










Serviços Personalizados
Journal

artigo
 Inglês (pdf)
Inglês (pdf)
 Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
Indicadores
Compartilhar

 Permalink
PermalinkJournal of Human Growth and Development
versão impressa ISSN 0104-1282
Rev. bras. crescimento desenvolv. hum. vol.24 no.2 São Paulo 2014
ORIGINAL RESEARCH
Level of physical activity and functional in athletes children
Evelyn Souza RochaI; George Jung RoseII; Camila Isabel Santos SchivinskiIII
IPhysiotherapist, State University of Santa Catarina - UDESC, Centre for Health Sciences and Sports - CEFID
IIPhysiotherapist, Master in Physical Therapy from the UDESC - CEFID
IIIPhysiotherapist, PhD Professor at UDESC- CEFID
ABSTRACT
The improvement of physical ability and functional performance of children are acquisitions of physical activity, but studies about the impact of sports on functional capacity and respiratory muscles in children are still scarce.
OBJECTIVE: to assess the respiratory muscle strength, the functional and physical activity levels of athletes children when compared with no athletes children, both in the same age group.
METHODS: the study involved 20 children from schools (non-athletes group, NAGN n = 10), and sports training centers (athletes group, AG n = 10) from Florianópolis-SC/Brazil, aged between 7 and 10 years. We used the International Physical Activity Questionnaire (IPAQ) and evaluated the respiratory muscle strength (RMS) with a manuvacuometer (MVD-300, Microhard). The functional capacity was evaluated with the six minute walking test (6MWT).
RESULTS: respiratory muscle strength and functional capacity did not differ between groups. Differences were found in heart rate in the third minute, between the first and second 6MWT in both groups - GA: 91.20 ± 7.57 and 129.20 ± 33.81 (p = 0.005) and NAG: 96,10±1,45 e 122,00 ± 22,62 (p = 0,008). Dyspnea scale was different between two groups on the beginning of second 6MWT, bigger in NAG group (0.6 ± 0.65 x 0.10 ± 0.31, p = 0.029). Characteristics of physical activity, assessed by IPAQ were different between groups.
CONCLUSION: the athletes and non-athletes children presented similar respiratory muscle strength and functional capacity. A bigger sample is relevant to accomplish new outcomes.
Key words: exercise, child, athletes, respiratory muscles/physiology.
INTRODUCTION
The activity can be conceived as a complex human behavior, voluntary and autonomous, with components and determinants of biological, psycosocial and cultural order1. The main health benefits provided by their regular practice refer to physical aspects, such as anthropometric, neuromuscular and metabolic criteria, and psychological aspects, also essential to men2.
The period of childhood represents a fundamental step in human development. This period is marked by intense physical activities. These important and necessary for the child to get to know the environment around them, growing normally and improving their knowledge of the world activities.3,4
Among the positive features of physical activity, can be highlighted in their physiological benefits, increased cerebral oxygenation, corporal5 weight control, reduction of cardiovascular risk6, ossification and growing7, and psychological5: which is part distraction and increase efficiency, not to mention the improved self-esteem, reducing depression, anxiety, stress and psychological disorders.5,6 However, especially among children, it is observed that physical activity is relatively low, even though the school environment be considered a motivator for the year and recognized role in establishing it as routine.7,8
The low level of physical activity among children is attributed to their lifestyle.8-10 Today, this age group is characterized by attitudes such as watching television, playing video games and using the computer for long periods of time - practices that, in fact, contribute to behavior sedentário10,11 and especially for obesity.12 It is believed that promoting this type of activity in childhood and adolescence contributes to the establishment of a better control of chronic diseases10 and a solid basis for reducing sedentary lifestyle in adulthood.
It is evident that being physically active since childhood can pose many benefits, not only in the physical area, but also the psychological, emotional and even social spheres. The practice of motor activities like games and sports activities, presents "costs" because demands on time and energy consumption of the child.3 They claim that their benefits are superior show, turning into real investment as promote social interaction among children, a fact that will prevent the psychological / social isolation and improve self-image and self-assurance.3,9
The improvement of physical fitness and performance of the child are also acquisitions of this kind of practice because different driving experiences provide basic experiences of movement, which, over the years, will be enhanced. Optimization of child growth and stimulate healthy habits are other benefits pointed as well as a harmonious relationship between the growth and development of children.1
In this context, studies that analyze the impact of regular physical activity pertaining to the various aspects of organic systems have great relevance. However, there are few that address the impact of sports on functional capacity and respiratory muscle strength in the general pediatric population. This study may identify effects of school physical activity, supporting programs to combat sedentary lifestyle and primary prevention of diseases, reinforcing the importance of integrating this practice into daily life of children. Assess variables such as level of physical activity and functional capacity in healthy children, practitioners and non-practitioners of physical activity, which enables better know the impact of this practice and also its relationship with the body. Specifically in the musculoskeletal system, there is a belief that a concomitant respiratory muscle training to the practice of some exercise occur.13
Given the above, the objective of this study is to evaluate the level of physical activity, respiratory muscle strength and functional capacity of collegiate athletes and non-athletes.
METHODS
Characterized as analytical observational transversal14 two populations, this study was conducted with children from public and private schools and specific training in Florianópolis / SC. We adopted a convenience sampling (n = 24) which was divided into two groups, according to the practice or not practice regular physical activity, composed of athletes healthy infants (AG) and non-athletes healthy infants (NAG). The sample size calculation was not performed due to the absence of previous similar studies.
Children who were aged between seven and ten full years and whose soundness was proven by health questionnaire duly answered by the parents / guardians were included. To ensure the soundness children were evaluated by a physician prior to participation in pediatric trials. To characterize the AG, this was formed by students who undertake training for the sport of competitive performance, guaranteed by their respective federation (football, volleyball, martial arts) at least twice a week. This group were excluded children who were not athletes performing sports training that frequency for at least three months. In both groups , the students who had some limitations/ restrictions or problems during the application of some of the assessment instruments (such as difficulties of understanding , intolerance, lack of cooperation or malaise), who delivered the physical activity questionnaire wrongly answered or, further, that manifested disease picture on the assessment day, did not participate in the sample . Two subjects were excluded for not meeting the conditions of health - one for asthma and other by diabetes, and two others for failing to complete the tests
The research has developed a data collected from a pediatrician and sports training centers. In these places, after signing the consent form for parents / guardians and explanation about the study, students were asked to carry out assessment procedures. IPAQ, measure of respiratory muscle strength (RMS) and 6MWT, in this order. To achieve this, three instruments were applied.
The IPAQ was applied to the short form and was self-administered by parents or legal guardians. This is a questionnaire originally developed in order to estimate the level of habitual physical activity of populations of different countries15, divided into four questions related to time spent in physical activities, and the individual must consider the activities performed in the last prior to the interview week. The prestigious categories according to the IPAQ are: sedentary, insufficiently active (which has two subdivisions - The insufficiently active and insufficiently active B), active and very active16. At that time, parents/guardians also completed a questionnaire prepared by the researchers about the health of the child.
Respiratory muscle strength was measured by the manometer apparatus of MVD-300 (Microhard) mark for identification of maximal inspiratory pressure (MIP) and expiratory (MEP), representing the strength of respiratory muscles, lung volume at which the measurements are performed and the corresponding value of the elastic recoil pressure in the respiratory system17. The evaluation of MIP and MEP was taken with the patient seated comfortably, using tracheal connector, mouthpiece and nose clip. To obtain the final measure, was considered the greatest result of three attempts18.
Then, the students performed the 6MWT according to the standards of the American Thoracic Society (ATS)19, which states that the test begins with the collection of baseline parameters of heart rate (HR), respiratory rate (RR), peripheral oxygen saturation (SpO2) , arterial blood pressure (BP) and dyspnea sensation. Data for HR and SpO2 were measured with digital pulse oximeter (Nonin, onys 9500), the RR was given by counting the breaths in one minute. Dyspnea was measured using the Visual Analog Scale of Perceived Effort (VASPE).20 Prior to this initial collection, the participant remained seated at rest for about ten minutes, when he received guidance to the test: walk as fast as possible without running around a track 30 meters for six minutes. Child was allowed to stop, rest or walk slower if you had need; over time, however, continued to be recorded, regardless of the interruption. Standardized verbal stimuli were given every minute. In the middle of the test, all parameters except BP, were measured, and the sixth minute, the patient was advised to stop and the distance was calculated. The initial parameters were collected again and the test was repeated after 30 minutes.
The collected data were stored in a database and to analyze the results, we used the SPSS ® 17.0 software for Windows ®. The data were presented by descriptive analysis and frequency. The Wilcoxon test for statistic were used in each group and the Mann-Whitney test for comparison between groups. Still, we considered a p of 0.05 for statistical significance.
All parents/guardians for school groups of all signed a consent form (108/2010).
RESULTS
The study included 20 children, ten of AG and ten of the NAG. The first was composed of seven boys, while the NAG for eight, with no statistical difference between them in relation to gender (p = 0.261).
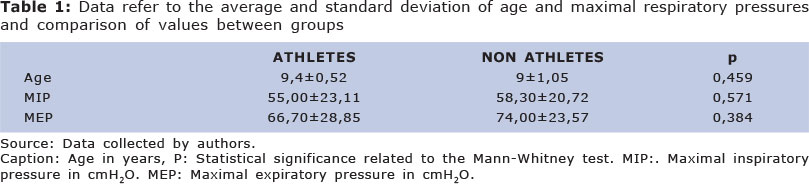
The mean and standard deviation in the age and gender of both groups are shown in Table 1.
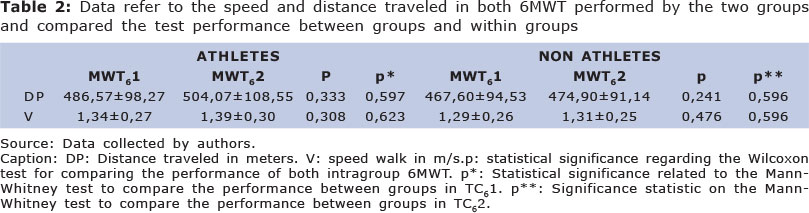
In AG, ages ranged between nine and ten, while the NAG was the minimum age seven and maximum ten years. There was no significant difference between groups with respect to age (p = 0.459) and maximal respiratory pressures (Table 1). The NAG and AG were also not different performances in either 6MWT, as table 2.
Tables 2,3,4 and 5 show the data of athletes and non-athletes for the two walk tests (6MWT).
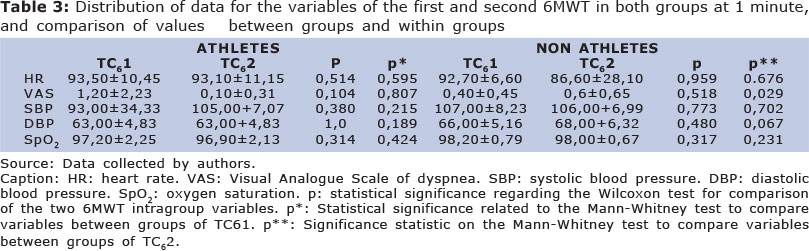
Only in dyspnea scale, early in the second 6MWT, there was significant difference between groups (p = 0.029**). Children of the NAG reported more fatigue than children of AG (0.6 ± 0.65 x 0.10 ± 0.31, p = 0.029) (Table 3).
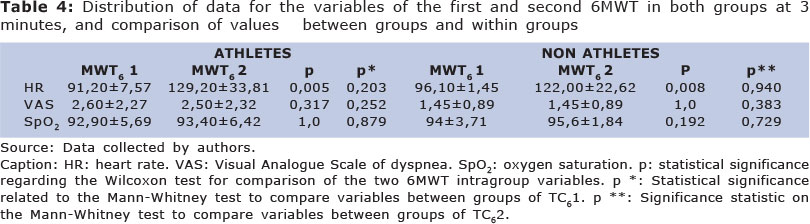
When comparing the behavior of the variables between the two 6MWT performed in each group (intra-group), using the Wilcoxon test, we observed an increase in heart rate of athletes in the second test (91.20 ± 7.57 x 129.20 ± 33.81), as the data in table 4. The other variables in the course of 6MWD did not differ in any of the three time points (1 minute, 3 and 6), any two groups.
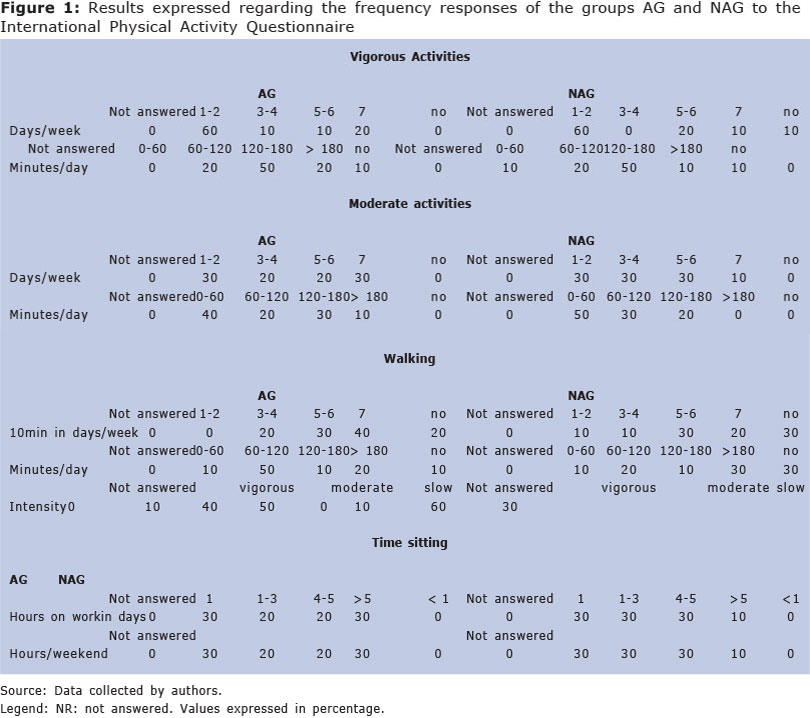
Regarding the IPAQ questionnaire, answered by the parents, it was found that 60% of children in both groups, practicing vigorous activities one to two days a week and on those days, the length of which is 60 to 120 min. 50% of children in each group.
However, in moderate activities, we observed that 30% of the AG perform during all days of the week, while the NAG only 10% have the same habit. Most children in groups practicing less than 60 min. moderate activities (AG = 40% and NAG = 50%).
With respect to walking, 40% of the AG perform walk during all days of the week, while only 20% of NAG has the same attitude. In addition, 50% of AG go between 10 and 30 min. daily, while 20% of NAG refer the same. The speed of step shows that 50% of AG walks in slow steps and 60% of NAG to moderate steps.
The last block of questions relates to remain seated during weekdays and weekends. The parents of 80% of the NAG reported that their children are more than 5hs for weekday sitting. In this frequency AG was 40%. Already weekend groups exhibit similar behaviors as (NAG 40% and 30% AG are 5 hours per day of the weekend sitting).
Figure 1 shows the frequency responses of the two groups related to the IPAQ questions.
DISCUSSION
The theme of the current research has been the focus of ongoing discussions. This is because studies have shown that children and adolescents are less physically fit than their peers in previous decades or good portion of them do not meet desirable criteria for a recommended health-related physical fitness.
There are several motivations that have led to reduced levels of physical activity in children: urbanization, new technologies, violence in cities10. Study of brazilian children identified that they remain an average of 21 hours per week in front of the television, reaching an impressive 10 hours a day21. This information corroborates the behavior of children observed in the current study, by applying the IPAQ, where 50% of the NAG did not perform any physical activity, excluding escolar physical education.10,22,23 These data draw attention, since, according to Cao et al (2011), a low level of physical activity combined with too much time watching television contribute to anxiety, depression and unsatisfactory school life.24
The responsibility of that physical inactivity is due to technological advent, which possibly makes the man of the future an obese subject23. In this line, the preferences regarding the games of children who were referred by their parents / guardians about, since 40% of NAG choose to play with computer and video games. Furthermore, an australian study found that so-called "active games game" may positively influence body composition and reduced fat mass compared to traditional games, with a direction to the familiar orientation.25
Although half of the students do not realize the NAG no physical activity, both groups showed a right balance between sedentary behavior and active behavior. The NAG had become so active in moderate physical activity (70%), as the AG, not fitting in featuring a sedentary lifestyle. Have the time spent in sedentary activities (AG = 3.7 h; NAG = 4.2) were better than that found in previous studies in the national literature. What is odd is that unlike these studies included adolescents, while the present study examined school. The literature points to a decline in the level of physical activity from 11 years of age25-27, not a premature inactivity as seen here.
Regarding the characteristic of physical activity for children, important to note that the most appropriate in this age group should involve dynamic movement of large muscle groups for periods of 20 minutes or more, three or more times per week, at an intensity that stimulates the heart beat to 140 or more per minute.² A description compatible with this activity is the walk itself. In addition to the known cardiovascular benefits, Taylor (2009) identified that 20 minute walk outdoors for a week were able to reduce clinical attention deficit disorder and hiperativity29, incident disease in 8% of childrens.30 However , in this study, it was observed that even this practice is uncommon. The time spent walking per day at NAG was up to ten minutes for 10 % of the participants, and between ten and 30 minutes for 20 % and 60 % of children walk at a moderate pace and only 10 % go on vigorous steps. Thus, as discussed by the group of Teixeira (2005)31, children remain at moderate to high physical activity in very short periods. In everyday life, do not perform physical activity in sufficient quantities and intensities to promote beneficial effects on health, staying most of the time in low-intensity physical activity.
These data are reinforced by the responses obtained by the IPAQ with respect to the time in which children engage in moderate physical activity. Half the NAG performs this type of dynamic up to 60 minutes a day and no child of this group performs this activity for more than 180 minutes per day. In addition, the parent / guardian 80% of NAG reported that children remain seated over five hours a day which, according to the study mentioned above, shows the maintenance convenience and sedentary behavior of children.
Another interesting finding in the current study relates to the perception of parents/guardians as to the physical condition of children. Although the responses of parents/guardians of children athletes reinforce this practice higher level than the parents/guardians of children non-athletes through the issues of IPAQ, some statements of parents / guardians AG intrigue regarding the habits of children. Many answers are more compatible with sedentary habits than with the real activity that school athletes develop. An alternative to this result is the fact that many parents/guardians have difficulty understanding what would be really sedentary. This may have become the method of subjective evaluation.
The contradiction in the answers, according to the parents/guardians, themselves may also have occurred due to their assumption that the evaluators knew that children practiced sports, eliminating the need to answer the questions about it. Self-administered questionnaires have advantages such as lower cost and the possibility of information gathering in large groups with respect to the type of activity and context in which they are held. Nevertheless, often demonstrate difficulties in meeting the criteria of reliability and validity, recall bias and also by misinterpretation of perguntas.32-35
With respect to the data presented in the assessment of functional capacity and respiratory muscle strength between groups, failure to identify significant differences between them points to the need to expand the sample size, considering the expectation that the AG presented superior performance in both tests. In an indian study two groups of adolescents submitted or not to a regular program of physical activities outside the regular class period, from the same school were compared. The first group showed higher values of RMS, which were attributed to the practice of exercises.36
Also in this line, Santiago et al.37 discuss the influence of age on maximal respiratory pressures. Whereas the groups had the same mean age and gender to prevalence same, may have been the contribution of factors like hormone and growth itself so that the values of the two groups were so close.
The only variable that was statistically different between the AG and NAG was the sensation of dyspnea, according to VASPE . Children non-athletes showed more fatigue that athletes just 1 minute in the second 6MWT. A likely explanation for this event would be the very lack of fitness of these children. Another possibility could be that the 30-min interval between the two tests was not sufficient for recovery of the participants NAG. Aquino38, who checked whether there was difference between the distance traveled by healthy subjects between walking tests with different size runners, not found significant changes in 6MWT variables involved in performing the tests at an interval of 24 hours.HR in 3 minutes was the only variable that the 6MWT increased significantly in both groups compared to FC in the first test. As in both groups showed better performance of children in the second test, there may have been more physical engagement of such and such, enhanced physical wear, which reflected that accelerated heart beat.
Although the results are insubstantial in relation to the same functional performance and muscle strength between AG and NAG, notes the importance of doing an intervention with children to increase opportunities to practice physical activities, especially with more intensity. The frequency with which children are forced or encouraged to engage in physical activity is inversely related to the level of physical activity practiced in the adult age.² In this context, understanding the social and environmental factors that influence the level of physical activity is important for the development of effective interventions to change for physical activity in children and adolescents behavior.
Accordingly, changes in children's behavior are necessary. Among them, the reduction of the number of hours spent with television, video games and computer as well as encouraging them to participate in sports competitions and physical education classes in schools. The education of parents/guardians for these children through their own exemple, is also key. This strategy aims to deploy a sound practice since childhood, combating sedentary lifestyle, and with it, the emergence of diseases such as obesity, psychological stress, immune disorders, heart disease and osteoporosis , which seem to have its beginnings in adolescence.39,40
How to be physically active since childhood not only brings benefits in the physical area, but also in the social and emocional,10 plus an improvement in lipid profile and metabolic22, it is clear that their early involvement in children's routine should be aimed at parents, caregivers, educators and health professionals involved with this age group .
Thus, the sample of children studied, athletes and non-athletes, no differences between respiratory muscle strength and functional capacity. Only the level of physical activity, assessed by questionnaire, differed between groups.
REFERENCES
1. Tenroller CA. Asthma and Physical Activity in Children [Monograph]. Canoes: Lutheran University of Brazil, Specialist in Public Health, 2004. [ Links ]
2. Matsudo SM, Matsudo VKR. Evidence of the Importance of Physical Activity in Cardiovascular Diseases and Health Diagn. Treatment. 2000 Apr-Jun; 5 (2) :10-7. [ Links ]
3. Hansen, J et al. The play and its implications for child development from Evolutionary Psychology. Rev. Bras. Development growth. Hum., Sao Paulo, vol. 17, n. 2 August 2007. [ Links ]
4. Oliveira, LDB et al. The hospital playroom as a promotional factor in childhood development: an experience report. Rev. bras. Development growth. hum., Sao Paulo, vol. 19, n. 2 August 2009. [ Links ]
5. Ribeiro SNP. Physics and Intervention for Depression Along its activity. Rev. bras. conn. phys. health. 1998 Feb, 3 (2) :73-9. [ Links ]
6. Ekelund U, Luan J, Sherar LB, et al. Moderate to Vigorous Physical Activity and Sedentary Time and Cardiometabolic Risk Factors in Children and Adolescents. JAMA.2012;307(7):704-712. [ Links ]
7. Mirtz TA, Chandler JP, Eyers CM. The Effects of Physical Activity on the Epiphyseal Growth Plates: A Review of the Literature on Normal Physiology and Clinical Implications. J Clin Med Res. 2011 Feb; 3(1): 1 - 7. [ Links ]
8. Ahn S, Fedewa AL. A meta-analysis of the relationship between children's physical activity and mental health. J Pediatr Psychol. 2011 May;36(4): 385-97. [ Links ]
9. Teixeira LR, Andrade J, Saraiva PAP. Effects of a physical activity program for asthmatic children, assessed by pulmonary function tests. Rev. paul. Educ. phys. 1992, 6 (1): 3-15. [ Links ]
10. Alves JGB. Physical activity in children: promoting adult health. Rev. Bras. Mater Health. Infant. 2003 Mar; 3 (1): 5-6. [ Links ]
11. Silva DAS, OJ Lima, RJS Silva Prado RL. Physical Activity and Sedentary Behaviour in School Children. Rev. bras. cineantropom. hum performance. 2009; 11 (3): 299-306. [ Links ]
12. Maher C, Olds TS, Eisenmann JC, Dollman J. Screen time is more strongly associated than physical activity with overweight and obesity in 9- to 16-year-old Australians. Acta Paediatr. 2012 Nov;101(11): 1170-4. [ Links ]
13. Lima EVNCL, Lima WL, Noble A, Santos AM, Brito LMO, Costa MRSR. Inspiratory Muscle Training and Breathing Exercises in Asthmatic Children. J Pulmonology. Aug 2008, 34 (8): 552-8. [ Links ]
14. Marques AP, Peccin MS. Physiotherapy Research: The Evidence-Based Practice and Business Studies. Fisioter Pesq. 2005 Jan-Apr, 11 (1):43-8. [ Links ]
15. Pardini R, Matsudo S, Araujo T, Andrade E, Braggion G, Andrade D, Oliveira L, Figueira Jr A, Raso V. Validation Questionnaire International Physical Activity. Rev. Bras. Sciences. mov and. 2001 Jul, 9 (3): 45-51. [ Links ]
16. Ainsworth B, Macera C, Jones D, Reis J, Addy C, Bowles H, Kohl, H. Comparison of the 2001 BRFSS and the IPAQ Physical Activity Questionnaires. Med. sci. sports exerc. 2006 Sep; 38(9):1584-1592. [ Links ]
17. Souza, RB. Maximal static respiratory pressures. J Pulmonology. 2002, 28 (3): 155-165. [ Links ]
18. Rodrigues SL, Viegas CAA. Study of Correlation Between Respiratory Function Tests and the Six Minute Walk Test in Patients with Chronic Obstructive Pulmonary Disease. J Pulmonology. 2002 Nov. 28 (6):324-8. [ Links ]
19. ATS statement: guidelines for the six-minute walk test. Am J Respir Crit Care Med. Jul 2002; 166(1): 111-7. [ Links ]
20. Irwin A, Tecklin JS. Cardiopulmonary Physical Therapy. 2nd ed. Sao Paulo: Manole, 2004. [ Links ]
21. Rivera IR, MAM Silva, Almeida Silva RDT, BAV Oliveira, Carvalho ACC. Physical, hours of assistance to the TV and Body Composition in Children and Adolescents activity. Arq Bras Cardiol 2010, 95 (2): 159-165. [ Links ]
22. Lazzoli JK, Nobrega ACL, Carvalho T, MAB Oliveira, JAC Teixeira, Piglet MB, et al. Physical activity and health in childhood and adolescence. Rev Bras Med Esporte. Aug 1998, 4 (4) :107-109. [ Links ]
23. Glaner MF. Importance of Physical Fitness-Related Health cieneantropom Rev. bras. hum performance. 2003, 5 (2) :75-85 [ Links ]
24. Cao H, Qian Q, Weng T, Yuan C, Sun Y, Wang H, Tao F.. Screen time, physical activity and mental health among urban adolescents in China. Prev Med. 2011 Oct;53(4-5):316-20. [ Links ]
25. Maddison R, Foley L, Ni Mhurchu C, Jiang Y, Jull A, Prapavessis H, Hohepa M, Rodgers A. Effects of active video games on body composition: a randomized controlled trial. Am J Clin Nutr. 2011 Jul;94(1):156-63. [ Links ]
26. Oliveira TC, Silva AAM, Santos CJN, Silva JS, Conception SIO. Physical activity and inactivity among schoolchildren from public and private schools in San Luis Rev Public Health. 2010 Dec, 44 (6): 996-1004. [ Links ]
27. Guedes DP, Guedes JERP. Practice levels of habitual physical activity in adolescents. Rev Bras Med Esporte. 2001, 7 (6) :187-99. [ Links ]
28. Hallal PC, Bertoldi AD, Goncalves H, Victora CG. Prevalence of physical inactivity and associated factors in adolescents 10-12 years of age. Cad Saude Publica. 2006, 22 (6): 177-87. [ Links ]
29. Taylor AF, Kuo FE. Children with attention deficits concentrate better after walk in the park. J Atten Disord. 2009 Mar;12(5):402-9. [ Links ]
30. Bloom B, Cohen RA, Freeman G. Summary health statistics for U.S. children: National Health Interview Survey, 2010. Vital Health Stat 10. 2011 Dec;(250):1-80. [ Links ]
31. Teixeira CGO, Teixeira Júnior J; Venancio PSM; N. France Physical Activity in Class Periods and Holidays in Annapolis School-GO. Rev. Bras. Sciences. mov and. 2005 Nov, 13 (1) :45-9. [ Links ]
32. Pena JCO, Macedo LB. There is an association between venous disease and level of physical activity in youth?. Fisioter. mov. 2011 Mar, 24 (1): 147-154. [ Links ]
33. Ainsworth BE, MPH, Caspersen CJ, Matthews CE, Mâsse LC, Ph.D., Tom Baranowski T, Zhu W. Recommendations to Improve the Accuracy of Estimates of Physical Activity Derived from Self Report. J Phys Act Health. 2012 Jan; 9(Suppl 1): S76 - S84. [ Links ]
34. Pinto DG, Correa CL, Guedes JERP. Reproducibility and validity of the International Physical Activity Questionnaire in adolescents. Rev Bras Med Esporte. 2005 Apr, 11 (2): 151-158. [ Links ]
35. Corder K, Ekelund U, Steele RM, Wareham NJ, Brage S. Assessment of physical activity in youth. J appl physiol. September 2008; 105(3):977-987 [ Links ]
36. Choudouri D; Aithal M, Kuhlkarni VA. Maximal Expiratory Pressure in Residential and Non-Residential School Children. Indian J Pediatr. 2002;69:229-232. [ Links ]
37. Santiago SQ, MLP Silva, J Davidson, Aristotle LRCRB. Evaluation of respiratory muscle strength in children and adolescents who are overweight / obese. Rev. paul. Pediatr. 2008 Jun, 26 (2): 146-150. [ Links ]
38. Aquino ES, Mourao FAG, Souza RKV, Glicério BM, CC Coelho. Comparative analysis of six-minute walk in healthy children and adolescents test. Rev. bras. Fisioter. 2010 Feb, 14 (1): 75-80. [ Links ]
39. Loprinzi PD, Trost SG. Parental influences on physical activity behavior in preschool children. Prev Med. 2010 Mar;50(3):129-33. [ Links ]
40. Zecevic CA, Tremblay L, Lovsin T, Michel L. Parental Influence on Young Children's Physical Activity. International Journal of Pediatrics. 2010;2010:1-9. [ Links ]
Manuscript submitted Aug 01 2013
Accepted for publication Dec 28 2013
Based on the final course work physiotherapy student Evelyn Souza Rocha, presented in 2011.
Corresponding author: cacaiss@yahoo.com.br

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}