










Serviços Personalizados
Journal

artigo
 Inglês (pdf)
Inglês (pdf)
 Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
Indicadores
Compartilhar

 Permalink
PermalinkJournal of Human Growth and Development
versão impressa ISSN 0104-1282
Rev. bras. crescimento desenvolv. hum. vol.23 no.1 São Paulo 2013
ORIGINAL RESEARCH
Prevalence of obesity and the body fat topography in children and teenagers with down syndrome
Fabio BertapelliI; José Irineu GorlaII; Fábia Freire da SilvaIII; Leonardo Trevisan CostaIV
IDoutorando em Saúde da Criança e do Adolescente, Faculdade de Ciências Médicas, Universidade Estadual de Campinas - FCM/UNICAMP/CAMPINAS
IIProf. Dr. do Departamento de Estudos da Atividade Física Adaptada - FEF/UNICAMP. Universidade Estadual de Campinas
IIIMestre em Educação Física, FEF/UNICAMP
IVDoutorando em Educação Física, FEF/UNICAMP
ABSTRACT
OBJECTIVE: to evaluate the prevalence of obesity and the body fat topography in children and adolescents from both sexes aged 6 to 19 years old with Down syndrome, residents in the city of Campinas, São Paulo.
METHODS: there were nine anthropometric measurements taken, including weight, height, and tricipital, bicipital, subscapular, suprailiac, abdominal, thigh, and calf skin folds. The fat percentage was determined by employing the prediction equations from Slaughter et al. Statistical analysis was performed using the computer package R Commander 1.6-3, with the descriptive statistics (median and 25th and 75th percentiles), the Mann-Whitney test, and the t-test for comparison between age groups, at the 5% (p 0.05) level.
RESULTS: most subjects had excess body fat, with the higher values being found among the females. The obesity was not a prominent characteristic among the boys, unlike the other age groups who had manifestations of elevated obesity. Regarding the body fat topography, most showed higher concentration of fat in the thigh, and smaller deposits in the biceps region. In the transition from childhood to adolescence, it was verifiable that boys and young men differ in the amounts of adipose tissue. However, no significant differences were observed among the girls, and the young women.
CONCLUSION: the assessment of the prevalence of obesity and subcutaneous fat topography are important resources to support researchers, and practitioners who work directly on improving the quality of life of children and adolescents with Down syndrome.
Key words: down syndrome; body composition; obesity; body fat distribution.
INTRODUCTION
It is known that excess body fat is associated with heart disease, diabetes, hypertension, and certain types of cancer1-3. Since the 80s, studies have shown a higher prevalence of obesity among the various populations in developed and developing countries4.
In children and adolescents with Down syndrome (DS), high obesity levels were also recorded from the 80's to the present days5,6. Thus, care with the obesity control in children and adolescents with DS should be redoubled, because excess body fat is one of the characteristics of the syndrome, which can seriously contribute to the increased incidence of several diseases.
Therefore, the study of the body fat behavior through the assessment of the body composition, occupies an important space in the identification of the levels of obesity in various populations, especially in children and adolescents with Down syndrome. Body composition is usually conceptualized as a designation given to represent the set of physical components, which make up the human body. In evaluative terms, generally, the physical components of children and adolescents are interpreted through the bi-compartmental model; i.e., the fat body mass is determined by fat percentage (BF %), and lean body mass (LBM), based on the development of equations for estimating body fat7.
There are fewer methods for estimating body fat in children and adolescents compared to the number of existing methods for adults, since ethical issues prevent the use of certain methods with this population. Among them, the photon absorption technique exposes the individual to radiation, the densitometry requires the individuals to be fully adapted to the liquid medium, the gamma ray spectrometry is impractical due to the high costs associated with the equipment, and the hydrometry requires an extended amount time for the determination of the body water contents. Moreover, there are other means that require more sophisticated technology, such as ultrasound, x-rays, computed tomography, creatinine excretion, bioelectric impedance, the total body electrical conductivity, the near infrared interactance, and the nuclear magnetic resonance8.
Given the inherent difficulties of applying the above methods of body fat estimation; the anthropometry tries to solve this problem, especially in the research involving populational surveys. Thus, the body fat estimate can be achieved by using equations involving skin fold thickness measurements. This method have being widely used in children and adolescents, (Durnin and Rahaman, Brook, Durnin and Womersley, Johnston and Slaughter et al.,)9. In DS children and adolescents, the Slaughter et al.,7 equation was the most accurate for determining the total body fat, because it was highly correlated with the air displacement method, employing the plestimographic wave9.
The measurement of the subscapularis and the tricipital skin fold thickness, are basic gauges for the total body fat determination. In addition, for the pattern analysis of the fat distribution on the various body parts, the measurements at various segments of the upper and lower body are essential10. Besides the obvious benefits of the skin fold measurements in determining BF %, there is also the possibility of obtaining information regarding the body fat topography; specifically directed to the study of fat distribution in the different regions of the body; thus, consolidating it as one of the most relevant techniques in the understanding of the body composition11.
Therefore, the objective is to estimate the prevalence of obesity in Down syndrome children and adolescents.
METHODS
The sample comprised 41 children and adolescents aged 6 to 19 years with DS, enrolled in specialized institutions located in the municipality of Campinas - SP. The convenience sampling was chosen because of the unknown characteristics of the sampled population. The selection included the largest available number of children and adolescents, from institutions agreeable to the research, in the age group established by the World Health Organization4. In healthy individuals (free of the Down syndrome), the most significant changes in the percentage of body fat start occurring around the twelve years of age12. Additionally, the early childhood and the puberty represent the most critical periods for changes in the adipose tissue13. Therefore, the sample was divided into two separated age groups (children: 6-12 years, and adolescents: 13-19 years).
The individual inclusion in the study followed these parameters: guardian's permission, acceptance during the measurements, and most of all, no health problems that could cause harm to the physical, or the psychological well-being of the volunteers. The study was approved by the Research and Ethics Committee from the School of Medical Sciences (FCM), at the State University of Campinas (opinion #1027/2009).
All data were collected with the accompaniment of a professional attached to the institution or, when such professional was unavailable, the parents were invited to stay during the entire process. Under no circumstances, the measurements were taken without the presence of a responsible party.
Measurements were performed by an experienced evaluator, preceded by the technical standards11. A Harpenden® skin fold caliper with a 0.2 mm resolution unit was employed in the skin fold measurement. The BMI was determined by dividing the body mass by the square of the height (Kg/m2). The body weight was achieved through a Plenna anthropometric scale with 100g of accuracy. The height was obtained using a stadiometer constructed from rigid PVC, containing a retractable steel measuring tape, with measuring length of 220 cm with exact scale of 0.1 cm, made by Seca. The percentage of body fat was determined by measuring the skin fold thickness of both the tricipital and the subscapular regions, using the proposed equations7.

The criteria used for the total body fat were set higher than 20% for the boys, and 30% for the girls, respectively for the classification of obesity14. The regional distribution of fat was analyzed by measuring seven skin folds (triceps - TR, biceps - BC, subscapular - SS, suprailiac - SI, abdomen - AB, thigh - T, and calf - C).
Statistical analysis were performed with the computerized package 1.6-3 R Commander (Rcmdr) from the R plus software, version 2.12.1. The possibility of using parametric or nonparametric tests was analyzed with the Shapiro-Wilk normality test. The t test or Mann-Whitney test was used to check for differences between the sexes in terms of age, weight, height, BMI, skin folds, sum of seven folds and fat percentage, at 5% (p d" 0.05), being used median values, 25th and 75th percentiles, and percentage frequencies.
RESULTS
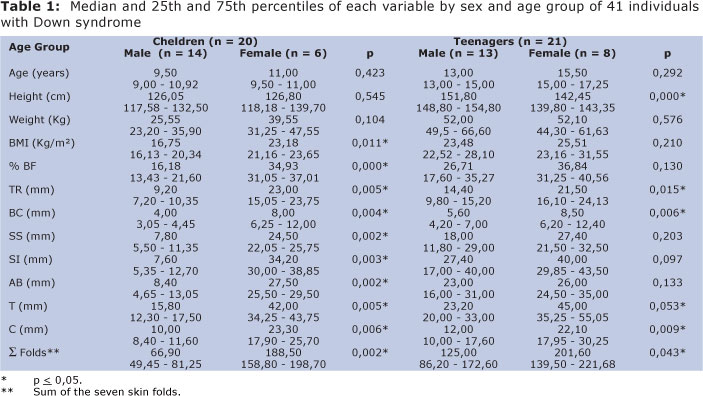
In the 6-12 age groups, there were statistically significant differences with the BMI, the BF %, all skin folds, and the sum of the seven folds, with the higher values being observed in the females. In the 13-19 age groups, females had significantly lower height, while the tricipital, bicipital, thigh, and calf skin folds, and the total sum total of the seven folds were significantly higher (Table 1).
Regarding the prevalence of obesity in the 6-12 age groups, 29% of the males, and 67% of the females were classified as obese. Among the 13-19 years old, 69% of the males and 88% of the females were obese.
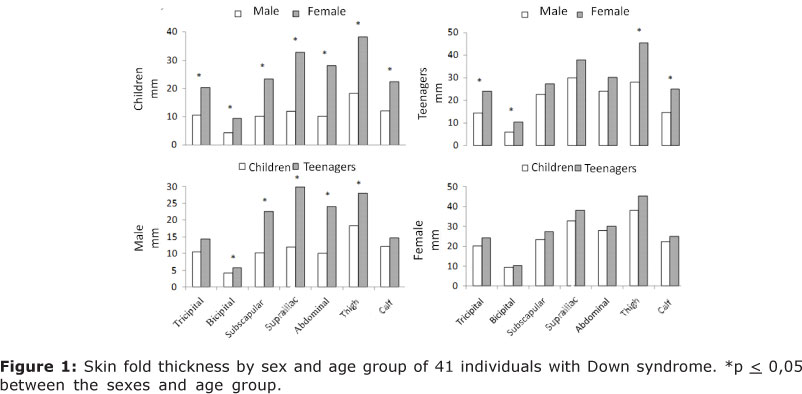
Figure 1 shows the fat topography in the 6-12, and the 13-19 years old groups. All age groups showed a higher concentration of subcutaneous fat in the thigh; with the exception of males in the 13-19 groups, who demonstrated a greater accumulation of fat in the trunk, specifically in the suprailiac skin fold, and the smallest tendencies to subcutaneous fat reserves occurred in bicipital fold in all the age groups.
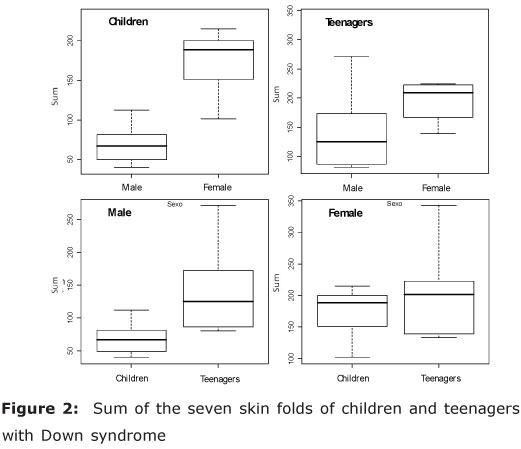
Overall, females in both age groups showed an increased amount of subcutaneous fat (Figure 2). Notably, the sum of seven folds appeared higher in the females. A lower amount of fat was verified among the 6-12 years old males. No significant differences were present among the females.
DISCUSSION
There were established cutoff points concerning the amounts of body fat relative to the body weight, which could lead to health risks, such as changes in blood pressure and dyslipidemia, with limits of 20% and 30% set for males and females, respectively14.
Based on the benchmarks suggested for the body fat percentages, an extremely high prevalence of obesity was observed among the individuals in all age groups, but for the male children. Similar results were found in other studies, with the prevalence of obesity in this population5.
These results may be explained with the analyzes of factors influencing the inadequate accumulation of body fat. Genetic, physiological, and environmental dysfunctions can lead DS children and adolescents to show a greater risk of becoming obese.
On the genetic aspect, studies point to the importance of the genes linked to mechanisms involving the accumulation of body fat15. The relationship between estrogen receptor gene (ER α) associated with the Pvull and Xbal polymorphisms, and the obesity in children with the syndrome indicates the genotype involvement with a predisposition to acquire high levels of fat tissue in this population16.
As for physiological changes, individuals with DS are at a higher risk of suffering cardiac and thyroidal alterations, protein hormone (leptin) dysfunctions, insulin resistance, low concentrations of zinc, high levels of triglycerides, and decreased basal metabolic rate17.
The environment plays a significant role as well. Specifically in relation to inadequate food consumption, parental attitudes toward good nutrition, and low levels of physical activity18. It is known that there is a strong relationship between obesity and energy imbalance, as evidenced by the association between caloric supply, from high calories foods, and the energy expenditure through physical activity19.
As for male children, most are not presented with high obesity. Some hypotheses can be raised from this observation, especially in relation to the physiological aspects, such as the absence of metabolic, cardiac and endocrine disorders. Another indication refers to the environmental aspect, mainly the with largest attendance in physical activity programs, and better eating habits compared to other age groups.
In regard to the topography of the subcutaneous fat in DS children and adolescents, the thigh region was predominant, with the greatest accumulation of fat cells in all age groups, except for the males adolescents. The bicipital skin fold reached the lowest fat index, compared to the other regions in all groups.
Regarding the trend of fat accumulating in the thigh area, there are indications of increased activity of the lipoprotein lipase in the adipose tissue, and of lipidic storage in the subcutaneous regions of the thighs and buttocks in females; thus, resulting in adipocyte hypertrophy, and the consequent predominance of fat in the lower body12. Moreover, there were no scientific evidence explaining the higher amounts of thigh subcutaneous fat in male children.
Costa20 conducted a study on body proportion in children and adolescents with DS, and with the application of the Cormic Index (CI) found that the lower limbs were proportionately shorter in relation to the trunk. Similarly, Velásquez-Meléndez et al.,21 demonstrated that a greater disproportionality verified with the CI, may represent a risk factor for increased deposition to subcutaneous fat; however, they did not specify the exact region with the greatest accumulation. Other studies verified a lower rate of lower limbs growth in fetuses with Down syndrome through tests conducted during prenatal testings, especially in the abnormal linear development of the femur; thus, becoming an object of study by several researchers22. Given these findings, it is arguable that greater amounts of subcutaneous fat located in the thigh can be explained by abnormalities in the linear growth of the femur in the DS population.
Regarding the adiposity in male adolescents, there was higher concentrations in the suprailiac region, indicating a slight centripetal tendency of body fat in young men. Studies seem to express greater concern regarding the central fat distribution patterns, because of the high correlation with diseases caused by metabolic and cardiovascular disorders23. In children and adolescent females, the suprailiac skin fold became the second region with the highest concentrations of adipose tissues, followed by the abdominal region. All age groups showed similar skin fold values for both the suprailiac, and the abdominal regions.
By comparing the folds values between the trunk and the limbs, the subscapular, suprailiac, and abdominal folds were balanced in children of both sexes and in female adolescents, as well as in the tricipital and calf regions.
In contrast, an analysis related to the sum of five skin folds located on the trunk (pectoral, subscapular, mid-axillary, abdominal and suprailiac), and in five folds of the limbs (triceps, biceps, forearm, thigh and calf) in healthy children and adolescents of both sexes, revealed that the sum of the skin fold located in the limbs was higher than those of the trunk in all age groups. When compared between the sexes, the differences were higher in the limbs than in the trunk12. In the present study sample, the differences between the sexes were also observed, and higher skin fold thickness values were found for all regions in female children. As for the teenagers, the adipose tissue behavior in the females resulted in larger amounts, only in relation to the tricipital and calf folds compared to the males.
Regarding the distribution of fat investigated in other studies, it was found that DS girls showed higher amounts of fat and lean mass in the trunk, compared to healthy girls; thus, suggesting a higher risk for developing cardiovascular disease. The males had higher levels of body fat, and lower amounts of lean mass in the upper and lower body5.
With respect to the transitional fat periods between childhood and adolescence, with the exception of the triceps and calf, all folds suffered statistically significant increases of subcutaneous fat in males. However, in relation to the females, despite the observed changes in the fat's composition, statistical tests did not show significant increases during the transition to puberty. Thus, the greatest concern resides in the extremely high levels of fat in females during childhood, with a lasting effect throughout the adolescence. It is known that to prevent obesity in the adulthood, it is vital to control the body fat during childhood, through adequate intakes of food, physical activity, and access to basic health services 7.
According to Guedes and Guedes13, there is a critical period of the adipose tissues development in children and adolescents, and with the early childhood, and puberty representing the major development periods. The greatest accumulation of body fat in healthy people can also be evidenced during pregnancy and the first months of life, beyond the early childhood and the puberty24. Unfortunately, few studies have investigated the critical periods of increased susceptibility to the accumulation of body fat in people with DS. According to Rogers et al.,25, the obesity observed in children with the syndrome, was a common problem evident from the age of two.
In general, girls and young women showed higher amount of body fat than boys and young men. By analyzing individual folds and observing the behavior of the sum of the seven folds, it was verified a higher sum in the females. Similarly, in the transition from childhood to adolescence, the sum of the skin folds behaved the same way in relation to the regional analysis, showing no significant differences between girls and young women. This information agrees with the results observed in DS children and adolescents from other studies, with higher values of total body fat and the sum of the abdominal, calf, thigh, suprailiac, subscapular, triceps and biceps skin folds in females compared to males6.
The adaptations in the adipose cells, the energy imbalance, the age at which this occurs, and the persistence of excess fat, are factors that may contribute to the increase in adipose tissue during the critical periods24.
The reasons that induce excess fat in childhood affect the social, psycho-emotional, metabolic and functional outcome, which lead children and adolescents to inadequate food intake, and decreased physical activity; thus, contributing to the increase in obesity13.
Given the high prevalence of obesity, and the association between the exacerbated accumulation of subcutaneous fat, and metabolic and cardiovascular diseases observed in children and adolescents. The findings from this study suggest the development of new researches to analyze not only the behavior of the body fat, but also the relationship of the adipose tissue values with other variables related to the health, involving growth, maturing, motor performance, and physical activity levels in DS individuals.
REFERENCES
1. Speiser PW, Rudolf MCJ, Anhalt H, Camacho-Hubner C, Chiarelli F, Eliakim A et al. Consensus statement: childhood obesity. J Clin Endocrinol Metab. 2005; 90(3): 1871-1887. [ Links ]
2. Reilly JJ, Methven E, Mcdowell ZC, Hacking B, Alexander D, Stewart D et al. Health consequences of obesity. Arch Dis Child. 2003; 88(9): 748-752. [ Links ]
3. Grundy SM, Benjamin IJ, Burke GL, Chait A, Eckel RH, Howard BV et al. Diabetes and cardiovascular disease: a statement for healthcare professionals from the American Heart Association. Circulation. 1999; 100(10): 1134-1146. [ Links ]
4. World Health Organization. Obesity: preventing and managing the global epidemic. Geneva: Report on a WHO Consultation on Obesity; 2000. [ Links ]
5. González-Agüero A, Ara I, Moreno LA, Vicente-Rodríguez G, Casajús JA. Fat and lean masses in youths with Down syndrome: Gender differences. Res Dev Disabil. 2011; 32(5): 1685-1693. [ Links ]
6. González-Agüero A, Vicente-Rodriguez G, Moreno LA, Casajús JA. Dimorfismo sexual en grasa corporal en adolescentes com síndrome de Down. Rev Esp Obes. 2010; 8(1): 28-33. [ Links ]
7. Slaughter MH, Lohman TG, Boileau RA, Horswill CA, Stillman RJ, Van Loan MD et al. Skinfold equations for estimation of body fatness in children and youth. Hum Biol. 1988; 60(5): 709-723. [ Links ]
8. Guedes DP, Guedes JERP. Crescimento, composição corporal e desempenho motor em crianças e adolescentes. São Paulo: CLR Balieiro; 1997. [ Links ]
9. González-Agüero A, Vicente-Rodríguez G, Ara I, Moreno LA, Casajús JA. Accuracy of prediction equations to assess percentage of body fat in children and adolescents with Down syndrome compared to air displacement plethysmography. Res Dev Disabil. 2011; 32(5): 1764-1769. [ Links ]
10. Queiroga MB. Utilização de medidas antropométricas para a determinação da distribuição de gordura corporal. Atividade física & saúde. 1998; 3(1): 37-47. [ Links ]
11. Guedes DP, Guedes JERP. Manual prático para avaliação em educação física. Barueri: Manole; 2006. [ Links ]
12. Malina RM, Bouchard C, Bar-Or O. Growth, Maturation, and Physical Activity. Champaign, IL: Human Kinetics; 2004. [ Links ]
13. Guedes DP, Guedes JERP. Controle do peso corporal: composição corporal, atividade física e nutrição. Rio de Janeiro: Shape; 2003. [ Links ]
14. Dwyer T, Blizzard CL. Defining obesity in children by biological endpoint rather than population distribution. Int J Obes Relat Metab Disordv. 1996; 20(5): 472-480. [ Links ]
15. Cooke PS, Heine PA, Taylor JA, Lubahn DB. The role of estrogen and receptor-alpha in male adipose tissue. Mol Cell Endocrinol. 2001; 178(1-2): 147-154. [ Links ]
16. Ferrara M, Capozzi L, Russo R. Impact of er gene polymorphisms on overweight and obesity in Down syndrome. Cent Eur J Med. 2008; 3(3): 271-278. [ Links ]
17. Marreiro DN, De Sousa AF, Nogueira NN, Oliveira FE. Effect of zinc supplementation on thyroid hormone metabolism of adolescents with Down syndrome. Biol Trace Elem Res. 2009; 129(1-3): 20-27. [ Links ]
18. Ordóñez-Munoz FJ, Rosety M, Rodriguez MR. Influence of 12-week exercise training on fat mass percentage in adolescents with Down syndrome. Med Sci Monit. 2006; 12(10): 416-419. [ Links ]
19. Guedes DP, Guedes JERP. Prevalência de sobrepeso e obesidade em crianças e adolescentes do município de Londrina (PR), Brasil. Motriz. 1998; 4(1): 18-25. [ Links ]
20. Costa LT. Alternativa metodológica para mensurar a maturação somática em crianças e adolescentes com síndrome de Down. (Dissertação). Campinas: Faculdade de Educação Física da Universidade Estadual de Campinas; 2011. [ Links ]
21. Velásquez-Meléndez G, Silveira EA, Allencastro-Souza P, Kac G. Relationship between sitting-height-to-stature ratio and adiposity in Brazilian women. Am J Hum Biol. 2005; 17(5): 646-653. [ Links ]
22. Tannirandorn Y, Manotaya S, Uerpairojkit B, Tanawattanacharoen S, Wacharaprechanont T, Charoenvidhya D. Evaluation of fetal femur length to detect Down syndrome in a Thai population. Int J Gynaecol Obstet. 2001; 73(2): 117-123. [ Links ]
23. Despres JP, Moorjani S, Lupien PJ, Tremblay A, Nadeau A, Bouchard C. Regional fat distribuition of body fat, plasma lipoproteins, and cardiovascular disease. Arterioscler Thromb Vasc Biol. 1990; 10: 497-511. [ Links ]
24. Dietz WH. Critical periods in childhood obesity. Am J Clin Nutr. 1994; 59(5): 955-959. [ Links ]
25. Rogers PT, Coleman M, Buckley S. Medical care in Down syndrome - A Preventive medicine approach. Pediatric Habilation: Marcel Dekker; 1992. [ Links ]
 Correspondence to:
Correspondence to:
fabiob@fcm.unicamp.br
Manuscript submitted Feb 01 2012,
Accepted for publication Oct 29 2012
Baseado em Dissertação: Composição corporal e somatotipo em pessoas com síndrome de Down, FEF/UNICAMP, 2013.

{kind=link}
{kind=link}