










Serviços Personalizados
Journal

artigo
 Inglês (pdf)
Inglês (pdf)
 Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
Indicadores
Compartilhar

 Permalink
PermalinkPsicologia: teoria e prática
versão impressa ISSN 1516-3687
Psicol. teor. prat. vol.20 no.3 São Paulo set./dez. 2018
https://doi.org/10.5935/1980-6906/psicologia.v20n3p329-342
ARTICLES
CLINICAL PSYCHOLOGY
An interventional proposal for binge eating among individuals who have undergone bariatric surgery
Una propuesta de intervención para la compulsión alimentaria de individuos sometidos a la cirugía bariátrica
Beatriz Azevedo Moraes; Paola Espósito de Moraes Almeida
Pontifical Catholic University of São Paulo - PUC-SP SP Brazil
ABSTRACT
This study's objective was to investigate the effects of providing instructions and token reinforcement in the control of the eating behavior for two women who had undergone bariatric surgery and described a compulsive eating pattern. The design consisted of four phases: 1. baseline, 2. reinforcing correspondence between electronic recording and pictures of meals, 3. composed of two subphases: 3.1. instruction and contingent reinforcement of eating every three hours and 3.2. instructing and reinforcing the preparation and ingestion of a daily portion of palatable food, up to 150 kcal. The results show a decrease in the intervals between meals and an increase in the continuous and limited intake of palatable foods, accompanied by a decrease in the report of compulsive episodes. The results suggest that a decrease in binge eating can be achieved by avoiding food restrictions and intermittent access to palatable foods, as previously reported by experimental studies.
Keywords: palatable foods; bariatric surgery; binge eating; food restriction; behavioral therapy.
RESUMEN
En el presente trabajo se investigó el efecto de instrucciones y un procedimiento de economia de fichas en el control del comportamiento alimentario compulsivo de dos mujeres que realizaron la cirugia bariátrica. El diseno tuvo cuatro fases: 1. linea de base, 2. reforzamiento para la correspondencia entre el registro electrónico y la foto de las comidas, 3. compuesta por dos subfases: 3.1. instrucción y refuerzo contingente para una alimentación de tres en tres horas y 3.2. instrucción y reforzamiento contingente para la preparación e ingestión de una porción diaria de alimentos palatables (150 calorias). Los resultados senalaron la reducción en los intervalos entre las comidas y el aumento en la ingestión de palatables de forma continua y limitada, acompanada de una reducción en el relato de episodios compulsivos. Tal constatación sugiere que la reducción en la compulsión alimentaria puede alcanzarse al evitar la restricción alimentaria y el acceso intermitente a los alimentos palatables.
Palabras clave: alimentos palatables; cirugia bariátrica; compulsión alimenticia; restricción alimentaria; terapia conductual.
Introduction
Binge eating is listed in the classification of eating disorders of the Diagnostic and Statistical Manual of Mental Disorders (DSM-V), organized by the American Psychiatric Association (APA, 2013). Binge eating is defined as the intake of large amounts of food, larger than most people would consume in similar circumstances, in a short period of time (Moshe, Bekker, & Weller, 2017). Binge eating episodes are marked by a sense of lack of control, guilt or shame, usually described by those whose eating behavior is defined as compulsive.
In behavior analysis, overeating, as well as any other behavior, is determined by biological, ontogenetic, and cultural variables, such as: an appreciation for a slender body in Western cultures; the role of the media in encouraging the consumption of foods with poor nutritional value; the vulnerability to the reinforcement of sweet and fatty foods widely available after industrialization; the effects that follow food response; and the antecedent conditions that control such behavior (Turton, Chami, & Treasure, 2017; Schulte, Potenza, & Gearhardt, 2017).
In the case of binge eating, the literature highlights the importance of a history of food restriction and access to palatable foods as one of the determinants of compulsive eating patterns (Corwin, Avena, & Boggiano, 2011; Hagan, Chandler, Wauford, Rybak, & Oswald, 2003). Experimental studies submitting animals to a history of food restriction combined with feedback of sweet and fatty goods report excessive food consumption, even in the absence of food deprivation (Corwin, Avena, & Boggiano, 2011; Novelle & Diègues, 2018). Even animals initially less susceptible to excessive eating behavior came to show it after such a combination (Oswald, Murdaugh, King, & Boggiano, 2011), an effect especially noticed among females (Sinclair, Hildebrandt, Culbert, Klump, & Sisk, 2017). On the other hand, when not associated with food restriction, continuous and restricted access to palatable foods does not seem to produce excessive eating patterns in animals (Kreisler, Garcia, Spierling, Hui, & Zorrilla, 2017; Wojnicki, Johnson, & Corwin, 2008) or in humans (Temple, Bulkley, Badawy, Krause, McCann, & Epstein, 2009).
In the study by Wojnicki et al. (2008) for instance, vegetal fat was intermittently or continuously presented to different groups of mice, in limited or unlimited amounts, throughout five weeks. In the next five weeks, the animals' eating behavior was assessed when freely supplied with fatty foods. In this condition, those animals that had continuous and limited access to palatable foods consumed less than those that initially had continuous and unlimited or intermittent access to these foods.
Temple et al. (2009), in turn, investigated the effects of consuming different portions of palatable foods on the reinforcing value of foods (chosen through a preference test applied to each participant) among 31 obese and 27 non-obese women. The reinforcing values were measured using many responses provided via a computer game to obtain points that would be exchanged for foods in a reinforcing scheme of a variable ratio. The reinforcing values of foods were tested at the beginning of the experiment and after two weeks of daily consumption of 0, 100 or 300 kcal/day of the same chosen food. The results of the operating measures show that the daily consumption of a 300 kcal snack for two weeks resulted in an increase in the reinforcing value of food in the group of obese women, while non-obese women exhibited the opposite response. No significant differences were found in the value of the food as reinforcement for the conditions of the size of portions of 0 and 100 kcal. These findings suggest that obese and non-obese women respond differently to the daily intake of snacks and that continuous access to small portions of foods may be a viable mechanism to decrease the value of food reinforcement in obese women.
Even though the regular consumption of palatable foods seems desirable to avoid binge eating episodes, such foods seem to interfere with the regulation of a healthy diet in experimental animals, which present a lower response to previously accepted feed after having access to sweet foods for long periods (Kreisler et al., 2017).
Data suggest that there is a need to avoid food restrictions and their combination with an intermittent supply of palatable foods when a healthy diet is intended.
In this study, the control of these variables was investigated in a population of women with a prior history of obesity and who had undergone bariatric surgery. The treatment of obesity involves nutritional, drug and psychotherapeutic approaches, along with physical exercise. When a patient does not respond to these treatments, bariatric surgery is frequently recommended, which consists of interventions performed in the digestive tract using either malabsorptive or restrictive techniques (Fandino, Benchimol, Coutinho, & Appolinario, 2004), in order to cause weight loss (Quadros, Bruscato, & Branco, 2017). Even though this surgery causes structural changes in the body, it does not seem to impede overeating in a portion of patients, so the report of weight regain due to patients having gone back to inadequate eating patterns is evident within two or three years after surgery (Nasirzadeh et al., 2018; Siqueira & Zanotti, 2017), requiring new surgery due to various complications (Souto et al, 2017).
This study's objective was to assess the effect of strategies intended to regulate the eating behavior of post-surgical patients based on the control of variables indicated in the literature as being related to compulsive overeating. This study proposes the investigation of: 1. the effect of providing instructions and reinforcing the control of eating responses at regular mealtimes, ensuring continuous and limited access to palatable foods; and 2. the effect of such control on the frequency of compulsive overeating, using a self-monitoring strategy.
Method
Participants
Two women who had undergone bariatric surgery participated in the study. They were recruited from a social network group organized around this topic. Inclusion criteria were: the participants should report compulsive overeating (concerning the frequency, amount, and caloric intake) after the surgery and the ability to use electronic devices (tablets). The researcher held two individual meetings with the participants to collect data concerning the type of surgery and information regarding the history of weight-loss diets, consumption pattern (weekly frequency/amount) of sweet or fatty foods (palatable), and weight history. Data resulted in the following characterization of participants:
• P1, 29 years old with a history of various attempts to lose weight before the surgery; lost 45 kg with the surgery that took place 15 months before the study; reported the daily intake of sweet and fatty foods.
• P2, 36 years old with a history of various attempts to lose weight before the surgery; lost 39 kg with the surgery that took place nine months before the study; reported an intake of sweet and fatty foods two or three times a week.
Material
• Tablet devices, which were provided by the researcher and contained an application that allowed the participants to make photographic recordings, food consumption recordings, and report dates and times when the recordings were performed.
• A form developed by the researcher for the participants to record their body-weight history.
• A self-monitoring form addressing the participant's name, food consumed, time of consumption, amount, and an assessment as to whether there was compulsive overeating or not based on four different requirements (amount, speed, quality and interval between meals). This form also included a category named "other" where the participants could report conditions that evoked, by description, an overeating episode;
• Tokens signed by the researcher that could be exchanged for gift cards and a catalog of products from the department store where the participants would exchange these gift cards.
• A form listing ten nutritional instructions meant for individuals who had bariatric surgery more than six months ago; and free and informed consent forms.
The study was submitted to and approved by the Institutional Review Board regulating research with human subjects through Plataforma Brasil (Protocol No. 15171614.3.0000.5482).
Procedure
• Phase 1 - Eating behavior baseline: a meeting was held with the participants to teach them to use the equipment and make the photographic recording and to use the self-monitoring form. After training, each participant started recording their meals and the recordings were sent daily to the researcher via e-mail. In this phase (and during the entire phase of data collection), three meetings were held every week (one every two days) for the researcher to collect the recording forms and clarify the participants' potential doubts. The criterion used to determine whether this phase was complete was the record of 70% of meals throughout seven consecutive days at the end of 60 days of data collection. The number of days (more than 30 days) was used in this phase and remaining phases of the study to identify regularities in the participants' eating patterns and avoid temporary changes caused by occasional and unusual circumstances (weekends, parties, among other reasons) being taken as representative of this pattern. The participants would be excluded from the study if they did not meet this criterion.
• Phase 2 - Reinforcing correspondence between photographic recording and self-monitoring recording: in this phase, food intake was recorded for two weeks using the aforementioned strategies. To ensure there was a correspondence between both records, the participants started earning tokens whenever the description of foods consumed provided in the self-monitoring form corresponded to the pictures they took. The objective was to promote contingencies in which the participants would provide an accurate report, regardless of its content. Hence, during this phase, each participant could, for instance, earn a token for having reported the intake of fatty food and food with little nutritional value, as long as the photographic image showed this consumption. Accurate description of eating episodes was important because the measures used to assess the effects of the intervention (changes in eating patterns and frequency of compulsive overeating) were based on the verbal reports of each participant, and the requirement of a photographic recording of meals was an indirect measure of such reporting.
The researcher was present for the first meal of this phase and each participant recorded the meal and received the first token because of the correspondence between recordings. The participants also received a catalog from the department store listing the products for which the tokens could be exchanged after the last meeting of the week.
The criterion to complete this phase was that the participants presented a minimum of 70% correspondence between the self-monitoring report and pictures for four consecutive days. Correspondence between self-monitoring and pictures was reinforced in all the phases that followed and a minimum of 70% correspondence was required for the participants' data to be considered in the analysis.
Table 1 indicates the number of tokens that could be earned during the different phases based on correspondence found between the pictures and reports of participants' meals.
• Phase 3 - Procedure in which eating responses according to prescriptions were instructed and reinforced: during this phase, in addition to the tokens the participants received for achieving correspondence between recordings (initiated in the previous phase), the participants also began to receive tokens of different colors that could be exchanged at the end of the week for a gift card of a higher value, if the researchers' instructions had been followed. The value of the gift card was adjusted according to the total tokens received, as shown in Table 1. The experimental design implemented in this phase was the Multiple-Baseline between responses. Instructions and reinforcement were initially presented for the first class of responses (regular mealtimes), followed by regular changes, experienced by the participants, for this class of responses produced by the introduction of experimental variables. The same procedure was then adopted for the second class of responses (eating palatable foods in a continuous manner and limited amounts). The criterion established for the introduction of experimental variables in Subphase 3.1 was that 80% of the participants' recordings from previous phases indicated some meals within the same range. In the case of Subphase 3.2, the experimental variables were introduced after an effect was shown for the first class of responses.
In Phase 3.1, oral and written instructions were presented concerning the need to maintain regular mealtimes (every three hours). An alarm was set up on the cellphone of each participant, with the times when meals were supposed to be eaten. The participants should follow the instructions to have their meals according to the scheduled times and update their records, while the electronic device indicated the time when the picture was taken - information that was used as an indirect measure of the intervals of meals throughout the day. If the meal were eaten within the prescheduled timeframe (from 2 to 4 hours after the previous meal), the participant would get a token for each meal. Based on nutritional guidance and data obtained at baseline, under this condition, the participants could earn up to six tokens a day, one for each meal that followed the prescribed instructions. Criteria for exchanging the tokens for gift cards are described in Table 1.
When the manipulated variables showed an effect on the participants' eating behavior, that is, that they were eating at regular intervals of time, Phase 3.2 was initiated, in which instructions and reinforcement were given for the participants to present continuous and limited responses to palatable foods. In this condition, the participants should choose and prepare beforehand a portion of palatable food (of up to 150 kcal) to be eaten daily. Every day, the participant could get a token for having followed the instructions to prepare the food and another token for having eaten the amount indicated. The criteria for exchanging the tokens for gift cards of different values at the end of the week are described in Table 1.
• Phase 4 - No reinforcement: to assess the effect of the variables introduced in the previous phases, in this one, the participants kept recording their meals using the self-monitoring form and pictures. However, they were not given any instruction or tokens for their performance. The procedure was the same as the one implemented at the baseline.
Analysis of inter-rater agreement
Two observers analyzed 10% of the recordings of each phase as a sample throughout the entire data collection period, one of whom was the researcher herself. Percentage of inter-rater agreement was calculated by dividing inter-rater agreement by the sum of total agreement with non-agreement in each of the phases of data collection. The observers were considered apt if they reached 70% agreement in the analysis of correspondence between picture and self-monitoring recording after a previous training session at the beginning of the study. Inter-rater agreement remained at 91% during the entire design.
Results
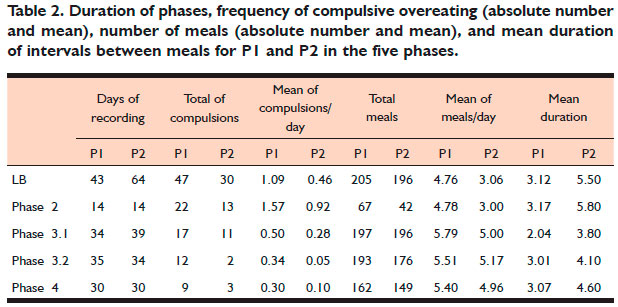
The results presented here refer to the performance of both participants in each phase of the study. Table 2 summarizes the duration of the intervention phases, total frequency, and mean of compulsive overeating episodes reported during this period, and total number and mean of meals per day. The analysis of means was considered because the duration of the different phases varied throughout the study for the different participants, hindering comparison between the absolute number of times in which compulsive overeating took place or number of meals.
Table 2 shows that the intervention produced similar effects for both participants concerning frequency of compulsive episodes. Note that a decrease in the mean of compulsive overeating accompanies an increase in the number of meals, and a consequent decrease of intervals between meals, an effect that is visible in Subphase 3.1, when the variables were applied to control the regular mealtimes' response. Under this condition, P1 obtained a mean of 5.79 daily meals, with shorter intervals between meals, while P2 also obtained a mean 5.0 meals per day, also at shorter intervals. These numbers seem to indicate the efficiency of the procedure to promote changes in the participants' eating patterns, accompanied by a decrease in compulsive overeating episodes. The interruption of this procedure in the following conditions (phases 3.2 and 4) was accompanied by a decrease in the number of daily meals and an increase in the interval between meals. Nonetheless, a comparison of the results obtained at the end of the study with those obtained at the baseline indicates that the benefits of the intervention held for both.
A second aspect to be highlighted in Table 2 is the increase in the reports of compulsive overeating for both participants during Phase 2, when correspondence between self-reporting and photographic recording was demanded. Such an increase
BB6
may be because this phase was composed of fewer days, which may have changed the opportunity for reporting, or, due to an effect of having reinforced correspondence between intake report and photographic recording, regardless of the content of verbal responses. In the second case, the results may also suggest that requiring correspondence between recordings was an important strategy for obtaining the description of compulsive episodes that may have been omitted in the previous phase.
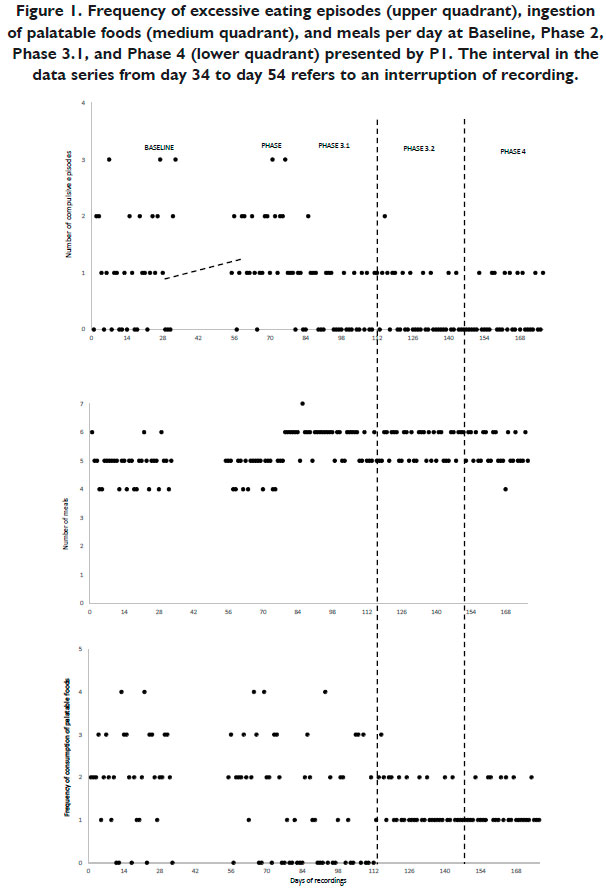
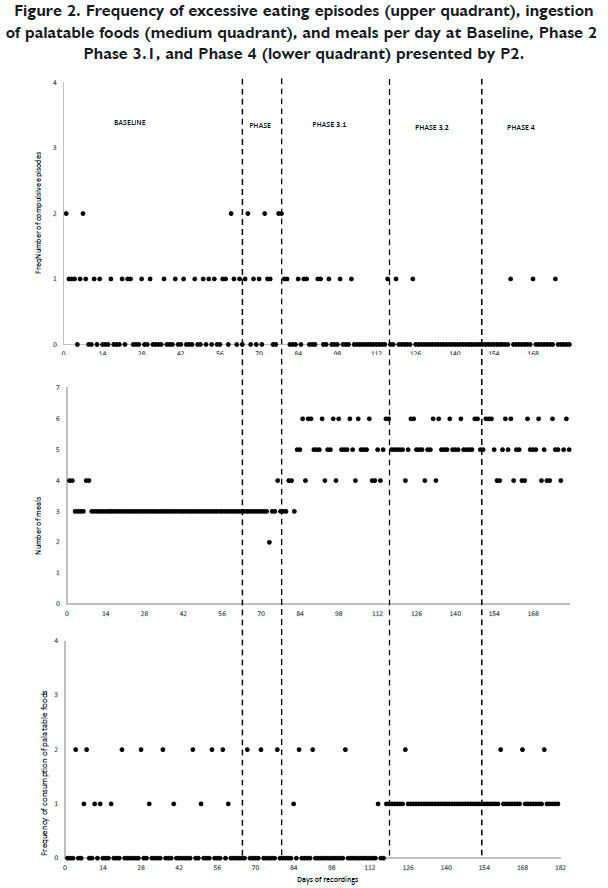
Figures 1 and 2 portray the daily frequency of compulsive overeating episodes (upper quadrant), the number of daily meals (middle quadrant), and frequency of palatable foods intake (lower quadrant), of each participant in the study's different phases. The interruption in the data indicates a lack of recordings for the day.
Figure 1 shows that, during phases 1 (baseline) and 2, P1 reported a frequency of compulsive overeating episodes that ranged from one to three daily episodes, while in 40 days (70%) she reported at least one episode. In the two first phases, P2, in turn, reported from 0 to two daily episodes in 36 days (46%), as shown in Figure 2.
With the beginning of the intervention, starting with Subphase 3.1, an increase in the number of meals was observed for P1 and P2 (medium quadrant of Figures 1 and 2). Such an increase was accompanied by a decrease in the number of compulsive overeating episodes (upper quadrant). With the beginning of Phase 3.1, the number of meals reached a value never attained in the previous phases, an effect visible in the case of P2. Note that the smaller number of meals, a situation that was frequent at baseline and Phase 2, no longer occurred in Phase 3.1 for both participants. In the case of P1, an increase in the number of daily meals was accompanied by fewer than three binge episodes per day, and a decrease in the number of days in which they reported such episodes (44% of the days during Subphase 3.1, compared to 70% of the days reported in the previous phases). P2, in turn, no longer reported two-compulsive overeating episodes/day and reported the occurrence of 11 episodes considered to be compulsive, that is, compulsive overeating was reported in only 28% of the days in Phase 3.1, compared to 46% of the days previous to the inclusion of experimental variables.
When the participants received instructions and reinforcement to prepare and consume a small portion of palatable food during Phase 3.2, the frequency of compulsive overeating reports continued to decrease: on only 11 (32%) and two (6%) days of this phase, respectively, P1 and P2 reported compulsive overeating. Analysis of the lower quadrants presented in Figures 1 and 2 seems to indicate that at baseline, P1 had (almost) continuous though unlimited access to this quality of food, while for 51 days (90%) the participant reported the ingestion of palatable foods and, on 45 days (80%), she reported eating portions of these foods (not necessarily portions up to 150 kcal) more than once a day. In Phase 1 - baseline and Phase 2, P2's consumption of palatable foods was intermittent and unlimited, and for 19 days (25%) of phases 1 and 2, she ingested two portions of these foods. With the beginning of Subphase 3.2, P1 decreased the ingestion of these foods, and on 24 days (68%) she started consuming only the portion recommended. P2, in turn, started eating palatable foods daily, and reported having eaten two portions of this food on only one day.
In Phase 4, when the contingencies for controlling eating responses were suspended, the ingestion of palatable foods was more easily maintained compared to regular mealtimes. Even though compulsive overeating episodes still occurred during Phase 4, in nine (30%) and 12 of the days (40%), the frequency of these reports decreased for both for P1 and P2, respectively. Comparison, between the occurrence of compulsive overeating episodes during Phase 4 and those described at Baseline when compulsive overeating episodes were reported on 70% of the days for P1 and 46% of the days for P2, indicates this intervention was beneficial.
Conclusion
The literature addressing variables that determine overeating episodes highlights the importance of having access to palatable foods and food restrictions to determine the phenomenon called compulsive overeating (Novelle & Diegues, 2018; Sinclair et al., 2017; Hagan et al., 2003; Oswald et al., 2011).
This study's results seem to confirm the effect of these variables, indicating that regular mealtimes and continuous and limited access to palatable foods may favor a decrease in compulsive overeating among bariatric patients. Considering that weight loss achieved after bariatric surgery is hindered among patients with compulsive overeating complaints (Nasirzadeh et al., 2018; Siqueira & Zanotti, 2017; Niego, Kofman, Weiss, & Geliebter, 2007) and that structural changes in the body do not seem sufficient to avoid binge eating episodes, the identification of efficient procedures to change this eating pattern can contribute to clinical practice.
Additionally, considering the difficulties in directly observing the occurrence of compulsive overeating episodes among outpatients, this study is expected to contribute to proposals of alternatives for collecting data in this population. The use of electronic devices for self-monitoring and the photographic recording of meals are strategies intended to ensure greater reliability of data, as they facilitate adherence to self-monitoring procedures and serve as indirect measures of eating behaviors. These strategies are important because they allow studies to be developed that respond to criticism directed to behavior analysts, accused of not contributing significantly to the treatment of clinical complaints reported by the non-institutionalized adult population (Woods, Miltenbergr, & Carr, 2006).
This study's limitations include that fact that the participants may have omitted information from the manual and photographic recordings of their meals or recorded meals they did not consume. This study intended to reduce potential distortions by reinforcing, during Phase 2, the correspondence between the participants' verbal (written self-monitoring) and non-verbal reports (eating behavior recorded through pictures), regardless of content. This strategy seemed efficient to ensure accurate reports of eating episodes, considering these episodes were properly described even when considered undesirable (e.g., the consumption of palatable foods in a greater amount than prescribed by the researcher was reported). A suggestion is that this strategy is reassessed in future studies that depend on verbal reports as sources of data and are intended to investigate clinical behaviors that are not easily or directly observed.
Finally, analysis of the participants' general eating behaviors indicates that, even though both described compulsive overeating patterns, differences in what is considered to be irregular in the eating behavior of each of the participants could be verified. P1 showed an excessive consumption of sugar, while P2 presented an inappropriate interval between meals. Therefore, note that there is a need to plan individualized interventions that take into account the particular difficulties presented in each case regarding common diagnostic classification.
References
American Psychiatric Association (2013). Diagnostic and statistical manual of mental disorders (5th ed.). Washington: American Psychiatric Association. [ Links ]
Corwin, R. L., Avena, N. M., & Boggiano, M. M. (2011) Feeding and reward: perspectives from three rat models of binge eating. Physiology and Behavior, 104,87-97. doi:10.1016/j.physbeh.2011.04.041 [ Links ]
Fandino, J., Benchimol, A. K., Coutinho, W. F., & Appolinário, J. C. (2004). Cirurgia bariátrica: aspectos clínico-cirúrgicos e psiquiátricos. Revista de Psiquiatria do Rio Grande do Sul, 26(1),47-51. doi:10.1590/S0101-81082004000100007 [ Links ]
Hagan, M. M., Chandler, P. C., Wauford, P. K., Rybak, R. J., & Oswald, K. D. (2003). The role of palatable food and hunger as trigger factors in an animal model of stress-induced binge-eating. International Journal of Eating Disorders, 34, 183-197. doi:10.1002/eat.10168 [ Links ]
Kreisler, A. D., Garcia, M. G., Spierling, S. R., Hui, B. E., & Zorrilla, E. P. (2017). Extended vs. brief intermittent access to palatable food differently promote binge-like intake, rejection of less preferred food, and weight cycling in female rats. Physiology & behavior, 177,305-316. doi:10.1016/j.physbeh.2017.03.039 [ Links ]
Moshe, L., Bekker, L., & Weller, A. (2017). A potential animal model of maladaptive palatable food consumption followed by delayed discomfort. Frontiers in Neuroscience, 11,377. doi:10.3389/fnins.2017.00377 [ Links ]
Nasirzadeh, Y., Kantarovich, K., Wnuk, S., Okrainec, A., Cassin, S. E., Hawa, R., & Sockalingam, S. (2018). Binge eating, loss of control over eating, emotional eating, and night eating after bariatric surgery: results from the Toronto Bari-SYCH Cohort Study. Obesity Surgery, 28,2032-2039. doi:10.1007/s11695-018-3137-8
Niego, S. H., Kofman M. D., Weiss, J. J., Geliebter, A. (2007). Binge eating in the bariatric surgery population: a review of the literature. International Journal of Eating Disorders, 40(4),349-359. doi:10.1002/eat.20376 [ Links ]
Novelle, M. G., & Diéguez, C. (2018). Food addiction and binge eating: lessons learned from animal models. Nutrients, 10(1),1-24. doi:10.3390/nu10010071 [ Links ]
Oswald, K. D., Murdaugh, L. D., King, L. V., & Boggiano, M. M. (2011). Motivation for palatable food despite consequences in an animal model of binge-eating. International Journal of Eating Disorders, 44,203-211. doi:10.1002/eat.20808 [ Links ]
Quadros, M. R. R., Bruscato, G. T., & Branco, A. J., Filho (2017). Compulsão alimentar em pacientes no pré-operatório de cirurgia bariátrica. Psicologia Argumento, 24(45),59-65. doi:10.7213/psicolargum.v24i45.20159
Schulte, E. M., Potenza, M. N., & Gearhardt, A. N. (2017). A commentary on the "eating addiction" versus "food addiction" perspectives on addictive-like food consumption. Appetite, 115,9-15. doi:10.1016/j.appet.2016.10.033 [ Links ]
Sinclair, E. B., Hildebrandt, B. A., Culbert, K. M., Klump, K. L., & Sisk, C. L. (2017). Preliminary evidence of sex differences in behavioral and neural responses to palatable food reward in rats. Physiology & behavior, 176,165-173. doi:10.1016/j.physbeh.2017.03.042
Siqueira, A. C. D., & Zanotti, S. V. (2017). Programa de cirurgia bariátrica e reganho de peso: case study of a bariatric surgery program. Psicologia, Saúde & Doenças, 18(1),157-159. doi:10.15309/17psd180114 [ Links ]
Souto, K. P., Meinhardt, N. G., de Azevedo Dossin, I., Ramos, M. J., Carnellos, G., Mazzaferro, C., ... & Damin, D. C. (2017). Revisional Malabsorptive Bariatric Surgery: 29-Year Follow-up in a Brazilian public hospital. Obesity Surgery, 28(6),1-7. doi:10.1007/s11695-017-3023-9. [ Links ]
Temple, J. L., Bulkley, A. M., Badawy, R. L., Krause, N., McCann, S., & Epstein, L. H. (2009). Differencial effects of daily snack food intake on the reinforcing value of food in obese and nonobese women. American Journal of Clinical Nutrition, 90,1-10. doi:10.3945/ajcn.2008.27283 [ Links ]
Turton, R., Chami, R., & Treasure, J. (2017). Emotional eating, binge eating and animal models of binge-type eating disorders. Current obesity reports, 6(2),217-228. doi:10.1007/s13679-017-0265-8 [ Links ]
Wojnicki, F. H., Johnson, D. S., & Corwin, R. L. (2008). Access conditions affect binge-type shortening consumption in rats. Physiology and Behavior, 95(5),649-657. doi:10.1016/j.physbeh.2008.09.017 [ Links ]
Woods, D. W., Miltenberger, R. G., & Carr, J. E. (2006). Introduction to the special section on clinical behavior analysis. Journal of Applied Behavior Analysis, 39,407-411. doi:10.1901/jaba.2006.intro [ Links ]
 Mailling address:
Mailling address:
Beatriz Azevedo Moraes
Rua Bernardo Guimarães, 105, sala 909
Sorocaba, SP, Brasil. CEP: 18030050
E-mail: biaamoraes@gmail.com
Submission: 31.1.18
Acceptance: 14.6.18


{kind=link}
{kind=link}
{kind=link}
{kind=link}