











 (pdf)
(pdf)




 Permalink
PermalinkJournal of Human Growth and Development
ISSN 0104-1282 ISSN 2175-3598
J. Hum. Growth Dev. vol.31 no.3 Santo André set,/dez. 2021
https://doi.org/10.36311/jhgd.v31.12770
ORIGINAL ARTICLE
DOI: 10.36311/jhgd.v31.12770
Epidemiological profile of COVID-19 in the State of Espírito Santo, Brazil, from march 2020 to june 2021
Claudia Dobes Kawatake de SousaI; Tassiane Cristina MoraisII, III; Blanca Elena Guerrero DaboinI; Isabella PortugalIV; Matheus Paiva Emidio CavalcantiI; Jorge de Oliveira EcheimbergV; Lucas Cauê JacinthoVI; Rodrigo Daminello RaimundoV; Khalifa ElmusharafI; Carlos Eduardo SiqueiraI, VII
IMaster of Public Health Program, School of Medicine, University of Limerick, V94 T9PX, Limerick, Ireland
IIEscola Superior de Ciências da Santa Casa de Misericórdia (EMESCAM), 29045-402 Vitória, ES, Brazil
IIIDepartamento de Educação Integrada em Saúde, Universidade Federal do Espírito Santo, 29075-910 Vitória, ES, Brazil
IVDepartamento de Clínica Médica, Faculdade de Medicina da Universidade de São Paulo, 05403-000 São Paulo, SP, Brazil
VLaboratório de Delineamento de Estudos e Escrita Científica, Centro Universitário FMABC, 09060-870 Santo André, SP, Brazil
VIDivisão de Imunologia e Alergia Clínica, Departamento de Medicina, Faculdade de Medicina da Universidade de São Paulo, 05403-000 São Paulo, SP, Brazil
VIIDepartment of Urban Planning and Community Development, School for the Environment, University of Massachusetts Boston, 100 Morrissey Boulevard, Boston, MA 02125
ABSTRACT
INTRODUCTION: coronavirus 2019 Disease (COVID-19) was quickly declared a pandemic, and Brazil is facing the most significant health and hospital crisis in its history. From March to June 2021 represented 50.8% of all deaths in the State of Espirito Santo
OBJECTIVE: to analyze the lethality and mortality by COVID-19 in the State of Espirito Santo from March 2020 to June 2021.
METHODS: an ecological study was carried out, using a time series of public and official data available on the Health Department of the State of Espirito Santo, Brazil. Were considered information about cases and deaths (from March 2020 to June 2021) of COVID-19. Percentage case-fatality and mortality and incidence rates per 100,000 population were calculated. Time-series analyses were performed using the Prais-Winsten regression model, estimating the Daily Percent Change (DPC), and the trends were classified as flat, increasing, or decreasing. Significant differences were considered when p<0.05.
RESULTS: 524,496 confirmed cases of COVID-19 as of June 30, 2021, and 11,516 progressed to death. The presence of cardiovascular diseases represents more than half of confirmed comorbidities (54.37%) in patients with COVID-19, followed by diabetes (19.95%) and obesity (9.34%). Men had higher mortality and lethality, especially in older age groups, but the incidence was higher among women. A characteristic profile of two waves was observed; the first wave was extended from March to October 2020 and the second complete wave from November 2020 to June 2021. During the second wave, high peaks of incidence, lethality, and mortality were recorded. At the end of the second wave, the incidence rate remained with increasing trends (p < 0.05), with a DPC of 2.06%.
CONCLUSION: the peak concentration of cases, deaths, and indicators of lethality, mortality evidenced even after one year of pandemic, characterizes the severity of the COVID-19 pandemic, still in entire evolution in the State Espirito Santo and Brazil.
Keywords: case fatality, mortality, COVID-19, SARS-CoV-2.
Authors summary
Why was this study done?
This study was carried out due to the need for epidemiological studies on the COVID-19 pandemic, especially in the state of Espírito Santo. Thus, it is of paramount importance to identify trends in incidence, lethality, and mortality to elucidate the epidemiological parameters of the first and second wave to develop pandemic planning.
What did the researchers do and find?
This study aims to analyze the incidence, mortality, and lethality by COVID-19 in the State of Espírito Santo from March 2020 to June 2021. An ecological study was carried out using a time series of public and official data available on the Health Department of the State of Espírito Santo, Brazil. The effective reproduction number (Rt), the incidence, mortality and lethality were estimated, then the trend analysis according to the wave period were classified in increased, decreased, or flat. We found that the first wave of COVID-19 in the analyzed region was marked by stationary lethality trends, increasing mortality and incidence trends and in the second wave, despite the incidence growing trends, mortality showed stationary trends, with lethality with decreasing trends.
What do these findings mean?
The pandemic is still in evolution in the State of Espírito Santo. Therefore, needing a focus on non-pharmacological measures as well as reducing the movement of people to reduce the spread of the virus and advances in vaccination to fight COVID-19.
INTRODUCTION
Coronavirus Disease 2019 (COVID-19) was quickly declared a pandemic, causing a global recession in the economic and health systems1-4. In Brazil, the fight against the disease resulted in the most significant health and hospital crisis in its history, marked by the lack of government control. It can be evidenced by the number of notifications of more than 19 million cases confirmed of the disease, with 550,502 thousand lives lost until July 26, 2021, 11,826 of them notified by the State of EspíritoSanto5.
COVID-19 is a respiratory tract infection caused by the Severe Acute Respiratory Syndrome of coronavirus 2 (SARS-CoV-2). While the majority population has mild symptoms, about 20% of patients develop severe complications such as Acute Respiratory Syndrome (SARS), septic shock, and multiple organ failure, with 3-6% achieving mortality. Due to the lack of specific antiviral treatment, the management of this condition remains primarily symptomatic, with intensive support treatment for critically compromised patients6.
The severity and lethality of COVID-19 have been associated with chronic non-communicable diseases (NCDs) such as high blood pressure, diabetes, respiratory infections, and cardiovascular diseases7-9. There is a demographic and epidemiological transition in progress in the Brazilian case, with a high prevalence of NCDs, especially cardiovascular diseases related to obesity and sedentary lifestyle10-12. These comorbidity associations make the country's scenario during the pandemic even more problematic from the point of view of Public Health.
For Mesenburg et al.13, the prevalence of chronic NCD in the country is high. However, people with comorbidities have more severe forms of COVID-19 and a higher prevalence of symptoms. It is highlighted that the transmissibility of the Sars-CoV-2 virus is similar in people with or without these pathologies. Cardiovascular diseases represent 56% of the comorbidities of the COVID-19 confirmed cases, followed by diabetes (20%) and obesity with 8,4%14.
According to public data from the EspíritoSanto State Health Department15, there is a more significant number of confirmed cases in females (53%) but a higher frequency of deaths in males (53%). Regarding the age group, there is a predominance of confirmed cases of Coronavirus disease in an economically active age group, but with the highest frequency in people between 20 and 59 years (74%). The number of deaths is high, especially in the elderly over 60 years of age (69%).
Thus, epidemiological analyses based on the triad person, time, and place generate transformations in the characterizing elements of EspíritoSanto society. The context of the COVID-19 pandemic is complex, and measures to promote the flattening of the epidemiological contamination curve will require multiple analyses and contributions to the knowledge of the pandemic situation and its social repercussions.
According to Malta and collaborators16, Brazil is the only country globally with more than 200 million inhabitants and has unrestricted access to Unified Health System (SUS-Sistema Único de Saúde). Therefore, it is crucial to understand the dynamics of the pandemic in the most distinct regions of the country, especially the high incidence and mortality caused by the disease. Thus, this study's objective is to analyze the lethality and mortality by COVID-19 in the State of EspíritoSanto from March 2020 to June 2021.
METHODS
Study Design
An ecological study was carried out using a time series of public and official data available on the Health Department of the State of EspíritoSanto, Brazil15 (2021). This study is part of a population-based umbrella project, where each state of Brazil was analyzed separately, following a standard protocol for ecological time-series studies as described by Abreu, Elmusharaf and Siqueira17.
Study Location and Period
The State of EspíritoSanto belongs to the southeast region of Brazil; it is formed by 78 municipalities, with Vitória as the capital. The State has a territorial extension of 46,074,447 km2, a demographic density of 76.5 inhabitants/km2, and an average number of inhabitants per household of 2.8 people. The monthly per capita income is 1,347 reais, the human development index (HDI) is 0.740, and the State has 790 basic health units18,19. Furthermore, according to the EspíritoSanto State Health Department15, until June 13, 2021, the State had 5,013 infirmary beds and 2,560 ICU beds, with 1,300 infirmary beds and 1,611 ICU beds for COVID-19 patients, with an occupancy rate of 62.73% and 42.54% respectively.
The database was updated on July 20, 2021, considering information about cases (from March 2020 to June 2021) and deaths (from April 2020 to June 2021) of COVID-19.
Study Population and Eligibility Criteria
This study included data on 524,496 cases and 11,516 deaths accumulated of COVID-19 reported by EspíritoSanto's municipalities. The cases were classified according to the diagnosis date, while the deaths were classified according to the death date.
All notifications of COVID-19 cases and related deaths were confirmed by clinical, laboratory and/or epidemiological confirmation of disease.
Data Collection
Two researchers independently extracted the data to minimize collection bias and guarantee the quality and reliability of the data obtained. The collected data were organized into spreadsheet software Microsoft® Excel 2016.
Data Analysis
The effective reproduction number (Rt) was estimated using R studio software EpiEstim package20, version 2.2.4, a previously time-varying reproduction number for epidemics model, developed by Thompson and colleagues21. Our model used a mean serial interval of 2.97 days with an average standard deviation of 3.29 days, as described in previous studies22,23.
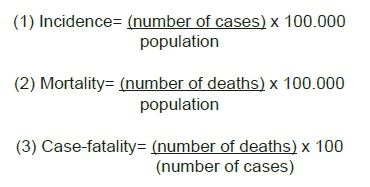
The incidence (1) and mortality rates (2) by 100,000 inhabitants and the case-fatality (3) (%) were calculated according to the equations:
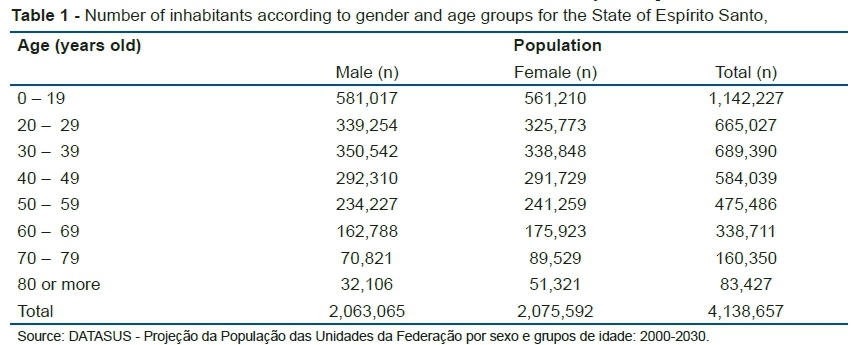
Mortality rates were also calculated and stratified by sex and age for the same period. According to the populational projection of Federation Units for the year 2020, the State of EspíritoSanto had 4,138,657 inhabitants24. The distribution of the population by gender and age is described in table 1.
For trend analysis, the period was divided into the first wave (1st Wave - March to October 2020) and second wave (2nd Wave - November 2020 to June 2021) to define the end of the first wave, the month with the lowest mortality rate was considered, which suggested the end of a first wave in the curve.
The trends were analyzed according to the methodological guidelines by Antunes and Cardoso25, the Prais-Winsten regression model for population mortality rates was used to build time series, series as well as to determine incidence, case fatality and mortality trends. Were estimated the probability (p), and Daily Percent Change (DPC), considering a 95% level significance, according to equations (1), (2), and (3):
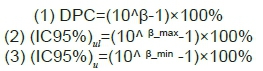
In these equations, we considered β as the angular coefficient from the linear regression, the indexes ul as the upper limit, and ll as the lower limit of the confidence level.
The case-fatality, mortality and incidence trends were classified in increased, decreased, or flat. Flat trends were considered when p value was not significant (p<0.05).
Statistical analyses were performed using the STATA 14.0 software (College Station, TX, U.S. 2013).
Ethical and Legal Aspects of the Research
Ethics committee approval was not required because only secondary data available on the internet were used in this study.
RESULTS
There were 524,496 cases and 11,516 deaths accumulated from COVID-19 in EspíritoSanto from March 2020 to June 2021. There was a higher proportion of female individuals in the cases (53.48%) and male (54.71%) in deaths. There was a higher percentage of confirmed cases among people aged 30 to 39 years, while deaths were more prevalent among the elderly (60 to 69 years - 24.85%; 70 to 79 years - 24.85%; and 80 years or more - 23.11%) (table 2).
It was observed that 126,981 comorbidities reported in cases and 12,324 in deaths from COVID-19. Among the comorbidities reported, cardiovascular comorbidities were the most prevalent in both groups (54.37% cases; 49.13% deaths), followed by diabetes (19.95% - cases; 26.19% - deaths) and obesity (9.34% - cases; 9.19% - deaths) (table 2). The lethality (%), mortality and incidence rates (per 100,000 inhabitants) of COVID-19 in the analyzed State, distributed by sex and age, were illustrated in table 2.
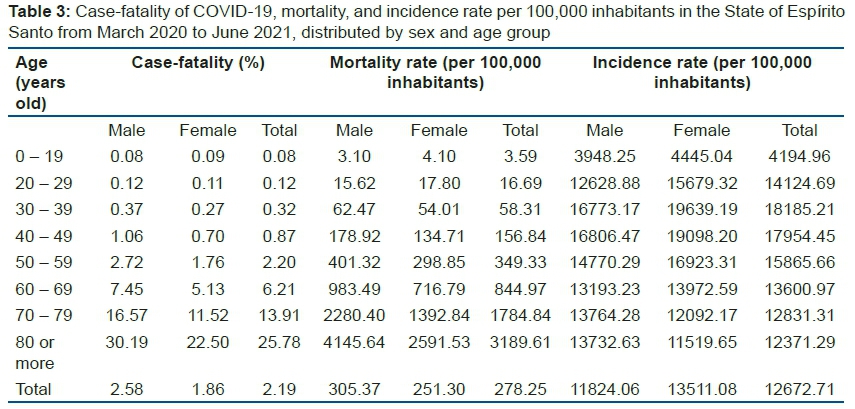
The lethality (%), mortality and incidence rates (per 100,000 inhabitants) of COVID-19 in the analyzed State, distributed by sex and age, were illustrated in table 3.
The mortality rate of COVID-19, considering the entire period analyzed, was 2.19%, with mortality rates of 278.25 deaths per 100,000 inhabitants and an incidence of 12,672.71 new cases per 100,000 inhabitants. It was observed that the lethality and mortality rates were higher at older ages, in which male individuals aged 80 years or older had the most increased lethality (30.19%) and mortality (4,145.64 deaths per 100,000 population) scores. At the same time, the highest incidence rates were found among females' individuals aged 30 to 39 years (19,639.19 cases per 100,000 inhabitants) and 40 to 49 years old (19,098.20 cases per 100,000 inhabitants) (table 3).
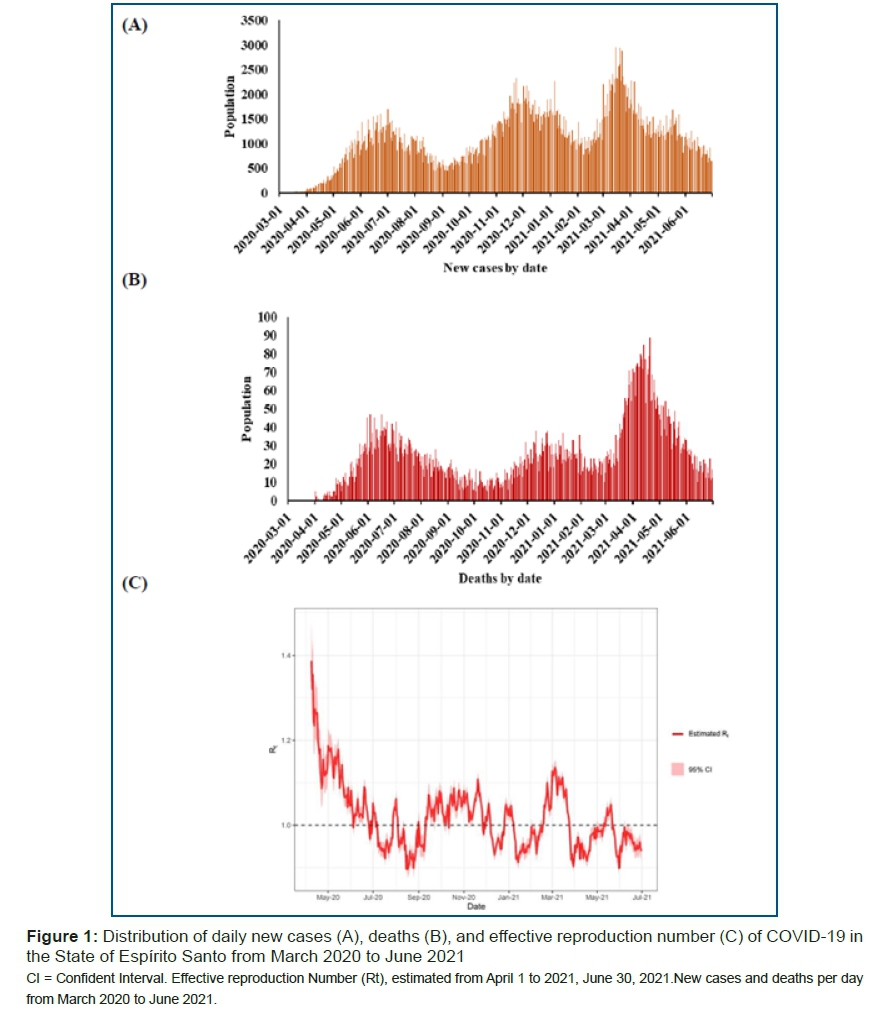
The distribution of cases and deaths per day and the Effective reproduction number (Rt) of COVID-19 in the State of EspíritoSanto were highlighted in figure 1.
There was a significant oscillation in the distribution of new cases and deaths of COVID-19, with maximum peaks of daily cases observed during March 2021 (figure 1A) and fatalities in April 2021 (figure 1B). The Effective reproduction number also suffered large fluctuations; only in July, August, December 2020, and January 2021 did the transmissibility of SARS-COV-2 controlled, with a predominance of Rt with values below one. However, there was an increase in transmissibility during March 2021 (Rt >1), with controlled levels in the subsequent months (figure 1C).
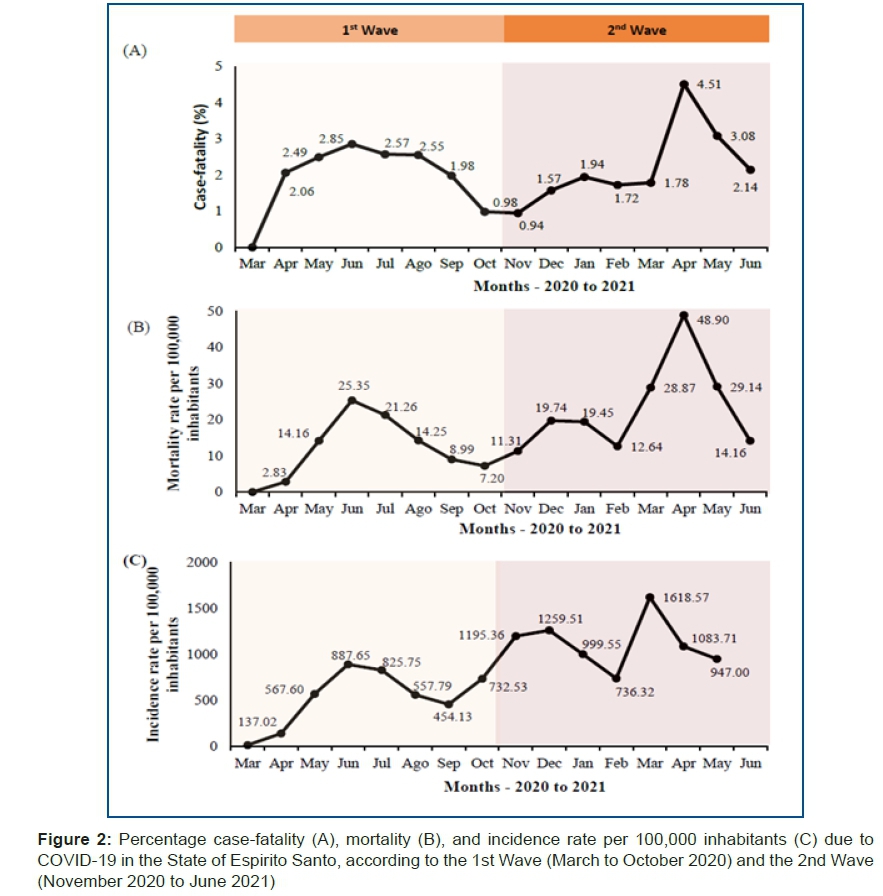
The indicators of lethality, mortality, and incidence varied according to the months analyzed, presenting a two-wave profile, as illustrated in figure 2. It was evidenced that even after one year of pandemic, the State of EspíritoSanto described higher rates of lethality (4.51%) and mortality (48.90 deaths per 100,000 inhabitants) in April 2021, with a peak incidence in March 2021 (1,618,57 new cases per 100,000 inhabitants) (figure 2).
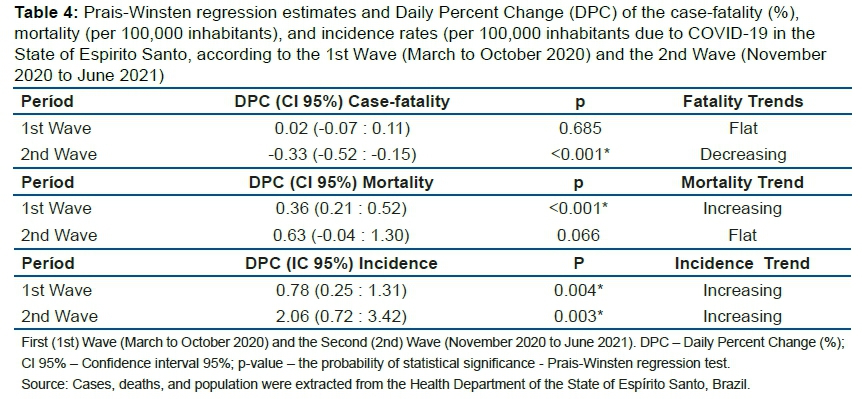
Prais-Winsten regression estimates and Daily Percent Change (DPC) of the case-fatality (%), mortality (per 100,000 inhabitants), and incidence rates (per 100,000 inhabitants due to COVID-19 in the State of EspíritoSanto according to the first and second wave (table 4). The first wave of COVID-19 in the analyzed region was marked by stationary lethality trends, increasing mortality and incidence trends (p<0.05) with respective DPC: 0.36% and 0.78%. In the second wave, despite the incidence growing trends (p<0.05), mortality showed stationary trends, with non-significant p-value (p<0.05), with lethality with decreasing trends (p<0.05) with DPC of -0.33% (table 4).
DISCUSSION
The State of EspíritoSanto, reported 524,496 cases accumulated from COVID-19 up to June 30, 2021, of which 11,516 died from the disease. There were oscillations in viral transmissibility, in the number of cases and deaths, with high peaks in the incidence indicators (March 2021), mortality, and lethality (April 2021) observed even after one year of pandemic. Although lethality rates have decreasing trends at the end of the second wave (November 2020 to June 2021) and mortality is stationary, the incidence remains with increasing trends throughout the analyzed period.
The first case notification of COVID-19 in the State began on February 25, 2020; however, this confirmation was dismissed out by the Central Laboratory of EspíritoSanto. On March 5, 2020, the first case was confirmed, from a resident of the Metropolitan region of Vitória with a history of international travel26. Thus, subsequent cases followed similar behavior in the first half of March 2020, with predominant origin abroad and in the State of São Paulo (Brazil), the epicenter of the disease in Latin America27,28.
Although the first suspicions of COVID-19 were reported in February 2021, there is evidence that the virus circulated in EspíritoSanto before this date. In a study that analyzed samples of 7,370 patients, without prior suspicion of COVID-19, but who had symptoms compatible with viral infections such as Dengue or Chikungunya, from December 1, 2019, to June 30, 2020, the results illustrated that 210 SARS-CoV-2 positive cases were detected. These hidden cases possibly indicate delays in seeing patients, which may have contributed to the rapid expansion of the COVID-19 outbreak29.
Community transmission in EspíritoSanto began in March 2020, and cases increased with the first deaths, and the territorial extension of the disease grew, incorporating other neighborhoods and cities. In this initial phase of the disease, there was a predominance of the regions with the highest human development index (HDI) in the State of EspíritoSanto, such as Vitória (MHDI = 0.845) and Vila Velha (MHDI = 0.8)18,27, evidencing the manifestation of the pandemic stratified by social class, sex, and race30.
Concerning sociodemographic aspects, similar findings were reported by the State Government, with predominant COVID-19 cases in females (53%) but with a higher frequency of deaths in males (53%). There is a predominance of confirmed cases of COVID-19 in populations of economically active age in the age variable. Even with the highest frequency of cases in the 20 to 59 age group (74%), the number of deaths occurs mainly in the elderly population aged 60 and over (70%)14.
Thus, greater susceptibility to severe conditions of COVID-19 and higher mortality are associated with biological sex and age group. Males have a higher risk of mortality than women; the elderly also have a higher mortality rate than younger individuals31.
It is noteworthy that comorbidities also represent significant risk factors in addition to gender and age group. According to Wang et al.32 which evaluated data from 36 patients affected by COVID-19 who required care in the Intensive Care Unit (ICU), illustrated that 72.2% of the individuals had comorbidities. This finding indicates that a history of chronic diseases can lead to the development of complications.
In this context, it is essential to analyze health indicators, especially lethality and mortality rates. Lethality measures the number of deaths about people with active disease and not concerning the total population; that is, it evaluates the percentage of infected people who progress to death, while the mortality rate is used to analyze the impact of a disease or condition on the entire population of a region. These two variables were influenced by associated comorbidities and the immunosuppression presence, especially in elderly patients, with median age above 60 years33,34. Moreover, as the pandemic progressed, other elements became risk factors for worsening the situation, such as gender, ethnicity, particularly blacks and Hispanics and comorbidities35.
The main categories of comorbidities associated with COVID-19 in the State of Espírito Santo, were related to the presence of CVDs, and indicate a higher risk of mortality. The CVDs represented more than half of the morbidities reported (54.37%) by confirmed cases in this State, followed by diabetes (19.95%) and obesity (9.34%). In line with the study by Silva et al.,36 conducted in the state capital of Amapá, Brazil, the authors highlighted those 102 patients with comorbidities and diagnosed with COVID-19 had chronic CVD (38.33%), diabetes (24.16%), and chronic respiratory diseases (13.33%) as the most prevalent risk factors.
Pre-existing conditions impair the body's immune response, such as diabetes mellitus (DM) and obesity, which are potential aggravating factors of the infectious illness generated by SARS-Cov-2, impacting the patient's evolution to death. In a study by Oliveira et al.,37 the main comorbidities reported in patients with COVID-19 were DM, chronic heart diseases, and hypertension-related to cardiovascular conditions and chronic respiratory diseases. In this case, the comorbidity with the highest record in cases of death was hypertensive disease. Furthermore, several authors highlight systemic arterial hypertension as one of the main aggravating factors for the COVID-19 condition, together with other CVDs, being associated with worse prognoses and high lethality rates38-40.
Previous coronavirus outbreaks have been associated with comorbidities and cardiovascular complications41. Increased inflammatory and immunological responses, endothelial damage, microvascular dysfunction or thrombosis due to hypercoagulability, and stress cardiomyopathy are possible pathways of the acute coronary syndrome42. A recent systematic review and meta-analysis by Cochrane showed that 20.0% (95% CI 16.1-23.8% with substantial heterogeneity - I2 = 94.9%) of patients hospitalized with COVID-19 had an acute myocardial infarction43. For example, a study involving 5,119 Danish patients diagnosed with COVID-19 revealed that the incidence of Acute Myocardial infarction (AMI) was approximately five times higher during the 14 days after infectious diagnosis than the control interval44. However, there remains a scarcity of data regarding the true incidence of acute AMI due to microvascular dysfunction and coronary thrombosis in patients with COVID-19, given the difficulty of outlining such dedicated studies.
About obesity, it has long been known that it is directly associated with poor prognoses and prolonged recovery in cases of viral infections. In the context of COVID-19, other factors related to obesity may be responsible for the higher chances of worsening the clinical picture, which includes deficient respiratory mechanics, low gas exchange rate in the lungs, increased airway resistance, reduced lung strength, and lower lung volume45.
Among the other most prevalent risk factors, Bornstein et al.,46 also highlight the direct relationship between DM and the COVID-19 with greater severity of the clinical condition, resulting in a glycemic increase in patients with type 2 DM. In addition, the pre-existence of respiratory diseases was the first and primary risk factor associated with severe conditions of COVID-1947,48. Finally, comorbidities such as cerebrovascular diseases, neoplasms, smoking, Alzheimer's disease, pancreatic disease, dengue, alcohol consumption, and puerperal period were also related to the worse prognosis of COVID-19, although to a lesser extent.
Time analysis
After the beginning of community transmission in the State of Espírito Santo in March 202027, the distribution of new cases per day showed a high degree of variation in the distribution of COVID-19 cases throughout 2020, peaking in March 2021, recording an incidence rate of 1,618.57 new cases per 100,000 inhabitants. The estimated Rt is important to understand the changes in the transmissibility of infectious diseases over time. In COVID-19, this parameter has been adopted to evaluate the effects of interventions and support the creation of Public Policies49. During the period from March 1, 2020, to June 30, 2021, Rt suffered oscillations and remained higher than one (R>1) for most of the studied period, with higher peaks at the beginning of the pandemic and in March 2021, illustrating a dyscontrol in the transmissibility of SARS-CoV-2 in the analyzed period.
By analyzing the daily percentage variation in lethality, mortality, and incidence rates due to COVID-19, indicating increasing, decreasing, or stationary trend rates, it is possible to understand the dynamics of the pandemic compared to a simple rate analysis.
The highest percentage values of lethality were observed during the first wave in May 2020 (2.85%), and during the second wave and in April (4.51%) and May (3.08%) 2021. In this same period, the highest mortality rates (deaths per 100,000 inhabitants) were also recorded: June 2020 (25.35), April (48.90), and May (29.14) 2021. Despite the peaks of mortality and lethality observed during the second wave, stationary trends for mortality and decreasing for lethality were evidenced. However, the incidence remained increasing, with a DPC of 0.36% during the first wave and 0.78% during the second wave. Trends in lethality, mortality, and incidence rates may change according to the region. The stationary trends in lethality rates found during the first wave followed the global trend of lethality of COVID-19 that remained stationary between December 31, 2019, and August 31, 202050.
Spatial analysis
According to Bernal et al.,50, the COVID-19 pandemic is still in a global progression phase. In the State of Espírito Santo, this same trend is observed today.
In the analysis of the monitoring of the spread of COVID-19 based on the cartographic analysis of thematic maps on the notifications of confirmed cases, Ferreira et al., (2020)51 highlight that the first cases occurred in cities with a larger population and have a greater connection with metropolises and medium-sized cities, indicating a possible correlation between the hierarchy of cities in the urban network and the spread of the virus in populations.
Moreover, the spatial propagation of COVID-19 in the State of Espírito Santo territory followed a pattern of combined diffusion, with hierarchical and contagion stages, severely affecting the Metropolitan Region of Greater Vitória (RMGV) at first, but with a tendency to internalization in the State. In the scale of the urban space of the metropolitan agglomeration, there is a process of peripheralization, in which the central neighborhoods have lower lethalities than the peripheral ones14.
The geographical analysis of the spread of SARS-Cov-2 and the manifestation of COVID-19 shows that population density and mobility are determinants in pandemic control. The mathematical models of transmissibility are supported by the results observed in regions with denser populations that did not implement non-pharmacological contagion prevention measures in their daily lives52. These variables contributed to the increase in viral transmissibility and the consequent manifestation of COVID-19, which may increase population lethality and mortality and the impacts already caused by comorbidities and advanced ages associated with more favorable outcomes of death.
Thus, population density/concentration and mobility/flow criteria were determinants for the observed increase in lethality and mortality during the first period of COVID-19 pandemic registration. The population clusters of the RMGV presented the highest viral transmission outcome, and the disease's development was observed in the first cycle of the pandemic analyzed14,26,27.
Epidemiological analysis
The COVID-19 pandemic has led health systems to collapse worldwide. According to the World Health Organization53, almost all countries (90%) experienced some interruption in health care at the beginning of the pandemic, with the most considerable number reported in low- and middle-income countries. However, interruptions in essential services are widespread geographically around the world. In Brazil, the dissemination of SARS-CoV-2 presented a complex epidemiological picture, which evidenced the greatness and diversity of the health care network of the unified health system (SUS) public, allowing the maximization of its use and rescue of its classic principles of universality, integrality, and equity.
In each Brazilian State, different strategies were observed by the health authorities to contain the dissemination and spread of the virus. Given the epidemiological picture of COVID-19, there is a need to develop different forms of analysis of outcomes to better understand the aspects of the current pandemic regarding lethality and mortality.
The geographic-temporal distribution of COVID-19 cases in the State of Espírito Santo, in the Southeastern Brazilian Region, was performed from data clusters and divided into two periods: first wave and second wave of COVID-19, with the closing of the analysis on June 30, 2021.
The behavior of the outcome variables lethality and mortality by COVID-19 evidences the difficulties of dealing with transmissibility due to the low testing of individuals in the State of EspíritoSanto. Added to these data clusters is the expectation of the action of herd immunity, which according to Kadkhoda54 this immunity represents the population's immune protection to cease the chain of transmission of an infectious disease, which can be obtained through infection or vaccination. The adoption of strategies based on herd immunity is implicit in community actions and the feeling of diminishing the severity of the pandemic, mainly due to the absence of education and health actions aimed at disseminating the fundamental aspects of the evolving pandemic in that federative State28,55.
The profile of the epidemiological manifestation of the pandemic caused by the uncontrolled transmissibility of COVID-19 occurred in municipalities with similar demographic characteristics, high population density, and migration of people within and between cities of the State of Espírito Santo. In the first cycle of the pandemic, characterized by community transmission in the State of Espírito Santo, there was an increase in lethality and mortality evidenced in the records of the March data clusters. The commemorative date of a great migration of people in this period was the celebration of the largest and most popular Brazilian cultural festival, Carnival.
In the following months, these variables decreased, maintaining this behavior until October 2020. It is noteworthy that non-pharmacological measures of social distancing, as well as the cultural impregnation of the use of masks and local economic incentive to reduce agglomerations, such as the implementation of virtual educational platforms for non-presential (remote) classes at different levels of education (elementary, middle and university education) were adopted in all the municipalities of Espírito Santo.
In the epidemiological phases of the pandemic, three steps stand out. The first phase, consisting of imported cases through infected people in other countries, with March 2020 as the time frame. The second phase is characterized by local transmission when people with no recent international travel history become ill. This phase is characterized by increased lethality and mortality outcomes. It is also noteworthy that it is possible to identify the definitive host (human beings) of the etiological agent (SARS-CoV-2), who are usually relatives or people of close social life. In this way, it is possible to track cases and isolate suspected and confirmed cases. However, this type of intervention for epidemiological control/surveillance is dependent on testing, which was very low in the State during the first wave of COVID-19 due to the still incipient availability in the national market. Finally, in the third phase, characterized by community transmission, there was an increase in confirmed cases and the number of people who evolved with the disease in the State of EspíritoSanto. It was no longer possible to identify the transmitting source.
In March 2020, during the first cycle of the COVID-19 pandemic, community contamination was already included in the State of EspíritoSanto. Following the epidemiological analysis, considering the lethality and mortality outcomes in the second cycle of the COVID-19 pandemic in the State, the evolution of the 2nd epidemiological wave of the COVID-19 pandemic (November 2020 to June 2021) was characterized by a stationary mortality rate and decreasing lethality rate, with a DPC of - 0.37%. However, it is emphasized that the incidence remains with increasing trends illustrating the possibility of further contamination and subsequent wave formations.
Also, in this period, specifically from March to June 2021, there was a predominance of mortality, with 50.4% of all deaths that occurred since the pandemic in Brazil. In the distribution of mortality due to COVID-19, it was observed that in April, there were 82,401 victims, March with 66,868, May with 58,679, and June with 55,280 deaths per 100,00 inhabitants.
The event of the second wave of COVID-19 in Brazil was more lethal. In the State of EspíritoSanto, there were 586 deaths in June, 1,206 deaths in May, 2,024 deaths in April, which was more aggressive than the first, with a peak of incidence in March, and a rise of mortality and lethality in April 2021. Until July 17, 2021, Brazil was the sixth country with the highest mortality rate, after Peru, Mexico, Afghanistan, Tunisia, and South Africa.
As limitations to this study, it is emphasized that the statistical /epidemiological monitoring of COVID-19 continues to be challenging due to disparities in access to official data and, significantly, in different locations, social groups, as well as divergence of data in the first months on any cumulative indicator of cases. In addition, the use of variables, such as the number of hospitalizations, ICU admissions, and intubations, is restricted in different scenarios, limiting their usefulness for national global analysis. There is quiescence of these indicators in the Brazilian information repository (DATASUS), highlighted as a limitation of the study under discussion.
To our knowledge, this is the first work to comprehensively study the epidemiological profile of the State of EspíritoSanto, evidencing the formation of two possible waves. The findings of this study, such as the increasing trends in the incidence rate even after one year of pandemic, contribute scientifically to a warning that prevention measures such as double facial masking and social distancing are reinforced even after vaccination.
Moreover, due to the limitations arising from incidence rates, which are dependent on the number of tests, the attributes of this study are also associated with the analyses of indicators related to the number of deaths. It is a more reliable indicator to reflect the size of the pandemic impact; data on fatalities are more comparable and faithful, although not entirely immune to underestimations; this finding characterizes a strong point in data analysis over epidemiological weeks from 2020 to June 2021. Another aspect of the importance of this study is in its state scope, in the sample size and territorial coverage carried out so far, the multidimensional nature of the research.
CONCLUSION
The State of Espirito Santo, during the period from March 2020 to June 2021, presented 524,496 accumulated cases and 11,516 deaths due to COVID-19, with an accumulated lethality of 2.19%, with mortality rates of 278.25 deaths per 100,000 inhabitants and an incidence of 12,672.71 cases per 100,000 inhabitants, with transmissibility suffering large fluctuations during the period.
Notifications of 126,981 comorbidities were recorded between the cases, and 12.324 were mentioned in the reports of deaths. Cardiovascular diseases (69,029 in cases and 6.055 in deaths), followed by diabetes (25,337 in cases and 3,228 in deaths), and obesity (11,855 in cases and 1,132 in deaths) were the most prevalent comorbidities. Moreover, male gender and advanced age have higher lethality and mortality rates, with male individuals aged 80 years or older presenting the highest rates: lethality (30.19%) and mortality (4,145.64 deaths per 100,000 inhabitants).
The epidemiological profile of COVID-19 in the State of Espirito Santo was characterized by the formation of two waves, which evidenced the incidence with increasing trends and a Daily Percent Change of 0.78% during the first wave and 2.06% during the second wave. Although the second wave (November 2020 to June 2021) presented decreasing trends in lethality (DPC = -0.33%) and stationary mortality, this period had the highest rates of all indicators here discussed, and the peak of incidence in March (1,618.57 new cases per 100,000 inhabitants), and lethality (4.51%), and mortality (48.90 deaths per 100,000 inhabitants) in April.
The pandemic is still in evolution in the State of Espirito Santo. Therefore, non-pharmacological measures, such as facial masking use, reduction of agglomerations, hand hygiene with soap and water or gel alcohol, as well as the reduction of movement of people in the State are still necessary measures to combat COVID-19, in addition to the advance of immunization with the Vaccine against SARS-CoV-2.
Author Contributions
Conceptualization, C.D.K.S., B.E.G.D., T.C.M., I.P., M.P.R.C. and L.C.A.; methodology, C.D.K.S., T.C.M., J.O.E., L.C.J., R.D.R., K.E., C.E.S. and L.C.A.; software, J.O.E., L.C.J.; validation, T.C.M., J.O.E., C.E.S. and L.C.A.; data curation, C.D.K.S., T.C.M., L.C.A.; writing-review and editing, all the authors; visualization, all the authors; supervision, K.E., C.E.S. and L.C.A.; project administration, C.E.S. and L.C.A. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Acknowledgments
we want to thank Célia Guarnieri da Silva for providing the map illustrated in this study and Henrique Moraes Ramos da Silva for his support in retrieving and han-dling the data.
Conflicts of Interest
the authors declare no conflict of interest.
REFERENCES
1.Pimentel RMM, Daboin BEG, Oliveira AG, Macedo JrH. The dissemination of COVID-19: an expectant and preventive role in global health. J Hum Growth Dev. 2020; 30(1): 135-140. DOI: https://doi.org/10.7322/jhgd.v30.9976 [ Links ]
2.Abreu LC. Integrated actions and strengthening of Public Health System in Brazil in a time of pandemic. J Hum Growth Dev. 2020; 30(1): 05-08. DOI: https://doi.org/10.7322/jhgd.v30.9980 [ Links ]
3.Silva CMS, Andrade AN, Nepomuceno B, Xavier DS, Lima E, Gonzales I, et al. Evidence-based Physiotherapy and Functionality in Adult and Pediatric patients with COVID-19. J Hum Growth Dev. 2020; 30(1): 148-155. DOI: http://doi.org/10.7322/jhgd.v30.10086 [ Links ]
4.Abreu LC. The path of humanity in the pandemic of COVID-19: the choice of the realistic, optimist or pessimist scenario. J Hum Growth Dev. 2021; 31(1): 05-08. DOI: http://dx.doi.org/10.36311/jhgd.v31.11683 [ Links ]
5.Brasil. Ministério da Saúde, Secretaria de Vigilância em Saúde, Departamento de Análise em Saúde e Vigilância de Doenças não Transmissíveis. Vigitel Brasil 2018: vigilância de fatores de risco e proteção para doenças crônicas por inquérito telefônico nas capitais dos 26 estados brasileiros e no Distrito Federal em 2018[internet]. [cited 2021 jul. 17]. Available from:<https://portalarquivos2.saude.gov.br/images/pdf/2019/julho/25/vigitel-brasil-2018.pdf [ Links ]
6.Addeo A, Friedlaender, A. Cancer and COVID-19: Unmasking their ties. Cancer Treatment Reviews. 2020; 88(102041). DOI: 10.1016/j.ctrv.2020.102041 [ Links ]
7.Gold MS, Sehayek D, Gabrielli S, Zhang X, McCusker C, Moshe B. COVID-19 and comorbidities: a systematic review and meta-analysis. Postgraduate Medicine. 2020; 132(8): 749-755. DOI: 10.1038/s41562-020-0928-4 [ Links ]
8.Wang Z, Deng H, Ou C, Liang J, Wang Y, Jiang M, Li S. Clinical symptoms, comorbidities and complications in severe and non-severe patients with COVID-19: a systematic review and meta-analysis without cases duplication. Medicine (Baltimore). 2020; 99(48): e23327. DOI: 10.1097/MD.0000000000023327 [ Links ]
9.Jain V, Yuan JM. Predictive symptoms and comorbidities for severe COVID-19 and intensive care unit admission: a systematic review and meta-analysis. International Journal of Public Health. 2020; 65; 533-546. DOI 10.1007/s00038-020-01390-7 [ Links ]
10.IBGE - Instituto Brasileiro de Geografia e Estatística, Diretoria de Pesquisas, Coordenação de Trabalho e Rendimento. Pesquisa Nacional de Saúde. 2013: percepção do estado de saúde, estilos de vida e doenças crônicas: Brasil, grandes regiões e unidades da federação. 2014 [internet]. [cited 2021 jul. 17]. Available from: https://biblioteca.ibge.gov.br/index.php/biblioteca-catalogo?id=291110&view=detalhes [ Links ]
11.BRASIL. Ministério da Sáude. Painel de casos de doença pelo coronavírus 2019 (COVID-19) no Brasil pelo Ministério da Saúde. Versão 2.0[internet].[cited 2020 jul. 27]. Available from: https://covid.saude.gov.br/ [ Links ]
12.World Health Organization. Non-communicable diseases country profiles 2018. Geneva: WHO; 2018 [Internet]. [cited 2021 fev. 18]. Available from: https://www.who.int/nmh/publications/ncd-profiles-2018/en/ [ Links ]
13.Mesenburg MA, Hallal PC, Menezes AMB, Barros AJD, Horta BL, Barros FC, Hartwig FP, Jacques N, Silveira MFD. Chronic non-communicable diseases and COVID-19: EPICOVID-19 Brazil results. Rev Saude Publica. 2021; 2; 55:38. DOI: 10.11606/s1518-8787.2021055003673 [ Links ]
14.ESPÍRITO SANTO. Secretaria Estadual de Saúde. Covid-19 NOVO CORONAVÍRUS (COVID-19) INFORME EPIDEMIOLÓGICO - SEMANA 26. 2021a [internet]. [cited 2021 jul. 03]. Available from: https://saude.es.gov.br/Media/sesa/coronavirus/Boletins/Boletim%20Covid-19%2062.pdf [ Links ]
15.ESPÍRITO SANTO. Secretaria Estadual de Saúde, Brazil[internet]. [cited 2021 jul. 18]. Available from: https://coronavirus.es.gov.br/ [ Links ]
16.Malta DC, Duncan BB, Barros MBA, Katikireddi SV, Souza FM, Silva AG, Machado DG, Barreto ML. Medidas de austeridade fiscal comprometem metas de controle de doenças não transmissíveis no Brasil. Ciências Saúde Coletiva. 2018; 23(10): 3115-3122. DOI: 10.1590/1413-812320182310.25222018 [ Links ]
17.Abreu LC, Elmusharaf K, Siqueira CEG. A time-series ecological study protocol to analyze trends of incidence, mortality, lethality of COVID-19 in Brazil. J Hum Growth Dev. 2021; 31(3):491-495. DOI: 10.36311/jhgd.v31.12667 [ Links ]
18.Instituto Brasileiro de Geografia e Estatística. Cidades e Estados[internet]. [cited 2021 jun. 15] Available from: https://www.ibge.gov.br/cidades-e-estados [ Links ]
19.Sistema IBGE de Recuperação Automática. Banco de Tabelas estatística [Internet]. [cited 2021 jun. 15]. Available from: https://sidra.ibge.gov.br/home/ipp/brasil [ Links ]
20.Cori A, Ferguson NM, Fraser C, Cauchemez S. A new framework and software to estimate time-varying reproduction numbers during epidemics. Am J Epidemiol. 2013; 178(9): 1505-1512. DOI: 10.1093/aje/ kwt133 [ Links ]
21.Thompson RN, Stockwin JE, van Gaalen RD, Polonsky JA, Kamvar ZN, Demarsh PA, Dahlqwist E, Li S, Miguel E, Jombart T, Lessler J, Cauchemez S, Cori A. Improved inference of time-varying reproduction numbers during infectious disease outbreaks. Epidemics. 2019; 29: 100356. DOI: 10.1016/j. epidem.2019.100356 [ Links ]
22.Prete CA, Buss L, Dighe A, Porto VB, da Silva Candido D, Ghilardi F, Pybus OG, de Oliveira WK, Croda JHR, Sabino EC, Faria NR, Donnelly CA, Nascimento VH. Serial interval distribution of SARS-CoV-2 infection in Brazil. J Travel Med. 2021; 28(2): taaa115. DOI: 10.1093/jtm/taaa115 [ Links ]
23.Ali ST, Yeung A, Shan S, Wang L, Gao H, Du Z, Xu XK, Wu P, Lau EHY, Cowling BJ. Serial intervals and case isolation delays for COVID-19: a systematic review and meta-analysis. Clin Infect Dis. 2021;26:ciab491. DOI: 10.1093/cid/ciab491. Epub ahead of print. [ Links ]
24.DATASUS. Informações de Saúde (TABNET) - Demográficas e Socioeconômica. População residente[internet]. [cited 2021 jul. 20]. Available from: http://www2.datasus.gov.br/DATASUS/index.php?area=0206&id=6942 [ Links ]
25.Antunes JLF, Cardoso MRA. Uso da análise de séries temporais em estudos epidemiológicos. Epidemiol Serv Saúde 2015; 24(3): 565-576. DOI:10.5123/S1679-49742015000300024 [ Links ]
26.Prefeitura Municipal de Vitória. 1º Informativo coronavirus (COVID-19)[internet].[cited 2021 jul. 29] Available from: https://www.vitoria.es.gov.br/arquivos/20200403_boletim01coronavirus.pdf?1623880077 [ Links ]
27.Catão RC, Ribeiro FAS, Veltem CPCC, Freitas MH, Chrisostomo FC. Difusão espacial da covid-19 no espírito santo: uma abordagem inicial. Hygeia - Revista Brasileira de Geografia Médica e da Saúde. 2020; Edição Especial: Covid-19;349 - 360. DOI 10.14393/Hygeia0054639 [ Links ]
28.de Souza WM, Buss LF, Candido DDS, Carrera JP, Li S, Zarebski AE, Pereira RHM, et al. Epidemiological and clinical characteristics of the COVID-19 epidemic in Brazil. Nat Hum Behav. 2020; 4(8): 856-865. DOI: 10.1038/s41562-020-0928-4 [ Links ]
29.Stringari LL, de Souza MN, de Medeiros Junior NF, Goulart JP, Giuberti C, Dietze R, Ribeiro-Rodrigues R. Covert cases of Severe Acute Respiratory Syndrome Coronavirus 2: An obscure but present danger in regions endemic for Dengue and Chikungunya viruses. PLoS One. 2021; 6; 16(1): e0244937. DOI: 10.1371/journal.pone.0244937 [ Links ]
30.Harvey D, Davis M, Bihr A, Zibechi R, Badiou A, Zizek S. Política anticapitalista em tempos de COVID-19. In: Harvey D, Davis M, Bihr A, Zibechi R, Badiou A, Zizek S. CORONAVIRUS E A LUTA DE CLASSES. 2020. p. 13-24. [ Links ]
31.Yanez ND, Weiss NS, Romand JA, Treggiari MM. COVID-19 mortality risk for older men and women. BMC Public Health. 2020; 20(1): 1742. DOI: 10.1186/s12889-020-09826-8 [ Links ]
32.Wang D, Hu B, Hu C, Zhu F, Liu X, Zhang J, Wang B, Xiang H, Cheng Z, Xiong Y, Zhao Y, Li Y, Wang X, Peng Z. Clinical Characteristics of 138 Hospitalized Patients With 2019 Novel Coronavirus-Infected Pneumonia in Wuhan, China. JAMA. 2020; 323(11): 1061-1069. DOI: 10.1001/jama.2020.1585 [ Links ]
33.Luo L, Fu M, Li Y, Hu S, Luo J, Chen Z, Yu J, Li W, Dong R, Yang Y, Tu L, Xu X. The potential association between common comorbidities and severity and mortality of coronavirus disease 2019: A pooled analysis. Clin Cardiol. 2020; 43(12): 1478-1493. DOI: 10.1002/clc.23465 [ Links ]
34.Horn L, Garassino M. COVID-19 in patients with cancer: managing a pandemic within a pandemic. Nat Rev Clin Oncol. 2021; 18(1): 1-2. DOI: 10.1038/s41571-020-00441-5 [ Links ]
35.Jacobs J, Johnson AK, Boshara A, Hunt B, Khouri C, Cruz J, Glick N. COVID-19 health inequities and association with mechanical ventilation and prolonged length of stay at an urban safety-net health system in Chicago. PLoS One. 2021; 16(10): e0258243. DOI: 10.1371/journal.pone.0258243. [ Links ]
36.Silva AWC, Cunha AA, Alves GC, Corona RA, Dias CAGM, Nassiri R, Vedovelli S, Araújo MHM, Souza KO, Oliveira E. de; Dendasck CV, Fecury AA. Clinical characterization and epidemiology of 1560 cases of COVID-19 in Macapá/AP, extreme north of Brazil. Research, Society and Development. 2020; 9(8); e150985499. DOI: 10.33448/rsd-v9i8.5499 [ Links ]
37.Oliveira, AA, Moreira DJS, Pimentel JAS, Costa PHM, Dias CAGM, Araujo MHM, Oliveira E, Dendasck CV, Souza KO, Fecury AA. Análise dos principais fatores de risco preexistentes em pacientes diagnosticados com a covid-19 no amapá, amazônia, brasil. Revista Científica Multidisciplinar Núcleo do Conhecimento. 2021;17;56-72, 2021. DOI: 10.32749/nucleodoconhecimento.com.br/saude/risco-preexistentes [ Links ]
38.Aghagoli G, Gallo Marin B, Soliman LB, Sellke FW. Cardiac involvement in COVID-19 patients: Risk factors, predictors, and complications: A review. J Card Surg. 2020; 35(6): 1302-1305. DOI: 10.1111/jocs.14538 [ Links ]
39.Almeida JS, Cardoso JA, Cordeiro EC, Lemos M, Araujo TME, Sardinha AHL. Caracterização epidemiológica dos casos de covid-19 no maranhão: uma breve análise. Revista Prevenção de Infecção e Saúde. 2020;6. DOI: 10.1590/SciELOPreprints.314 [ Links ]
40.Ferrari F. COVID-19: Dados Atualizados e sua Relação Com o Sistema Cardiovascular. Arq. Bras. Cardiol. 2020; 114(5): 823-826. DOI: 10.36660/abc.20200215 [ Links ]
41.Xiong TY, Redwood S, Prendergast B, Chen M. Coronaviruses and the cardiovascular system: acute and long-term implications. Eur Heart J. 2020; 14; 41(19): 1798-1800. doi: 10.1093/eurheartj/ehaa231 [ Links ]
42.Simoni L, Ceka A, Tajaf, E, Gina M, Dibra A, Goda A. Coronavirus disease 2019 (covid-19) pandemic and the "paradox" of acute coronary syndrome hospitalizations. Archives of the Balkan Medical Union. 2021; 56(1): 88-93. DOI: 10.31688/ABMU.2021.56.1.11 [ Links ]
43.Prasitlumkum N, Chokesuwattanaskul R, Thongprayoon C, Bathini T, Vallabhajosyula S, Cheungpasitporn W. Incidence of Myocardial Injury in COVID-19-Infected Patients: A Systematic Review and Meta-Analysis. Diseases. 2020; 8(4): 40. DOI: 10.3390/diseases8040040 [ Links ]
44.Modin D, Claggett B, Sindet-Pedersen C, Lassen MCH, Skaarup KG, Jensen JUS, Fralick M, Schou M, Lamberts M, Gerds T, Fosbol EL, Phelps M, Kragholm KH, Andersen MP, Kober L, Torp-Pedersen C, Solomon SD, Gislason G, Biering-Sørensen T. Acute COVID-19 and the Incidence of Ischemic Stroke and Acute Myocardial Infarction. Circulation. 2020; 142(21): 2080-2082. DOI: 10.1161/CIRCULATIONAHA.120.050809 [ Links ]
45.Stefan N, Birkenfeld AL, Schulze MB, Ludwig DS. Obesity and impaired metabolic health in patients with COVID-19. Nat Rev Endocrinol. 2020; 16(7): 341-342. DOI: 10.1038/s41574-020-0364-6 [ Links ]
46.Bornstein SR, Rubino F, Khunti K, Mingrone G, Hopkins D, Birkenfeld AL, Boehm B, Amiel S, Holt RI, Skyler JS, DeVries JH, Renard E, Eckel RH, Zimmet P, Alberti KG, Vidal J, Geloneze B, Chan JC, Ji L, Ludwig B. Practical recommendations for the management of diabetes in patients with COVID-19. Lancet Diabetes Endocrinol. 2020 Jun; 8(6): 546-550. DOI: 10.1016/S2213-8587(20)30152-2 [ Links ]
47.Martins-Chaves RR, Gomes CC, Gomez RS. Immunocompromised patients and coronavirus disease 2019: a review and recommendations for dental health care. Braz Oral Res. 2020; 34: e048. DOI: 10.1590/1807-3107bor-2020.vol34.0048 [ Links ]
48.Yang J, Zheng Y, Gou X, Pu K, Chen Z, Guo Q, Ji R, Wang H, Wang Y, Zhou Y. Prevalence of comorbidities and its effects in patients infected with SARS-CoV-2: a systematic review and meta-analysis. Int J Infect Dis. 2020; 94: 91-95. DOI: 10.1016/j.ijid.2020.03.017 [ Links ]
49.Gostic KM, McGough L, Baskerville EB, Abbott S, Joshi K, Tedijanto C, Kahn R, Niehus R, Hay JA, De Salazar PM, Hellewell J, Meakin S, Munday JD, Bosse NI, Sherrat K, Thompson RN, White LF, Huisman JS, Scire J, Bonhoeffer S, Stadler T, Wallinga J, Funk S, Lipsitch M, Cobey S. Practical considerations for measuring the effective reproductive number, Rt. PLoS Comput Biol. 2020; 16(12): e1008409. DOI: 10.1371/journal.pcbi [ Links ]
50.Bernal, HM, Siqueira CE, Adami F, Santos EFS. Trends in case-fatality rates of COVID-19 in the World, between 2019 - 2020. Journal of Human Growth and Development. 2020; 30(3): 344-354. DOI 10.7322/jhgd.v30.11063 [ Links ]
51.Ferreira, RV et al. COVID-19 NA REGIÃO DE SAÚDE TRIÂNGULO SUL, MG: UMA PERSPECTIVA CARTOGRÁFICA. Hygeia - Revista Brasileira de Geografia Médica e da Saúde, Edição Especial: Covid-19, p. 49 - 59, 2017. DOI 0.14393/Hygeia0054379 [ Links ]
52.Sy KTL, White LF, Nichols BE. Population density and basic reproductive number of COVID-19 across United States counties.2020; 13. DOI: 10.1101/2020.06.12.20130021 [ Links ]
53.WHO. 2020. Pulse survey on continuity of essential health services during the COVID-19 pandemic. Interim report World Health Organization 2020[internet]. Some rights reserved. This work is available under the CC BY-NC-SA 3.0 IGO license. WHO reference number: WHO/2019nCoV/EHS_continuity/survey/2020.1 [ Links ]
54.Kadkhoda K. Herd Immunity to COVID-19. Am J Clin Pathol. 2021; 155(4): 471-472. DOI: 10.1093/ajcp/aqaa272 [ Links ]
55.CAMPOS, GWS. O pesadelo macabro da Covid-19 no Brasil: entre negacionismos e desvarios. Trabalho, Educação e Saúde. 2020; 18(3). DOI 10.1590/1981-7746-sol00279 [ Links ]
 Correspondence:
Correspondence:
luizcarlos.deabreu@ul.ie
Manuscript received: september 2021
Manuscript accepted: october 2021
Version of record online: november 2021


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}