










Serviços Personalizados
Journal

artigo
 Inglês (pdf)
Inglês (pdf)
 Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
Indicadores
Compartilhar

 Permalink
PermalinkJournal of Human Growth and Development
versão impressa ISSN 0104-1282
Rev. bras. crescimento desenvolv. hum. vol.22 no.1 São Paulo 2012
ORIGINAL RESEARCH
Prevalence and characteristics of women with a history of abortion among women who became pregnant
Rebeca de Souza e SilvaI; Marta Camila Mendes de Oliveira CarneiroI; Jefferson DrezettII; Solange AndreoniI
IDepartamento de Medicina Preventiva da Universidade Federal de São Paulo (UNIFESP)
IINúcleo de Violência Sexual e Aborto Previsto em Lei do Hospital Pérola Byington
ABSTRACT
OBJECTIVE: To evaluate the prevalence and characteristics of women with history of induced abortion among those who became pregnant, living in Vila Mariana, São Paulo, in 2006.
METHODS: This was a cross-sectional study involving 555 women, aged 15-49 with history of pregnancy. The women were classified as being without abortion (68.5%), with spontaneous abortion (22.7%) or induced abortion (8.8%). Age, education, number of live births, difference of number of children from the desired, and acceptance of abortion comprised the initial multinomial logistic regression model to describe the profile of women.
RESULTS: The odds ratio of having carried on without abortion induced abortion was 28.3 times (p<0.001) for those who had no children, 6.4 times (p<0.001) among those who accept abortion, and 4.9 times higher (p=0.002) in under 4 years of study, increased by 8% for each one year increment in age (p<0.001). The odds ratio of having a spontaneous miscarriage over without abortion was 15.0 times (p<0.001) for those who had no children; 3.6 times higher (p=0.055) in under 4 years of study, increased by 5% per year of age (p<0.001) and acceptance of abortion practice was not significant.
CONCLUSIONS: The main factor for the occurrence of abortion was not having live births, indicating a tendency of abortions to occur in the early reproductive life. Less education and acceptance of the practice were other variables associated with induced abortion. There was evidence of omission of the statement of abortion in the responses of the interviewees.
Key words: induced abortion; spontaneous abortion; logistic models; reproductive health.
INTRODUCTION
Induced abortion is an issue debated worldwide, whose motives and consequences affect women who decide to interrupt pregnancy1. Brazilian studies indicate difficulties in assessing accurately the levels and trends of induced abortion due to the obstacles and particularities in the process of obtaining the basic information2-5.
Those difficulties are tied to both the fact that it is an illegal and clandestine practice, as well as to the psychological, social, religious and cultural aspects associated with the subject. The stigma that permeates the termination of pregnancy can lead to deliberate omission of women when they are interviewed; often causing induced abortion to be hidden or to be declared as spontaneous.
This issue is also present in hospitalizations for post-abortion uterine evacuation that are performed through the Unified Health System in Brazil3. It is believed that a significant portion of medical care arises from non-informed induced abortions, either incomplete or with complications. The Alan Guttmacher Institute (1994)6 estimates that between 700 thousand and 1.4 million induced abortions occurred in Brazil in the early 90s, based on the assumption that the number of admissions for post-abortion complications is one third to one fifth of the total cases6.
Underreporting of abortion does not necessarily reflect their status as clandestine. Singh & Wulf (1994)7 found that in the American states where voluntary abortion is permitted, half of the women who had an abortion omitted this information when directly questioned7. Correa and Freitas (1997)8 suggested new scenarios from the correction factor applied to official records in order to minimize this obstacle.
The problem of underestimation has motivated the use of indirect techniques (IT) for data collection. Randomized response techniques, self-completion questionnaires or sealed ballot boxes allow better estimation of the prevalence of illegal abortion, because they provide the most appropriate conditions of secrecy and confidentiality. On the other hand, the use of IT restricts the characterization of the phenomenon, because they work with a limited number of questions5,9-12.
Most Latin American countries classify abortion as a crime, although some laws are permissive, as in the case of forced pregnancy by rape or to prevent the mother's death6. In Brazil, articles 124 to 128 of the Penal Code13 take into account these two aspects of abortion, corroborating to direct surveys to produce underestimated numbers. Silva (1998)9 showed that 80% of women hide induced abortions to unknown interviewers, a condition that is not differential by category or subgroup, allowing the use of cross-sectional studies to obtain more elaborate profiles of these women9.
The difficulty and high costs in obtaining the basic data are obstacles to epidemiological studies. Although Fusco et al (2008)2 consider that studies are more needed in vulnerable populations with high impact of abortion in the maternal morbidity and mortality rates, other initiatives to map those trends in the country should be considered.
Thus, the objective is to characterize and estimate the prevalences of women who had induced and spontaneous abortions among women of childbearing age with at least one pregnancy in a population of middle/high income.
METHODS
This study was part of the project "Integrality in Health", Department of Preventive Medicine of UNIFESP, funded by CNPq, process no 403258/2005-7, held in the region covered by Hospital São Paulo, subdistrict of Vila Mariana, focusing on epidemiology of induced abortion and their relationship with the local health services. The study was approved by the Research Ethics Committee of Universidade Federal de São Paulo (process number 0110/06).
This was a cross-sectional study carried out in women aged 15 to 49 years old with history of pregnancy, residing in the subdistrict of Vila Mariana, São Paulo, in 2006. The study sample consisted of 1121 women, of which 555 women had a history of pregnancy. The final sample size (555) provided a maximum error of 2% (0.02) in the estimation of a proportion of 0.088 (8.8%), assuming an infinite population.
We used a random sampling procedure often utilized in the assessments of immunization coverage, with low cost and compatible estimates with the ones obtained from simple random sampling14. The blocks of the subdistrict of Vila Mariana were numbered in circular clockwise order. Seventy-five blocks were randomly selected, and using the circular route and a casual start, their households should be covered until 16 interviews were completed. The procedure makes no provision for losses. Face to face interviews were carried out by trained female interviewers.
Each woman was classified into one of three mutually exclusive categories according to Abortion: Without Abortion, when the woman said she never had any kind of abortion; Spontaneous Abortion, when the woman declared at least one miscarriage and no induced abortion; and Induced Abortion, when the woman declared at least one induced abortion. The age of the woman at the time of the occurrence of the abortion events was not asked.
The independent variables were: Age, in complete years at the time of the interview; Gap, difference between number of live births and number of children considered ideal by the woman (categorized as Less than Ideal, Equal to Ideal, and Greater than Ideal); Employment (Yes if formal or informal, and No if no work, unemployed or retired); Education (completed years of study, at intervals of 0 to 4, 5 to 8, 9 to 11, 12 or more); Marital Status at time of interview (Single and Not Single - if married, engaged, separated, divorced or widowed); Current Use of Contraception Methods (None, Oral hormonal contraceptives or intrauterine device (IUD), Sterilization, and Others, if used any other method); Opinion on Induced Abortion (Accepted - at least one situation, Does Not Accept - in no situation); and Number of Live Births (None, One or More).
For data analysis, frequency tables were constructed to cross-classify the women based on abortion and the independent variables. The generalized likelihood ratio chi-square test was performed to investigate possible associations between having or not some kind of abortion with each of the independent variables.
Multinomial logistic regression models were used to determine which of the independent variables best describe the abortion status of these women. The odds ratios of women with spontaneous abortion on women without abortion, and women with induced abortion on women without abortion were calculated over a reference class, as well as their 95% confidence intervals. The backward procedure for removing variables was used to obtain the final model in order to include variables only with observed significance lower than 5% using the Wald chi-square test. Statistical analyses were performed with the SPSS program, version 15.0.
RESULTS
Among the 1121 women aged 15 to 49 years old, 555 (49.5%) reported at least one pregnancy. The median age of the 1121 women was 30.9 years and the median age of the 555 women was 37 years old. A total of 1266 pregnancies was observed, resulting in 1001 live births (79.1%); 175 spontaneous abortions (13.8%); 71 induced abortions (5.6%); 18 ongoing pregnancies (1.4%); and one stillbirth (0.1%). The mean number of children was 0.9 for 1121 women and 1.8 for the 555 women.
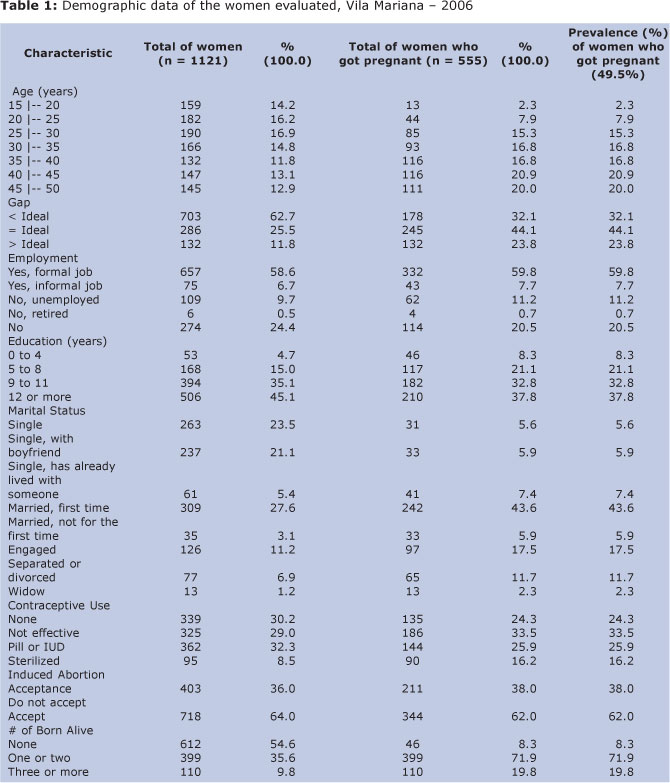
The profile of these women is presented in Table 1. It is observed that the total 1121 women interviewed were allocated proportionately in the five-year age groups considered. On the other hand, the number of women increases with age group among those with history of pregnancy. Most women work and have more than 8 years of education.
Table 1 also displays the prevalence of women that reported to have had at least one pregnancy. The prevalence increased with age group, with higher values occurring in women aged 35 or more. The highest prevalences of women with history of pregnancy occurred among those who had up to four years of study (86.8%), had been married, were sterilized or did not use contraceptive methods (Table 1).
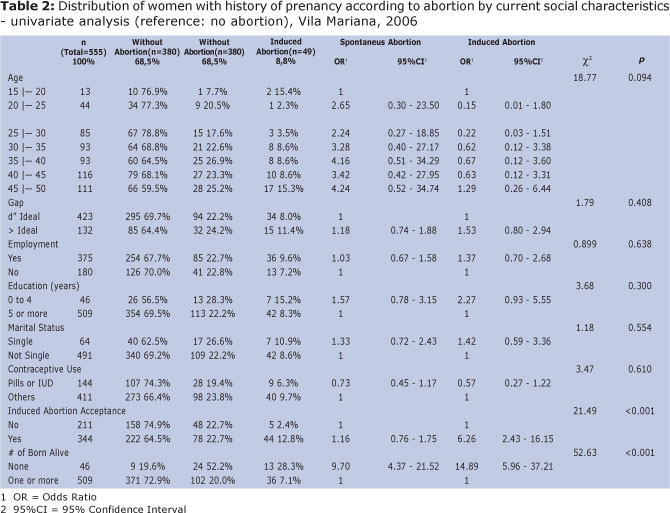
From the 555 women with history of pregnancy, 380 (68.5%) reported never having had any kind of abortion, 126 (22.7%) reported to have had at least one spontaneous abortion and no induced abortion, and 49 (8.8%) admitted to have had at least one induced abortion (Table 2). The analysis of the association of abortion with each independent variable showed that the acceptance of the practice of abortion and not to have any live births were strongly associated with induced abortion (Table 2).
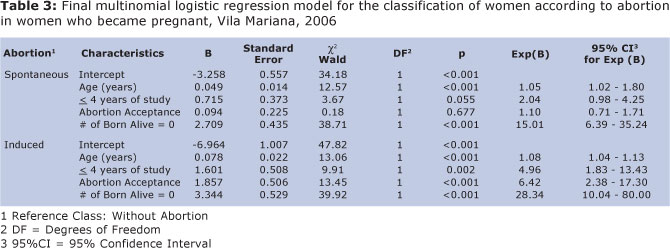
All independent variables were included in the initial logistic regression model. The results for the final model are presented in Table 3. The odds ratio of having induced an abortion over not having abortions was 28.3 times (p<0.001) among women with no live births, 6.4 times (p<0.001) for women who accept the practice of abortion, 4.9 times (p=0.002) among those with less than four full years of study, and increased by 8% for each one year increment in the age of the women (p<0.001). The odds ratio of having one or more spontaneous abortions over without abortion had a similar behavior. The odds ratio was 15 times (p<0.001) among women with no live births and two times (p=0.055) for women with less than four years of study, and increased by 5% for each one year increment in the age of the women (p<0.001). However, in this case, the odds ratio among women who accept abortion over the ones who totally reject the idea was not statistically significant (p=0.677). In summary, lower educational level was associated with a higher proportion of a history of pregnancy and abortions and not having a child was the variable with the greatest weight in the occurrence of abortion.
No not report of complications due to induced abortion was found in this study.
DISCUSSION
The subdistrict of Vila Mariana has privileged socioeconomic indicators, with a monthly income of around nine times the minimum wage and nearly 80% of the population with eight or more years of education. Data from Fundação Sistema Estadual de Análise de Dados15 indicate that the region is unique in the city of São Paulo, with an average of 1.5 children per woman in 2009, a figure that is similar to that of some European countries15.
With these indicators, it is possible to assume that a significant portion of the women living in the region has sufficient economic condition to resort to safe clandestine clinics to stop an unwanted pregnancy, with low risk of morbidity and mortality. At the same time, these women have more resources to develop strategies to if an abortion was performed, or to claim that the termination of an unwanted pregnancy was related to a spontaneous loss.
The low level of fecundity found in women living in Vila Mariana was consistent with data pointing the FSEADE - the late cusp to fecundity, with concentration of live births among women aged 30 to 40 years15. The same occurred on the age distribution, with most five-year age groups allocating a similar proportion of women with a median age of 30.9 years. In addition, the high proportion of women with eight or more years of study and reduced average number of 0.9 children per woman, were consistent with the low fertility15.
Studies conducted by Silva (1998)9 and Santos (2005)16 showed that women who seek induced abortion are young, unmarried, childless and in early reproductive life9,16. In this study, the abortion may have occurred at any time of the woman's reproductive life, prior to its statement. This limitation, however, can little distort the findings, since it is expected that the proportion of women with induced abortion at the beginning of reproductive life exceeds that of other ages.
Even for women with better socioeconomic conditions, the beginning of sexual and reproductive life is a more difficult moment to prevent pregnancy, either by the nature of casual relationships or by the lower prevalence of effective contraceptive use9. The National Survey on Demography and Health17, 1998, indicates that among couples with two living children, 90% of women and 88% of men do not want another pregnancy. Among couples with one child, 50% expressed intention not to enlarge the family17.
According to Sorrentino (2001)18, in a scenario where there are no adequate and safe practices to prevent pregnancy, and the national total fertility rate of 2.5 children per woman, the occurrence of unwanted pregnancies tends to be frequent. Although the proportion of pregnancies ending in miscarriage (13.8%) found in this study shows the expected, according to data of Barini et al. (2000)19, the value was 4.5 times greater than that observed for induced abortion, indicating the possibility of failure in the statements19. In addition, the prevalence of 4.3% for induced abortion proved to be far below other research reports in the region and the municipality of São Paulo9,10.
The number of induced abortions shows consistent decline in recent decades, a result of improvements in the quality of reproductive planning in the country. The socioeconomic indicators of Vila Mariana suggest that this population is among the most benefited by contraceptives advances. However, this factor seems insufficient to explain the lack of induced abortion statements found; even considering that part of the respondents went through the beginning of reproductive life for almost 30 years, when supply and access to contraceptives were more restricted. Thus, it is considered that part of the interviewees may have hidden induced abortion in their responses.
Women with a history of pregnancy had proportionately less education, possibly due to lower information about contraceptive methods or less access to regular and continuous use. This variable did not influence the position stated with respect to acceptance of induced abortion, a history of pregnancy being not against the practice. The data suggests that almost 60% of women could face an unintended pregnancy and resort to an illegal abortion. On the other hand, the history of not having a child born showed greater weight in the statement of abortion.
History of pregnancy was less common among younger women aged 20 years or less (8.2%). This finding reflects both the late onset of fertility recorded for the region evaluated, as it can indicate the strength not to report unintented pregnancies for younger women.
Assuming that the absence of such information is not differential by subgroups of women9, inferences that induced abortion has been deliberately concealed can be found in all groups of respondents. The prevalence of women with previous pregnancy that had practiced abortion showed to be lower than the expected, even considering a margin of error on the sampling process ranging from 6.8% to 10.8%. One can say that about 1/3 of abortions reported as spontaneous were in fact induced6.
Induced abortion is central in the debate on reproductive health since the 1990s, both in Brazil and in Latin America and the Caribbean. The consensus is that its criminalization and subsequent underground end up increasing maternal morbidity and mortality, especially for poorer women who perform abortions in unsanitary conditions6.
In Brazil, the official reason of maternal death is 76 for every 100,000 live births, mostly involving women with limited financial resources20. In fact, almost 80% of slum dwellers who resort to illegal abortions reported complications, especially bleeding2. In contrast, a study conducted by in São Paulo found 5% of women reporting some type of sequel9. In a research in Vila Madalena subdistrict, São Paulo, two complications were found in 20% of cases10. This evidence suggests that the higher socioeconomic level allows women to seek health services, although illegal, but perform abortions under less unsafe conditions. In this study, the interviewees did not report complications by induced abortion.
A recent study on the magnitude of abortion in Brazil, summarizing the major researches over the past 20 years shows that most women who terminate a pregnancy is between 20 and 29 years, stable, up to eight years of study, work, are Catholic, have at least one child and use some contraception12. In this investigation, however, it was expected a higher incidence of abortion among unmarried, young and childless women, considering the favorable socioeconomic profile of the population, as evidenced by Santos (2005)16.
In this respect, the results on the occurrence of abortions, induced or spontaneous, showed predominant among women who had no live birth. However, it was expected that miscarriages accompanied the profile of women with a pregnancy and were more frequent among those with a live birth. This finding is strongly suggestive that induced abortion may have been declared as spontaneous in the interviews.
Being young or unmarried was not important to explain the occurrence of induced abortion. It is possible that social changes have reduced the bias against young women who become pregnant before marriage, exerting less pressure to interrupt pregnancy. On the other hand, there was a greater tendency to postpone the first child's birth, particularly among women with higher income condition, interfering with the concentration of induced abortion among younger women. Confronted with unwanted pregnancy, more childless women resort to abortion, regardless marital status or age.
An important factor associated with induced abortion was accepting its practice in some situation, at least in those prescribed by legislation, with chance 6.4 times greater. Silva & Vieira (2009)21 found that single women living in São Paulo resort to abortion, even contrary to its practice21. This observation is not necessarily inconsistent.
According to Sihvo et al. (2003)22, socioeconomic factors and different types of relationships affect the decision to terminate the pregnancy. This decision may be different at each stage of a woman's life, referring to the social representations and perceptions of appropriate conditions for the exercise of motherhood.
The improvement and expansion of access to reproductive planning services to modern effective and safe contraceptives, sex and reproductive education programs, and public policies for gender equality are essential to avoid unwanted pregnancy. Still, there are not sufficient resources to eradicate this problem. Therefore, the decriminalization of abortion is a matter of public health and human rights, which guarantees equal access to health services that provide safe and humane conditions.
REFERENCES
1. Hardy E, Costa R, Rodrigues T, Moraes T. Características atuais associadas à história de aborto provocado. Rev Saúde Pública, 1994;28(1):82-5. [ Links ]
2. Fusco CLB, Andreoni S, Silva RS. Epidemiologia do aborto inseguro em uma população em situação de pobreza: Favela Inajar de Souza, São Paulo. Rev Bras Epidemiol 2008; 11(1):78-88. [ Links ]
3. Fonseca W, Misago C, Correia LL, Parente JAM, Oliveira FC. Determinantes do aborto provocado entre mulheres admitidas em hospitais em localidade da região Nordeste do Brasil. Rev Saúde Pública, 1996;30(1):13-18. [ Links ]
4. Osis MJD, Hardy E, Faundes A, Rodrigues T. Dificuldades para obter informações da população de mulheres sobre aborto ilegal. Rev Saúde Pública, 1996;30(5):444-51. [ Links ]
5. Silva RS. O uso da Técnica de Resposta ao Azar (TRA) na caracterização do aborto ilegal. Rev Bras Estudos Pop, 1993;10(1/2):41-56. [ Links ]
6. Alan Guttmacher Institute. Aborto clandestino: una realidad latinoamericana. Alan Guttmacher Institute [monografia en la Internet]. 1994 [citado 2006 Jul 13]. Disponível em: http://www.womenslinkworldwide.org/pdf/sp_proj_laicia_amicus_app_AGISP.pdf [ Links ]
7. Singh S, Wulf D. Estimated Levels of Induced Abortion in Six Latin American Countries. International Family Planning Perspectives, 1994;20:4-13. [ Links ]
8. Corrêa S, Freitas A. Atualizando os dados sobre a interrupção voluntária da gravidez no Brasil. Estudos Feministas, 1997;5(2):389-95. [ Links ]
9. Silva RS. Padrões de aborto provocado na Grande São Paulo, Brasil. Rev Saúde Pública. 1998; 32(1):7-17. [ Links ]
10. Silva RS, Fusco CLB. Saúde Reprodutiva, fecundidade e aborto provocado: análise de seis inquéritos populacionais realizados em São Paulo, Brasil. Rev Saúde Ética & Justiça, 2008;13(2):79-94. [ Links ]
11. Olinto MTA, Moreira Filho DC. Estimativa de aborto induzido: comparação entre duas metodologias. Rev Panam Salud Publica, 2004;15(5):331-6. [ Links ]
12. Diniz D. Aborto e Saúde Pública: 20 anos de pesquisas no Brasil. CFEMEA - Centro Feminista de Estudos e Assessoria [documento online]. 2009 [acesso em 05 jan 2009]. Disponível em: http://www.cfemea.org.br/noticias/detalhes.asp?IDNoticia=691 [ Links ]
13. Brasil. Código Penal: Decreto lei n. 1.004, de 21 de outubro de 1969. 4a ed. São Paulo: Saraiva; 1971. [ Links ]
14. Cardoso MRA. Comparação entre três métodos de amostragem que visam à estimação da cobertura vacinal [dissertação]. São Paulo: Faculdade de Saúde Pública da Universidade de São Paulo; 1990. [ Links ]
15. Fundação Sistema Estadual de Análise de Dados. Secretaria de Economia e Planejamento. Perfil Municipal de São Paulo, 2009 [documento online]. 2009. Disponível em: http://www.seade.gov.br/produtos/perfil/perfil.php [ Links ]
16. Santos EBC. Aborto induzido: ocorrência e características no antigo subdistrito de Vila Madalena, São Paulo, Brasil - 2000 [dissertação]. São Paulo: Universidade Federal de São Paulo. Escola Paulista de Medicina; 2005. [ Links ]
17. Sociedade Civil Bem-Estar Familiar no Brasil - BEMFAM. Relatório Preliminar. USA: London International Group; 1998. [ Links ]
18. Sorrentino SR. Aborto inseguro. In: Rede Nacional Feminista de Saúde e Direitos Reprodutivos. Saúde da mulher e direitos reprodutivos: dossiês. São Paulo: Rede Nacional Feminista de Saúde e Direitos Reprodutivos, 2001. p. 41-72. [ Links ]
19. Barini R, Couto E, Mota MM, Santos CTM, Leiber SR, Batista SCS. Fatores associados ao aborto espontâneo recorrente. Rev Bras Ginecol Obstet, 2000;22(4): 217-23. [ Links ]
20. Adesse L, Monteiro MFG. Magnitude do aborto no Brasil: Aspectos epidemiológicos e sócio-culturais. Instituto de Medicina Social - IMS [documento online]. 2008. Disponível em http://www.ipas.org.br/arquivos/factsh_mag.pdf 04 janeiro 2008. [ Links ]
21. Silva RS, Vieira EM. Aborto provocado: sua dimensão e características entre mulheres solteiras e casadas da cidade de São Paulo, Brasil. Cad Saúde Pública, 2009;25(1):179-87. [ Links ]
22. Sihvo S, Bajos N, Ducot B, Kaminski M. Women's life cycle and abortion decision in unintended pregnancies. J Epidemiol Community Health, 2003; 57(8):601-5. [ Links ]
 Corresponding author:
Corresponding author:
rebecaprev@globo.com
Manuscript submitted Oct 08 2011
Accepted for publication Feb 15 2012.

{kind=link}
{kind=link}
{kind=link}