










Serviços Personalizados
Journal

artigo
 Inglês (pdf)
Inglês (pdf)
 Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
Indicadores
Compartilhar

 Permalink
PermalinkPsicologia: teoria e prática
versão impressa ISSN 1516-3687
Psicol. teor. prat. vol.21 no.3 São Paulo set./dez. 2019
https://doi.org/10.5935/1980-6906/psicologia.v21n3p77-92
ARTICLES
PSYCHOLOGICAL EVALUATION
Cultural adaptation of the health behaviour protocol in school-aged children for the brazilian reality
Adaptación cultural del health behaviour protocol in school-aged children para la realidad brasileña
Juliana MaltoniI; Carolina S. de M. LisboaII; Margarida G. de MatosIII; Maycoln L. M. TeodoroIV; Carmem Beatriz NeufeldV
ICognitive Behavioral Research and Intervention Laboratory (LaPICC), University of São Paulo (USP)
IIPostgraduate Program in Psychology, Pontifical Catholic University of Rio Grande do Sul (PUCRS)
IIIDepartment of Education, Social Sciences, and Humanities, University of Lisbon (ULisboa)
IVPsychology Program: Cognition and Behavior, Federal University of Minas Gerais (UFMG)
VCognitive Behavioral Research and Intervention Laboratory (LaPICC), University of São Paulo (USP)
ABSTRACT
Adolescence is a period of intense transformations, and these may be inherent or present risks to development. Adolescent health directly influences on individual and society future trajectories, assuring the need for research about this life span stage. The Health Behaviour in School-aged Children task force, together with World Health Organization (HBSC-WHO), has been conducting health surveys for more than 30 years with its protocol, with approximately 40 countries in North America and Europe. This work aimed to present the translation and cultural adaptation process of the HBSC instrument for the Brazilian reality. This is the first study to carry out the adaptation of this instrument in Brazil. The process used the translation of judges, a committee, evaluation in the target public, and pilot study. It was concluded by the satisfactory adaptation of the instrument to the Brazilian reality, being configured as Questionnaire HBSC Brazil.
Keywords: translating; cultural adaptation; health surveys; adolescent health; HBSC.
RESUMEN
La adolescencia es una fase de intensas transformaciones, pudiendo ser positiva o presentar riesgos al desarrollo. La salud adolescente influye directamente en trayectorias futuras individuales y de la sociedad, confirmando la necesidad de investigaciones acerca de este período del ciclo vital. La fuerza de trabajo Health Behaviour in School-aged Children, con la World Health Organization (HBSC-WHO), ha realizado levantamientos de salud hace más de 30 años con un protocolo propio, contando con aproximadamente 40 países de América del Norte y Europa. El objetivo de este trabajo fue presentar el proceso de traducción y adaptación cultural del instrumento HBSC para la realidad brasileña. Este es el primer estudio a realizar la adaptación de este instrumento en Brasil. El proceso utilizó la traducción de jueces, un comité del área, evaluación en público objetivo y estudio piloto. Se concluyó por la adaptación satisfactoria del instrumento a la realidad brasileña, configurándose Cuestionario HBSC Brasil.
Palabras clave: traducción; adaptación cultural; encuestas epidemiológicas; salud del adolescente; HBSC.
1. Introduction
Adolescence comprises the period between the ages of 10 and 20, with some variation in this range, depending on the literature (Brasil, 1990; Papalia, Olds, & Feldman, 2010; World Health Organization, 2011, 2014). Adolescence is marked by intense physical, biological, social, and cognitive transformations and, although it is considered a favorable developmental stage, it is also characterized by the presence of risk behaviours that can influence physical and mental health in adulthood (Bower, Carroll, & Ashman, 2012; Hallal, Victoria, Azevedo, & Wells, 2006; Inchley et al., 2016; Lansford, Dodge, Fontaine, Bates, & Pettit, 2014; Romer, Reyna, & Satterthwaite, 2017; Schneider, Dumith, Orlandi, & Assunção, 2017). Assessing health during adolescence is indispensable to understand these individuals' current condition and demands, indicators, and associated risk and protection factors for the development of appropriate preventive interventions and strategies.
In Brazil, one of the most extensive studies on adolescent health is the National School Health Survey (PeNSE) (Instituto Brasileiro de Geografia e Estatística, 2016), which has three editions with national samples representative of the different Brazilian states. Another important survey in the area was the VI National Survey on Psychotropic Drug Use among Primary and Secondary Students of Public and Private Education Networks in the 27 Brazilian Capitals (Carlini et al., 2010), but it was only based on the indicators and behaviours related to substance use.
In the international scenario, the transnational survey Health Behaviour in School-aged Children (HBSC)1 aims to investigate adolescent health behaviours and indicators. The HBSC task force has existed for more than 30 years, constituting a transnational survey that conducts studies every four years. The project is a collaborative study of the World Health Organization (WHO). It currently involves 47 European and North American countries in international surveys, whose data are published in national and international reports and scientific circles.
According to a report by Currie, Gabhainn, Godeau, and the International HBSC Network Coordinating Committee (2009), the study emerged from the discussion of European researchers in 1982, when they perceived problems comparing data on youth smoking among their countries. A standard research protocol was then developed for more secure cross-border comparisons. The study aims to understand these results as part of a complex system, recognizing the changes over time and how they occur in different national, cultural, social, and economic realities. The study is carried out with 11-, 13- and 15-year-old school children, aiming to cover the ages that represent the beginning and middle of adolescence - the initial transformations and challenges, increased autonomy, and decision making for the future and career. The 11, 13, and 15-year-old range also covers the ages of compulsory schooling in the investigated countries.
The HBSC project does not aim to be a general epidemiological study because it works within the perspective that health behaviours are formed and derive from patterns interconnected with the adolescents' lifestyle and context. The HBSC Protocol used purposes to quantify patterns of behaviour, indicators, and contextual variables related to health, demonstrating the changes that occurred in the transition from childhood to adulthood in the most diverse areas. The thematic axes of the aspects are: sociodemographic factors, food, hygiene, body, substance consumption, school, quality of life, physical and psychological well-being, physical activity, sexual behaviour, provocation, injuries, family relationship, relationship with peers, free time, and communication through electronic equipment. The study is a valid and reliable source about adolescent health indicators and behaviours, and the most recent survey involved approximately 220 thousand individuals (Inchley et al., 2016).
With regard to regional (Braz, Filho, & Barros, 2013; Reis, Almeida, Miranda, Alves, & Madeira, 2013; Sousa et al., 2010) and Brazilian surveys (Carlini et al., 2010; IBGE, 2016), the HBSC study is more focused on the differences in sex, age, and study regions, also considering the peers, relationship with the school, and the use of electronic media for communication. Also, it counts on the evaluation of several health spheres and performs descriptions and recommendations of intervention guidelines, seeking to assess the implied health inequalities among adolescents. The range of the issues investigated and their international validation indicates the relevance of this project and the gains in using it in the Brazilian context.
In 2015, Brazil was approved to act as an International Linked Project, through the approval of the Brazilian application in the HBSC project. This is the first application in the country, permitting participation in conferences, data dissemination and scientific forums in the area, with the future objective of integrating transnational surveys into the task force. The project under development in Brazil occurs since 2015, being considered a multicenter study, with a coordinating center in Ribeirão Preto, in the State of São Paulo. It currently includes five other Brazilian states - Minas Gerais, Rio Grande do Sul, Paraná, Rondônia, and Pernambuco - totaling eight Brazilian cities. The objective of this project is to evaluate the health and well-being of adolescents aged between 13 and 15 enrolled in the country's state education system, investigating the differences concerning to sex, regions of each city, and regions of the country. Because this was an initial study using the HBSC questionnaire and methodology, we chose to withdraw the 11-year age group. The estimated sample of the study is 3,000 individuals. The Brazilian insertion counted on the advice of a Portuguese team working in the area. The protocol used in the 2014 survey (Matos, Simões, Camacho, Reis, & Equipa Aventura Social, 2015) was granted by the Portuguese language research team so that the Brazilian translation and adaptation could be carried out.
The adaptation of an existing international instrument was chosen considering the scope and relevance of the HBSC study, as well as the possibility of comparing samples with different participating countries. The importance of linguistic translation combined with cultural adaptation in the cross-cultural work of adapting self-applied tools in health is well established in the literature (Beaton, Bombardier, Guillemin, & Ferraz, 2000). According to the review by Manzi-Oliveira, Balarini, Marques, and Pasian (2011), the adaptation of instruments is justified by the resources saved and the gains from the comparison of results with international samples. The objective of this study was to demonstrate the translation and cultural and linguistic adaptation process carried out by the center responsible for this study, unpublished in Brazil.
2. Method
2.1 Instrument Research and Translation Procedures
The translation and linguistic adaptation process of the instrument were carried out in two stages. The first stage was related to the translation of the instrument into Brazilian Portuguese by three experts in the area of Psychology and its respective evaluation by a committee. For translation and adaptation, the Portuguese and English versions of the instrument were used. The second stage involved linguistic analysis and the initial evaluation of the protocol, and it included two phases: the first was a linguistic comprehension study, and the second was a pilot study for the sake of initial evaluation.
The stages of the linguistic and cultural translation and adaptation process were based on the work by Borsa, Damásio, and Bandeira (2012), except for the reverse translation. The back-translation was considered unnecessary, as one of the original versions was in Portuguese spoken in Portugal. The HBSC 2013/2014 protocol was translated and adapted to Brazilian Portuguese, based on the Portuguese version of 2013/2014 (Matos et al., 2015) and the English version of 2009/2010 (Currie et al., 2012). Figure 2.1.1 displays a schematic representation of the adaptation process in question, based on the methodological scheme of Borsa et al. (2012).

Following the recommendations in Manzi-Oliveira et al. (2011), three experts in the areas translated and adapted the protocol conceptually. Each judge produced a translated version, which was forwarded for further synthesis by the evaluation committee (Beaton et al., 2000). The committee decided on the final version of the protocol following the recommendations and items in the English language of the HBSC-WHO research protocol 2009/2010 (Griebler et al., 2010).
After the approval of the synthesis, the instrument layout was adapted according to the Portuguese questionnaire. The second step of the method was to verify the comprehension of the instructions, items, and answers (Borsa et al., 2012). The evaluation method was qualitative, based on aspects reported by the study participants during the collection and individual inquiry at the end of the application.
Four girls participated in the first phase of the linguistic assessment of the instrument. The data collection took place in a private room indicated by the school, coordinated by a postdoctoral student and a scientific initiation student of the project. The participants were instructed to read carefully and ask questions to the coordinators in case of comprehension difficulties, problems with the layout or errors. It was also highlighted that there were no right or wrong answers. At the end, participants were asked questions individually about the instrument.
The second phase of the linguistic assessment was carried out through a pilot study (Borsa et al., 2012). Eleven boys and eight girls participated in this stage, coming from another school in the region that was also contacted randomly. The collection took place in a location designated by the school, with the same coordinators. After the application, an individual interview was conducted to explore the items of the questionnaire and the corresponding answers, thus guaranteeing the equivalence of the instrument (Beaton et al., 2000). It was also evaluated if the instruction of the procedure and the layout were appropriate.
All the participants in the survey received authorizations from parents or guardians through the signing of the Informed Consent Term (TCLE). Also, participants signed, at the time of data collection, the Term of Assent (TA) to participate in the research. All participants were initially asked if they had any difficulty and demonstrated proper reading and writing skills.
2.2 Participants
Three Brazilian experts holding a Ph.D. in psychology and knowledgeable in the research areas took part in the translation and adaptation of the instrument to Brazilian Portuguese. All were Brazilian nationals and native Portuguese speakers, besides understanding and speaking the English language satisfactorily. An evaluation committee analyzed the initial translation, including the coordinator of the study, one of the translators and a health professional.
A group of four girls did the initial linguistic analysis of the translated instrument with a mean age of 13.50 years old (SD = 0.30). In the second step of this phase, the instrument was applied to 18 adolescents, being 44.44% female (n = 8), mean age 13.69 years old (SD = 0.35). When adding up the participants in the two phases, 22 adolescents took part in the linguistic assessment of the translated and adapted protocol, being 54.50% female (n = 12), 13 years old with an average of 13.50 years old (SD = 0.30). The participants were enrolled in the 8th grade in two state schools in a city in the countryside of São Paulo.
2.3 Instrument
HBSC Protocol 2013/2014: The HBSC started to develop the questionnaire in cooperation with WHO in 1982. Since then, it has been assessed continuously on the occasion of each survey. The most recent questionnaire was applied in 2013/2014 in more than 42 European and North American countries.
The instrument evaluates indicators and behaviours related to health and well-being, lifestyle, and social context variables in adolescents of 11, 13, and 15 years of age. It contains approximately 80 closed questions, but each country is allowed to include questions. The 16 thematic axes of the questions are: sociodemographic factors, food, oral hygiene, Body Mass Index, diet, substance use, school, satisfaction and quality of life, physical and psychological well-being, physical activity, sexual behaviour, provocation, injuries, family relationships, peers, free time and communication through electronic media. The instrument is self-applied and can be administered on paper or digitally. It takes approximately 40 minutes to complete.
2.4 Data analysis
The Brazilian research committee analyzed the translations made by the judges. The research authors analyzed all the information concerning the intelligibility of items and language appropriateness to the target population.
3. Results
3.1 Translation and adaptation of the HBSC Protocol
The committee defined the final version of the Brazilian version of the HBSC protocol. Concerning the original versions, three items referring to the self-declared color (based on the census of the Brazilian Institute of Geography and Statistics, IBGE), parental supervision, and self-harm were included (based on non-mandatory HBSC Protocol items included in the Portuguese HBSC protocol of 2013/2014). The judges and the committee also analyzed these items.
Table 3.1.1 presents the main translation divergences and adaptation of concepts from the questionnaire to the Brazilian reality among the judges. Based on the version of each judge, fifteen words were adapted to Portuguese and to the Brazilian reality, the synthesis being at the discretion of the evaluation committee.
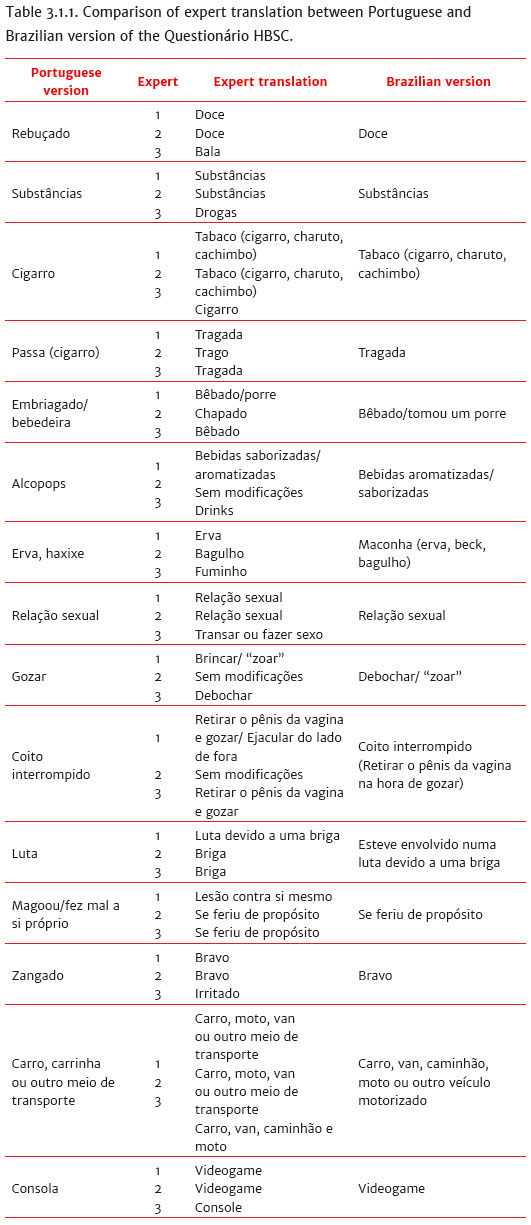
Some terms were adapted from expressions commonly used in the Brazilian adolescent reality, such as the synonyms for marijuana, drunkenness, and jeers/curses among peers, based on the judges' expertise in the area. At the end, the Brazilian version was concluded, integrated into the instrument and evaluated satisfactorily by the participants.
3.2 Linguistic evaluation of the HBSC Protocol
No participant reported comprehension difficulties during or after the application of the questionnaire. The adolescents also quickly understood the layout of the presentation and evaluated the application instructions as clear. Based on the qualitative analyses, the semantic, idiomatic, experiential, and conceptual equivalence (Manzi-Oliveira et al., 2011) of the questionnaire was reached through the participants' verbal evaluation of their understanding of the instrument and later when the answers to the questions were verified. No participant reported comprehension difficulties during or after the application in the two phases of the process. The validation of the instrument went beyond the objectives of this study.
The phases executed to evaluate the translation demonstrated the satisfactory understanding of the questionnaire's target audience for which the questionnaire is intended. The target audience assessed the synthesis and observed no difficulty during the application. The understanding of the instrument was also observed, as no adolescent reported any incomprehension or difficulty. In the pilot study, again, despite repeated requests, no difficulties were found, nor suggestions were made regarding the instructions, items, responses, and layout of the instrument. The study sample also understood the items appropriately added.
4. Discussion
Although there is no consensus on the instrument adaptation methodology, this process certainly goes beyond mere translation and requires methodological rigor to guarantee the reliability and validity of measures and constructs (Borsa et al., 2012). This study aimed to recognize the Brazilian adaptation of the adolescent health questionnaire Health Behaviour in School-aged Children and to demonstrate the translation and adaptation processes of the instrument. All steps followed the recommendations described in the literature (Borsa et al., 2012; Beaton et al., 2000; Manzi-Oliveira et al., 2011). No difficulties were found as described by Asian researchers (Smet, Maes, Clercq, Haryanti, & Winarno, 1999) regarding the translation and adaptation of the questionnaire in a developing country, where adjustments were required in questions related to the diet and foods consumed, for example, also citing the influence of notable cultural and religious issues in this process, as in the evaluation of sexual behaviours. The questionnaire derived from this study can be considered suitable for use in Brazilian studies that evaluate the subject matter within the age group represented.
The importance of research on adolescent health is evident in the specific literature. Several Brazilian studies have investigated health indicators and behaviours in this age group in their different settings and contexts (Braz et al., 2013, Reis et al., 2013, Sousa et al., 2010), even in extensive national surveys (Carlini et al., 2010; IBGE, 2016). What distinguishes the HBSC questionnaire, however, is the range of concepts investigated in a single instrument - covering 16 health spheres - its validation in more than 40 countries involving more than 220 thousand adolescents and the consolidation as an international task force, thus permitting the transnational comparison of the data. Inserting Brazil in the HBSC taskforce will permit the development of the study in the country and the consolidation of the instrument, with the subsequent goal of integration in international surveys, highlighting the importance of a proper adaptation of the instrument in question.
The main limitation of the study refers to the fact that the HBSC Brasil questionnaire has not been validated, which is complementary to the adaptation of the instrument. The compliance with guidelines that guarantee the quality of the adaptation process is highlighted, such as methodological controls regarding the choice and the criteria for the selection of the judges, a detailed description of the method and formal authorization and assistance from the country of origin for the instrument used (Borsa et al., 2012; Manzi-Oliveira et al., 2011). The validation will be one step further after the objectives of this national project that has been developed in the country. In conclusion, the HBSC protocol was translated and adapted to the Brazilian reality satisfactorily, resulting in the questionnaire HBSC Brasil 2016/17.
References
Beaton, D. E., Bombardier, C., Guillemin, F., & Ferraz, M. B. (2000). Guidelines for the process of cross-cultural adaptation of self-report measures. Spine, 25(24),3186-3191. [ Links ]
Borsa, J. C., Damásio, B. F., & Bandeira, D. R. (2012). Adaptação e validação de instrumentos psicológicos entre culturas: Algumas considerações. Paidéia, 22(53),423-432. doi:10.1590/1982-43272253201314 [ Links ]
Bower, J. M., Carroll, A., & Ashman, A. F. (2012). Adolescent perspectives on schooling experiences: The interplay of risk and protective factors within their lives. International Journal of Educational Research, 53,9-21. doi:10.1016/j.ijer.2011.12.003 [ Links ]
Brasil (1990). Estatuto da Criança e do Adolescente (ECA). Câmera dos Deputados, Lei n. 8.069, de 13 de julho de 1990. DOU de 16 jul. 1990. Brasília: DF. [ Links ]
Braz, M., Barros, A. A. B., Filho, & Barros, M. B. A. (2013). Saúde dos adolescentes: Um estudo de base populacional em Campinas, São Paulo, Brasil. Cadernos de Saúde Pública, 29(9),1877-1888. doi:10.1590/0102-311X00169712 [ Links ]
Carlini, E. A., Noto, A. R., Sanchez, Z. M., Carlini, C. M. A., Locatelli, D. P., Abeid, L. R., ... Moura, Y. G. (2010). VI Levantamento Nacional sobre o Consumo de Drogas Psicotrópicas entre Estudantes do Ensino Fundamental e Médio das Redes Pública e Privada de Ensino nas 27 Capitais Brasileiras. São Paulo: Centro Brasileiro de Informações sobre Drogas Psicotrópicas, Universidade Federal de São Paulo. [ Links ]
Currie, C., Gabhainn, S. N., Godeau, E., & International HBSC Network Coordinating Committee (2009). The Health Behaviour in School-aged Children: WHO Collaborative Cross-National (HBSC) Study: Origins, concept, history and development 1982-2008. International Journal of Public Health, 54,131-139. doi:10.1007/s00038-009-5404-x [ Links ]
Currie, C., Zanotti, C., Morgan, A., Currie, D., Looze, M., Roberts, C., ... Barnekow, V. (Eds.). (2012). Social determinants of health and well-being among young people. Health Behaviour in School-aged Children (HBSC) study: International report from the 2009/2010 survey. (Health policy for children and adolescents, n. 6). Copenhagen: WHO Regional Office for Europe. [ Links ]
Griebler, R., Molcho, M., Samdal, O., Inchley, J., Dur, W., & Currie, C. (Eds.) (2010). Health Behaviour in School-aged Children: a World Health Organization cross-national study, Research Protocol for the 2009/2010 survey. Vienna: LBIHPR; Edinburg: CAHRU. [ Links ]
Hallal, P. C., Victoria, C. G., Azevedo, M. R., & Wells, J. C. K. (2006). Adolescent physical activity and health. A systematic review. Sports Medicine, 36(12),1019-1030. [ Links ]
Inchley, J., Currie, D., Young, T., Samdal, O., Torsheim, T., Augustson, L., ... Barnekow, V. (Eds.). (2016). Growing up unequal: gender and socioeconomic differences in young people's health and well-being. Health Behaviour in School-aged Children (HBSC) study: International report from the 2013/2014 survey. (Health policy for children and adolescents, n. 7). Copenhagen, WHO Regional Office for Europe. [ Links ]
Instituto Brasileiro de Geografia e Estatística (2016). Pesquisa Nacional de Saúde do Escolar (PeNSE): 2015. Retrieved from www.ibge.gov.br/home/estatistica/populacao/pense/2015/ [ Links ]
Lansford, J. E., Dodge, K. A., Fontaine, R. G., Bates, J. E., & Pettit, G. S. (2014). Peer rejection, affiliation with deviant peers, delinquency, and risky sexual behavior. Journal of Youth and Adolescence, 43,1742-1751. doi:10.1007/s10964-014-0175-y [ Links ]
Manzi-Oliveira, A. B., Balarini, F. B., Marques, L. A. da S., & Pasian, S. R. (2011). Adaptação transcultural de instrumentos de avaliação psicológica: Levantamento dos estudos realizados no Brasil de 2000 a 2010. Psico-USF, 16(3),367-381. [ Links ]
Matos, G. M., Simões, C., Camacho, I., Reis, M., & Equipa Aventura Social (2015). A saúde dos adolescentes portugueses em tempos de recessão - dados nacionais do estudo HBSC de 2014. Lisboa: Centro de Malária e Outras Doenças Tropicais, IHMT, UNL. [ Links ]
Papalia, D. E., Olds, S. W., & Feldman, R. D. (2010). Desenvolvimento humano (10a ed.). Porto Alegre: Artmed. [ Links ]
Reis, D. C., Almeida, T. A. C., Miranda, M. M., Alves, R. H., & Madeira, A. M. F. (2013). Vulnerabilidades à saúde na adolescência: Condições socioeconômicas, redes sociais, drogas e violência. Revista Latino-Americana de enfermagem, 21(2),1-9. [ Links ]
Romer, D., Reyna, V. F., & Satterthwaite, T. D. (2017). Beyond stereotypes of adolescent risk taking: Placing the adolescent brain in developmental context. Developmental Cognitive Neuroscience, 27,19-34. doi:10.1016/j.dcn.2017.07.007 [ Links ]
Schneider, B. C., Dumith, S. C., Orlandi, S. P., & Assunção, M. C. F. (2017). Diet and body fat in adolescence and early adulthood: A systematic review of longitudinal studies. Ciência e Saúde Coletiva, 25(5),1539-1552. doi:10.1590/141381232017225.13972015 [ Links ]
Smet, B., Maes, L., Clercq, L., Haryanti, K., & Winarno, R. D. (1999). The Health Behavior in School-Aged Children study in Semarang, Indonesia: methodological problems in cross-cultural research. Health Promotion International, 14(1),7-16. doi:doi. org/10.1093/heapro/14.1.7 [ Links ]
Sousa, T. F., Silva, K. S., Garcia, L. M., Del Duca, G. F., Oliveira, E. S. A., & Nahas, M. V. (2010). Autoavaliação de saúde e fatores associados em adolescentes do Estado de Santa Catarina, Brasil. Revista Paulista de Pediatria, 28(4),333-339. [ Links ]
World Health Organization (2011). Preventing early pregnancy and poorreproductive outcomes: Among adolescents in developing countries. Geneva: WHO. Retrieved from http://whqlibdoc.who.int/publications/2011/9789241502214_eng.pdf?ua=1 [ Links ]
Word Health Organization (2014). Health for the World's Adolescents. A second chance in the second decade. Geneva: WHO. Retrieved from http://apps.who.int/iris/bitstream/10665/112750/1/WHO_FWC_MCA_14.05_eng.pdf?ua=1 [ Links ]
 Mailling address:
Mailling address:
Juliana Maltoni
Av. Bandeirantes, 3900, Monte Alegre
Ribeirão Preto, SP, Brazil. CEP 14040-901
E-mail: julianamaltoni@gmail.com
Submission: 02/05/2019
Acceptance: 03/06/2019

