










Serviços Personalizados
Journal

artigo
 Inglês (pdf)
Inglês (pdf)
 Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
Indicadores
Compartilhar

 Permalink
PermalinkJournal of Human Growth and Development
versão impressa ISSN 0104-1282
Rev. bras. crescimento desenvolv. hum. vol.21 no.3 São Paulo 2011
ORIGINAL RESEARCH
Parents' death and its implications for child survival
Hani K. Atrash, M.D., M.P.H.
Division of Blood Disorders. National Center on Birth Defects and Developmental Disabilities Centers for Disease Control and Prevention, Atlanta, GA 30333. U.S.A.
ABSTRACT
Reduction of child mortality is a global public health priority. Parents can play an important role in reducing child mortality. The inability of one or both parents to care for their children due to death, illness, divorce or separation increases the risk of death of their children. There is increasing evidence that the health, education, and socioeconomic status of mothers and fathers have significant impact on the health and survival of their children.We conducted a literature review to explore the impact of the death of parents on the survival and wellbeing of their childrenand the mechanisms through which this impact is mediated. Studies have generally concluded that the death of a mother significantly increased the risk of death of her children, especially during the early years; the effect continues but is significantly reduced with increasing age through the age of 15 years. The effect of the loss of a father had less impact than the effect of losing a mother although it too had negative consequences for the survival prospect of the child. A mother's health, education, socioeconomic status, fertility behavior, environmental health conditions, nutritional status and infant feeding, and the use of health services all play an important role in the level of risk of death of her children. Efforts to achieve the Millennium Development Goal No. 4 of reducing children's under-5 mortality in developing countries by two thirds by 2015 should include promoting the health and education of women.
Key words: Maternal death; parent death; child survival; child mortality
INTRODUCTION
Under-5 child mortality continues to be an important public health problem and a serious challenge for developing countries. There continues to be a huge disparity in under-5 child mortality between high- and low-income countries, and many of these deaths are preventable. Most of the 8.1 million children who died before their fifth birthday in 2009 died in Africa and in low income countries1,2. In 2009, under-5 mortality rates (deaths per 1,000 live births) were 127 in Africa and 117 in low income coun-tries compared with 7 in high income countries1. Most children in developing countries continue to die from preventable or treatable causes, with pneumonia and diarrhea accounting for 18% and 15%, respectively, of all under-5 child deaths in 20081,2. Reducing under-5 child mortality has recently received attention as an important global challenge; the United Nations in 2000 included the reduction of under-5 child mortality as one of the Millennium Development Goals (MDGs)3. MDG-4 calls for reducing under-5 child mortality rates by 2015 by two thirds of the year 1990 rate3,4.
One approach to help achieve the MDG-4 is to ensure the ability of parents, especially mothers, to care for and protect their young children. The importance of the role of parents for the survival and wellbeing of their children has been recognized for many years.Although the loss of the mother, the father or both parents have been demonstrated to increase the risk of death of their children, it has been repeatedly documented that the loss of a mother carries more significant consequences than the loss of a father. Moreover, there is increasing evidence that the health, education, and socioeconomic status of mothers and fathers have significant impact on the health and survival of their children.
Analysis of historical data from Sweden, Canada, and the Netherlands all concluded that the death of a mother significantly increased the risk of death of her children5,6,7,8.In previous years, when maternal deaths were much more common than they are today,"Parent loss" discussions usually focused on the consequences to the children of the death of a mother during childbirth. Even today, it is common to hear health leaders around the world draw attention to the importance of maternal mortality by highlighting the impact of maternal death on children, families and communities. Statements like "Maternal death is a tragedy for individual women, for families, and for their communities" were repeated in many publications9.In recent years, however, the main causes of losing a parent have changed. Injuries and HIV/AIDS,which usually cause the death of young adults (15 to 59 years of age -parents of young, dependent children), are now among the top ten leading causes of death worldwide10. According to the World Health Organization, in 2004, HIV/AIDS was the leading cause of adult mortality in Africa, and injuries were the main cause of death for adult men in Latin America and the Caribbean10.
In developing countries today, early adulthood deaths create a significant social problem for orphaned children and their communities. In particular, the HIV epidemic has left millions of children without parents. It is estimated that in 2009, there were 16.6 million children 0-17 years of age who had lost their parents to AIDS - almost 90% of these children live in Sub-Saharan Africa11,12. Orphans with no family or community support face very risky life situations having no social network of families, lacking food and healthcare and sometimes having to assume the role of "heads of households" and taking care of their younger siblings.
We conducted a literature review to explore the impact of the death of parents on the survival of their children and explored the mechanisms through which the death of parents influenced the survival and wellbeing of their children.
METHODS
We conducted a review of the literature using PubMed13. PubMed comprises over 20 million citations for biomedical literature from Medline (published since 1940), life science journals, and online books. The database includes citations and abstracts from the fields of medicine, nursing, dentistry, veterinary medicine, the health care system, and preclinical sciences and it provides access to additional relevant Web sites and links to the other molecular biology resources13.
We searched the database for published English-language, full-size articles. The database was searched using relevant terms to identify publications pertinent to the subject of this manuscript. The principal terms used included: mother death, maternal death, maternal mortality, parent mortality, father death, parent death, orphan, orphanage, child death, childhood death, child survival, and child mortality. We reviewed the pertinent publications and included their findings in this manuscript.
RESULTS
Most of the work that we found concerning the death of parents and survival of their children has focused on death of children under-5 years of age. This is expected because, according to the World Health Organization, in 2004, under-5 child deaths accounted for 87.4% (10.4 million) of the estimated 11.9 million under-15 child deaths worldwide10. It is also important to note that much of the work in this area has come from historical data when death during childbirth was relatively common 5,6,7,8. In recent years, most of this work came from Africa where the largest proportion of child and "parents" deaths occurs. For example, although only 15% of the estimated world population lived in Africa in 2009, over 38% of the estimated 153 million orphans worldwide lived there11. Moreover, it is estimated that over 50% of the world's 8.1 million under-5 child deaths in 2009occurred in Africa11. According to the World Health Organization, in the African Regionin 2004, 46% of alldeaths were children aged under 15 years, 34% were people aged 15-59 years, and only 20% were people aged 60 years and over. Incontrast, in the high-income countries, only 1% ofdeaths were children aged under15 years, whereas84% were people aged 60 years and older10. Thus, proportionately many more children, especially those under 5 years of age, and parents of young children (15-59 years) die in Africa than in other parts of the World; consequently, researchers tend to focus their work on African countries because of the need for action and because the numbers are large enough to study and make conclusions.
Death of a mother and survival of her children:
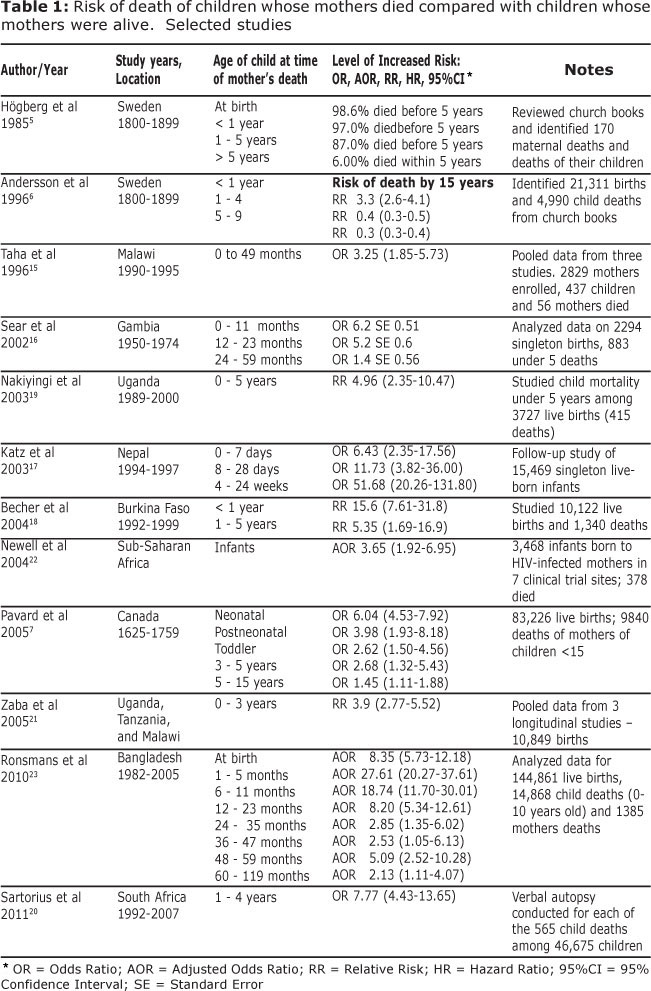
Several studies used historical data to examine the effect of a mother's death on the survival of her children. A study of survival of children born to mothers who died in childbirth during the 19 century in Sweden reported that, of those who lost their mothers at birth, 98.4% died before their fifth birthday; of children under the age of 1 when their mothers died, 97% died before their fifth birthday; and of children 1-5 years of age when their mother died 87% died during the following five years. However, of children who were over the age of 5 when their mother died, only 6% died during the following five years5. Another report from Sweden discussed survival of orphans in the 19th century and reported that being an orphan significantly reduced the chances of survival: 60% of motherless infants and 30% of fatherless infants died before their fifteenth birthday in comparison to 25% if both parents were alive6. Interestingly, this same reportconcluded that family reconstruction, whether achieved through kinship, remarriage, or foster care improved children's survival to levels similar to or above that of children with both parents alive6. A review of all maternal deaths in Quebec, Canada between the years 1625 and 1759 concluded that the risk of death was 6 times and 4 times higher for children who lost their mother during the neonatal and post-neonatal periods, respectively7. In the Netherlands, analysis of vital records for the years 1850 to 1930 indicated that the death of a mother resulted in a two times increased risk of death of her children when compared to children whose mothers and fathers were alive8.
Findings from more recent studies from Haiti14, Malawi15, Gambia16, Nepal17, Burkina Faso18, Uganda19, and South Africa20 as well as studies which pooled data from multiple African countries21,22 found similar results and concluded that a mother's death significantly increased the risk of death of her children.(Table 1) Overall most studies have also found that the effects of a mother's death on the survival of her children is greatest during the early years, especially the neonatal and post-neonatal periods17,18 and that the effect continues but is significantly reduced with increasing age through the age of 15 years7,16,18,21,22.In contrast, a study from Gambia concluded that the death of a mother had no impact on child survival after the age of 216. (Table 1)
Perhaps the definitive study of the relationship between a mother's death and the survival of her children is one published in 2010 from Bangladesh23. The study reviewed all maternal deaths as well as child deaths up to age 10 years in a rural area in Bangladesh from 1982 to 2005and included 144,861 live-births, 14,868 deaths of children younger than 10 years, and 1,385 deaths of mothers. Researchers concluded that children whose mothers died in the neonatal period were over 8 times more likely to die than were children whose mothers were alive. The death of the mother after the first month but before six months of lifeincreased child mortality by 27.6 times. The increased risk of children's death continued at all ages and was 18 times higher, 8.2 times higher, and 2.1 to 5.1 times higher if the mother died when the child was 6-11 months, 12-23 months, and 24 to 119 months old, respectively (Table 1). The proportions of children wholost their mothers and who died before their tenth birthday were: 86%, 61%, 32%, 19% and 2% if they lost their mothers at birth, 0 to 1 month, 1 to 6 months, 6 to 12 months and 12 to 60 months respectively. In comparison, the proportions of children whose mothers survived and who died during the respective age periods were: 11%, 7%, 5%, 4%, and 1% respectively23.
Death of a father and survival of his children:
Interest in the effects of the death of a father on child survival has increased recently because of the large number of orphans in countries with a high prevalence of HIV/AIDS11,12,15,21,22. The role of the father's death has been investigated in a few studies6,16,20,23.A historical study from Denmark concluded that the effect of the loss of a father was much lower than the effect of losing a mother although it too had negative consequences on survival of the child8. Another historical study from Sweden concluded that the loss of a father increased the risk of death slightly for infants (RR 1.5, 95% CI 1.0-2.1) but had no effect on survival of children 1 year or older at the time of father's death6. Similarly, a report from rural Gambia concluded that a father's death had no effect on child survival16, on the other hand, a study from South Africa reported that the death of a father either before a child's birth or during a child's first 4 years of life, is a significant factor in child mortality with a relative risk of 2.41 (95% CI 1.53-3.82)20.
Consistent with previous studies, the recent study from Bangladesh found that, in general, age-specific death rates were slightly higher in children whose fathers died than in those whose fathers had survived; however, the differences in mortality rates between children whose fathers died and other children for all age groups were not statistically significant23. The effect of father's death on the cumulative probability of survival in children up to age 10 years was also small. However, although there was no effect on the cumulative survival of children whose fathers died during the neonatal period (89% for both groups), there was a small but significant reduction of the cumulative survival of children who survived their neonatal period if their fathers died compared with those whose fathers were still alive (89% versus 93%)23.
Parents' death and the wellbeing of surviving children:
Following the death of a parent, children live with the surviving biological parent or live with the surviving parent and a step-parent. Some children are cared for by other members of the family or by adoptive parents, or are placed in an orphanage or are left homeless. Research has shown that most children who survive their parents' death suffer from negative consequences independent of who cares for them following the death of their parent.
In Bangladesh, children aged 6-12 years in families where a parent died, were significantly more likely to be uneducated and out-of-school after the death of a father or a mother compared to children in families where neither of the parents died independent of the educational status of the parents who died24.Findings of the study showed that the negative impact was more pronounced among children of poor families, and that female children were most severely affected. Moreover, death of a father or mother was associated with a higher rate of out-migration (especially marriage) of adolescent daughters24. A study from Uganda reported that children living with widowed fathers and those living on their own were significantly more depressed, and that children of all ages were likely to drop out of school when their parents became sick or died25.In Rural Uganda, children aged 11-15 years whose parents (one or both) were reported to have died of AIDS were at greater risk of higher levels of anxiety (OR 6.4) depression (OR 6.6), and anger (OR 5.1)26.
Adopted children were also found to suffer a negative impact of the death of their parents. A study from Missouri, United States, reported that the risk of maltreatment death was elevated for children residing with step, foster or adoptive parents (4.7 times)27. In Uganda, most children when they were adopted felt angry and depressed25. In China, children whose parents died of HIV/AIDS and who lived in orphanages mostly felt that the living conditions were better than the families they lived with after the death of their parents. However, institutional care had some disadvantages such as administrative restraints, limited psychological guidance, stigma, lack of education on AIDS, and financial burden of the operation28. In another study in China of HIV/AIDS orphans living in orphanages, a significantly higher proportion of orphans reported their relationship with peers became worse after parental illness or death than non-orphans29.In Zimbabwe, orphans had more psychosocial distress than did non-orphans. For both genders, paternal, maternal and double orphans exhibited more severe distress and were significantly more likely than were non-orphaned, non-vulnerable children to have engaged in sexual activity30.
Family structure - Restructure:
Studies suggest that family "reconstruction" through re-marriage reduces the risk of child death caused by the loss of a parent. Analysis of data from 19th century Sweden concluded that step-parents had a significant effect on improving the survival of children; the cumulative mortality to 15 years of motherless infants who got a stepmother decreased from 60% to 15%6. Simi-larly,the cumulative mortality to 15 years of fatherless infants who got a stepfather decreased from 30% to zero6.In nineteenth century Denmark, it was found that remarriage of the widow or widower resulted in a child death rate that was not different from that of children in complete families8. In the West Bank, most men had remarried shortly after the death of their wives and a stepmother had joined the family in 85% of the cases. All orphans who could be reached were alive. The authors concluded that early family reconstruction is suggested to be a contributing factor to the high survival rate31. A study from Fin-land reported that, compared with children to married parents, children of single parents carried an excess risk in mortality in ages 1-4 (Hazard Ratio 2.02) and in ages 5-9 (Hazard Ratio 1.44)32. In Denmark, remarriage of the widow or widower resulted in a child death rate similar to that of children with complete families8. In Bangladesh, researchers reported that the chances of survival were always lower for children of divorced mothers than for those non-divorced mothers33. As in the case of the mother's death, the effect of mother's marital stability on child survival was greater during infancy than during childhood33.
Studies from some developed, industrialized countries suggest that the family composition and the relationship of adults living in a household may be a risk to orphaned children. A report from Missouri, United States concluded that children residing in households with adults not related to them were 8 times more likely to die of maltreatment than children in households with 2 biological parents27. Children residing in households with unrelated adults were nearly 50 times as likely to die of inflicted injuries as were children residing with 2 biologic parents34. In Sweden, children of teenage mothers were at an increased risk of hospital admissions for violent as well as unintentional injury35. Finally in Finland, there was no difference in mortality among children in cohabiting-parent families compared with children of married parents32. Mainly due to accidental and violent causes of death, the largest excess mortality risks concentrated among children of single,less-educated and less earning parents32. The most vulnerable age period in this respect was early childhood (1-4 years old), whereas no association between mortality and family type was found among children aged 10-14 years32.The relationship between single parenthood and mortality was largely, but not entirely, explained by associated low parental education and lower household income32.
DISCUSSION
Reducing childhood mortality continues to be a public health priority around the world. Parents can play a very important role in reducing illness and death among their children if they were able to protect them and provide them with proper care. At worst, a parent's death deprives children of this protection and care and places them at an increased risk. The inability of parents to provide protection and care for their children may also be caused by their illness or their absence because of divorce or separation. Studies over the years have consistently reported that, when a mother dies, her children are at significantly increased risk of death. This risk is highest during the early years (under 5 years of age) when the child is very vulnerable and dependent on his mother for care, nutrition and protection (Table 1). The loss of the father has a similar effect but to a much lesser extent. Why does a parent's loss have a negative impact on the survival and wellbeing of their children? The answer is that most deaths among children, especially in developing countries, are preventable and the protection of children against harm and death is very much dependent on the presence of healthy parents who know how and can afford to protect their children.
Many factors contribute to the increased risk of child mortality. Researchers have for a long time grouped these factors into five major risk groups: socioeconomic status (e.g. financial assets, education, quality of water and sanitation facilities, housing conditions), fertility behavior (e.g., parity, birth spacing), environmental health conditions (e.g., exposure to toxic substances, clean water, sanitation, hand washing with soap and other practices related to child care), nutritional status and infant feeding (e.g.,breastfeeding and complementary feeding practices), and the use of health services (e.g., distance from services, affordability, service utilization)1,18. Specific factors which compound the above contributors and further increase the risk of child mortality have been identified by studies from various countries. These factors include poor maternal education36,37, lack of exclusive breastfeeding in the first 3 months23,37,38, lack of immunization39 and low socioeconomic status20,37,40,41,42,43, maternal age, birth order, and the length of the previous and following birth intervals44,45, parity >5, distance from health center and invalidating maternal illness46,47and teenage pregnancies19,45.In 2008, UNICEF reported that, across all regions, under-5 mortality was higher in rural areas, among less educated women, and in the poorest households2.The immediate causes of death reported in studies from different countries include respiratory infections and diarrhea20,47,48,49,50, malnutrition20,drowning, neonatal tetanus and measles49,50.
Most of the above factors are dependent on the parents' socioeconomic and educational status, and, in many cases, may be under the control of the parents. Thus, the absence of parents because of death, divorce, separation or serious illness is likely to reduce the level of protection of children against harm and have a serious negative impact on the health and survival of the children, especially the young children and especially in poor settings where "replacement" care and support may not be available. For young infants, the presence of the mother is critical where breastfeeding is the norm51.Children to mothers who are in poor health were found to have a higher risk of death than children whose mothers were healthy15,17,19,20,21. For example, analysis of data from Uganda, Tanzania, Malawi, and South Africa indicates that children whose mothers were HIV-positive were at significantly increased risk of death15,19,20,21.
Compromised ability of parents to have positive and intimate interactions with their children can cause detachment and maltreatment or even unexpected death among offspring. A 2005 meta-analysisof studies published since 1960 generally indicated a twofold higher risk of fetal death/stillbirth among offspring of women with psychosis52. In Taiwan, children whose mothers suffered from postpartum depression53, mental illness54, or affective disorders55had a significantly higher risk of death. In Denmark, children whose parents were admitted with any type of psychopathology and children whose mothers or fathers suffered from schizophrenia had a significantly higher risk of child death56. Another study from Denmark reported a 5 to 10 times increased risk of homicide among children of psychiatric inpatients57.
Maternal education has been shown to be a very important factor that reduces the risks of childhood mortality independent of other risk factors36,37,41,58,59,60,61. It is assumed that one way a mother's education improves child survival is because education enhances knowledge about effective ways to prevent, recognize and treat childhood diseases41.In a review of the literature, Cleland et al concluded that on average each one-year increment in mother's education corresponds with 7-9% decline in under-5 mortality59, and that even after adjusting for economic factors, 1-3 years of schooling was associated with a fall of 20% in childhood risks of death. In Guatemala and India,children with the most educated parents were found to experience substantially lower levels of mortality36,44.Father's education has also been found to have a positive impact on child survival, although to a lower extent than mother's education41,50,58,60,61,62. The influence of father's education is assumed to be largely through his socioeconomic status and contributions41,62. Father's support in child rearing was also shown to be an important factor in improving child survival50,63. Similarly, father's occupation and working status appear to be a major factor determining childhood mortality40,58.
Child mortality in developing countries is mainly associated with measurable socio-economic conditions such as poor living conditions. Poor children are more likely to be exposed to health risks,and have less resistance to disease because of malnutrition and other risk factors typical of poorer communities. These inequities are further compounded by reduced access to health care in the form of preventive and curative interventions. In low- and middle-income countries, the probability of dying in childhood is strongly related to the socio-economic position of theparents or household in which the child is born11,2,40,42.In the United States, children in the most deprived socioeconomic group had an overall mortality rate of approximately twice that of children in the least deprived socioeconomic group and an unintentional injury and homicide mortality rate 2.6 to 2.8 times higher than children in the least deprived socioeconomic group42. In New Zealand there was approximately 2 fold increased risk of mortality among the lowest compared with the highest socioeconomic categories of education, income, car access, and neighborhood deprivation43.
CONCLUSION
The death of parents has a significant negative impact on the wellbeing and survival ofyoung children, especially those who are young and most vulnerable (under 5 years old). The death of a mother has a much more significant impact and is associated with a 2 to 50 times increase risk of death among the under-5 children she leaves behind. The obvious immediate result of a woman's death is the loss of her contribution to her family and her community: maintaining the household, providing nutrition, protecting the health and facilitating education of children, and earning income. Furthermore, the absence of a mother because of ill health, divorce, separation or her inability to "protect" her children for lack of education or poverty also affects the wellbeing and survival of her children. Thus, an important contributor to under-5 child mortality in developing countries is the health and education of women. Improving the health and education of women is an important step towards achieving the MDG-4 of reducing under-5 mortality.
REFERENCES:
1. World Health Organization. World Health Statistics 2011. Available from:http://www.who.int/whosis/whostat/2011/en/index.html [ Links ]
2. UNICEF. Progress for children: achieving the MDGs with equity. Number 9, September 2010. Available from: http://www.unicef.org/publications/files/Progress_for_Children-No.9_EN_081710.pdf [ Links ]
3. United Nations Resolution 55/2: United Nations Millennium Declaration; September 18, 2000. Available from: http://www.un.org/millennium/declaration/ares552e.pdf [ Links ]
4. United Nations (2000). Millennium Development Goals. Available from:http://www.development-goals.com [ Links ]
5. Högberg U, Broström G. The demography of maternal mortality-seven Swedish parishes in the 19th century.Int J Gynaecol Obstet. 1985;23(6):489-97. [ Links ]
6. Andersson T, Högberg U, Akerman S. Survival of orphans in 19th century Sweden-the importance of remarriages. ActaPaediatr. 1996;85(8):981-5. [ Links ]
7. Pavard S, Gagnon A, Desjardins B, Heyer E. Mother's death and child survival: the case of early Quebec.J Biosoc Sci. 2005;37(2):209-27. [ Links ]
8. Beekink E, Van Poppel F, Liefbroer AC. Surviving the loss of the parent in a nineteenth-century Dutch provincial town. Journal of Social History. 1999; 32(3): 641-669. [ Links ]
9. Department of Reproductive Health and Research, WHO. Reduction of maternal mortality: a joint WHO/UNFPA/UNICEF/World Bank statement.1999. Available from: http://www.who.int/reproductivehealth/publications/ monitoring/9789241561952/en/index.html [ Links ]
10. World Health Organization.The global burden of disease: 2004 update. 2008. Available from: http://www.who.int/healthinfo/global_burden_disease/GBD_report_2004update_full.pdf [ Links ]
11. UNICEF. The state of the world's children 2011: Adolescence: an age of opportunity. Available from: http://www.unicef.org/sowc2011/pdfs/SOWC-2011-Main-Report_EN_02092011.pdf [ Links ]
12. Joint United Nations Program on HIV/AIDS (UNAIDS). Global report: UNAIDS report on the global AIDS epidemic 2010. Available from: http://www.unaids.org/documents/20101123_GlobalReport_em.pdf [ Links ]
13. PubMed. Available from: http://www.ncbi.nlm.nih.gov/books/NBK3827/#pubmedhelp.FAQs [ Links ]
14. Anderson FW, Morton SU, Naik S, Gebrian B. Maternal mortality and the consequences on infant and child survival in rural Haiti.Matern Child Health J. 2007; 11(4): 395-401. [ Links ]
15. Taha TE, Miotti P, Liomba G, Dallabetta G, Chiphangwi J. HIV, maternal death and child survival in Africa.AIDS. 1996; 10(1): 111-12. [ Links ]
16. Sear R, Steele F, McGregor IA, Mace R. The effects of kin on child mortality in rural Gambia.Demography. 2002; 39(1): 43-63. [ Links ]
17. Katz J, West KP Jr, Khatry SK, Christian P, LeClerq SC, Pradhan EK, et al. Risk factors for early infant mortality in Sarlahi district, Nepal.Bull World Health Organ. 2003;81(10):717-25. [ Links ]
18. Becher H, Müller O, Jahn A, Gbangou A, Kynast-Wolf G, Kouyaté B. Risk factors of infant and child mortality in rural Burkina Faso.Bull World Health Organ. 2004 Apr;82(4):265-73. [ Links ]
19. Nakiyingi JS, Bracher M, Whitworth JA, Ruberantwari A, Busingye J, Mbulaiteye SM, et al. Child survival in relation to mother's HIV infection and survival: evidence from a Ugandan cohort study. AIDS. 2003; 17(12): 1827-34. [ Links ]
20. Sartorius B, Kahn K, Collinson MA, Vounatsou P, Tollman SM. Survived infancy but still vulnerable: spatial-temporal trends and risk factors for child mortality in the Agincourt rural sub-district, South Africa, 1992-2007. Geospat Health. 2011; 5(2): 285-95. [ Links ]
21. Zaba B, Whitworth J, Marston M, Nakiyingi J, Ruberantwari A, Urassa M, et al. HIV and mortality of mothers and children: evidence from cohort studies in Uganda, Tanzania, and Malawi. Epidemiology. 2005; 16(3): 275-80. [ Links ]
22. Newell ML, Coovadia H, Cortina-Borja M, Rollins N, Gaillard P, Dabis F, et al. Mortality of infected and uninfected infants born to HIV-infected mothers in Africa: a pooled analysis, Lancet. 2004; 364: 1236-1243. [ Links ]
23. Ronsmans C, Chowdhury ME, Dasgupta SK, Ahmed A, Koblinsky M. Effect of parent's death on child survival in rural Bangladesh: a cohort study. Lancet. 2010; 375: 2024-31. [ Links ]
24. Roy NC, Kane TT, Barkat-e-Khuda. Socioeconomic and health implications of adult deaths in families of rural Bangladesh.J Health PopulNutr. 2001; 19(4): 291-300. [ Links ]
25. Sengendo J, Nambi J. The psychological effect of orphanhood: a study of orphans in Rakai district.Health Transit Rev. 1997; 7 Suppl: 105-24. [ Links ]
26. Atwine B, Cantor-Graae E, Bajunirwe F. Psychological distress among AIDS orphans in rural Uganda. SocSci Med. 2005; 61(3): 555-64. [ Links ]
27. Stiffman MN, Schnitzer PG, Adam P, Kruse RL, Ewigman BG. Household composition and risk of fatal child maltreatment.Pediatrics. 2002; 109(4): 615-21. [ Links ]
28. Zhao Q, Li X, Kaljee LM, Fang X, Stanton B, Zhang L. AIDS orphanages in China: reality and challenges.AIDS Patient Care STDS. 2009; 23(4): 297-303. [ Links ]
29. Xu T, Wu Z, Duan S, Han W, Rou K. The situation of children affected by HIV/AIDS in Southwest China: Schooling, physical health, and interpersonal relationships.J Acquir Immune DeficSyndr. 2010; 53Suppl 1: S104-10. [ Links ]
30. Nyamukapa CA, Gregson S, Lopman B, Saito S, Watts HJ, Monasch R, et al. HIV-Associated Orphanhood and Children's Psychosocial Distress: Theoretical Framework Tested With Data From Zimbabwe Am J Public Health. 2008; 98(1): 133-141. [ Links ]
31. Al-Adili N, Shaheen M, Bergstrom S, Johansson A. Survival, family conditions and nutritional status of motherless orphans in the West Bank, Palestine. Scand J Public Health. 2008; 36(3): 292-7. [ Links ]
32. Remes H, Martikainen P, Valkonen T. The effects of family type on child mortality.Eur J Public Health. 2010 Nov 4. [Epub ahead of print] [ Links ]
33. Bhuiya A, Chowdhury M. The effect of divorce on child survival in a rural area of Bangladesh.Popul Stud. 1997;51:57-61. [ Links ]
34. Schnitzer PG, Ewigman BG. Child deaths resulting from inflicted injuries: household risk factors and perpetrator characteristics. Pediatrics. 2005; 116(5): e687-93. [ Links ]
35. Ekéus C, Christensson K, Hjern A. Unintentional and violent injuries among pre-school children of teenage mothers in Sweden: a national cohort study. J Epidemiol Community Health. 2004; 58(8): 680-5. [ Links ]
36. Simmons GB, Bernstein S. The educational status of parents, and infant and child mortality in rural North India.Health Policy Educ. 1982; 2(3-4): 349-67. [ Links ]
37. Armstrong Schellenberg JR, Nathan R, Abdulla S, Mukasa O, Marchant TJ, Tanner M,et al. Risk factors for child mortality in rural Tanzania. Trop Med Int Health. 2002; 7(6): 506-11. [ Links ]
38. Saha KK, Frongillo EA, Alam DS, Arifeen SE, Persson LA, Rasmussen KM. Appropriate infant feeding practices result in better growth of infants and young children in rural Bangladesh. Am J ClinNutr. 2008; 87(6): 1852-9. [ Links ]
39. Fantahun M, Berhane Y, Wall S, Byass P, Högberg U. Women's involvement in household decision-making and strengthening social capital-crucial factors for child survival in Ethiopia. ActaPaediatr. 2007; 96(4): 582-9. [ Links ]
40. Houweling TA, Kunst AE. Socio-economic inequalities in childhood mortality in low- and middle-income countries: a review of the interna-tional evidence. Br Med Bull. 2010; 93: 7-26. [ Links ]
41. Majumder AK, Islam SM. Socioeconomic and environmental determinants of child survival in Bangladesh. J Biosoc Sci. 1993; 25(3): 311-8. [ Links ]
42. Singh GK, Kogan MD. Widening so-cioeconomic disparities in US childhood mortality, 1969 2000. Am J Public Health. 2007; 97(9): 1658-65. [ Links ]
43. Blakely T, Atkinson J, Kiro C, Blaiklock A, D'Souza A. Child mortality, socioeconomic position, and one-parent families: independent associations and variation by age and cause of death. Int J Epidemiol. 2003; 32(3): 410-8. [ Links ]
44. Pebley AR, Stupp PW. Reproductive patterns and child mortality in Guatemala.Demography. 1987;24(1):43-60. [ Links ]
45. Mturi AJ, Curtis SL. The determinants of infant and child mortality in Tanzania. Health Policy Plan. 1995; 10(4): 384-94. [ Links ]
46. Van den Broeck J, Eeckels R, Massa G. Maternal determinants of child survival in a rural African community. Int J Epidemiol. 1996; 25(5): 998-1004. [ Links ]
47. Ibrahim MM, Omar HM, Persson LA, Wall S. Child mortality in a collapsing African society.Bull World Health Organ. 1996; 74(5): 547-52. [ Links ]
48. Adjuik M, Smith T, Clark S, Todd J, Garrib A, Kinfu Y, et al. Cause-specific mortality rates in sub-Saharan Africa and Bangladesh.Bull World Health Organ. 2006; 84(3): 181-8. [ Links ]
49. Baqui AH, Black RE, Arifeen SE, Hill K, Mitra SN, al Sabir A. Causes of childhood deaths in Bangladesh: results of a nationwide verbal autopsy study. Bull World Health Organ. 1998; 76(2): 161-71. [ Links ]
50. Agha A, Ajmal F, Iqbal A, White F. Father's support and literacy-factors associated with child mortality in Gambat, Sindh-Pakistan.J Pak Med Assoc. 2010; 60(2): 81-5. [ Links ]
51. Alam N, Saha SK, Razzaque A, van Ginneken JK. The effect of divorce on infant mortality in a remote area of Bangladesh. J Biosoc Sci. 2001; 33(2): 271-8. [ Links ]
52. Webb R, Abel K, Pickles A, Appleby L. Mortality in offspring of parents with psychotic disorders: a critical review and meta-analysis. Am J Psychiatry. 2005; 162(6): 1045-56. [ Links ]
53. Chen YH, Tsai SY, Lin HC. Increased mortality risk among offspring of mothers with postnatal depression: a nationwide population-based study in Taiwan. Psychol Med. 2011; 28: 1-10. [ Links ]
54. Chen YH, Chiou HY, Tang CH, Lin HC. Risk of death by unnatural causes during early childhood in offspring of parents with mental illness. Am J Psychiatry. 2010; 167(2): 198-205. [ Links ]
55. Liu TC, Chen CS, Loh CP. Do children of parents with mental illness have lower survival rate? A population-based study.Compr Psychiatry. 2010;51(3):250-5. [ Links ]
56. Webb RT, Abel KM, Pickles AR, Appleby L, King-Hele SA, Mortensen PB. Mortality risk among offspring of psychiatric inpatients: a population-based follow-up to early adulthood.Am J Psychiatry. 2006;163(12):2170-7. [ Links ]
57. Webb RT, Pickles AR, Appleby L, Mortensen PB, Abel KM. Death by unnatural causes during childhood and early adulthood in offspring of psychiatric inpatients.Arch Gen Psychiatry. 2007;64(3):345-52. [ Links ]
58. O'Toole J, Wright RE. Parental education and child mortality in Burundi. J Biosoc Sci. 1991; 23(3): 255-62. [ Links ]
59. Cleland JG, Van GinnekenJK.Maternal education and child survival in developing countries: the search for pathways of influence. SocSci Med. 1988;27(12):1357-68. [ Links ]
60. Kiros GF, Hogan DP. War, famine and excess child mortality in Africa: the role of parental education. Int. J. Epidemiol. 2001;30(3): 447-455. [ Links ]
61. Oliveira ZA, Bettiol H, Gutierrez MR, Silva AA, Barbieri MA. Factors associated with infant and adolescent mortality. Braz J Med Biol Res. 2007;40(9):1245-55. [ Links ]
62. Macassa G, Ghilagaber G, Bernhardt E, Diderichsen F, Burström B. Inequalities in child mortality in Mozambique: differentials by parental socio-economic position. SocSci Med. 2003; 57(12): 2255-64. [ Links ]
63. Bhuiya A, Binka FN, Maude GH, Gyapong M, Ross DA, Smith PG. Risk factors for child mortality in northern Ghana: a case-control study. Int J Epidemiol. 1995;24(1):127-35. [ Links ]
 Corresponding Author:
Corresponding Author:
hatrash@cdc.gov
Artigo submetido em 04.03.11, aceito em 29.07.11.
The author declares that hehas no conflicts of interest.
The findings and conclusions in this report are those of the author and do not necessarily represent the official position of the Centers for Disease Control and Prevention.


{kind=link}