (5%) adolescents were classified as pre-contemplation 16 (20%) contemplation, 35 (43.8%) preparation, 21 (26.3%) action and four (5%) maintenance for the "size and amount of portions" domain. In the "amount of fat in diet" domain, three (3.8%) were classified as pre-contemplation, 12 (15%) contemplation, 27 (33.8%) preparation, 30 (37.5%) action and eight (10%) maintenance.
For the "consumption of fruits and vegetables" domain, there were two (2.5%) pre-contemplation, 13 (16.3%) contemplation, 32 (40%) preparation, 24 (30%) action and nine (11.3%) maintenance. In the "physical activity practice" domain, one (1.3%) adolescent was classified as pre-contemplation, 22 (27.5%) contemplation, 38 (47.5%) preparation, 15 (18.8%) action and four (5%) maintenance.
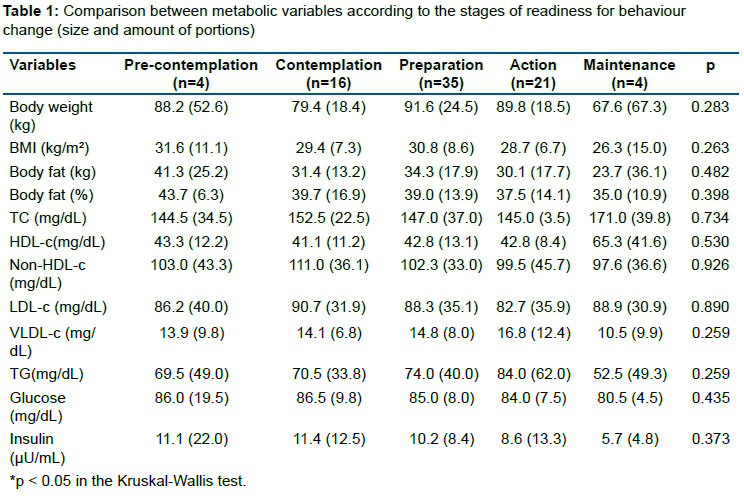
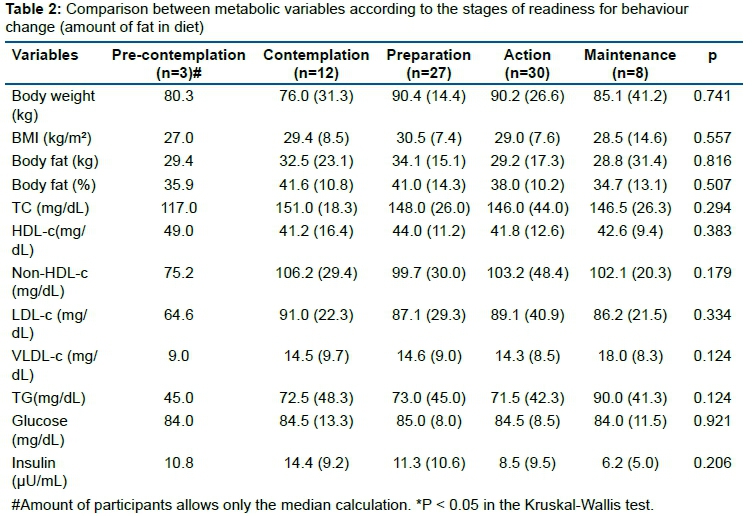
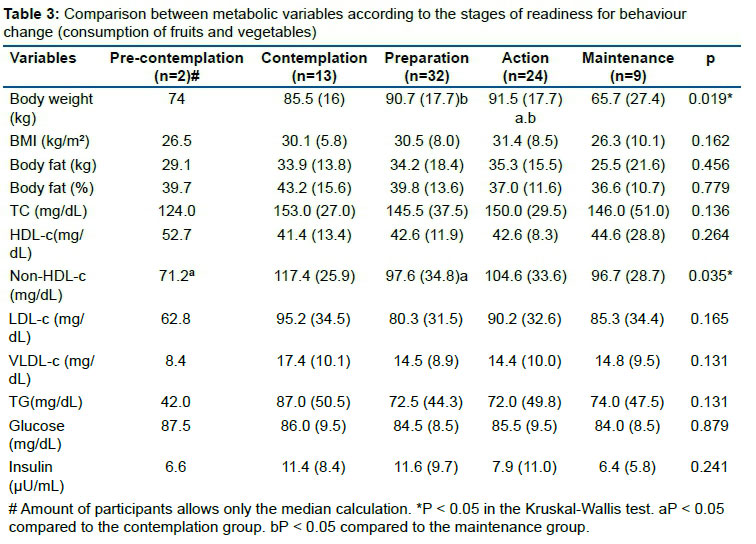
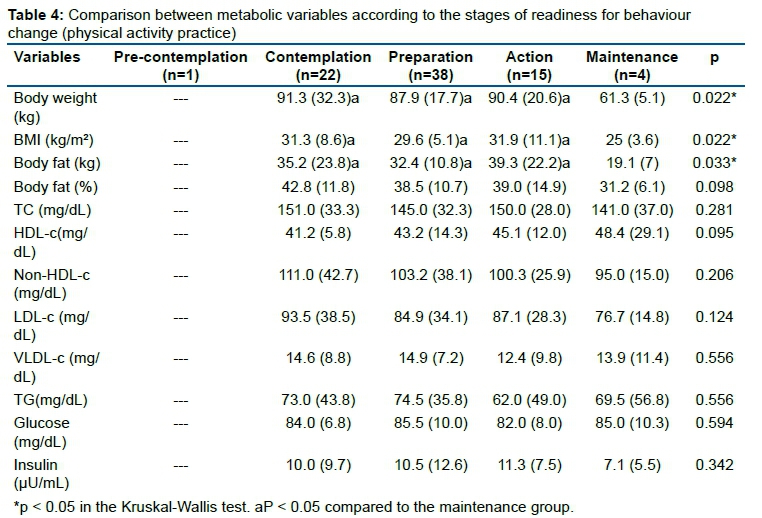
Tables 1,2,3 and 4, describe a comparison among the five readiness stages of behavior change of the metabolic variables, according to the each domain of SOC questionnaire.
Differences were statistically significant for the "consumption of fruits and vegetables" and "physical activity practice" domains. Concerning the "consumption of fruits and vegetables" domain, the adolescents classified as "maintenance" presented lower body weight than those classified in "action" and "preparation" stages. Besides, the "action" group showed higher body weight than the "contemplation" group; this last one showed higher non-HDL cholesterol than adolescents in the "pre-contemplation" and "preparation" stages.
In the "physical activity practice" domain, those individuals included in the "maintenance" stage had lower body weight, BMI, and body fat (in kg) than those categorized in the stages "action," "preparation," and "contemplation."
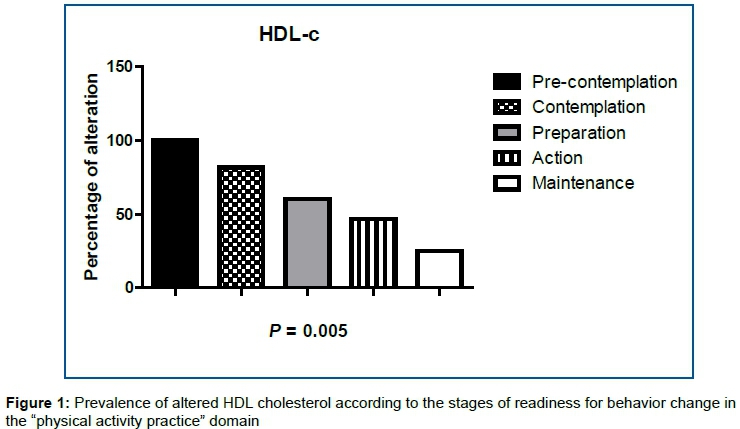
There was no association between the stages of readiness for behavior change and metabolic impairment, except for HDL cholesterol alteration which was lower as stages progressed for the "physical activity practice" domain (pre-contemplation: 100%; contemplation: 81.8%; preparation: 60.5%; action: 46.7%; maintenance: 25%) (Figure 1).
DISCUSSION
The "size and amount of portions" and "amount of fat in diet" domains did not present differences among the stages of readiness for behavior change for any of the analyzed variables (i.e., anthropometric or metabolic profile), which means that the stage the adolescent was classified did not affect these outcomes. In contrast, with regards to the "consumption of fruits and vegetables," adolescents from the "maintenance" stage showed lower body weight than those in the "action" and "preparation" groups. Moreover, those adolescents classified in the "action" range had higher body weight than those of the "contemplation" group. and this last one had higher non-HDL cholesterol than the "pre-contemplation" and "preparation" groups.
In the "physical activity practice" domain, the "maintenance" group showed lower body weight, BMI, and body fat (in kg) than the "action," "preparation," and "contemplation" groups. In this way, adolescents who embarked in the MPOT in more advanced stages for "consumption of fruits and vegetables" and "physical activity practice" presented more favorable anthropometric and metabolic profiles, mainly for the "action" and "maintenance" stages. The prevalence of altered HDL cholesterol was lower as stages progressed for the "physical activity practice" domain.
The fact that more adolescents in almost all the SOC questionnaire domains classified in the "preparation" stage is a positive outcome for the multidisciplinary team. In this stage, individuals tend to be more open to the treatment requirements, and consequently, they have more considerable changes in presenting satisfactory results from the intervention21,22. According to Toral et al.23, many individuals have a wrong interpretation of eating behaviors and believe they already have appropriate eating habits without knowing that they can be harmful. It is one of the biggest obstacles to achieving healthful eating changes23. It is crucial to recognize that changes are required, not only for eating habits but also for physical activity practice24.
The stages of readiness for behavior change are components of the Trans theoretical model, initially proposed as a component of intervention programs to cease tobacco use25. However, the stages were adapted to assess patients seeking for eating changes23 and increase physical activity levels24.
Da Silva et al.16 studied the impact of readiness's stages on behavior change of physical activity and its effects on physical fitness and body composition. They identified that adolescents who initiated the intervention program in more advanced stages (e.g., maintenance) achieved better outcomes on anthropometric variables, diastolic blood pressure, and cardiorespiratory fitness. They also highlighted that an intervention program based on cognitive behavioral therapy could promote benefits even for adolescents in the early stages of readiness for behavior change (e.g., pre-contemplation or contemplation)16.
According to the Trans theoretical model25, individuals classified in advanced stages tend to increase positive attitudes towards nutrition and physical activity, which will ultimately allow them to have a better health status. This current study evidenced a better HDL cholesterol profile. These positive outcomes reflect the relationship between the stages of readiness to modify behaviors and the factors that facilitate behavioral transformations, mainly with greater stimulus control26,27. This factor can exist before the intervention, even before the baseline assessment, which would explain the best results observed in advanced stages.
In contrast with that, adolescents in early stages can have this relationship between their readiness for behavior change (e.g., pre-contemplation and contemplation) and the change processes, however, in a lower magnitude. According to Prochaska28, Prochaska, and Di Clemente27, long-term improvements can occur due to increased knowledge and their capacity to self-evaluate, followed throughout the treatment by the psychology team16.
From a practical point of view, the association between the progress in the readiness stages of behavior change for the "physical activity practice" domain and the decrease in the frequency of adolescents with altered HDL cholesterol was expected, given the potential benefits of exercise to control this cholesterol fraction29. The study performed by Chen et al.30 did not identify changes in HDL cholesterol in children living with excess body weight, and a hypothesis they raised to explain this finding is that the physical activity levels of these children were already relatively high.
Our study presents interesting findings with potential practical implications; however, there are still limitations. A minimal sample size calculation was not performed since our study focused on adolescents engaging in a multidisciplinary intervention program to treat pediatric obesity. In this case, it is expected a low sample size in the last stages (i.e., pre-contemplation and maintenance) even though the determination of the stages of readiness for behavior change and their impact on metabolic variables are essential to understand the fundamental characteristics of adolescents to seek this type of health service.
Given that, our study brings the novelty related to the association between stages of readiness for eating and physical activity behavior change with the metabolic profile. Before beginning the intervention, an association between how opened for behavior changes the adolescent is, and their anthropometric and metabolic profile was observed. These results can provide useful information for a multidisciplinary team during the intervention program.
CONCLUSION
The "consumption of fruits and vegetables" and "physical activity practice" domains found an association between readiness stages for behavior changes on anthropometric variables and metabolic profile.
The alteration in the HDL cholesterol was associated with the readiness stages for behavior change for the "physical activity practice" domain.
REFERENCES
1.Ho M, Garnett SP, Baur, LA. Childhood obesity and insulin resistance: how should it be managed? Curr Treat Options Cardiovasc Med.2014 Dec; 16(12): 351. DOI: https://doi.org/10.1007/s11936-014-0351-0 [ Links ]
2.Ho HCH, Maddaloni E, and Buzzetti, R. Risk factors and predictive biomarkers of early cardiovascular disease in obese youth. Diabetes Metab Res Rev. 2019; 35:e3134. Doi: 10.1002/dmrr.3134. [ Links ]
3.Mayerhofer E, Ratzinger F, Kienreich NE, et al. A multidisciplinary intervention in childhood obesity acutely improves insulin resistance and inflammatory markers independent from body composition. Front Pediatr. 2020 feb21;8:52. Doi: 10.3389/fped.2020.00052. [ Links ]
4.Ruminska M, Witkowska-Sedek E, Artemniak-Wojtowicz D, et al. Changes in leukocyte profile and C-reactive protein concentration in overweight and obese adolescents after reduction of body weight. Cent Eur J Immunol. 2019; 44(3):307-3015. Doi: 10.5114/ceji.2019.89608. [ Links ]
5.Moraes ACF, Fulaz CS, Oliveira ERN, Reichert FF. Prevalência de síndrome metabólica em adolescentes: uma revisão sistemática. Cad Saúde Pública. 2009; 25(6): 1195-202. [ Links ]
6.Kuschnir MCC, Bloch KV, Szklo M, et al. ERICA: prevalence of metabolic symdrome in Brazilian adolescents. Rev SaúdePública. 2016; 50(suppl 1):11s. [ Links ]
7.Weiss R, Dziura J, Burgest TS, Tamborlane WV, Taksali SE, Yeckel CW.et al, Obesity and the metabolic Syndrome in Children and Adolescents. N Engl J Med. 2004 Jun; 350:2362. DOI: https://doi.org/10.1056/NEJMoa031049 [ Links ]
8.Elitok GK, Duru NS, Elevil M, et al. Prevalence of Metabolic Syndrome in Middle School Chidren and Evaluation of Components Of Metabolic Syndrome. SisliEtfalHastan Tip Bul. 2019 Nov 21;53(4):403-408. Doi: 10.14744/SEMB.2018.50479. [ Links ]
9.Cook S, Weitzman M, Auinger P, Nguyen M, Dietz W H. Prevalence of metabolic syndrome phenotype in adolescents: findings from the third national health and nutrition examination survey, 1988-1994. Arch Pediatr Adolesc Med. 2003 Aug; 157(8): 821-7. [ Links ]
10.Rizzo AP, Goldberg T, Silva CC, Kurokawa CS, Nunes H, Corrente J. Metabolic Syndrome Risk Factors in Overweight, Obese, and Extremely Obese Brasilian Adolescents. Nutr J. 2013 Jan 30; 12: 19. DOI: https://doi.org/10.1186/1475-2891-12-9 [ Links ]
11.Hintze LJ, Cattai, GBP, Da Silva DF, Nardo Junior N. Estágio de prontidão para mudança de adolescentes interessados e ingressar no programa multiprofissional de tratamento da obesidade. Rev Paul Pediatr. 2012; 30(2): 237-43. [ Links ]
12.Rank M, Siegrist M, Wilks DC, Langhof H, Wolfarth B, Haller B, et al. The Cardio-Metabolic Risk of Moderate and Severe Obesity in Children and Adolescents. J Pediatr. 2013 Jul; 163(1): 137-42. DOI: https://doi.org/10.1016/j.jpeds.2013.01.020 [ Links ]
13.Ricco RC, Rubens GR, Almeida CAN, Ramos APP. Estudo comparativo de fatores de risco em crianças e adolescentes com diagnóstico antropométrico de sobrepeso ou obesidade. Rev Paul Pediatr. 2010; 28(4): 320-5. [ Links ]
14.SIGN. Scottish Intercollegiate Guidelines Network. Management of obesity. a national clinical guideline. Edinburgh: SIGN; 2010. [ Links ]
15.Anderson YC, Dolan GMS, Wynter LE, et al. Caregiver's Readiness for Change as a Predictor of Outcome and Attendance in an Intervention Programme for Children and Adolescents With Obesity: A Secondary Data Analysis. BMJ Open. 2019; 9(3):e023195. Doi: 10.1136/bmjopen-2018-023195. [ Links ]
16.Da Silva DF, Bianchini JAA, Lopera CA, Capelato DA, Hintze LJ, Nardo CCS, et al. Impact of readiness to change behavior on the effects of a multidisciplinary intervention in obese Brazilian children and adolescents. Appetite. 2015 Apr; 87: 229-35. DOI: https://doi.org/10.1016/j.appet.2014.12.221 [ Links ]
17.Cole TJ, Lobstein, T. Extended international (IOTF) body mass index cut-offs for thinness, overweight and obesity. Pediatr Obes. 2012 Aug; 7(4): 284-94. DOI: https://doi.org/10.1111/j.2047-6310.2012.00064.x [ Links ]
18.Back GI, Caramelli B, Pellanda L. I diretriz brasileira para a prevenção da aterosclerose na infância e na adolescência. Arq Bras Cardiol. 2005; 85(Suppl 6): 4-36. [ Links ]
19.International Diabetes Federation (IDF). IDF consensus definition of the metabolic syndrome in children and adolescents. Brussels: IDF; 2007. p. 2-19. [ Links ]
20.Cattai GBP, Hintze LJ, Nardo Junior N. Validação interna do questionário de estágio de prontidão para mudança do comportamento alimentar e de atividade física. Rev Paul Pediatr. 2010; 28(2): 194-9. DOI: http://www.scielo.br/pdf/rpp/v28n2/v28n2a11.pdf [ Links ]
21.Matias T, Andrade A, Maciel G, et al. O estágio de manutenção para o exercício está associada à uma melhor percepção de diferentes indicadores de saúde na adolescência. Rev Bras Ativ Fís & Saúde. 2017; 22(5):1-7. Doi: https://doi.org/10.12820/rbafs.v.22n5p479-485. [ Links ]
22.Moore JB, Singletary CR, Skelton JA, et al. The Design of A Clinical Trial to Increase Self-Monitoring of Physical Activity and Eating Behaviors Among Adolescents: Protocol for the ImPACT Feasibility Study. JMIR Publication. 2020. Doi: 10.2196/18098. [ Links ]
23.Toral N, Slater B, Cintra I de P, Fisberg M. Comportamento alimentar de adolescentes em relação ao consumo de frutas e verduras. 2006. Rev Nutr. 2006 maio-jun; 19(3): 331-40. DOI: http://www.scielo.br/pdf/rn/v19n3/30138.pdf [ Links ]
24.Maddison R, Prapavessis H. Exercise behavior among New Zealand adolescents. A test of the transtheoretical model. Pediatric Exercise Science. 2006;18 (3): 351-63; 2006. DOI: https://doi.org/10.1123/pes.18.3.351 [ Links ]
25.Prochaska JO, DiClemente CC.Stage and process of self-change in smoking. Toward an integrative model of change. J Consult Clin Psychol. 1983 Jun; 51(3): 390-5. [ Links ]
26.Chae SM, Kwon I, Kim CJ, Jang J. Analysis of weight control in Korean adolescents using the transtheoretical model. West J Nurs Res. 2010 Jun; 32(4): 511-29. DOI: https://doi.org/10.1177/0193945909355996 [ Links ]
27.DiClemente CC, Prochaska JO, Fairhurst SK, Velicer WF, Velasquez MM, Rossi JS. The process of smoking cessation. An analysis of precontemplation, contemplation, and preparation stages of change. J Consult Clin Psychol. 1991 Apr; 59(2): 295-304. [ Links ]
28.Prochaska JO. Decision making in the transtheoretical model of behavior change. Med Decis Making. 2008 Nov-Dec; 28(6): 845-9. DOI: https://doi.org/10.1177/0272989X08327068 [ Links ]
29.Kelly AS, Wetzsteon RJ, Kaiser DR, et al. Inflammation, insulin, and endothelial function in overweight children and adolescents: the role of exercise. J Pediatr 2004; 145: 731-6. [ Links ]
30.Chen AK, Roberts CK, Barnard RJ. Effect of a short-term diet and exercise intervention on metabolic syndrome in overweight children. Metabolism. 2006 Jul; 55(7): 871-8. [ Links ]
 Correspondence:
Correspondence:
Josiane Aparecida Alves Bianchini
josianeaabianchini@gmail.com
Received: August 2020
Revised: September 2020
Accepted: September 2020


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}