











 (pdf)
(pdf)




 Permalink
PermalinkJournal of Human Growth and Development
ISSN 0104-1282 ISSN 2175-3598
J. Hum. Growth Dev. vol.30 no.1 São Paulo jan./abr. 2020
https://doi.org/10.7322/jhgd.v30.9960
ORIGINAL ARTICLE
Evaluation of growth and nutritional condition of children in Public Schools in Florianópolis, Santa Catarina, Brazil
Avaliação do crescimento e do estado nutricional de crianças em idade escolar em Escolas Públicas de Florianópolis, Santa Catarina, Brasil
Cícero Cruz MacêdoI,II; Claudio LeoneIII; Viviane Gabriela NascimentoIII; José Lucas Souza RamosIV; Jane Laner CardosoV; Debora A. Zambrano OleaV; Italla Maria Pinheiro BezerraII,VI,VII; Luiz Carlos de AbreuII,VII
IUniversidade Federal do Cariri, UFCA, Barbalha, CE, Brasil
IIPós-graduação, Pesquisa e Inovação, Centro Universitário Saúde ABC (CUSABC). ciceropediatra@hotmail.com
IIIDepartamento de Saúde Materno Infantil da Faculdade de Saúde Pública da Universidade de São Paulo. São Paulo (SP), Brasil. leone.claudio@gmail.com;
IVLaboratório de Escrita Científica. Escola Superior de Ciências da Santa Casa de Misericórdia de Vitória (EMESCAM) - Vitória (ES), Brasil; joselucas@usp.br;
VDepartamento de Saúde Pública da Universidade Federal de Santa Catarina (UFSC) - Florianópolis (SC), Brasil. jane.laner@hotmail.com;
VIBolsista CAPES Brasil
VIIPrograma de Pós-graduação em Políticas Públicas e Desenvolvimento Local, Escola Superior de Ciências da Santa Casa de Misericórdia de Vitória (EMESCAM) - Vitória, (ES), Brasil; italla.bezerra@emescam.br
ABSTRACT
INTRODUCTION: Obesity is becoming more and more frequent in children, which can result in health problems both in childhood and in adulthood. Considering that, at school age, eating habits may be influenced by the context in which the child is inserted, mainly, lifestyle, inside and outside the school environment, it is important to evaluate the growth achieved in height, as well as their nutritional status, since this can be an indication of future and possible nutritional disorders, allowing to direct resources and effective public policies in this age group
OBJECTIVE: Evaluate the growth in stature and nutritional condition of schoolchildren by gender and age in Florianopolis, Santa Catarina, Brazil, in the first semester of the 2012 school year
METHODS: A cross-sectional study was conducted with 595 children of six to ten years of age, through the marketing of Public Municipal Elementary Schools, in the city of Florianópolis, State of Santa Catarina, Brazil. The statistical analysis of the data was performed with the Statistical Package for the Social Science, version 20.0
RESULTS: It was assessed a larger proportion of children between seven and nine years of age, and both in relation to the stature as the Body Mass Index (BMI). The medians are higher when compared to the reference (World Health Organization), revealing that the children are growing well, even above the average for the benchmark. However, at the same time, they have a BMI higher than expected, even considering their high stature. The diagnosis of nutritional status among the boys and girls showed no statistical differences. However, it is worth highlighting that, although the bigger prevalence is eutrophic children (70.3%), a high prevalence of excess weight (overweight, obesity and severe obesity) can also be observed, around 28% of the sample
CONCLUSION: Although most children were found to be in normal nutritional condition, some were identified as being overweight or obese. It was evident that nutritional condition does not differ in relation to gender, but is influenced by age and height
Keywords: nutritional status, sex, Body Mass Index.
Authors summary
Why was this study done?
The period of growth from childhood to adolescence is fundamental for the development of human beings and their future physiological functions. Thus, monitoring the nutritional status at this stage is essential to take preventive and effective public health measures in order to avoid practices that do not promote health in this population, which is the justification for carrying out the study.
What did the researchers do and find?
A cross-sectional cohort study was carried out in public schools in Santa Catarina and it was found that the nutritional transition from malnutrition to eutrophy until then, is pointing to overweight and obesity.
What do these findings mean?
The results imply the need to reorient practices that promote healthy habits in this audience in order to avoid possible future complications.
INTRODUCTION
Obesity has become increasingly common in children, which may result in damages to health both in childhood and in adulthood1. Children in education are in the process of transition, in which they are constantly undergoing biopsychosocial changes that can lead to nutritional needs for different foods, which are not always considered healthy. The influence of the regular eating habits of parents, relatives, and friends can also lead to changes in behavior, which are directly involved in nutritional condition2,3.
In children in school stage, i.e. from six to ten years of age, overweight is the nutritional condition arising. In the past two decades, national surveys demonstrate that there was an increase in the prevalence of cases of overweight children, from 4.9% to 17.4% among children in this age group4. According to data from the Surveillance System of Food and Nutrition (SISVAN), cases of being overweight or obese correspond to a prevalence of 13.1%, and the risk of being overweight is 16.9%, while severe thinness and thinness are equivalent to approximately 4.5%5,6.
Occurrences of overweight children and childhood obesity have increased alarmingly. The prevalence of obesity among school children is constantly growing, regardless of the social class of children in the school7. In some states and municipalities, this prevalence arises as a result of the American prevalence, as is the case in the states of São Paulo and Rio Grande do Sul, Brazil, since they are regions with bigger development. As such, overweight children and childhood obesity is currently a public health problem that requires more attention to8,9.
Whereas, in school age, nutritional habits can be influenced by the context in which the child is inserted, especially lifestyle, inside and outside the school environment. It is important to evaluate children's growth in stature, as well as their nutritional condition, since this can be an indicator of future and potential nutritional disorders, allowing direct resources and effective public policies to be targeted at this age range.
Therefore, the objective of this study is to evaluate the growth in stature and nutritional condition of schoolchildren by gender and age in Florianopolis, Santa Catarina, Brazil, in the first semester of the school year 2012.
METHODS
A cross-cutting study was conducted with children from 6 to 10 years of age who attend to Public Municipal Elementary Schools, in the city of Florianópolis, State of Santa Catarina, Brazil.
With a basis in the relation of Public Municipal Schools, was made a probabilistic and random draw by conglomerates, having, as the sampling unit, classes of students in school until they complete the sample plot necessary.
For the calculation of the sample, an alpha of 0.05 and a power test of 0.80 was considered, with the minimal effect to be detected defined as a difference of 1/4 of standard deviation between the z scores of body mass index (zBMI) of children of both genders, on the assumption that the average zBMI among schoolchildren, without discrimination by gender, is around 0.6 and that its standard deviation corresponds to a value of around 1.110.
Therefore, the initial value estimated for the sample was 278 children of each gender, i.e. a total of 556 children, adding 10% for possible losses, eventually resulting in an initial size of a sample of approximately 610 children. The final sample of the study was 595 children.
The measured values of weight and stature were transformed into z score based on the referential values of the world of health11, using as z scores the weight (zW), the height (zH) and the body mass index (zBMI).
Diagnosis of the nutritional condition of schoolchildren using the parameter of zBMI was carried out in accordance with the reference of the World Health Organization (WHO) curves for children of 5 years or more. According to the Ministry of health and the WHO, severe thinness corresponds to z scores smaller than -3 ; thinness to z scores equal to or larger than -3 and less than -2 ; eutrophy to z scores larger or equal to -2 and less than +1 ; overweight to z scores equal to or larger than +1 and less than +2; obesity to z scores equal to or larger than +2 and less than +3 ; and severe obesity when the child showed zBMI z scores equal to or greater than +312,13.
The data were entered and stored in spreadsheets, using Microsoft Excel 2007. The quality of the categorization of anthropometric measurements was verified from scatter charts and, for children with very disparate values, the categorization data were reviewed in the original spreadsheets. In order to establish the prevalence of nutritional conditions, frequency ratios were used, with confidence intervals of 95% according to the points of cutting used. To check any differences in the prevalence of strata considered, significance for comparisons of multiple proportions was assessed using the test of nonparametric Chi-square.
The statistical analysis of the data was performed with the Statistical Package for the Social Science (SPSS) version 20.0. Anthropometric data were initially compared to the normal curve, applying the test of Kolmogorov-Smirnov distance. Descriptive statistics were used, as was a test of Pearson correlation.
This study follows the ethical principles for research with human beings, complying with resolution CNS of Brazil 466/12, and was approved by the Research Ethics Committee of the Faculty of Public Health of the University of São Paulo, in line with the document CONEP n° 2325, adopted on 31 January 2012.
RESULTS
A total of 595 children participated in this study, and 51.8% (595/308) were male, with an average of age of 8.0 years and standard deviation of 1.24, regardless of gender. When comparing boys and girls, there was no significant difference in age (p=0.8153) (Table 1).
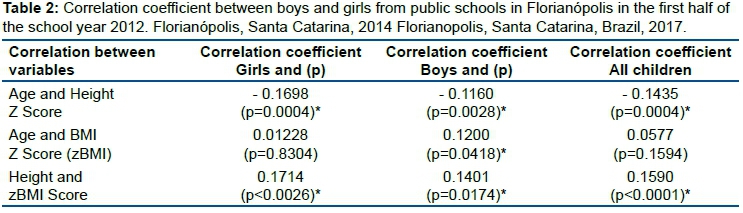
Table 1 shows that the absolute number of a child with excess weight (overweight + obesity + severe obesity) in boys was 87/308 and girls 75/287. This difference was not statistically significant (p=0.8030) (Table 2).
The correlation coefficient, in Table 2, shows that, with the exception of the variable age and zBMI for girls and for the group as a whole, the remaining variables are statistically significant.
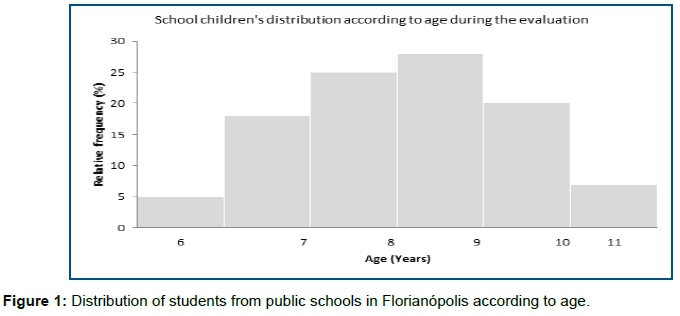
Figure 1 shows that over 50 percent of the children studied are aged between 7 and 9 years.
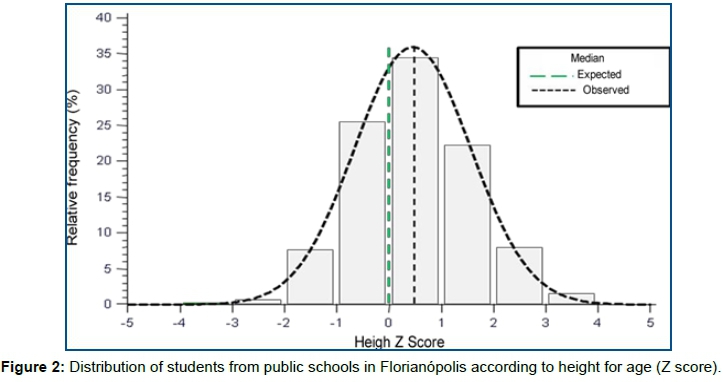
The average height of the schoolchildren was 0.44 (+ -1.11), with the girls presenting 0.38 (+- 1.11) and the boys, 0.50 (+- 1.10) (p = 0.2205 s). The comparison of the median of the group as a whole with the referential value was statistically significant (p 0.0001 <) (Figure 2).
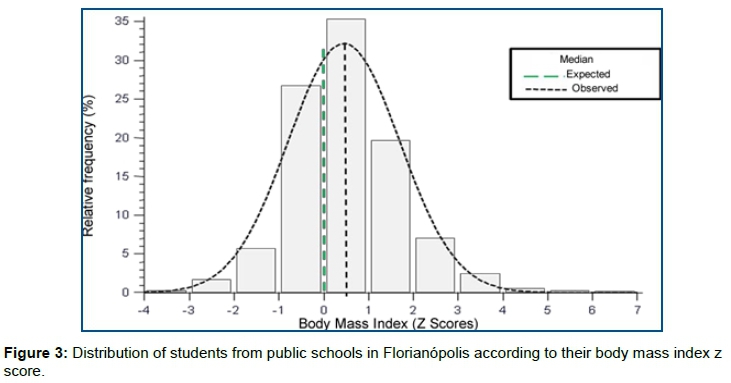
The average score was zBMI of 0.46 (+ -1.25), where that of girls was 0.40 (+-1.13) and boys 0.51 (+-1.34) (p=ns 0.2700). The comparison of the median of the group as a whole with the referential value was statistically significant (p 0.0001 <) (Figure 3).
DISCUSSION
Figures 1, 2 and 3 present information relating to measures of age, stature, and Body Mass Index (BMI) of the sample studied. They show a larger proportion of children between 7 and 9 years of age, and, for both stature and BMI, the medians are higher when compared to the reference11. This suggests that the children are growing well, above the average of the reference, but that, at the same time, they present a BMI higher than expected, even taking into account their high stature.
The diagnosis of the nutritional condition among boys and girls showed no statistical differences (p=0.8030). However, it is worth highlighting that, although the higher prevalence is eutrophic children (70.3%), a high prevalence of overweight children (overweight, obesity and severe obesity), around 28% of the sample, can also be observed. Several other studies corroborate this finding3,9,14,15, also indicating, in particular, the larger number of school children with appropriate BMI. However, in a study by Nobre et al.16, while the majority of their sample showed adequate nutritional status for age, their results diverge from the results of the present study in terms of reports that the condition of thinness or severe thinness was larger than the conditions of overweight and obesity.
In Florianopolis, Santa Catarina, Brazil, the nutritional transition, already described in research carried out in 2004 by Soar et al.17, presents evidence of the prevalence overweight children and childhood obesity of 17.9% and 6.7%, respectively, in students of public schools. In the last National Survey of Health of School, carried out with students from ninth grade of elementary school, Florianópolis, Santa Catarina, Brazil, was found to be the second location in the Country, in which the largest portion of the school is perceived as fat or too fat (21.9%). In the 2009 survey, the percentages were already similar to18.
In the city of Niterói, Rio de Janeiro, Brazil, research conducted with a sample of 328 school children demonstrates that most children are overweight and obese primarily as a result of screen time (time exposed to various forms of video, television, computer or video-game)3.
There is a significant difference between the age of the children studied and the z score of height (p=0.004), revealing that older children are proportionately shorter. When compared by gender, the differences were statistically significant, showing a stronger correlation to the boys (p<0.0001).
Height can be considered a risk factor for excess weight, as the children that are taller are also those that have a higher BMI. When compared by gender, the taller the boy, the larger the BMI. This is also the case in girls, although this correlation is stronger for males, converging with the results of the studies19,20, performed this comparison between genders, identifying that the BMI value is equivalent to the height of each child, without differences between genders, convergent with the outcome of this study.
Several studies have shown that height is a risk factor and that BMI, associated with the height, can be a good anthropometric indicator for the health of children and adolescents. It is also important to consider if there are regular changes in body composition during the process of development, tending to change the points of the cut for some of the anthropometric measures9,19,20.
The data show that there are no statistical differences between the age and BMI (p=0.1594). However, when compared by gender, there is a significant difference in girls (p=0.0418), revealing that they, with the passing of the age, tend to have a higher BMI than the boys.
Such an event may be related to a bigger hormonal load in girls than in boys during the period of puberty, primarily for the stimulation of menstruation and formation of female organs, as well as sexual maturation19.
Several studies have come to agree with this analysis, indicating that the average of BMI, from ten years of age, is substantially bigger in girls compared to their opposite gender, confirming the nutritional trend pointed to in the study20,21.
The curves of the WHO are currently recommended by the Ministry of health to assess child growth, and are already being included in the children's book on basic attention to the health of Florianópolis, Santa Catarina, Brazil.
This high growth of height and BMI can happen as a result of a nutritional transition, in which children of new generations tend to grow more, due to constant adjustments that the human being has been subjected in recent years, among them changes in nutrition22.
Urbanization can be a contributing factor to the rapid growth in terms of BMI, since, in recent years, this has been accentuated even in small centers, reflecting greater access to food area, leading to the replacement of healthy food and, thus, generating an imbalance in energy consumption and prevalence of overweight children and/or childhood obesity4,23,24.
However, despite this growth among the countries of South America, Brazil has one of the most diverse diets, as well as positioning itself among those most concerned with physiological well-being24.
This accelerated growth takes place mostly as a result of health conditions in children's first two years of life, classifying this time as essential for a child's healthy growth and emphasizing a large number of newborns with weight above the normal. In addition, the duration of breastfeeding, as well as complementary feeding, is considered essential and can interfere directly in growth, reflecting on the BMI in future ages14.
It is observed that the causes of the increase in obesity aren't sufficiently clarified. A hypothesis is a possibility that certain genetic groups are more susceptible to obesity, and that some form of nutritional transition associated with certain environmental factors such as urbanization, enhances this effect.
Following another line of thought, which compares consumption versus calorie expenditure, the behavior in terms of patterns of physical activity of the population is not yet sufficiently known, mainly in relation to the determinants of energy balance.
In Brazil, the presence of students in full-time public schooling is not always associated with the practices that require activities of energy expenditure. This, to some extent, could explain the association with the rise of obesity.
Moreover, it seems quite likely that, in recent times, the reduction of physical activity associated with leisure, is one of the determinants of nutritional condition, which has led to a higher BMI in children and adolescents. It is possible that the difficulties in proving the obesity determinants are due, in part, to the variability of individual energy expenditure, and to the evaluation of the relationship between food consumption and obesity and the association, or lack thereof, with physical activity.
It should also be noted that, in the school context, food habits, likes and dislikes, which may be established during this phase, form the basis for all life. The child has more interest in food and their nutritional needs are bigger. Their behavior is predisposed to change, given the environment that they are in, and may, thus, involve changes in nutritional condition, either positive or negative2,3.
However, the school environment is conducive to stimulating the healthy habits of life. Children spend a large part of their time in this place, which makes it important for the implementation of health policies, the prevention of obesity and the reduction of excess weight. In addition, pedagogical tools can enable the insertion of these themes into the curriculum, thus, exerting direct influence on children's development and contributing to changes in eating habits, even among families in the school community25.
Actions geared to prevention and control of obesity are the most important as first steps in a food policy that aims to be efficient. Obesity needs to be and should be regarded as a priority control event.
A school is a place that, although already seen as a backdrop for the deployment of health actions, still needs to be better used. It is necessary that health professionals start composing partnerships with educational institutions and bodies, in order to include in the curriculum actions for promoting Adequate Nutrition and Healthy Weight; knowledge to encourage healthy eating and living habits; and activities of health promotion.
It is also necessary that health services start to organize, in order to deploy proposals and strategies that attend to primary prevention of obesity.
With the advancement of technology and the globalization process, which involves changes in education and family culture, nutritional conditions, especially of children, tend to differ, leading to sedentarism, because children spend more time in their homes, working directly in their indexes of nutritional States26.
A range of different factors have been suggested as reasons for the significant increase in prevalence of obesity being observed since the last century as an injury to the health of the population, such as easy access to foods of high energy density; decreased physical activity; exposure to processed foods at low cost, which contain large amounts of fat, salt and sugar; food being packaged or sold in large portions; and the sedentary lifestyle, which results in greater access to means of transport and the increase of passive leisure activities, including TV and computer games27-30.
Yet, whereas the risk of obesity is greater for children when at least one parent is overweight, it is conceivable to imagine that a familiar environment more suitable can make a difference. It's undeniable that there is a parental influence on the consumption of certain foods 27-30.
In this sense, given that the growth in the number of children that are overweight or obese is increasing significantly, it is necessary to encourage dietary re-education, mainly in schools, accompanied by professional nutritionists, thereby aiming to decrease these anthropometric indexes, as well as preventing chronic diseases, such as hypertension and diabetes, with which they are correlated31.
It is possible that the supply of healthier food in schools and in canteens, as well as emphasizing this in meetings with parents about the subject, may represent an important strategy for facing the problems of obesity and its consequences. Other strategies may be discussed with the parents, such as providing more interactive activities and avoiding idleness of children, which, in most cases, is associated with the habit of watching TV and being exposed to media consumption.
The movement related to healthier eating patterns in individual and population levels can help improve programs for the prevention of overweight children and adolescents and childhood and adolescent obesity31.
The world is facing features of the disease of the modern era, including obesity. Often coexisting in countries with developing malnutrition, obesity is a complex condition with severe social and psychological dimensions, affecting virtually all ages and socioeconomic groups32.
Finally, several countries are going through a period of epidemiological transition, with reductions in the incidence of infectious diseases, infant mortality and birth rates, associated with a high prevalence of chronic diseases and increased life expectancy at birth.
CONCLUSION
Analysis of the growth in stature and the nutritional status of children in school age, in relation to gender and age, showed the presence of overweightness and obesity in school. The nutritional status shows no difference according to gender, even though age and stature are influencers.
An attitude that supports the development of an adequate nutritional status among children and adolescents, can aid working professionals in the field of schooling (teachers, coordinators, directors, teachers, physical education teachers, among others), and, in this case, can promote the promotion of healthy eating and physical activities inside and outside of school.
Furthermore, the careful monitoring of the nutritional status of these young children, held periodically at school, aiming at the control of related to any nutritional deficit, to pre-obesity or to obesity, would be a high-impact strategic measure in tackling the problem of childhood obesity.
REFERENCES
1.Mello ED, Luft VC, Meyer F. Childhood obesity-towards effectiveness. J Pediatr. 2004;80(3):173-82. DOI: http://dx.doi.org/10.2223/JPED.1180 [ Links ]
2.Barbosa RMS, Croccia C, Carvalho CGN, Franco VC, Salles-Costa R, Soares EA. Consumo alimentar de crianças com base na pirâmide alimentar Brasileira infantil. Rev Nutr. 2005;18(5):633-41. DOI: http://dx.doi.org/10.1590/S1415-52732005000500006 [ Links ]
3.Levy RB, Castro IRR, Cardoso LO, Tavares LF, Sardinha LMV, Gomes FS, et al. Consumo e comportamento alimentar entre adolescentes brasileiros: Pesquisa Nacional de Saúde do Escolar (PeNSE), 2009. Cienc Saude Coletiva. 2010;15(Supl 2):3085-97. DOI: http://dx.doi.org/10.1590/S1413-81232010000800013 [ Links ]
4.Wang Y, Monteiro C, Popkin BM. Trends of obesity and underweight in older children and adolescents in the United States, Brazil, China, and Russia. Am J Clin Nutr. 2002;75(6):971-7. DOI: http://dx.doi.org/10.1093/ajcn/75.6.971 [ Links ]
5.Brasil. Ministério da Saude. Secretaria de Atenção à Saúde. Departamento de atenção Básica. Orientações para a coleta e análise de dados antropométricos em serviços de saúde: Norma Técnica do Sistema de Vigilância Alimentar e Nutricional (SISVAN). Brasília: Ministério da Saúde, 2011. [ Links ]
6.Monteiro CA, Benicio MHA, Konno SC, Silva ACF, Lima ALL, Conde WL. Causas do declínio da desnutrição infantil no Brasil, 1996-2007. Rev Saude Publica. 2009; 43(1):35-43. DOI: http://dx.doi.org/10.1590/S0034-89102009000100005 [ Links ]
7.Nascimento VG, Schoeps DO, Souza SB, Souza JMP, Leone C. Risco de sobrepeso e excesso de peso em crianças de pré-escolas privadas e filantrópicas. Rev Assoc Med Bras. 2011;57(6):657-61. DOI: http://dx.doi.org/10.1590/S0104-42302011000600012 [ Links ]
8.Costa RF, Cintra IP, Fisberg M. Prevalence of overweight and obesity in school children of Santos city, Brazil. Arq Bras Endocrinol Metabol. 2006;50(1):60-7. DOI: http://dx.doi.org/10.1590/s0004-27302006000100009 [ Links ]
9.Salvador CCZ, Kitoko PM, Gambardella AMD. Estado nutricional de crianças e adolescentes: fatores associados ao excesso de peso e acúmulo de gordura. J Hum Growth Dev. 2014;24(3):313-9. DOI: http://dx.doi.org/10.7322/jhdg.88969 [ Links ]
10.Tagliari IA, Ferreira MBR, Silva LR, Pizzi J, Leite N. Overweight and low height in children of urban, rural and indigenous communities. J Hum Growth Dev. 2016;26(1)67-73. DOI: https://doi.org/10.7322/jhgd.113723 [ Links ]
11.World Health Organization (WHO). Adolescents. In: Physical status: the use and interpretation of anthropometry. Geneva: WHO, 1995; p.263-311. [ Links ]
12.Alves KP, Jaime PC. The national food and nutrition policy and its dialogue with the national food and nutrition security policy. Cienc Saude Coletiva. 2014;19(11):4331-40. DOI: https://doi.org/10.1590/1413-812320141911.08072014 [ Links ]
13.Toschke AM, Kohl L, Mansmann U, von Kries R. Meta-analysis of blood pressure tracking from childhood to adulthood and implications for the design of intervention trials. Acta Paediatr. 2010;99(1):24-9. DOI: https://doi.org/10.1111/j.1651-2227.2009.01544.x [ Links ]
14. Bertotto ML, Valmórbida J, Broilo MC, Campagnolo PB, Vitolo MR. Associação entre ganho de peso no primeiro ano de vida com excesso de peso e adiposidade abdominal na idade pré-escolar. Rev Paul Pediatr. 2012;30(4):507-12. DOI: http://dx.doi.org/10.1590/S0103-05822012000400008 [ Links ]
15.Silveira JAC, Taddei JAAC, Guerra PH, Nobre MRC. Effectiveness of school-based nutrition education interventions to prevent and reduce excessive weight gain in children and adolescents: a systematic review. J Pediatr (Rio J). 2011;87(5):382-92. DOI: http://dx.doi.org/10.1590/S0021-75572011000500004 [ Links ]
16.Nobre GC, Lima KSC, Silva ADG, Souza Filho AN, Letieri RV, Bandeira PFR. Índices de crescimento estatural e estado nutricional de escolares de 6 a 14 anos escolares de 6 a 14 anos. Conexões. 2014;12(1):126-41. DOI: https://doi.org/10.20396/conex.v12i1.2184 [ Links ]
17.Soar C, Vasconcelos FAG, Assis MAA. Waist-hip ratio and waist circumference associated with body mass index in a study with schoolchildren. Cad Saúde Pública. 2004;20(6):1609-16. DOI: http://dx.doi.org/10.1590/S0102-311X2004000600019 [ Links ]
18.Garcia LP, Sant'Anna AC, Magalhães LCG, Freitas LRS, Aurea AP. Gastos das famílias brasileiras com medicamentos segundo a renda familiar: análise da Pesquisa de Orçamentos Familiares de 2002-2003 e de 2008-2009 . Cad Saúde Pública. 2013;29(8): 1605-16. DOI: http://dx.doi.org/10.1590/0102-311X00070912 [ Links ]
19.Cossio-Bolaños MA, Maria TS, Campos RG, Pascoal EHF, Hespanhol JE, Arruda M. O uso das curvas de crescimento da organização mundial da saúde em crianças e adolescentes que vivem em regiões de altitude moderada. Rev Paul Pediatr. 2012;30(3):314-20. DOI: http://dx.doi.org/10.1590/S0103-05822012000300003 [ Links ]
20.Silva DAS, Pelegrini A, Petroski EL, Gaya ACA. Comparação do crescimento de crianças e adolescentes brasileiros com curvas de referência para crescimento físico: dados do Projeto Esporte Brasil . J. Pediatr. (Rio J.). 2010;8692):115-20. DOI: http://dx.doi.org/10.1590/S0021-75572010000200006 [ Links ]
21.Gilglioni EH, Ferreira TV, Bennemman RM. Estado nutricional dos alunos das escolas da rede de ensino Municipal de Maringá, Estado do Paraná, Brasil. Acta Sci Heal Sci. 2011;33(1):83-8. DOI: https://doi.org/10.4025/actascihealthsci.v33i1.6349 [ Links ]
22.Alencar MSS, Barros SEL, Borges IS, Cavalcante KN, Melo MTSM, Nunes IFOC, et al. Adequacies and inadequacies in the anthropometric and dietetic profiles of preschool children. J Hum Growth Dev. 2016;26(2):234-42. DOI: http://dx.doi.org/10.7322/jhgd.119290 [ Links ]
23.Bontorin MS, Barbosa Filho VC, Moreira NB, Barbacena MM, David A. Estado nutricional segundo as curvas de crescimento da Organização Mundial de Saúde em crianças de Taguatinga - DF, Brasil. Motricidade. 2012;8(Supl. 2):700-8. [ Links ]
24.Moratoya EE, Carvalhaes GC, Wander AE, Almeida LMCM. Mudanças no padrão de consumo alimentar no Brasil. Rev Política Agrícola. 2013;22(1):72-84. [ Links ]
25.Assis MAA, Rolland-Cachera MF, Grosseman S, Vasconcelos FAG, Luna MEP, Calvo MCM, et al. Obesity, overweight and thinness in schoolchildren of the city of Florianopolis, Southern Brazil. Eur J Clin Nutr. 2005;59(9):1015-21. DOI: https://doi.org/10.1038/sj.ejcn.1602206 [ Links ]
26.Guedes DP, Paula IG, Guedes JERP, Stanganelli LCR. Prevalência de sobrepeso e obesidade em crianças e adolescentes : estimativas relacionadas ao sexo , à idade e à classe socioeconômica. Rev Paul Educ Fís Esp. 2006;20(3):151-63. [ Links ]
27.Onnerfalt J, Erlandsson L-K, Orban K, Broberg M, Helgason C, Thorngren-Jerneck K. A family-based intervention targeting parents of preschool children with overweight and obesity: conceptual framework and study design of LOOPS- Lund overweight and obesity preschool study. BMC Public Health. 2012;12:879. DOI: https://doi.org/10.1186/1471-2458-12-879 [ Links ]
28.Quaioti TCB, Almeida SS. Determinantes psicobiológicos do comportamento alimentar: uma ênfase em fatores ambientais que contribuem para a obesidade . Psicol USP. 2006;17(4):193-211. DOI: http://dx.doi.org/10.1590/S0103-65642006000400011 [ Links ]
29.Hirschler V, Roque MI, Calcagno ML, Gonzalez C, Aranda C. Maternal waist circumference and the prediction of children's metabolic syndrome. Arch Pediatr Adolesc Med. 2007;161(12):1205-10. DOI: http://dx.doi.org/10.1001/archpedi.161.12.1205 [ Links ]
30.Hoehr CF, Reuter CP, Tornquist L, Nunes HMB, Burgos MS. Prevalência de obesidade e hipertensão arterial em escolares: estudo comparativo entre escolas rurais do município de Santa Cruz do Sul/RS. Rev Epidemiol Control Infec. 2014;4(2):122-6. [ Links ]
31.Feferbaum R, Abreu LC, Leone C. Fluid intake patterns: an epidemiological study among children and adolescents in Brazil. BMC Public Health. 2012;12(105). DOI: http://dx.doi.org/10.1186/1471-2458-12-1005 [ Links ]
32.Shoeps DO, Abreu LC, Valenti VE, Nascimento VG, Oliveira AG, Gallo PR, et al. Nutritional status of pre-school children from low income families. Nutr J. 2011;10:43. DOI: http://dx.doi.org/10.1186/1475-2891-10-43 [ Links ]
 Correspondence:
Correspondence:
italla.bezerra@emescam.br
Manuscript received: September 2019
Manuscript accepted: February 2020
Version of record online: March 2020


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}