










Serviços Personalizados
Journal

artigo
 Inglês (pdf)
Inglês (pdf)
 Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
 Curriculum ScienTI
Curriculum ScienTIIndicadores
Compartilhar

 Permalink
PermalinkSMAD. Revista eletrônica saúde mental álcool e drogas
versão On-line ISSN 1806-6976
SMAD, Rev. Eletrônica Saúde Mental Álcool Drog. (Ed. port.) vol.11 no.2 Ribeirão Preto jun. 2015
Suicide risk in cocaine addicts with a current depressive episode: feelings and experiences
Caroline Neubüser RochaI; Daniélle Bernardi SilveiraII; Roger Santos CamargoIII; Simone FernandesIV; Maristela FerigoloV; Helena Maria Tannhauser BarrosVI
IPsychologist, Trainee, Universidade Federal de Ciências da Saúde, Porto Alegre, RS, Brazil
IIMaster's Student, Universidade Federal de Ciências da Saúde de Porto Alegre, Porto Alegre, RS, Brazil
IIIMSc, Biologist, Universidade Federal de Ciências da Saúde de Porto Alegre, Porto Alegre, RS, Brazil
IVPhD, Psyschologist, Universidade Federal de Ciências da Saúde de Porto Alegre, Porto Alegre, RS, Brazil. Profesor, Universidade Federal de Ciências da Saúde de Porto Alegre, Porto Alegre, RS, Brazil
VPhD, Professor, Universidade Federal de Ciências da Saúde de Porto Alegre, Porto Alegre, RS, Brazil
VIPhD, Full Professor, Universidade Federal de Ciências da Saúde de Porto Alegre, Porto Alegre, RS, Brazil
ABSTRACT
Death by suicide is now the third most frequent cause of death in the population 15-44 years old. This self-inflicted death has meaning that requires understanding and attention. The objective of this study was to understand the experiences and feelings of cocaine users within the relationship of addiction and suicide. This is a qualitative study conducted from August 2012 to February 2013. The 18 individuals who met criteria for a depressive episode responded to the semi-structured interview for suicide risk, the Mini International Neuropsychiatric Interview. During the analysis of the narrated content, there were three categories established: previous history, previous suicide attempts, and depression. The results were evaluated seeking to reflect and understand the experiences exposed by users. This study helps to understand the meaning of the experiences and feelings of crack/cocaine users who are at the risk for suicide.
Descriptors: Substance-Related Disorders; Suicide; Depression.
Introduction
In 2000, approximately one million people died by suicide, with a global rate of 16 deaths per 100 thousand inhabitants, which represents one death every 40 seconds(1). Suicide is among the three leading causes of death in the population between 15 and 44 years, with self-inflicted violence present in almost all countries(2).
In Brazil, suicide rates have increased 21% in a span of 20 years(2). Within the population 15-44 years, injury or trauma resulting from suicide attempts are the sixth leading causes of health problems and physical disability(3). Furthermore, with regards to depression, suicide and suicide attempts are symptoms of relapse(4).
Suicide is not an act with mechanisms well understood, it is difficult to understand how someone conceives and/or plans his own death, chooses a method he will use, and puts it into practice(5). Families who reported relatives who committed suicide had depression, drug abuse and disturbing feelings(6). Qualitative studies help to understand this kind of experience and its associated meanings(7). In addition, the personal conversation leads to the possibility of recognizing, in the history of individual, perceptions of their experiences, whereas users with suicidal behavior tend to seek help before they die(5-7).
Given the importance of the subject, there is still little studied by the scientific community(8), we sought to know the experiences and feelings of crack/cocaine users in the relationship of addiction and suicide.
Method
We conducted a qualitative study, based on a textual analysis of semi-structured interviews. Content analysis was based on the most reported user's experiences. These were: a previous history, previous suicide attempt and depression. The interview aimed to encourage the respondent to examine the subject of addiction and suicide, understand the purpose of the research, and be comforted with rapport (empathy). Theoretical saturation, from the reports, was made by a continuous process of data analysis that started at the beginning of the collection process. The interviews described and selected were subjected to content analysis(9).
The study was conducted in a call center LIGUE 132 (the National Guidance and Information on Drug Abuse Prevention), based in Porto Alegre, RS. The telephone answering service is open to the public and provides guidance and information about drugs, free of charge and offers confidentially by telephone and monitoring for drug users(10). The service is in partnership with the Federal Government, through the National Secretary on Drug Policy, the Ministry of Justice and the Federal University of Health Sciences of Porto Alegre.
All service calls are made exclusively by telephonic means. The recruitment of the patients in this study was selected from the call center LIGUE 132. A phone call was made to 330 individuals who had made their first and only contact with the service about crack/cocaine. Inclusion criteria were: 18 years old, had called between the period between August 2012 and February 2013, and on the second contact agreed to participate in research about a depressive episode and risk of suicide. The Mini International Neuropsychiatric Interview scale was applied – the Brazilian version 5.0.0 (MINI), for the assessment of a current depressive episode and if there was a depressive episode, the scale for risk of suicide. We made three attempts to contact the individuals and if there were no success they were excluded. The data collected and the demographic information of users had been written down by attendants and sent to a specific software service(10), and subsequently transferred to a research database. At the end of the study, 18-contacted individuals were recorded. Users were from different regions of the country, due to the nationwide service.
During the semi-structured interview, the first call, we used the Substance Abuse and Mental Health Services Administration (SAMSHA) questionnaire(11), for drug addiction of crack/cocaine, on the last contact, we used the MINI for assessment if suicide risk and a current depressive episode. The SAMSHA is based on 6 of the 7 existing items in the DSM-IVTR for chemical dependency, and the individual is considered dependent if they respond affirmatively to at least 2 of the questionnaire criteria.
The MINI is a structured interview with an axis of I of the DSM IV and of the 10th revision of the International Classification of Diseases (ICD-10). For a current depressive episode, the questionnaire contains 11 questions, with yes or no answer options. The interview involves feelings of sadness, guilt, changes in appetite and physical disposition, seen in the last two weeks. The risk of suicide may be risk-free, mild, moderate or severe(10). Each affirmative score adds to the identification of the degree of risk. In this questionnaire, the following questions were added: Do you want to harm yourself? How? Have you thought of a way to commit suicide? In what way? Did you attempt suicide? How old? Have you ever attempted suicide? How? How many times?
To participate in the study, there was information about the objectives given to participants as well as a verbal consent. Participants with suicide risk were advised to seek help from a health professional and we made a No Suicide Contract (NSC)(11). Interviewers CMR and DBS were graduate students in the health field, with training in drug abuse and brief motivational intervention(10). The study was approved by the Ethics Committee of the Federal University of Health Sciences of Porto Alegre (FUHSPA), through the Addendum 1812/12.
Results and dicussion
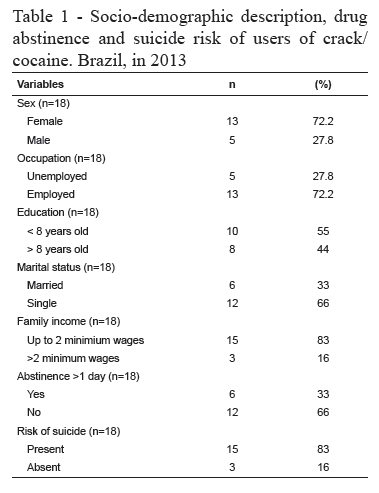
Table 1 shows the demographic data, drug abstinence and suicide risk of those involved in the study. The average age of users was 30.7 years with a standard deviation of 6.83. To maintain the confidentiality of respondents, their names were identified with their initials.
Previous history
The subject AJ (high suicide risk) had severe violence reports and childhood sexual abuse, a factor that is consistent with what the literature focuses on in relation to previous history of traumas. There are more suicide attempts in individuals who had experiences of negligence and a dysfunctional family environment (substance abuse, mental illness or suicide, exposure to domestic violence, arrest of a family member and divorce or parental separation) (14).
A history of family members who attempted or committed suicide is an aggravating factor for suicidal behavior, and also, suicide attempts may be a result from family conflicts with emotional disorders such as difficulty in social adaptation and interpersonal relations(5). The case of BC (high suicide risk) represented this context, having in his family a maternal aunt who had attempted suicide with a firearm when he was 10.
The mother of the patient DE (high suicide risk) attended a psychiatric care facility and was taking medications to sleep. As a child he witnessed the physical abuse of the father against the mother, confirming a fragile household situation. The father of this client had died shortly before the date of the telephone contact. It is noteworthy, therefore, that the mourning period is a critical time that requires attention from professionals who assist users. The case of EF (high suicide risk) showed that his companion had passed away seven months ago. The main protective factor against suicide attempts are satisfaction with family relationships and self-esteem(15).
With respect to crack/cocaine, those who had parental neglect and poor perception of their paternity demonstrated significantly higher levels of depression and aggression, which can put them at a greater risk of self-harm, compared with those who reported a caring family(16).
FK (high suicide risk) and HC (moderate suicide risk) reported being victims of sexual violence during childhood, but did not wish to talk about it. The patient HC had a father with a history of suicidal behavior. The risk of suicide may be compounded when one experiences a history of suicide, because this can become a learned behavior as conflict resolution(17). In another case, AJ suffered attempted sexual abuse at 11 years old (he said the abuser was killed from shots due to drug debts). He never told anyone about the violence inflicted, and declared that he was caught up in a lot of violence.
Previous suicide attempts
The fear of disappointing parents is the case for BC; suffering for not being able to meet the expectations of the people who love him made him feel worthless. He decided to end his life to free his parents of concerns about the use of cocaine. I have already attempted suicide several times, I lost count: with knives, with rat poisin, and others (BC). Talking about suicide gives the opportunity for the individual to talk about their suffering and think about it(18). I have never had a conversation with anyone about my attitudes (BC). AJ first spoke about suicide with someone. It was much easier to talk over the phone (FK).
The patient FK was hospitalized seven times. I took many medications and was asleep a long time sleeping and not nearly as (...) when I always talk to health professionals about my bad thoughts they hospitalize me, so I don't talk to them anymore (FK). Between 15 and 25% of subjects who attempt suicide have a repeated attempt, and 10% take their life in the following years(18). The interviewee FK attempted suicide three times. The first time she took all the medications that were available, two months ago the interviewee had cut her wrists, and on the last attempt, tried to hang herself on her birthday. If I had achieved it, it would be better. I feel ashamed for not having...earlier this month I got my salary and I'm going to send my daughter to her father in another state, I will lock myself in the house and shoot myself in the heart. I have a friend that sells weapons, but did not tell him anything. It's no fun to live (FK).
The client JT (light suicide risk) tried to hang up, during the call, he thought about suicide, again, but this time with a gun to shoot himself in the head. AJ also already reported his history of suicide attempts. The first time he slashed his wrists, in another attempt took twenty anxiolytic tablets (diazepam); during his last attempt he used cocaine and overdosed. If you knew you would not go to hell then it would already been done...I thought about killing all my family and then myself (JT).
The respondents EF and DE reported attempts on their life on three occasions, among them as with drug intoxication and wrist cutting. The client DE reported I get mad when I use crack (DE) and killed two people. He declared that these thoughts plagued him and because of this, a knife was always at the door; this is the same instrument that he plans on using to self-destruct, and always carries it around his waist.
Drugs, depression and suicide
Psychiatric disorders are closely linked to suicides, with a strong association with depression(19). Alcohol and crack/cocaine is related to suicide attempts, with an increase of depressive symptoms and impulsivity20-21). Impulsivity with the use of alcohol has shown evidenced in the relationship of use with depressive symptoms and suicidality. The patient AJ used crack, cocaine, and alcohol weekly and marijuana daily when he sought the support service. When I get home I'm in my room crying a lot. I do not let my saddness transpire (AJ). He is a watchman and works at night alone and armed, even after not passing psychometric testing through the company. He already attempted suicide three times. The client took many non-prescription drugs, including an antidepressant.
The user FK was retired by a depressive disorder; taking, among others, psychiatric drugs, antidepressants for 4 years. The use of antidepressants, which do not reach therapeutic success, show a greater relationship between suicide and the use of drugs(20).
The patient HC at the time of data collection, used alcohol, tobacco, marijuana and cocaine daily, and the consumption of lysergic acid diethylamide (LSD), weekly. Note the concomitant use with drugs that alter the central nervous system, such as alprazolam (benzodiazepine), bupropion hydrochloride (antidepressant) and risperidone (antipsychotic). He reported that 2 years ago he sought help from a psychiatrist because of depression and began treatment with medications. The use of psychoactive substances is often used as self-medication for depression, because this substance releases dopamine in the central nervous system(23).
The client described to dream constantly with the use of drugs, and that it generated feelings of anger. The user did not appear to display resolution of their problems, a characteristic symptom of a possible depression. Recurrent depression is a serious public health problem, and it is a challenge to treat patients who do not respond to antidepressants(24).
The client EF has accepted the help to stop alcohol and cocaine, which she used weekly for 2 years. Her husband died after 7 months together and she was 5 months pregnant. She had two years of counseling for depression, and homeopathic treatment, and had already attempted suicide three times. The duration of treatment for depression coincides with the time of alcohol and cocaine use, and probably interfered with treatment efficacy. Interestingly, the client said she never talked about her suicidal thoughts.
It is known that there are biological and social factors inherent that predispose females to increased risk of depression(25). The client also reported moments of weeping and sorrow, which are important symptoms that are often raised in studies about the differences in gender, for depression.
JR used crack, alcohol, tobacco and marijuana. The patient reported a family environment in which drug use is common. He used crack with his brother, and also sought to motivate him to stop. His mother died when he was 14. He says that because of having to play an important role for his brothers and the depression, he started using marijuana. His brother became a dealer and sister a crack user. The client JT tried the intentional death by hanging on a tree, his words about the incident were: Symptom post-use. Depression of use (JT). During the conversation, he said he had serious problems with his wife because of their consumption, and that in a fight, she broke a mirror on the back of his neck. He was treated for depression for 2 years, but said he was depressed and did not believe the words of a psychologist could help; he did not believe in it or anyone. When he is home he is in the room and cries a lot. I am crying at anything. I do not want to have a conversation with anyone (JT).
Final Considerations
Given the reports described by the individuals, we observed the complexity of the relationship of comorbid depression, substance abuse and suicidal ideas, and how they can generate suffering. Words such as "sadness", "death" and "pain" refer to representation and humanization of experience that some of the users were experiencing, regardless of whether or not they were abstinent from crack/cocaine.
The knowledge of the feelings and experiences of the patients and their perception of suicide can translate to professionals the gravity of the situation, which can be confirmed with results of specific questionnaires, such as the MINI. These reported personal stories expose the attention that is needed to understand the unique experiences of crack/cocaine users and realize the possibility for suicide risk. In addition, further studies are needed to know the significance of the experiences and feelings of these patients in clinical practice, in order to increase the chances of approach in the patient/professional relationship and possible suicide prevention.
References
1. Organização Mundial da Saúde (OMS). Prevenção do Suicídio: um manual para profissionais de saúde em atenção primária [Internet]. Genebra: OMS; 2000 [acesso 17 mar 2013]. Disponível em: http://www.who.int/mental_health/prevention/suicide/en/suicideprev_phc_port.pdf. [ Links ]
2. Bertolote JM, Mello-Santos CD, Botega NJ. Detecting suicide risk at psychiatric emergency services. Rev Bras Psiquiatr. 2010;32(2):87-95. [ Links ]
3. Peuker AC, Rosemberg R, Cunha SM, Araújo LB. Fatores associados ao abuso de drogas em uma população clínica. Paidéia (Ribeirão Preto). 2010;20(46):165-73. [ Links ]
4. Schmitt A, Falkai P. Suicide ideation, stability of symptoms and effects of aerobic exercise in major depression. Eur Arch Psychiatry Clin Neurosci. 2014 Oct;264(7):555-6. doi: 10.1007/s00406-014-0526-4. [ Links ]
5. Abreu KP, Lima MAD, Kohlrausch E, Soares JF. Comportamento suicida: fatores de risco e intervenções preventivas. Rev Eletr Enferm. [Internet]. 2010 [acesso 14 dez 2012];12(1):195-200. Disponível em: http://www.fen.ufg.br/fen_revista/v12/n1/pdf/v12n1a24.pdf [ Links ]
6. Sousa GS, Silva RM, Figueiredo AEB, Minayo MCS, Vieira LJES. Circunstâncias que envolvem o suicídio de pessoas idosas. Interface - Comunicação, Saúde, Educação. 2014;18(49):389-402. [ Links ]
7. Lakeman R. What can qualitative research tell us about helping a person who is suicidal? Nurs Times. 2010;24-30;106(33):23-6. [ Links ]
8. Andrade TM. Reflexões sobre Políticas de Drogas no Brasil. Ci Saúde Coletiva. 2011;16(12):4665-74. [ Links ]
9. Bardin L. Análise de conteúdo. 6 ed. Lisboa: Edições 70; 2011. 280 p. [ Links ]
10. Barros HM, Santos V, Mazoni C, Dantas DC, Ferigolo M. Neuroscience education for health profession undergraduates in a call-center for drug abuse prevention. Drug Alcohol Depend. 2008;98:270-4. [ Links ]
11. SAMSHA. Synar Regulation Implementation: Report to Congress on FFY 97 State Compliance. Rockville (MD): Center for Substance Abuse Prevention; 1998. [ Links ]
12. Amorin P. Mini International Neuropsychiatric Interview (MINI): validação de
entrevista breve para diagnóstico de transtornos mentais. Rev Bras Psiquiatr. 2000;22:106-15.
13. Howe E. Ethical Considerations When Making Exceptions to "Rules" in Psychiatry. Innov Clin Neurosci. 2014 Jan-Feb;11(1-2):32–8. [ Links ]
14. Silva S, Maia AC. Experiências adversas na infância e tentativas de suicídio em adultos com obesidade mórbida. Rev Psiquiatr Rio Gd Sul. 2010;32(3):69-72. [ Links ]
15. Braga LL, Dell'Aglio DD. Suicídio na adolescência: fatores de risco, depressão e gênero. Contextos Clín. [Internet]. 2013 [acesso 15 nov 2014];6(1):2-14. Disponível em: http://revistas.unisinos.br/index.php/contextosclinicos/article/view/ctc.2013.61.01/1533. [ Links ]
16. Gerra G, Leonardi C, Cortese E, Zaimovic A, Dell'Agnello G, Manfredini M, et al. Childhood neglect and parental care perception in cocaine addicts: Relation with psychiatric symptoms and biological correlates. Neurosci Biobehav Rev. 2009;33(4):601–10. [ Links ]
17. Werlang BG, Botega NJ. Comportamento Suicida. Porto Alegre: Artmed Editora; 2004. 204 p. [ Links ]
18. Barbosa FO, Macedo PCM, Silveira RMC. Depressão e o suícido. Rev SBPH. [Internet]. 2011 [acesso 19 nov 2013];14(1):233-43. Disponível em: http://pepsic.bvsalud.org/scielo.php?script=sci_arttext&pid=S1516-08582011000100013&lng=pt. [ Links ]
19. Gagné P, Moamai J, Bourget D. Psychopathology and Suicide among Quebec Physicians: A Nested Case Control Study. Depress Res Treat. [Internet]. 2011 Jul [acesso 19 set 2013]; 2011 Article ID 936327. Disponível em: http://www.hindawi.com/journals/drt/2011/936327/http://dx.doi.org/10.1155/2011/936327 [ Links ]
20. Conner KR, Houston RJ, Swogger MT, Conwell Y, You S, He H, et al. Stressful life events and suicidal behavior in adults with alcohol use disorders: Role of event severity, timing, and type. Drug Alcohol Depend. 2012;120(1-3):155–61. [ Links ]
21. Winhusen TM, Somoza EC, Lewis DF, Kropp FB, Horigian VE, Adinoffd B. Frontal Systems Deficits in Stimulant-Dependent Patients: Evidence of Pre-illness Dysfunction and Relationship to Treatment Response. Drug Alcohol Depend. 2013;127(1-3):94–100. [ Links ]
22. Vento AE, Schifano F, Corkery JM, Pompili M, Innamorati M, Girardi P, et al.
Suicide verdicts as opposed to accidental deaths in substance-related fatalities (UK, 2001-2007). Prog Neuropsychopharmacol Biol Psychiatry. 2011;1;35(5):1279-83.
23. Khantzian EJ. Addiction as a self-regulation disorder and the role of self-medication. Addiction. 2013;108(4):668-9. [ Links ]
24. Plewnia C, Padberg F. Transkranielle und invasive Hirnstimulationsverfahren bei Depression. Der Nervenarzt. 2012;83(8):1006-12. [ Links ]
25. Parker G, Fletcher K, Paterson A, Anderson J, Hong M. Gender differences in depression severity and symptoms across depressive sub-types. J Affect Disord. 2014 Oct;167:351-7. doi: 10.1016/j.jad.2014.06.018. Epub 2014 Jun 19. [ Links ]
![]() Correspondence
Correspondence
Helena Maria Tannhauser Barros
Universidade Federal de Ciências da Saúde de Porto Alegre
Rua Sarmento Leite, 245
CEP: 90050-170, Porto Alegre, RS, Brasil
E-mail: helenbar@ufcspa.edu.br
Received: Apr. 28th 2014
Accepted: Feb. 11th 2015
