










Serviços Personalizados
Journal

artigo
 Inglês (pdf)
Inglês (pdf)
 Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
Indicadores
Compartilhar

 Permalink
PermalinkJournal of Human Growth and Development
versão impressa ISSN 0104-1282
Rev. bras. crescimento desenvolv. hum. vol.23 no.1 São Paulo 2013
ORIGINAL RESEARCH
Tetraparetic children and caregivers: featuring the profile and accessibility assistive technology
Tatiana Cristina AlcassaI; Rosangela FilipiniII, IV; Jesus Carlos Delgado GarciaII, IV; Sandra Terezinha AmaranteII, IV; Fernando AdamiIII, IV; Maria Claudia de Brito LuzIII, IV; Renata Macedo Martins PimentelIV; Ligia Ajaime AzzalisV; Virginia Berlanga Campos JunqueiraV; Fernando Luiz Affonso FonsecaV
IPós-graduação em Tecnologia Assistiva, FMABC, Santo André, SP, Brasil
IICoordenação do curso de Pós-graduação em Tecnologia Assistiva, FMABC, Santo André, SP, Brasil
IIICurso de Gestão em Saúde Ambiental, FMABC, Santo André, SP, Brasil
IVLaboratório de Delineamento de Estudos e Escrita Científica. Faculdade de Medicina do ABC, Santo André, SP
VCurso de Gestão em Saúde Ambiental, FMABC, Santo André, SP; Brasil, Departamento de Ciências Biológicas - Universidade Federal de São Paulo, Diadema, SP, Brasil
ABSTRACT
The objective of this study was to describe the profile of caregivers and children with tetraparesis according to their characteristics, sociodemographic aspects and accessibility, by means of a questionnaire developed and applied during the physical therapy sessions, performed at the sector of child neurology from the Rehabilitation Municipal Center of Santo André. We interviewed 19 caregivers of tetraparetic children diagnosed with Cerebral Palsy.Analysis of the results showed that the majority of caregivers were the mothers of selected children and that these women were engaged, fully, to take care of their children, abdicating their own professional or educational activities.The children had important motor impairment (GMFCS V), being dependent for many functional activities and needing some Assistive Technologies. It was also found little knowledge on the part of caregivers, in relation to this terminology that, associated with the lack of financial resources, may cause harm in the process of autonomy, participation and social inclusion of these children.
Key words: cerebral palsy; children; self-help devices.
INTRODUCTION
According to data from the Brazilian Institute of Geography and Statistics (IBGE), 23.9 % of the Brazilian populations have some type of disability and about 7% of these people present a motor disability1. Using these data for the population of Santo André, where, according to 2010 census, 676,407 inhabitants live, we have approximately 47,348 people with some type of motor disability, including these children with a diagnosis of cerebral palsy (CP).
Cerebral palsy is a disorder of movement and posture due to a defect or an injury of the immature brain2. Individuals with CP have a wide range of disabilities that primarily affects the development of postural and motor control; it also interferes with the performance of motor activities and the quality of the movement, affecting the way the mobility and other functional activities are held3.
The etiology of CP can be divided into prenatal, perinatal, neonatal and the postnatal. It can be classified by its clinical type asspastic (75 %); ataxic (2 %); dyskinetic, choreoathetoid, dystonic (9 - 22 %) and mixed (9 - 22 %). In relation to the topography or anatomy, it can be called tetraparesis, diparetic and hemiparesia4.
In order to have not only a better functional diagnostic understanding but also a common language among the rehabilitation team, aerating scale for individuals with motor PC can be used. The Gross Motor Function Classification System (GMFCS)5 was developed specifically for individuals with CP and is used to classify the children motor function from birth to the age of 18. It is divided into fivedistinct age groups: up to 2 years old, 2 to 4 years old, 4 to 6 years old, 6 to 12 years old and from 12 to 18 years old; all of them described in five levels.The use of this scale facilitates the understanding of the child motor condition with CP in his/her various stages and ages favoring therapeutic strategies with the goal of providing his/her social participation and independence, even with the use of support devices for walking, wheelchair and mobility resources3,6.
In the daily routine of tetraparetic children we notice that they receive much more attention from their caregivers than those children who have a normal growth. The use of assistive technologies tends to alleviate this routine3.
Assistive Technology is a term used to identify the whole arsenal of resources and services that contribute to provide or enhance the functional abilities of people with disabilities and consequently promote independent living and inclusion7.
In this study the following assistive technology resources will be considered: adapted wheelchair, positioning chair, bath chair, stabilizer standing posture and position in orthoses. These resources should be included in the tetraparetic child's life, enabling his/her better positioning, functionality and participation. Some factors may interfere in getting these resources, and we should also pay attention to the social, economic and cultural conditions of these families8.
The use of an appropriate technology can transform a barrier in a facilitator and allows the participation of children with Cerebral Palsy in their homes, at school and in the community.
Thus, the objective of this study is to describe the caregivers and the children with tetraparesis, according to their characteristics, sociodemographic aspects and accessibility.
METHODS
We developed a cross-sectional study with a sample of convenience. The study was conducted at the Rehabilitation Municipal Center of Santo André, in the sector of child neurology. The study population was made up of 19 tetraparetic children with a diagnosis of cerebral palsy, classified by GMFCS in levels III, IV and V, and all of them were being attended at that sector.
This study used a questionnaire for data collection. IT was composed of questions that addressed the knowledge about the characteristics of children, sociodemographic aspects and accessibility to assistive technologies.
The request for collecting the data was sent to the responsible for the Institution where the research took place and, after his approval and signature of the Data File for Research Involving Human Beings, was submitted to the Ethics Committee in Research of the Health Department of the Municipal Government of Santo André, affiliated to the National Council for Human Research (CONEP), where the project was subsequently approved by the Committee under the number 30/2011.
People involved in this study took a fifteen minute pre-test to analyze the efficiency of this instrument, before the real data collection. In the beginning, everyone was informed about the objectives of the research, their voluntary participation and the guarantee of confidentiality about their responses; they were also asked to fill out the "Statement of Free and Known Consent" .
The collection was made by the researcher herself, who observed how people answered the questionnaire and solved the doubts that have arisen.
The presentation of data was performed by means of tables, which have demonstrated quantitatively the collected data. The analysis used a simple frequency table to describe the caregivers and the children according to independent variables. The data entry was performed on Excel program and the analysis in Stata11.0.
The subjects who were surveyed din this study did not suffer damage before, during or afterdata collection. The benefits have been translated into knowledge for society, science and related professionals.
RESULTS
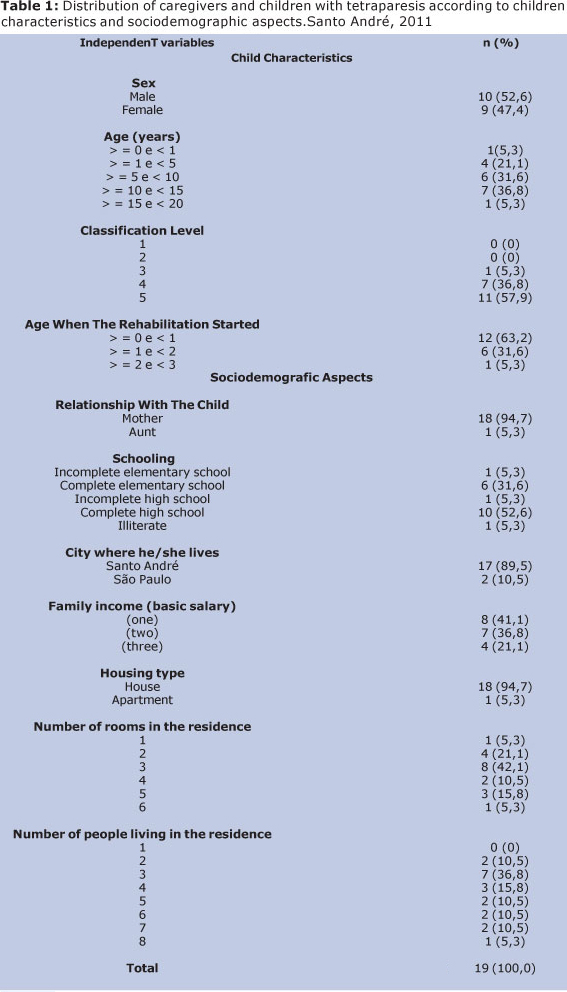
The study showed that 94.7 % of the questionnaires were completed by mothers of children with quadriplegia. The age range of 52.7 % of the children studied is between 2 and 9 years, and 52.6 % are male.
According to Gross Motor Function Classification System (GMFCS), 57.9% of the children selected for this study are presented in grade V; and 63.2% of these started rehabilitation in their first year of life
Concerning to the city, 89.7 % live in Santo André and 94.7 % of them live in houses. Then, 63.1 % of the families have 2, 3 or 4 people in their houses, and 57.9 % of these families have income from 2 to 3 minimum wages.
In relation to the educational level of these children caregivers, 52.6 % of the interviewees have completed high school.
DISCUSSION
The study was conducted with19 tetraparetic children what can be considered a small number of subjects for are search; however it was found that the incidence often traparesis as a topographic diagnosis in children with cerebral palsy sequels less than 50% (about 9 to 43% of cases)4. As a background, we can say that there is a work with a number of subject sequel to ten9.This allows us to think about the relationship between the severity of the cases and the consequences presented in tetraparesias.
The data obtained in the questionnaires showed that 52.6%of the interviews had completed high school, contrasting the data from the IBGE1, which says that about 42.3% of the population of São Paulo has this level of education. However, when asked about the knowledge of the term Assistive Technology, 94.7% of them did not know this terminology, thus justifying the fact that AT is a new area of knowledge in Brazil, and it was instituted by The Technical Help Committee10,on 10th September 2006.
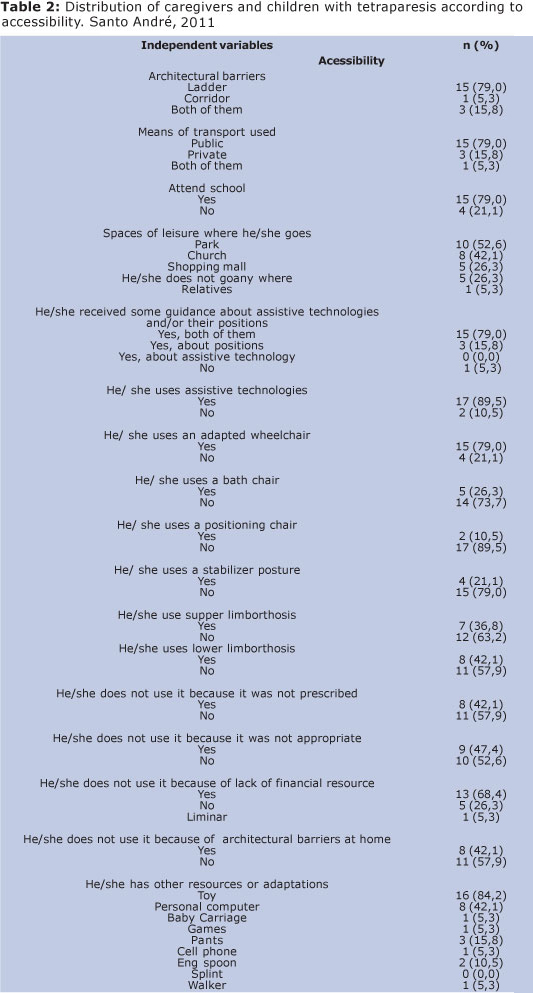
About 57.9% of these families have a family income between 2 and 3 minimum wages, in opposition to the national average whichis 10.6%, according to the census of 2010. However, 68.4% of the interviews showed lack of financial resources and this is the main reason for not purchasing AT (11). This reinforces the need for greater investment in this area, both from the point of view of AT development in Brazil, but also in public policies what may facilitate the access to these technologies. The most used AT is the wheelchair, according to 79% of the interviews, and this shows that it becomes easier for these children attend school and go to community spaces12-14-15.
According to the study and the data analysis, we can conclude that most of the caregivers are the mothers themselves and they are totally engaged in taking care of their children and in their treatment; besides these women have quitted their professional educational activities.
These children and their mothers live in Santo André, they have a monthly income of 2-3 minimum wages and share their homes with 2 other people.
The Assistive technologies present in these families daily lives; however, it is an area that most of the mothers of the children with tetraparesias do not know very well. Both this lack of information and the lack of financial resources complicate the process of autonomy, participation and social inclusion of these children.
REFERENCES
1. IBGE: Instituto Brasileiro de Geografia e Estatística. Disponível em: http://www.ibge.gov.br. [ Links ]
2. Bobath K. A neurophysiological basis for the treatment of the cerebral palsy. London: William Heinemann Medical books,1980. Págs 12-21. [ Links ]
3. Cury VCR, Brandão MB. Reabilitação em Paralisia Cerebral. Rio de Janeiro: Medbook, 2011. [ Links ]
4. Fernandes AC, Ramos ACR, Casalis MEP, Herbert SK. Medicina e reabilitação: princípios e prática. São Paulo: Artes Médicas, 2007; 27-36 [ Links ]
5. Palisiano R, Rosembaum P, Walter S, Russell D, Wood E, Galuppi B. CanChild Centre for Childhood Disability Research, Institute for Applied Health Sciences, McMaster University. Website: www.canchild.ca;1-42 [ Links ]
6. Teixeira E, Sauron FN, Santos LSB, Oliveira MC. Terapia Ocupacional na reabilitação física. São Paulo: Roca, 2003; 6-26 [ Links ]
7. BerschR,Tonolli JC. Tecnologia Assistiva. Disponível em www.assistiva.com.br. Acesso em: 23 agosto 2011; 1-15 [ Links ]
8. Braccialli LMP, Oliveira FT, Braccialli AC, Sankako AN. Influência do assento da cadeira adaptada na execução de uma tarefa de manuseio. Rev. Bras. Ed. Esp.,2008;14:141-54. [ Links ]
9. Farceta Junior F, Abreu FP, Neves DL, Kertzman PF, Zuccon A, Bittencourt SO, Lopes DML. Tratamento da luxação paralítica do quadril na paralisia cerebral tetraparéticaespástica com osteotomia do fêmur e do ilíaco sem abertura da cápsula articular (capsuloplastia). Rev. Bras. Ortop. 2010;45(2):181-5. [ Links ]
10. CAT: Comitê de Ajudas Técnicas. Disponível em: http://www.mj.gov.br/sedh/ct/corde/dpdh/corde/comite_at.asp [ Links ]
11. Phillips B, Zhao H. Predictors of assistive technology abandonment. Assistive Technology, v. 5, p. 36 -45, 1993. [ Links ]
12. Rosembaum PL, Palisano RJ, Bartlett DJ, Galuppi BE, Russel DJ. Development of the gross motor function classification system for cerebral palsy. DevMedChildNeurol 2008; 50:249-53 [ Links ]
13. Sposito MMM, Ribeiro M. Avaliação da funcionalidade da criança com Paralisia Cerebral espástica. Acta Fisiatr., 2010;17(2):50-61. [ Links ]
14. Brasileiro IC, Moreira TMM, Jorge MSB. Interveniência dos fatores ambientais na vida de crianças com Paralisia Cerebral.ActaFisiatr., 2009;16(3):13 [ Links ]
15. Atrash H K, Carpentier R. The evolving role of public health in the delivery of health care. Journal of Human Growth and Development. [ Links ]
 Correspondence to:
Correspondence to:
profferfonseca@gmail.com
Manuscript submitted Oct 16 2012
Accepted for publication Dec 30 2012.
