










Serviços Personalizados
Journal

artigo
 Inglês (pdf)
Inglês (pdf)
 Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
Indicadores
Compartilhar

 Permalink
PermalinkJournal of Human Growth and Development
versão impressa ISSN 0104-1282versão On-line ISSN 2175-3598
J. Hum. Growth Dev. vol.30 no.3 São Paulo set./dez. 2020
https://doi.org/10.7322/jhgd.v30.11076
ORIGINAL ARTICLE
Preconception care: developing and implementing regional and national programs
Hani AtrashI; Brian JackII
IMD, MPH, Adjunct Professor, Department of Epidemiology Emory University, Rollins School of Public Health
IIMD, Professor and Vice Chair, Department of Family Medicine Boston University School of Medicine / Boston Medical Center
ABSTRACT
INTRODUCTION: During the past few decades, health workers have come to agree that there is a very important place for preconception care (PCC) in improving maternal and infant pregnancy outcomes. The United States Centers for Disease Control and Prevention (CDC) and the World Health Organization issued recommendations encouraging countries to develop and implement preconception care programs. The reports include an in-depth discussion of the rationale and scientific evidence behind PCC as well as definitions, goals, components and recommended interventions to be included in PCC. These reports also offer very broad guidelines but do not offer details on how to develop and implement preconception care programs
OBJECTIVE: The CDC and WHO reports identify the need for multi-sectoral engagement in developing and implementing preconception care programs and propose some activities and strategies to be considered in developing PCC programs. However, the recommendations fall short of specifying real steps that countries and regions should take in implementing PCC programs. In this publication we propose action steps for developing and implementing regional or national preconception care programs
METHODS: We reviewed the published and unpublished literature (using PubMed and the Internet) to identify reports that describe processes for developing and implementing PCC programs. We used information from the literature along with experiences we gained through our work and interaction with States and developing countries to prepare a detailed description of the steps involved in developing and implementing a PCC program
RESULTS: We found very little in terms of "tools" for program managers and providers to use when developing and implementing PCC programs. We prepared a guide, including a summary of steps and a proposed timeline, for program directors to use for developing and implementing PCC programs
CONCLUSION: Developing and implementing a sustainable PCC program should address issues related to educating the public, providers and policy makers about the benefits of PCC. It also includes establishing an infrastructure within the departments of health and ensuring resources to build, guide, monitor and evaluate the PCC program. Finally, implementation of a successful program depends heavily on the proper training of public health and clinical care providers in the delivery of the services included in the program
Keywords: preconception care, preconception health, women's health, maternal health, infant health, program development, program implementation.
RESUMO
INTRODUÇÃO: Nas últimas décadas, os profissionais de saúde chegaram a um acordo sobre a importância dos cuidados preconcepção na melhoria dos resultados da gravidez materna e infantil. Os Centros dos Estados Unidos para Controle e Prevenção de Doenças (CDC) e a Organização Mundial da Saúde emitiram recomendações incentivando os países a desenvolver e implementar programas de assistência preconcepção. Os relatórios incluem uma discussão aprofundada da lógica e das evidências científicas por trás do PCC, bem como definições, objetivos, componentes e intervenções recomendadas a serem incluídas no PCC. Esses relatórios também oferecem diretrizes muito amplas, mas não oferecem detalhes sobre como desenvolver e implementar programas de assistência preconcepção
OBJETIVO: Os relatórios do CDC e da OMS identificam a necessidade de envolvimento multissetorial no desenvolvimento e implementação de programas de assistência pré-conceitual e propõem algumas atividades e estratégias a serem consideradas no desenvolvimento de programas do PCC. No entanto, as recomendações não especificam as medidas reais que os países e regiões devem adotar na implementação de programas de assistência preconcepção. Neste artigo, propomos etapas de ação para o desenvolvimento e implementação de programas regionais ou nacionais de assistência pré-conceitual
MÉTODO: Foi revisada a literatura publicada usando o PubMed para identificar relatórios que descrevem processos para o desenvolvimento e implementação de programas de assistência preconcepção. As informações da literatura foram utilizadas, juntamente com as experiências adquiridas por meio de nosso trabalho e interação com os Estados e os países em desenvolvimento, para preparar uma descrição detalhada das etapas envolvidas no desenvolvimento e na implementação de um programa de assistência preconcepção
RESULTADOS: Pouco foi encontrado em termos de "ferramentas" para os gerentes e provedores de programas usarem ao desenvolver e implementar programas de assistência preconcepção. Este artigo foi preparado como um guia, incluindo um resumo das etapas e um cronograma proposto, para os diretores de programas usarem no desenvolvimento e na implementação de programas de assistência preconcepção
CONCLUSÃO: O desenvolvimento e implementação de um programa sustentável do PCC deve abordar questões relacionadas à educação do público, fornecedores e formuladores de políticas sobre os benefícios do PCC. Também inclui o estabelecimento de uma infraestrutura nos departamentos de saúde e a garantia de recursos para construir, orientar, monitorar e avaliar o programa PCC. Finalmente, a implementação de um programa bem-sucedido depende muito do treinamento adequado dos prestadores de serviços de saúde pública e atendimento clínico na prestação dos serviços incluídos no programa
Palavras-chave: assistência preconcepção, saúde preconcepção, saúde da mulher, saúde materna, saúde infantil, desenvolvimento de programas, implementação de programas.
Authors summary
Why was this study done?
• States and countries have been working on developing and implementing preconception care programs for over 15 years. • Many training tools have been prepared and shared with program directors to assist them in this process. • There are tens maybe hundreds of publications related to preconception care, however, there is no guide to assist program managers in developing and implementing a preconception care program. • It is important to prepare a simple publication that describes step by step the process of developing and implementing a preconception care program. • Program managers can use this publication as a reference, a training tool, and a guide.
What did the researchers do and find?
• We reviewed published and un-published literature related to developing and implementing preconception care programs. • We searched PubMed for published articles. • We searched the internet for unpublished reports prepared by international organizations such as the World Health Organization and reports from governmental agencies. • We identified several reports from states, countries, and other organizations. However, none of the reports was comprehensive or offered a step by step guide for developing and implementing a program.
What do these findings mean?
• Developing and implementing a sustainable PCC program entails a wide range of activities and includes addressing issues related to educating the public, providers and policy makers about the benefits of PCC. • The process also includes establishing an infrastructure within the departments of health and ensuring resources to build, guide, monitor and evaluate the PCC program. • A successful program depends heavily on the proper training of public health and clinical care providers in the delivery of the services included in the program.
INTRODUCTION
During the past few decades, health workers have come to agree that there is a very important place for preconception care in this continuum of care. In 2004, the United States Centers for Disease Control and Prevention (CDC) convened experts who developed "Recommendations to Improve Preconception Health and Health Care"1. In February 2012, the World Health Organization (WHO) convened a meeting of researchers and partner organizations "to achieve a global consensus on the place of preconception care (PCC) as part of an overall strategy to prevent maternal and childhood mortality and morbidity"2. The group concluded that further improvements in maternal and infant pregnancy outcomes would be achieved through a "continuum of care" starting "before pregnancy and continuing through pregnancy, infancy, childhood, adolescence and adulthood"2. Both the CDC and WHO reports include an in-depth discussion of the rationale and scientific evidence behind PCC as well as definitions, goals, components and recommended interventions to be included in PCC. However, these reports stop short of providing guidance on how to develop and implement PCC programs within departments of health. The CDC expert panels identified five areas that need special focus when developing and implementing a preconception care program: clinical practice, consumer education, policy and finance, public health practice, and research. Workgroups were convened to discuss strategies for implementation within each of these focus areas. The workgroups concluded that strategies fall under 10 priority areas:
1. Developing and disseminating clinical guidelines and tools
2. Educating consumers
3. Integrating preconception care activities into clinical and public health programs
4. Ensuring monitoring and surveillance of preconception care knowledge, attitudes, and practices
5. Developing and promoting a research agenda
6. Promoting public policy and financing in support of preconception care
7. Educating and training clinical and public health care providers
8. Identifying, documenting, and promoting best practices
9. Implementing projects to demonstrate effectiveness, and
10. Supporting state and local initiatives3.
The WHO expert panel recommended that a wide range of sectors and stakeholders needs to be engaged to ensure universal access to PCC and guides non-health sectors, foundations and civil society organizations to collaborate with, and support, public health policy-makers to maximize gains for maternal and child health through PCC. The panel proposed "strategies for country action" composed of four steps as follows4:
1. Create national platforms and partnerships to ensure political commitment
2. Preconception care implementation strategy:
a. Assess the strengths and weaknesses of the preconception care system in place
b. Leverage on existing public health programs (Reproductive/maternal health, Early child development, Adolescent health, Nutrition, Immunization, HIV, Environmental health, Violence prevention, and Mental health)
3. Delivering the intervention package:
a. Adapt the intervention package
b. Explore innovative ways and channels in delivering preconception care interventions (Schools, Workplaces, Civil society groups, electronic health technologies, etc)
c. Identify target population
d. Mobilize financial resources
e. Strengthen human resources, and
f. Establish a plan for monitoring and evaluation
4. Maximizing the gains for maternal and child health
The CDC and WHO strategies, however, fell short of specifying real steps that countries and or regions should take in implementing preconception care programs. Some countries took the initiative and developed their own plans5-9, while some WHO regional offices took it upon themselves to develop guidance for countries in their regions. For example, In March 2015, WHO's Eastern Mediterranean Regional Office (EMRO), convened a meeting of experts on "Promoting Preconception Care in the Eastern Mediterranean Region", followed by a another meeting of an "Informal working group on promoting Preconception Care in the Eastern Mediterranean Region" in September, 201510,11. The working group objectives were to discuss and recommend evidence-based interventions to be included in a PCC package and discuss and agree on priority actions for the development of flexible PCC program guidance to be adopted/adapted by Member States for integrating/strengthening PCC in national health systems. Participants agreed that there was a need to select PCC core interventions based on the following criteria: scientific evidence, cost- effectiveness, feasibility, affordability, sustainability, relevance, acceptability and having an impact on reducing maternal and child mortality and morbidity. By the end of the meeting, members of the workgroup recommended a set of interventions and identified 10 main steps of building a PCC program at the country level: developing goals and objectives, involving policy makers and leadership, establishing a taskforce and engaging multilevel stakeholders and partners, implementing a communication and social mobilization strategy, building the capacity of PCC workforce, defining and implementing clinical PCC services, defining entry points for PCC services, monitoring PCC processes and outcomes, implementing the PCC program, and establishing a PCC network11.
DEVELOPING A PRECONCEPTION CARE PROGRAM
Due to our experience with states and countries, and based on proposals and recommendations made by various countries and workgroups, we propose action steps for developing and implementing a regional or national PCC program, as follows:
Step 1. Identify a Champion: the first, and perhaps most important step in establishing a preconception care program is to identify a senior level individual to champion the program. The champion needs to be an influential individual who can bring together cross-sector leaders and keep their active engagement over time. The champion should also have access to leadership within the department of health and other collaborating agencies to educate them about the importance of the program, update them on progress, and ensure their engagement and support as well as the availability of financial and human resources to maintain a successful program12.
Step 2. Establish a Preconception Care Unit within the department of health: preconception care activities are spread across many governmental and non-governmental entities. However, most of these activities reside within the departments of health and as such, the department of health should establish a preconception care unit (PCCU) to include staff with a very specific set of skills to develop and maintain the program through a collective impact approach12-14. Working closely with the champion, the PCCU will coordinate activities within the department of health and ensure resources to build, guide, monitor and evaluate the PCC program. The PCCU will also serve as a backbone organization for the program to ensure entities within and outside the department of health are informed, engaged and work well together. According to Turner, backbone organizations serve six essential functions: Provide overall strategic direction, facilitate dialogue between partners, manage data collection and analysis, handle communications, coordinate community outreach, and mobilize funding14.
Step 3. Prepare briefing material to share with leadership, partners, providers and the public: in preparation for informing and educating department of health leaders and other partners about PCC, the first task of the PCCU is to "define" the program and justify its need. The team should prepare a brief document and a set of slides describing PCC and the proposed program to hand out to program and policy leaders and to partners, and to use for raising awareness and educating providers and the public. These two documents should include the following:
a. A description of the current situation including the health, exposures, and behaviors of women of reproductive age, maternal and infant health statistics and trends, current services to non-pregnant and pregnant women aimed at improving pregnancy outcomes, and programs that provide or that potentially could provide preconception care services.
b. A description of preconception health and health care: its definition, scientific evidence of its effectiveness, and examples of programs from other countries. The program could adopt or adapt definitions produced by other groups such as the CDC or the WHO. The WHO defined PCC as "the provision of biomedical, behavioral and social health interventions to women and couples before conception occurs. It aims at improving their health status, and, reducing behaviors and individual and environmental factors that contribute to poor maternal and child health outcomes".
c. A description of the proposed program including its partners and activities, vision, goals and objectives.
i. Partners: A successful PCC program would be implemented in collaboration with multiple units within the department of health (training, communication, education, statistics, epidemiology, etc.) as well as partners outside the department including governmental (departments of education, labor, financing, transportation, etc.) and non-governmental organizations (private hospitals, physicians, nurses, laboratories, health educators and counselors, non-profit organizations, etc.)
ii. Vision: A program's vision is the big picture of what the program hopes to achieve and how things ought to be. A vision is a dream; it's what an organization believes are the ideal conditions for the community; that is, how things would look if the issue important to program were completely, perfectly addressed. By developing a vision statement the program clarifies its beliefs and governing principles to members of the program and to the greater community. For example, the CDC expert panel identified their vision for PCC as follows: "women and men of childbearing age have high reproductive awareness; women and men have a reproductive life plan; pregnancies are intended and planned; women and men of childbearing age have health-care coverage; women of childbearing age are screened before pregnancy for risks related to the outcomes of pregnancy; and, women with a previous adverse pregnancy outcome have access to inter-conception care aimed at reducing their risks"2.
iii. Goals: goals are broad statements about the long-term expectations of what should happen as a result of implementing the program. They are general guidelines that explain what the program wants to achieve in the community. They are usually long-term and represent global visions such as "protect public health and safety." In their recommendations for PCC, CDC's expert panel set four goals for PCC: "Improve the knowledge and attitudes and behaviors of men and women related to preconception health, assure that all women of childbearing age in the United States receive preconception care services, reduce risks indicated by a previous adverse pregnancy outcome through interventions during the inter-conception period, and reduce the disparities in adverse pregnancy outcomes2.
iv. Objectives describe the results to be achieved, and the manner in which they will be achieved. The program usually needs multiple objectives. And objectives need to be "SMART": Specific, Measurable, Achievable, Realistic, and Time-phased. Objectives should be very specific about the "who" and "what" of program activities (specific) - for example 50% of women of reproductive age will have an annual encounter with their provider which will include preconception care services. The focus is on "how much" change is expected (measurable), for example, the number of providers and consumers who know about PCC and its benefits will increase by 40%. Objectives should be achievable considering available program resources and should be realistic and accurately address the scope of the problem and programmatic steps that can be implemented within a specific time frame. Finally, objectives should provide a time frame indicating when the objective will be measured or a time by which the objective will be met, for example, in five years, 70% of women giving birth will have had preconception care services during the 3 months before pregnancy. The CDC expert panel did not develop any objectives and the WHO did not specify goals or objectives for PCC but stated an aim for PCC stating that the "ultimate aim of PCC is to improve maternal and child health, in both the short and long term"1. Some objectives to consider include: improving public and provider awareness and knowledge of PCC; enhancing the capacity of professionals to deliver PCC services; ensuring all women receive quality, evidence-based PCC services at healthcare facilities; identifying and managing women at risk of adverse pregnancy outcomes; assuring that all women with identified risk are followed up and managed; improving the health information system with unified data at national and district level; strengthening partnership and coordination mechanisms; and, establishing communication channels and tools to be used at different levels.
Step 4. Solicit and obtain policy-makers involvement and leadership: The success of any program, especially one that requires new policies and resources, depends heavily on the involvement and support of the leadership. Thus, it is essential that individuals leading the PCC program inform, educate, and convince health leaders and policymakers about the maternal, neonatal and child health needs, the existing gaps and the effect of PCC on maternal, neonatal and child health. This information-sharing and education should be done using data summarizing current pregnancy outcomes (maternal and infant) and the risks to pregnancy outcomes related to the health, behaviors, and exposures of women before pregnancy. It also should include information about the evidence showing that PCC works along with examples of programs in other countries.
Step 5. Establish a regional/national taskforce to guide and coordinate the program. The PCC program should be housed within the regional/national Maternal and Child Health program within the department of health. Because PCC services span across many program within the department of health as well as other departments and includes a variety of clinical services, educational and health promotion activities, screening, and preventive services, it is essential that the leadership of this program work closely with individuals who represent sectors within the department of health as well as other governmental and private entities who are engaged in caring for and promoting the health of women. To achieve such broad leadership and engagement, it is proposed that a PCC taskforce be established to guide, oversee the implementation, and monitor progress of the PCC program. Members of this taskforce will also advocate for the PCC program and potentially for additional funding and resources within their organizations and with their partners. It is recommended that members of the taskforce include the following:
• PCC program leaders from the department of health
• PCC experts
• Representatives of physicians and nurses from public and private clinics and hospitals
• Representatives of health educators, social workers, communication specialists, high schools and colleges
• Representatives of insurance companies
• Representatives of professional organizations
• Two or more consumers (men and women of reproductive age)
• Representatives of departments of statistics, information systems, financing
• Other representatives as needed.
Step 6. Establish workgroups to implement the program. To help plan the program and its implementation, it is recommended that a few workgroups by established. These workgroups of 5-10 individuals will work with the coordinator and the PCC team to support their efforts in all aspects of the program. The workgroups would be composed of interested experts in the relevant field as well as representatives of essential partner departments and organizations. The following workgroups are recommended:
• A clinical workgroup to review and keep up-to-date clinical recommendations and to develop or adopt/adapt training materials for clinicians
• A social marketing and health promotion for consumers workgroup to develop and review consumer educational material
• A public health workgroup to follow up on program implementation issues, and
• A data and monitoring workgroup to advise about data collection, analysis and interpretation
Step 7. Develop a monitoring and evaluation plan. Plans for monitoring and evaluating the PCC program must be developed before the program is implemented. There are two questions to be asked: are we doing the right things (outcome evaluation), and are we doing things right (process evaluation). For the first question (are we doing the right things?), we need to know whether what we are doing is helping us achieve the outcome we are trying to achieve, i.e. improving pregnancy outcomes. However, improving pregnancy outcomes is our long-term goal which will need a long time to achieve. Other measures we can use to determine if we are doing the right things in the immediate future are outputs and short-term outcomes. Examples of outputs are numbers of women receiving PCC services, number of women who were referred to family planning services, number of women referred to genetic counseling, etc.
An example of a short-term outcome is number of women consuming the recommended dose of folic acid or the number of women who quit smoking. Examples of long-term outcome are number of babies born preterm, number of infant deaths, number of women who had pregnancy complications, etc. To determine if we are doing things right, we need to collect information that tell us if we are doing the things we decided to do and if we are doing them correctly. For example, did we prepare educational and training materials to raise awareness among leadership, providers and the population? Have we disseminated this material through seminars, meetings, mass media, etc? Have we held training sessions for providers? Are we providing quality services to women and couples?
Some process, output, and outcome information can be easily obtained from existing records such as clinic and hospital records, birth and death certificates, or surveys routinely conducted. Other information may need to be collected through adding questions to or expanding clinic and hospital records or ongoing surveys or by conducting special surveys. Whatever information the program decides to collect, it is extremely important to have a baseline. In the absence of a baseline, it will not be possible to determine if the program has had any added value in terms of services provided or outcomes achieved.
The process of monitoring and evaluating the PCC program starts with deciding what indicators should be used to measure activities and outcomes. Indicators are measurable information used to determine if a program is implementing their program as expected and achieving their outcomes. There are several types of indicators discussed in the literature:
Input indicators: measure the quantity, quality and timeliness of resources provided or available for a project or program e.g. funding; human resources; equipment; materials; or organizational capacity.
Outcome indicators: measure whether the program is achieving the expected effects/changes in the short, intermediate, and long term. Because outcome indicators measure the changes that occur over time, indicators should be measured at least at baseline (before the program/project begins) and at the end of the project. Some programs refer to their longest-term/most distal outcome indicators as Impact indicators. Moreover, because long-term outcomes are often difficult to measure and attribute to a single program, and because programs need immediate information to monitor the effect of their program, some use Output indicators to measure activity implementation or immediate results.
The choice of indicators will often inform the rest of the evaluation plan, including evaluation methods, data analysis, and reporting. Strong indicators can be quantitative or qualitative and are part of the evaluation plan. To ensure the quality and success of the program, the indicators should be reviewed and used for program improvement throughout the program's life cycle.
When selecting indicators, programs should keep in mind that some indicators will be more time-consuming and more costly than others to collect and analyze. One should consider using existing data sources if possible and if not available then factor in the burden needed to collect each indicator before requiring collection. Strong indicators are simple, precise, and measurable. In addition, some programs aspire to indicators that are 'SMART': Specific, measurable, attainable, relevant, and timely.
The CDC workgroup identified eleven domains of preconception health and examined indicators under each domain. The eleven domains are: general health status and life satisfaction; social determinants of health; health care; reproductive health and family planning; tobacco, alcohol and substance use; nutrition and physical activity; mental health; emotional and social support; chronic conditions; infections; and genetics/epigenetics. Proposed indicators were evaluated based on five criteria: public health importance, policy/program importance, data availability, data quality, and the complexity of calculating the indicator.
Ninety-six possible indicators were identified from which 45 were proposed as core indicators to be used by states when evaluating PCC programs16,17. Examples of indicators include: proportion of pregnant women who took folic acid at least during three months before their pregnancy, proportion of pregnant women who received PCC, proportion of low weight births, proportion of newborns with neural tube defect (if possible), and gestational age at prenatal care registration.
Thus, developing a monitoring and evaluation plan includes the following action steps:
• Determine the indicators to be measured: input indicators, output indicators, and impact indicators (discussed in clinical guidelines document)
• Determine if these indicators can be obtained from routinely collected data
• If not already being collected, decide whether the data is essential and should be collected
• If yes, decide the best approach to use for collecting the data:
o Add questions to existing data collection forms (medical records, surveys, etc), or
o Develop a new data collection form, and
o Decide where and when to collect these data: at the PNC visit, at labor and delivery, during well baby visit, or by mail/phone in the postpartum period
IMPLEMENTING A PRECONCEPTION CARE PROGRAM
Once the leadership and staff of the PCC program and their responsibilities have been identified, and once a description of the program is prepared, the PCCU should proceed with implementing the program working closely with the taskforce and the various workgroups. Implementation starts with educating the leadership of the department of health and partner organizations, and then proceeding to implement the program in the field. Preconception health is about the health of women before pregnancy and PCC is only one of many factors that contribute to a woman's health. Thus, PCC services will not be limited to clinical care under the umbrella of maternal and child health, but rather quality PCC services should be delivered within primary health care services by integrating them into reproductive health services, maternal, neonatal, and child health services, premarital counseling services , school health services, and periodic annual exams services. Some programs follow the model of "every woman every time". They suggest that at the beginning of every encounter with a woman of reproductive age, all health care providers, independent of their specialties should ask the woman the following question: would you like to become pregnant in the next year? If the answer is "No": providers should advise the woman to use effective family planning methods and to obtain preconception care as soon as she starts planning a pregnancy; if the answer is "Yes": the providers should provide the woman PCC services or refer her to PCC services. "Every woman every time" implies using every opportunity to ensure that women are aware that their health, behaviors and exposures before pregnancy are important contributors to the outcome of their pregnancy for themselves and their babies. Thus, in implementing the PCC the program should consider various sites and points of entry and not limit itself to maternal and child health services.
Implementing the PCC program in the field should proceed only after the guidelines and communication and training materials have been finalized. Clinical practice guidelines may be adopted or adapted by the clinical workgroup from existing published guidelines. Implementation action steps include:
Step 1. Develop a communication and social mobilization plan. As a first step in implementing a PCC program, the PCCU staff should immediately start working on developing a national communication plan to raise awareness about PCC and its impact on maternal, neonatal and child health outcomes, among providers, consumers, and policy makers. Action steps in this area include the following:
• Start with raising awareness internally with MCH program staff and other leadership within the department of health
• Educate clinical care providers starting with MCH care providers in clinics and hospitals, public and private, by using the proposed policy brief and slide sets to disseminate information at regular staff meetings, seminars and grand rounds
• Encourage taskforce members to educate their organizational leadership and partners about PCC
• Hold regular meetings with other relevant units within the department of health for updates and coordination
• Implement the national PCC communication plan to raise awareness and educate the population about the importance and benefits of PCC and preconception health, with a special focus on school and university students, women, men and couples in the premarital and inter-conception stages
• Use various existing communication channels, including social media, religious leaders, civil society, national media, community leaders and social gatherings
• Working with communication specialists, develop and implement a PCC social mobilization plan.
Step 2. Educate and train the PCC workforce. A very important step in implementing a PCC program is to make sure clinicians know what to do when a reproductive-age woman visits their clinic seeking help whether related to pregnancy or not, and why to do it. Thus, PCC basic education should be provided to all health care providers even before raising awareness among the public so that they can be responsive to the needs of women. Action steps include:
• Develop standardized curricula and tools for training public health and clinical care providers by adapting existing curricula developed by others
• Curricula should include the following:
o Basic education about PCC, its definition, components, and its benefits
o The rationale for implementing PCC
o Interventions that have been identified to be implemented
o Clinical guidelines for managing identified risks through history, screening, and medical assessment
• Incorporate education about PCC into the medical and nursing schools' curricula
• Give special attention to conditions identified as more prevalent in the region/ country where the program is being implemented
• Start with training of trainers and online training in selected clinics to increase the number of trainers and meet demands around the country
• Make training materials and other PCC materials available on the department of health and partner organizations' websites
• Encourage providers to participate in trainings by offering CMEs and other incentives.
Step 3. Start implementation in select sites. Once the guidelines and communication and training materials have been finalized, the program should be implemented in a few select pilot sites (clinics and/or hospitals). This could be done at the same time as communication, education and training are proceeding at the national level. Action steps include:
• Identifying pilot locations for early implementation - consider availability of resources and support of practitioners and leadership
• Training staff in these locations in the delivery of PCC services
• Enrolling staff in a training of trainers program to help disseminate the implementation in other sites
• Modifying training curricula and the implementation process using lessons learned from pilot sites
• Integrating PCC into the health care and supply systems and ensuring sustainability by institutionalizing the program within the delivery systems of pilot sites. department of health, securing resources and maintaining partners' support and engagement.
Step 4. Expand implementation to "ready" sites. Disseminating to other sites should be started upon completion of satisfactory implementation in the pilot phase ensuring that lessons learned from pilot sites are incorporated into the program. Priorities for dissemination should be based on specific criteria developed by the program such as relevance and need of PCC to the target population, level of interest and support among providers and leaders within the sites, availability of resources to educate and train providers, etc. Special attention should be given to the following points when it comes to dissemination:
• Increasing need for trainers: as the number of sites implementing the program increases, the need for more trainers increases. It is not realistic to expect the PCCU staff alone to be able to provide training to the whole country. This need could be addressed by inviting providers from pilot sites to serve as trainers at dissemination sites. Additional trainers should be identified from dissemination sites.
• Sustainability and continuity of the program: to ensure sustainability, PCC should be institutionalized and integrated into the health care and supply systems locally and at the national levels, and by securing resources and maintaining partners' support and engagement. "Refresher" courses will be needed at all sites based on turnover of health care providers and performance following initial training.
Step 5. Initiate and continue monitoring and evaluation process. Data collection and analysis for the purpose of evaluating the program and monitoring its performance should start as soon as implementation is initiated. In fact, baseline data should be collected even before any implementation is initiated. Based on the information needs of the program as determined by the goals, objectives and indicators discussed above, the program should work closely with the health information team to determine what data are needed and where to get the data. This process is ongoing, and information produced must be used to monitor and improve the program performance on an ongoing basis.
Step 6. Establish PCC collaboration networks. To ensure sustainability and quality improvement of the PCC program, there is a need to establish collaborative networks at multiple levels to share updates and lessons learned and to maintain support for the program. Proposed networks include:
• An internal department of health network to include representatives of involved programs (MCH, Education, IT, Primary Health Care, etc)
• The PCC Taskforce
• Networks led by the workgroups described above to include interested individuals (Clinical, data and monitoring, consumer education, and public health)
• A network of intersectoral program workers, and
• A network of regional experts.
The activities and success of these networks could be enhanced and strengthened by having a central website to share educational materials, training tools, and information and updates about activities and results in various localities. These networks should have regular meetings to share practices and experiences and to offer information and technical support to members of the network or others as needed.
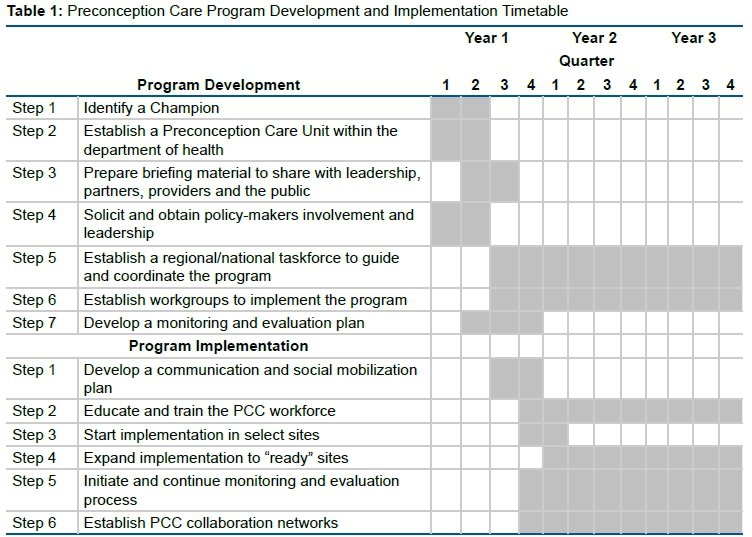
A summary of steps and a proposed timeline for developing and implementing a preconception care program are included in table 1. As indicated in the table, some of the activities are short term and may be completed within a few months while others (such as training and monitoring) are ongoing and should be incorporated in the daily activities of the program.
CONCLUSION
Improving the health of women during the preconception period and developing and implementing a successful preconception care program requires more than effective clinical care for women. Developing and implementing a sustainable PCC program should address issues related to educating the public, providers and policy makers about the benefits of PCC. It also includes establishing an infrastructure within the departments of health and ensuring resources to build, guide, monitor and evaluate the PCC program. Finally, implementation of a successful program depends heavily on the proper training of public health and clinical care providers in the delivery of the services included in the program.
REFERENCES
1.World Health Organization (WHO). Meeting to Develop a Global Consensus on Preconception Care to Reduce Maternal and Childhood Mortality and Morbidity. Geneva: WHO, 2013 [ Links ]
2.Johnson K, Posner SF, Bierman J, Cordero JF, Atrash HK, Parker CS, et al. Recommendations to Improve Preconception Health and Health Care - United States. A Report of the CDC/ATSDR Preconception Care Work Group and the Select Panel on Preconception Care. MMWR Reconn Rep. 2006;55(RR-6):1-23. [ Links ]
3.Hood JR, Parker C, Atrash HK. Recommendations to Improve Preconception Health and Health Care: Strategies for Implementation. J Women's Health. 2007;16(4):454-7. DOI: http://doi.org/10.1089/jwh.2007.CDC3 [ Links ]
4.World Health Organization (WHO). Preconception care: Maximizing the gains for maternal and child health [internet] 2013 [cited 2020 Jun 09] Available from: https://www.who.int/maternal_child_adolescent/documents/preconception_care_policy_brief.pdf [ Links ]
5.South Australian Perinatal Practice Guidelines. Preconception Advice [internet 2015. [cited 2020 Jun 09] Available from: https://www.sahealth.sa.gov.au/wps/wcm/connect/1f11de804eed8cb5afbeaf6a7ac0d6e4/Preconception+Advice_Sept2015.pdf?MOD=AJPERES&CACHEID=ROOTWORKSPACE-1f11de804eed8cb5afbeaf6a7ac0d6e4-n5jkcsW [ Links ]
6.Sheldon T. Netherlands considers introducing preconception care. BMJ. 2007;335(7622):686-7. DOI: http://doi.org/10.1136/bmj.39353.518067.DB [ Links ]
7.Ebrahim SH, Lo SST, Zhuo J, Han JY, Delvoye P, Han JY, Zhu L. Models of Preconception Care Implementation in Selected Countries. Matern Child Health J. 200610(Suppl 1):37-42. DOI: http://doi.org/10.1007/s10995-006-0096-9 [ Links ]
8.Lassi ZS, Dean SV, Mallick D, Bhutta ZA. Preconception care: delivery strategies and packages for care. Reprod Health. 2014;11(Suppl 3):S7. DOI: http://doi.org/10.1186/1742-4755-11-S3-S7 [ Links ]
9.Farahi N, Zolotor A. Recommendations for Preconception Counseling and Care. Am Fam Physician. 2013;88(8):499-506. [ Links ]
10.World Health Organization (WHO). Regional Office for the Eastern Mediterranean. Meeting on Promoting Preconception Care in the Eastern Mediterranean Region. Muscat, Oman, March 25-27 [internet] 2015. [cited 2020 Jun 09] Available from: https://apps.who.int/iris/handle/10665/253415 [ Links ]
11.World Health Organization (WHO). Eastern Mediterranean Regional Office (EMRO): Informal working group on promoting Preconception Care in the Eastern Mediterranean Region. Cairo, Egypt, September 7-8 [internet] 2015. [cited 2020 Jun 09] Available from: http://applications.emro.who.int/docs/IC_Meet_Rep_2015_EN_16669.pdf [ Links ]
12.Gloor PA. Swarm Creativity: Competitive Advantage through Collaborative Innovation Networks. New York: Oxford University Press, 2006. [ Links ]
13.Kania J, Kramer M. Collective Impact. Stanford Social Innovation Review [internet] 2011. [cited 2014 Mar 09] Available from: https://ssir.org/articles/entry/collective_impact [ Links ]
14.Turner S, Merchant K, Kania J, Martin E. Understanding the Value of Backbone Organizations in Collective Impact: Part 3. Stanford Social Innovation Review [internet] 2012. [cited 2014 Mar 09] Available from: https://ssir.org/articles/entry/understanding_the_value_of_backbone_organizations_in_collective_impact_3# [ Links ]
15.Developing Program Goals and Measurable Objectives. CDC [internet]. [cited 2020 May 09] Available from: https://www.cdc.gov/std/Program/pupestd/Developing%20Program%20Goals%20and%20Objectives.pdf. [ Links ]
16.Broussard DL, Sappenfield WB, Fussman C, Kroelinger CD, Grigorescu V. Core state preconception health indicators: a voluntary, multi-state selection process. Matern Child Health J. 2011;1592):158-68. DOI: http://doi.org/10.1007/s10995-010-0575-x [ Links ]
17.Robbins CL, Zapata LP, Farr SL, Kroelinger CD, Morrow B, Ahluwalia I, et al. Core State Preconception Health Indicators - Pregnancy Risk Assessment Monitoring System and Behavioral Risk Factor Surveillance System, 2009. MMWR Surveillance Summaries. 2014;63(3):1-61. [ Links ]
 Correspondence:
Correspondence:
Hani Atrash
hatrash@emory.edu
Received: May 2020
Revised: May 2020
Accepted: September 2020


{kind=link}