










Serviços Personalizados
Journal

artigo
 Inglês (pdf)
Inglês (pdf)
 Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
Indicadores
Compartilhar

 Permalink
PermalinkJournal of Human Growth and Development
versão impressa ISSN 0104-1282versão On-line ISSN 2175-3598
J. Hum. Growth Dev. vol.26 no.1 São Paulo 2016
https://doi.org/10.7322/jhgd.113712
ORIGINAL RESEARCH
Why do women in the private sector have shorter pregnancies in Brazil? Left shift of gestational age, caesarean section and inversion of the expected disparity
Carmen Simone Grilo DinizI, *; Marina Jorge de MirandaI; Jéssica Reis-QueirozII; Marcel Reis QueirozI, III; Heloisa de Oliveira SalgadoI
ISchool of Public Health, University of São Paulo - Sao Paulo - SP - Brazil
IISchool of Nursing, University of São Paulo - Sao Paulo - SP - Brazil
IIISchool of Arts, Sciences and Humanities, University of Sao Paulo - São Paulo - SP - Brazil
ABSTRACT
INTRODUCTION: Gestational age (GA) at birth is the main predictor of newborn health, and spontaneous birth occurs around 40 weeks. In Brazil there is a populational reduction of the GA (left shift), presently around 39 weeks
OBJECTIVE: To analyze the left shift of gestational age (LDGA) in São Paulo City (SP) and in Southeastern Brazil, and associated factors
METHODS: Epidemiological descriptive study of LDGA in SP (data from Live birth information system, SINASC) and in Southeastern Brazil (data from "Birth in Brazil Survey"). Differences in GA were estimated, by type of birth (vaginal or cesarean) and payment source (public or private), using GA distribution curves in weeks
RESULTS: In SP, the peak of the curve for GA for vaginal births was 39 weeks, while for cesarean was 38 weeks. Most vaginal births were full term (39-406/7) while most cesarean were early term (37-386/7). In the private sector, there were more caesarean sections and lower GA at birth, with more preterm newborns and 60.4% being born early term, while in the public sector, 58.7% of births were full term, and a much higher proportion reaching 40 weeks
CONCLUSIONS: Babies born by cesarean and in the private sector lost one additional gestational week. There was an inversion in the expected disparity, with well-off women achieving poorer outcomes compared to the disadvantaged mothers. The use of continuous variables to estimate the IG (in days or weeks of pregnancy lost) can contribute to a better understanding of the Brazilian perinatal paradox
Keywords: midwifery, cesarean section, premature infant, equity, women's health.
INTRODUCTION
The duration of pregnancy is the main neonatal health predictor and is usually reported in completed weeks1. The calculation of weeks of pregnancy is done by several methods, the most common being the onset of the last menstrual period (LMP) or by ultrasonography (USG).
WHO defines preterm birth as babies born alive before 37 completed weeks of pregnancy. The period between 34 weeks and 36 6/7 is referred to as late preterm2-4. The ideal period for birth is classically defined as being between 37 weeks and 41 6/7. However, in the last decade, an international consensus emerged, finding this definition inadequate, since it was established based on the understanding that the perinatal outcomes of this group would be uniform, when in fact, this supposed uniformity does not exist1,5,6.
Nowadays, it is known that babies born between 39 weeks and 41 6/7 have better outcomes when compared with those born between full 37 weeks and 38 6/7. These latter have significantly higher risk of medical complications during hospitalization and during the first weeks postpartum, including respiratory distress syndrome, mechanical ventilation, more admissions in intensive care unit and higher mortality2,6. Thus, babies born between 37 and 38 weeks and 6/7 are more similar to babies born preterm late.
In response to this problem, and using the best evidence base, the American College of Obstetricians and Gynecologists (ACOG) now recommends a new classification of the gestational age: early term (37 0/7 weeks through 38 6/7 weeks), full term (39 0/7 weeks through 40 6/7 weeks), late term (41 0/7 weeks through 41 6/7 weeks) and postterm (42 0/7 weeks and beyond)5.
Evaluating the gestational age (GA) using the traditional binary factor (term versus preterm) can mask the continuous effect of using GA as a predictor of morbidity and mortality within each period. Several studies have focused on those born in earlier ages, but the monitoring of GA distribution trends can contribute to assess its consequences in the short, medium and long term1,7.
In Brazil, as in some other countries, there has been a reduction in gestational age at birth throughout recent decades, featuring a left shift of gestational age (LSGA). Every year, babies are increasingly being born in late preterm and early term when compared with the previous years. This phenomenon affects all age, income and education groups, although in Brazil it is more pronounced among more educated women which have higher income, is more frequent in private sector users, where the practice of elective caesarean section is the rule8,9.
In general, richer people tend to have better health outcomes, and this disparity has been addressed mainly through the universalization of health services, seeking to promote health equity. However, the LSGA among the richest is a recent phenomenon and is an "inversion of the expected disparity," i.e. it is expected that pregnant women in more favorable socio-economic conditions have better outcomes, and not the opposite, as is happening nowadays8. There is international recognition that not only the caesarean section (CS), as well as the labour induction, increase the occurrence of Preterm and Early term delivery, with a decrease of Full term and Late term birth7. But little information on this intervention is available, especially because of the difficulty in separating those cases of inductions of those where oxytocin or other drugs are used for augmenting labor, a widespread and poorly reported practice9.
The hormonal processes that preceed the term delivery help to prepare the immune, respiratory and gastrointestinal fetal sectors, and to protect fetal brain of the stress of childbirth, providing mothers a more efficient labor, and protection against bleeding. Scheduled birth (via labour induction or elective cesarean) impairs this process10. Anticipating birth can increase vulnerability to hypoxia and to fetal distress during induction. Cesarean section performed before the spontaneous term inhibits the increase of catecholamines in newborns, and may be an explanation to the increased breathing difficulty and to the differences in brain maturity of these babies11.
One of the important priorities for assistance should be to promote the birth of babies that are physiologically mature and capable of a spontaneous and successful fetal-neonatal transition12.
The objective of this research to analyze the left shift of gestational age (LDGA) in São Paulo City (SP) and in Southeastern Brazil, and associated factors.
METHODS
It is an epidemiological descriptive study of the curves GA at birth, by type of delivery and type of funding, in 2012, in São Paulo City (MSP) and in Southeastern Brazil. For this purpose, it was used the SINASC data for MSP and Brazil´s Southeast data for National Survey on Labour and Delivery - "Born in Brazil" (NNB). SINASC is a Brazilian database where is gathered epidemiological information regarding births.
For MSP, it was used the "Live Birth Declarations" (LBD) information obtained in SINASC database, provided by the Municipal Health Department for 2012, amounting 199,785 births. "Live Birth Declarations", in portuguese, Declaração de Nascido Vivo (DNV) is an official formulary filled in to every baby who is born alive.
Curves were built using data for GA (in weeks), based on the new classification proposed by the ACOG (5), for those who were born by normal birth and cesarean section, and type of financing. It was considered as "public" those hospitals fully paid by the Brazilian SUS (SUS, the initial for "Sistema Único de Saúde" is the Brazilian unified public health sector), and also those philanthropic health institutions serving SUS users, and "private", those hospitals whose funding was entirely private as well as those paid by insurance.
For the Southeast, we used data of all births studied by NNB during 2011-12, after complex sample weighting, with a total of 10,248 births. The infants' data were retrieved through interviews with their mothers and from the information collected from hospital records. In this research were included living newborns (any weight) or stillbirths weighing > 500g and / or GA > 22 weeks. Mothers unable to respond interview (i.e., severe mental disorder, not being a Portuguese speaker or deaf women), as well as legal abortion cases, were excluded.
For GA was used an algorithm developed to define the GA based on several variables available in NNB Survey, in order to create uniformity in the studies using this database. This algorithm comprises the following variables: GA estimated by LMP reported by the mother; GA at birth reported by the mother; GA estimated by the LMP documented in the mother's medical record; GA estimated by LMP reported in the medical record at the time of admission; GA estimated by USG reported in the medical record at the time of admission; IG estimated by the USG reported on antenatal record card13.
For the variable "source of funding", we considered the funding for the cost of delivery care, irrespective of where such assistance eventually occurred. Thus, it was possible to differentiate births funded by SUS, by health insurance or paid directly by the women in philanthropy or mixed hospitals.
The NNB was coordinated by the "Sergio Arouca" National School of Public Health (ENSP/FIOCRUZ) in partnership with several Brazilian institutions. Further details on the sampling process, data collection or other information about NNB are available in Leal et al.14, Vasconcellos et al.15 and Pereira et al.13. Ethical aproval for the NNB Survey was granted by the Fiocruz Ethical Committee and all women who agreed in taking part of the survey signed an informed consent. Data from the SINASC database are ethically protected and publicly avaliable.
RESULTS
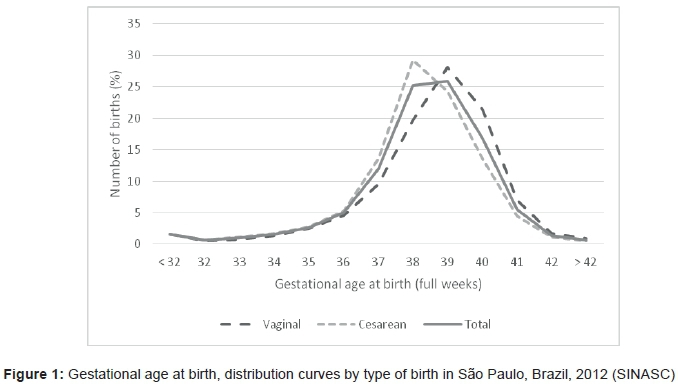
Figures 1 and 2 show the births on city of São Paulo (2012) for a total of 199,785 births, 42.3% (84 459) by vaginal delivery and 57.7% (115 326) by cesarean section.
The peak of the distribution curve of GA for those born by cesarean are at 38 weeks, whereas for those born by vaginal delivery is 39 weeks, with a left shift among those born by cesarean section (Figure 1). Most vaginal births occurred in the full term, while most cesareans occurred in the early term.
With regard to vaginal births, 14.4% (12 152) were funded by private sector, while 85.6% (72,307) had public funding, and for cesarean sections, the private sector funded 59.8% (68,979) and the public 40.2% (43,347).
Figure 2 shows that the peak of the GA for those born by cesarean section in the private sector occurred in 38 weeks (35%), with a large proportion of births before 38 weeks. In the public sector, these were less frequent and its peak was at full term, with 28% of births at 39 weeks and 22% at 40 weeks. This demonstrates a remarkable left shift in births by caesarean section in private sector.
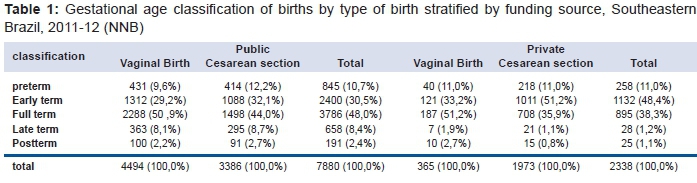
In the private sector, vaginal births were less frequent and occurred between 38 and 39 weeks. In the public sector, these show a peak at full term, with a concentration in 39 and 40 weeks. The mean GA (weeks) in Southeastern Brazil with data from the NNB was 38.36, in the early term period. Full term period birth were 45.7%.
However, those born in the private sector had a lower GA at birth, and 59.4% were born in preterm and early term periods. In the public sector, 41.2% were born in preterm and early term, and 59,8% of births took place after 39 weeks of gestation. (Table 1). Observing the division between the types of birth in the private sector, we can see that this shift occurs mainly when there was a cesarean, since 62.2% of them occurred in preterm or early term.
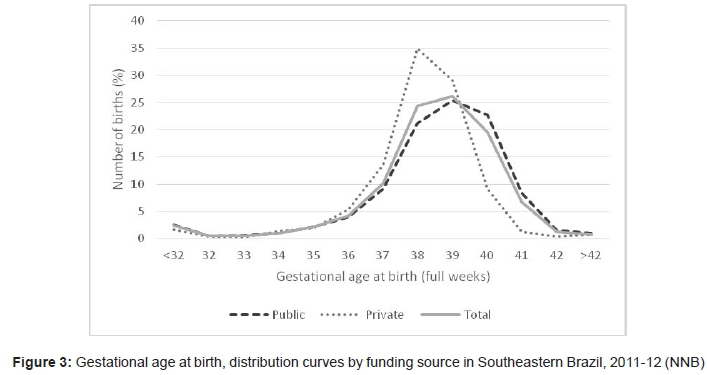
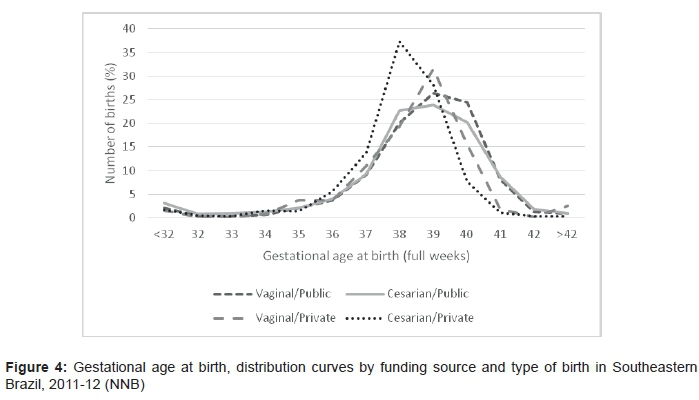
Figures 3 and 4 express graphically the GA at birth for infants in Southeast Brazil in the NNB data. When analyzing the GA distribution curve in Figure 3, the peak of the curve births in the private sector is in early term, while in the public sector, the peak of the curve is at full term. When separating the curves by type of birth (Figure 4), it is noted that those born by vaginal delivery with private funding has peak at 39 weeks, and only births by caesarean section with private funding have peak at 38 weeks. Higher proportions of newborns are found at 37 weeks in private sector, and a much higher proportion of babies born at 40 weeks of gestation in the public sector.
DISCUSSION
Over the past 30 years, since the meeting of WHO experts who drafted the "Fortaleza consensus" in 1985, the international community has considered that the ideal rate of cesarean section should be between 10-15%, since rates below or above these would be associated with poorer outcomes for mothers and babies. In 2015, an extensive review of the topic reaffirmed these rates for the general population, although this rate could be higher or lower, depending on the needs of mothers and babies in particular cases16.
This updated recommendation brings attention to the fact that when performed with real clinical indication cesareans can effectively reduce maternal and perinatal mortality and morbidity, and should be available to all women who need it. However, for women or babies who do not need it, there is no evidence of any benefit, and there is strong evidence of potential harm, with increased maternal and neonatal morbidity and mortality in the short and long term alike16. Elective caesareans also have increased risk of puerperal fever due to infections in surgical wounds, as well as greater difficulties in the care of the newborn. For these reasons the option of a caesarean section should be well justified and women should be informed properly about the risks associated with this surgical procedure17.
For newborns, it is associated with higher rates of preterm births, respiratory problems, hospital readmissions in neonatal intensive care unit and difficulties with breastfeeding. These risks can be even higher depending on the GA at birth. For example, the risk of serious respiratory morbidity is almost four times higher in neonates born at 37 weeks of GA, three times higher in newborns at 38 weeks and two times higher in newborns with 39 weeks18.
In the long-term, infants born via caesarean section have a higher risk of developing autoimmune diseases such as asthma, allergies, type 1 diabetes and celiac disease. Research has also indicated that there is a strong association between cesarean section and factors such as overweight or obesity19,20. Moreover, it has been shown that children born preterm also have a significantly lower performance in motor development, cognition and socialization compared to children without risk conditions identified at birth21.
However, these risks are not informed to pregnant women. On the contrary, during the interaction with the doctor during antenatal care there is an overestimation of the vaginal birth risks or for continue of pregnancy to beyond 38 weeks. These risks are often designed for the baby, who could "get distressed" if a caesarean section was not performed immediately. Thus, mainly because of the threat to the baby's safety, women are led to believe that cesarean section is safer for herself and for her baby, and to interrupt a pregnancy without clinical indication before 39 weeks is safer than wait for the full-term period22,23.
To overcome the present situation of stagnation in maternal and perinatal health indicators, particularly on the early neonatal component and the increase in preterm births, the main challenge in Brazil is changing the institutional culture toward an evidence based care, guided by human rights, sexual and reproductive health rights for woman9.
The current is the high medicalization and unregulated use of potentially harmful interventions in vaginal delivery and abuse of cesarean sections, may be canceling some positive effect on the health of mothers and babies, that was achieved by other beneficial interventions, such as universal pregnancy and childbirth care, high immunization coverage, and improvement of living conditions, maternal education and income24.
The LSGA observed in this study has also been observed in other studies in Brazil, as indicated by the results of the cohorts developed in the city of Pelotas, Brazil. The prevalence of preterm births increased from 6.2% in 1982 to over 15% in 2004, and births at 37 weeks also increased from 7.1% in 1982 to 11.4% in 2004. Although the causes for this increase in preterm births are not clear, it is possible that the early termination of pregnancies have an important role, considering that the cesarean rate doubled between 1982 and 200425.
According to the results of these cohorts the relative risk of neonatal death presented before 34 weeks was more than 30 times higher when compared to the group between 39 and 41 complete weeks. Using the same comparison group, babies born between 34 and 36 weeks had a relative risk 3.4 times higher, those born at 37 weeks had an almost three times higher rick and Post-term babies a double the risk25.
Preterm newborns, as well as those born at 37 weeks of pregnancy also had a higher risk of infant mortality. All preterm infants, including those born between 34 and 36 weeks were more likely to underweight at 12 months of age, as well as those born at 37 weeks GA. This corroborates the findings of international studies indicating that 37 weeks NB have more similar characteristics to preterm babies than those born full-term25.
Preliminary data from the Pelotas cohort (2015) have indicated that although women have improved socioeconomic status and have greater access to health services, the situation of newborns did not follow the same pattern of improvement. The low birth weight was 5% among the richest, and increased to 12%, and prematurity overall increased from 6% to 20% in 2015. Cesarean sections increased from 27% to 63% and infant mortality fell from 36 per thousand to less than 15 per thousand showing that "services save more babies, but they are born worse than 30 years ago"*.
Recent studies indicate that some aspects of the historical trend of inequality - the richest women have better neonatal outcomes - are being inverted. From 1995 to 2007, higher rates of low birth weight in Brazil are found in developed regions26. This is an "inversion of the expected disparity." The poorer results (more prematurity, lower birth weight) require more technology to compensate them, and most neonatal intensive care units are concentrated in richer areas27.
The stabilization of neonatal mortality rates in the last decade when a fall was expected possibly has to due to an excess of interventions during pregnancy and childbirth24. The abuse of interventions in childbirth has little regulation in both sectors, and adverse events are not reported or inquired systematically.
The promotion, support and protection of hormonal processes of spontaneous labor, delivery and postpartum is important for all women and newborns. Health professionals play a critical role in the preservation of physiological processes, using interventions only when it is really needed, knowing that such interventions can involve potential harm for the mothers, babies or both11.
As limitations of this study, in the case of the Birth in Brazil Survey, as any cross-sectional design, information on exposures and outcomes were collected simultaneously, making it impossible to establish a causal relationship. In the SINASC (universal livebirth database) data do not distinguish between women assisted in a mixed or philanthropic (private) hospital who had public financing, and those assisted with private funding in these hospitals. The decision was to include all women as public funded, regardless of the hospital status. However, the NNB data does allow this distinction, so that women assisted in mixed or philanthropic hospitals were considered separately, depending on the individuals public or private funding for childbirth care.
Among the strengths of the study, we highlight the fact that the MSP birth data (SINASC) are population-based, and that the NNB have a complex and representative sample of the most populous region of the country, where the City of São Paulo is included, ensuring greater robustness for the findings, and for the same period (2011-2012). The fact that these data converge to the same findings in the two databases, reinforces the robustness of the analysis.
Final considerations and recommendations for public policy-making
Although the LSGA and cesarean section have increased across the population, in Brazil both the reduction of GA and caesarean sections are more associated with the private sector users with higher education and income, unlike other countries, where they are characteristics of most socially vulnerable women. Babies of the richest women have a shorter G I at least a week compared to the whole population in Brazil.
These differences are an example of the Brazilian perinatal paradox, where women of higher socioeconomic status, private sector users with greater access to the consumption of medical services, may have some perinatal outcomes (birth at full term, respiratory complications, admission to NICU), worse than the poorest populations28.
In terms of equity, we have an inversion of the expected disparity by worsening of the indicators of the most privileged people, not by the improvement of services offered. When this inversion occurs, the safety of health care might be contributing to change the outcome, having a negative weight (iatrogenic) what can even nullify the socioeconomic advantages. In other words, it is not that the assistance to disadvantaged women is better, but that the assistance to the well-off women (with higher cesarean rates, mostly without any chance to go into labor) are more associated with adverse events such as preterm delivery and low birth weight, reducing benefits associated with income and education8.
The use of continuous variables in the estimation of GA (in weeks and / or days) can contribute to a better understanding of the Brazilian perinatal paradox, providing a deeper understanding of the role of health care to promote, or to hinder, the health and wellbeing of women and babies not only during the perinatal period, but also with consequences to their life course.
Statement of responsibility
Specific contributions: Simone G. Diniz proposed the concept of inversion of the expected disparity, the indicator days of potential pregnancy lost, and proposed a first draft of the paper. Marina Miranda worked in the acquisition, analysis and interpretation of SINASC data. Marcel Queiroz worked in obtaining, analysis interpretation of Birth in Brazil National Survey. Jessica Reis-Queiroz and Heloisa Salgado contributed content, critical review and standardization of the manuscript. All authors contributed to the design, planning, critical discussion of the content, review and final approval of the manuscript. There is no conflict of interest of the authors regarding this manuscript.
Acknowledgments
We thank the professional staff of SINASC from the Municipal Health Secretariat of São Paulo for granting the birth data for the year 2012. We also thank the regional and state coordinators, supervisors and interviewers from research "Born in Brazil," as well as to participating mothers.
REFERENCES
1. Nassar N, Schiff M, Roberts CL. Trends in the distribution of gestational age and contribution of planned births in New South Wales, Australia. PLoS One. 2013;8(2):e56238. DOI: http://dx.doi.org/10.1371/journal.pone.0056238 [ Links ]
2. Spong CY. Defining "Term" Pregnancy. Recommendations From the Defining "Term" Pregnancy. Workgroup. JAMA. 2013;309(23):2445-6. DOI: http://dx.doi.org/10.1001/jama.2013.6235. [ Links ]
3. Loftin RW, Habli M, Snyder CC, Cormier CM, Lewis DF, DeFranco EA. Late preterm birth. Rev Obs Gynecol. 2010;3(1):10-19. [ Links ]
4. Blencowe H, Cousens S, Oestergaard MZ, Chou D, Moller A-B, Narwal R, et al. National, regional, and worldwide estimates of preterm birth rates in the year 2010 with time trends since 1990 for selected countries: a sectoratic analysis and implications. Lancet. 2012; 79(9832):2162-72. DOI: http://dx.doi.org/10.1016/S0140-6736(12)60820-4. [ Links ]
5. The American College of Obstetricians and Gynecologists (ACOG). Committee on Obstetric Practice Society for Maternal-Fetal Medicine. Definition of term pregnancy. Obstet Gynecol. 2013;122:1139-40. [ Links ]
6. Engle WA. Morbidity and mortality in late preterm and early term newborns: a continuum. Clin Perinatol. 2011;38(3):493-516. DOI: http://dx.doi.org/10.1016/j.clp.2011.06.009 [ Links ]
7. Wu CS, Sun Y, Nohr EA, Olsen J. Trends in All-Cause Mortality across Gestational Age in Days for Children Born at Term. PLoS One. 2015; 10(12):e0144754. DOI: http://dx.doi.org/10.1371/journal.pone.0144754 [ Links ]
8. Diniz SG, d'Oliveira AF, Lansky S. Equity and women's health services for contraception, abortion and childbirth in Brazil. Reprod Health Matters. 2012;20(40):94-101. DOI: http://dx.doi.org/10.1016/S0968-8080(12)40657-7 [ Links ]
9. Leal MC, Pereira APE, Domingues RMSM, Theme Filha MM, Dias MAB, Nakamura-Pereira M, et al. Intervenções obstétricas durante o trabalho de parto e parto em mulheres brasileiras de risco habitual. Cad Saude Publica. 2014; 30(suol.1):17-32. DOI: http://dx.doi.org/10.1590/0102-311X00151513 [ Links ]
10. Hillman N, Kallapur SG, Jobe A. Physiology of transition from intrauterine to extrauterine life. Clin Perinatol. 2012;39(4):769-83. DOI: http://dx.doi.org/10.1016/j.clp.2012.09.009 [ Links ]
11. Sakala C, Romano AM, Buckley SJ. Hormonal physiology of childbearing, an essential framework for maternal-newborn nursing. J Obstet Gynecol Neonatal Nurs. 2016; S0884-2175(15)00052-0. DOI: http://dx.doi.org/10.1016/j.jogn.2015.12.006 [ Links ]
12. Engle WA, Kominiarek MA. Late preterm infants, early term infants, and timing of elective deliveries. Clin Perinatol. 2008; 35(2):325-41. DOI: http://dx.doi.org/10.1016/j.clp.2008.03.003 [ Links ]
13. Pereira APE, Leal MC, Gama SGN, Domingues RMSM, Schilithz AOC, Bastos MH. Determinação da idade gestacional com base em informações do estudo Nascer no Brasil. Cad Saude Publica. 2014;30(supl.1):S59-70. DOI: http://dx.doi.org/10.1590/0102-311X00160313 [ Links ]
14. Leal MC, da Silva AA, Dias MA, da Gama SG, Rattner D, Moreira ME, et al. Birth in Brazil: national survey into labour and birth. Reprod Health. 2012; 9:15. DOI: http://dx.doi.org/10.1186/1742-4755-9-15 [ Links ]
15. Vasconcellos MTL, Silva PLN, Pereira APE, Schilithz AOC, Souza Junior PRB, Szwarcwald CL. Desenho da amostra Nascer no Brasil: Pesquisa Nacional sobre Parto e Nascimento. Cad Saude Publica. 2014;30(supl.1): S49-58. DOI: http://dx.doi.org/10.1590/0102-311X00176013 [ Links ]
16. World Health Organization (WHO). WHO statement on caesarean section rates. Geneva: World Health Organization; 2015. [ Links ]
17. Bordner K, Wierrani F, Grünberger W, Bodner-Adler B. Influence of the mode of delivery on maternal and neonatal outcomes: a comparison between elective cesarean section and planned vaginal delivery in a low-risk obstetric population. Arch Gynecol Obstet. 2011;283(6):1193-8. DOI: http://dx.doi.org/10.1007/s00404-010-1525-y [ Links ]
18. Hansen AK, Wisborg K, Uldbjerg N, Henriksen TB. Risk of respiratory morbidity in term infants delivered by elective caesarean section: cohort study. BMJ. 2008;336:85-7. DOI: http://dx.doi.org/10.1136/bmj.39405.539282.BE [ Links ]
19. Cho CE, Norman M. Cesarean section and development of the immune sector in the offspring. Am J Obstet Gynecol. 2013; 208(4):249-54. DOI: http://dx.doi.org/10.1016/j.ajog.2012.08.009 [ Links ]
20. Darmasseelane K, Hyde MJ, Santhakumaran S, Gale C, Modi N. Mode of Delivery and Offspring Body Mass Index, overweight and obesity in adult life: a systematic review and meta-analysis. PLoS One. 2014;9(5):e97827. DOI: http://dx.doi.org/10.1371/journal.pone.0097827 [ Links ]
21. Rodrigues OMPR, Bolsoni-Silva AT. Effects of the prematurity on the development of lactentes. Rev Bras Crescimento Desenvolv Hum. 2011;21(14):111-21. [ Links ]
22. Domingues RMSM, Dias MAB, Nakamura-Pereira M, Torres JA, d'Orsi E, Pereira APE, et al. Processo de decisão pelo tipo de parto no Brasil: da preferência inicial das mulheres à via de parto final. Cad Saude Publica. 2014;S101-16. DOI: http://dx.doi.org/10.1590/0102-311X00105113 [ Links ]
23. Lino HC, Diniz SG.You take care of the baby's clothes and i take care of the delivery" - communication between professionals and patients and decisions about the mode of delivery in the private sector in São Paulo, Brazil. J Hum Growth Dev. 2015;25(1):117-24. DOI: http://dx.doi.org/10.7322/jhgd.96825 [ Links ]
24. Victoria CG, Aquino EML, do Carmo Leal M, Monteiro CA, Barros FC, Szwarcwald CL, et al. Maternal and child health in Brazil: progress and challenges. Lancet. 2011; 377(9780):1863-76. DOI: http://dx.doi.org/10.1016/S0140-6736(11)60138-4 [ Links ]
25. Barros FC, Rossello JLD, Matijasevich A, Dumith SC, Barros AJD, Santos IS, et al. Gestational age at birth and morbidity, mortality, and growth in the first 4 years of life: findings from three birth cohorts in Southern Brazil. BMC Pediatr. 2012;12(1):169. DOI: http://dx.doi.org/10.1186/1471-2431-12-169 [ Links ]
26. Silveira MF, Santos IS, Barros AJD, Matijasevich A, Barros FC, Victora CG. Aumento da prematuridade no Brasil: revisão de estudos de base populacional. Rev Saude Publica. 2008; 42(5):957-64. DOI: http://dx.doi.org/10.1590/S0034-89102008000500023 [ Links ]
27. Silva AAM, Silva LM, Barbieri MA, Bettiol H, Carvalho LM, Ribeiro VS, et al. The epidemiologic paradox of low birth weight in Brazil. Rev Saúde Pública. 2010; 44(5):767-75. DOI: http://dx.doi.org/10.1590/S0034-89102010005000033 [ Links ]
28. Diniz CSG. Gênero, saúde materna e o paradoxo perinatal. Rev Bras Crescimento Desenvolv Hum. 2009;19(2):313-26. [ Links ]
Manuscript submitted: Jan 16 2016
Accepted for publication Feb 18 2016.
* Corresponding author: Carmen Simone Grilo Diniz - E-mail: sidinizg@gmail.com


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}