










Serviços Personalizados
Journal

artigo
 Inglês (pdf)
Inglês (pdf)
 Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
Indicadores
Compartilhar

 Permalink
PermalinkJournal of Human Growth and Development
versão impressa ISSN 0104-1282versão On-line ISSN 2175-3598
J. Hum. Growth Dev. vol.26 no.2 São Paulo 2016
https://doi.org/10.7322/jhgd.119237
ORIGINAL RESEARCH
Tracking the origins, defining and quantifying quality of care: Can we reach a consensus?
Malgorzata Nabialczyk-Chalupowski MD PhD JD
Harvard T.H. Chan School of Public Health, Takemi Program in International Health
ABSTRACT
This editorial presents a summary of the narrative used in teaching fundamentals of quality management in healthcare to medical students and health professionals with limited or negative prior experience in the field of quality monitoring and improvement - i.e. those who find the topic dry and disconnected from their everyday clinical experience, lacking in human dimension, and confusing due to the multitude of definitions of quality of care and the considerable inconsistency of the terminology used in quality assessment. In order to remedy the problem, the topic is presented through an historical perspective of the concept of quality as seen throughout the ages - beginning in antiquity, through 19th and early 20th century quality control initiatives which evolved into the quality management policies and culture now firmly present in many of the contemporary domains of human endeavor. It is also envisioned that specific tools developed in this study for didactic purposes (a new definition of quality of care and a framework for classifying quality indicators) may play a role in encouraging a more effective dialog among all those passionate about the issue of healthcare quality monitoring, assessment, and improvement.
Key words: quality of care, management, ethical and healthcare.
RESUMO
Este editorial apresenta um resumo da narrativa usada nos fundamentos de ensino de gestão da qualidade em saúde para estudantes de medicina e profissionais de saúde com experiência prévia limitada ou negativa no domínio da monitorização e melhoria de qualidade - ou seja, aqueles que acham o tópico seco e desconectado de seu experiência clínica diária, falta de dimensão humana e confusa devido à infinidade de definições de qualidade dos cuidados e a inconsistência considerável da terminologia utilizada na avaliação da qualidade. Afim de remediar o problema, o tema é apresentado através de uma perspectiva histórica do conceito de qualidade como visto ao longo dos tempos - começando na antiguidade, através de iniciativas de controle de qualidade no início do século 20 que se transformaram nas políticas e cultura de gestão da qualidade agora firmemente no século19 e presente em muitos dos domínios contemporâneos do esforço humano. Também está previsto que as ferramentas específicas desenvolvidas neste estudo para fins didáticos (uma nova definição de qualidade dos cuidados e um quadro para a classificação de indicadores de qualidade) podem desempenhar um papel no sentido de incentivar um diálogo mais eficaz entre todos os apaixonados da questão da qualidade da saúde monitorização, avaliação e melhoria.
Palavras-chave: qualidade do cuidado; gerenciamento, ética e cuidado de saúde.
INTRODUCTION
The concept of quality - understood as a measure of doing the right thing in the right way at the right time and for the right reason in order to obtain a desired outcome - is as old as recorded human history.
All major world religions contain sets of rules, instructions, or guidelines designed to help their followers make right decisions and achieve desired results. Similar examples can be found in the history of literature, philosophy, and the military.
One of the pioneers of quality-related ways of thinking would be the ancient Greek storyteller Aesop (620-564), who is credited with creating a number of fables containing quality management-related morals useful for problem-solving and making right decisions1.
A treatise compiled by the legendary Chinese military strategist and philosopher Sun Tzu (544-496) contains principles and tactics necessary to overcome specific psychosocial obstacles, discord, and opposition in order to achieve desired organizational outcomes2.
Later, Socrates (469-399), whose teachings, as recorded by Plato and Aristophanes, promote self-examination and continuous self-improvement, developed a concept of didactic inquiry that leads to an improvement in understanding of issues, a technique still commonly used in education and law.
Quality Management in Industry
Sun Tzu's ancient technique of the strategic management of obstacles can be seen as having a direct connection with the ideas of modern quality management, which emerged in the manufacturing industry in the early 20th century and advanced to the point of being used by the U.S. Defense Department in World War II.
The early 20th century quality pioneers, often referred to as the 'grandfathers' of the quality management movement - Walter Shewhart, Harry Romig, George Edwards, and Harold Dodge - were followed by early American gurus of quality management such as W. Edwards Deming, Joseph Juran, and Armand V. Feigenbaum, who, having been underestimated in the U.S., took their message to Japan in the early 1950s, when invited by General Douglas McArthur3.
In Japan, the idea of quality management flourished once it merged with the Zen Buddhist philosophy of continual change and learning and was combined with the specifically Japanese managerial culture called Kaizen: the carefully nurtured, process-oriented way of thinking that works smoothly and steadily and values people on both sides of the process - the providers and the consumers of products and services. Quality improvement, promoted and developed by a number of Japanese quality gurus (e.g. Karou Ishikawa, Genichi Taguchi, Shigeo Shingo, Masaaki Imai) is credited for the unprecedented success of Japanese industry starting in the late 1950s and excelling in the 1970s and 1980s*.
By the 1970s, the West did catch up with the teachings of the early American quality pioneers and became much more receptive to the quality improvement ideas enthusiastically promoted by the new wave of Western quality management experts and bestselling authors such as Peter Drucker (Managing for the Future); Philip Crosby (Quality without Tears, The Eternally Successful Organization); Claus Moller (Personal Quality - The Basis of All Other Quality); and Tom Peters, (In Search of Excellence, Thriving on Chaos, The Little Big Things).
By the time these bestsellers became part of Western society's collective awareness of quality management-oriented ways of thinking, medicine and healthcare delivery systems in general had managed to build a considerable cultural foundation, which, in some instances, actually preceded the comparable efforts in quality management and improvement pursued in other domains of human endeavor.
Quality Management in Medicine
The history of efforts to ensure quality of care in medicine can be traced back in the East to Sushruta (6th century BC) - the author of the oldest known medical textbook - and in the West, to Hippocrates (460-370).
Hippocrates, the father of Western medicine and author of the oath, which constitutes a fundamental set of rules, instructions, guidelines, and professional ethical standards binding all physicians and other healthcare professionals,* is also known for accepting women into his training, although shortly after his death being a female doctor in Athens became a capital crime.
Gaius Julius Hyginus (64-17), author of Fabulae, records the story of the first legendary female gynecologist, Agnodice, educated at the University of Alexandria, Egypt, under Herophilos (335-280), one of the founders of the scientific method in medical inquiry. As the story has it, Agnodice disguised herself as a man to be able to practice obstetrics. When caught, tried, and condemned by the court for deceit and false pretense, Agnodice was acquitted after her patients arrived at her trial to praise the quality of the services she provided. As a result, Athenians changed the law to allow women to be treated by female physicians. According to some historians, Agnodice may be a mythical figure; however the story of her acquittal serves as a useful parable illustrating the power of patient satisfaction in setting standards of care4.
During the following several centuries, standards of care were based mostly on custom and oral tradition until the time of the Greek physician, Soranus of Ephesus (98-138). Soranus, commonly considered the foremost medical authority in antiquity, set standards of medical practice for nearly fifteen hundred years, with a specific emphasis on women's diseases, pregnancy and infant care.
Soranus, who like Hippocrates, emphasized the importance of collecting facts through accurate observation, and considering the best interest of the patient, is believed to have inspired Leonardo Da Vinci's interest in reproductive anatomy5,6.
Interestingly, Leonardo Da Vinci's statement, "science comes by observation, not by authority," is remarkably compatible with our contemporary concept of evidence-based medicine, which in the history of maternal and child health can be traced back to a number of landmark events, such as the initiative of the Swedish Health Commission to collect data about "avoidable maternal mortality" undertaken as early as 17517; or the observations regarding the spread and prevention of puerperal fever made by Alexander Gordon in Aberdeen in 1795 and by Ignaz Semmelweis in Vienna in 1847. Remarkably, both Gordon and Semmelweis were viciously ridiculed for voicing their groundbreaking ideas8. They did it anyway, like scores of their fellow physicians throughout the ages, who, intentionally or instinctively acting in compliance with the Hippocratic Oath, in good faith and to the best of their abilities, have been carrying out their duty to care for the sick and dying and to share with the world any new understanding of things relevant to the practice of medicine.
In the 19th and early 20th century history of medicine, there are a number of significant forerunners who, while following the principles of the Hippocratic Oath, built a foundation for modern quality management in healthcare.
In 1848, Elisha Bartlett (1804-1855) a Massachusetts physician, politician, and writer, published his book, An Inquiry into the Degree of Certainty in Medicine, illustrating the early attempts to ensure the standards of the medical profession9.
At the same time in Europe, Florence Nightingale (1820-1910) a British aristocrat turned wartime nurse pioneered routine health outcome measures resulting in the reduction of the mortality rates of soldiers wounded in the Crimean war (1853-56). Similar credit for trying to record and improve the outcomes of care goes to Harvey Cushing (1869 -1939), "the father of modern neurosurgery," and his classmate at Harvard Medical School, Ernest Amory Codman (1869-1940), a Boston orthopedic surgeon who, in 1910, created the concept of 'end results' and put the idea into practice by recording the long-term outcomes of the treatment performed by different physicians and different hospitals10. Cushing and Codman's work contributed to the establishment of the Hospital Standardization Program by the American College of Surgeons in 1917. In 1910, Abraham Flexner (1866-1959), commissioned by the American Medical Association, produced a report that set the stage for the improvement of quality and outcomes of medical education in the United States and in Europe11.
Bartlett, Nightingale, Cushing, Codman, and Flexner are predecessors of the ideas, trends, and policies further developed in the later part of the 20th century by a growing number of physicians and other health professionals inspired and fascinated by the concept of monitoring and improving the quality of medical care and its outcomes.
Even though it is widely believed that the quality culture was adopted into healthcare from industry, the modern concept of monitoring the quality of care had been steadily taking hold in the practice of medicine concurrently with the early quality management efforts pursued in the manufacturing industry.
In a landmark publication, Evaluating the Quality of Medical Care published in 1966, Avedis Donabedian (1919-2000), a physician and public health expert, universally recognized as "the father of quality management in healthcare," acknowledges the work of many of his predecessors and unsung heroes of quality management in medicine. Donabedian lists over sixty references discussing various issues related to quality of medical care published throughout the 1930s, 1940s, 1950s, and early 1960s, including e.g. the 1933 book by R. I. Lee and L. W. Jones, The Fundamentals of Good Medical Care published by the University of Chicago Press, or the 1955 publication of M.C. Sheps, Approaches to the Quality of Hospitals Care, published in Public Health Reports12.
Considering the multitude of publications, an argument can be made that, when Donabedian proposed his structure-process-outcome paradigm and advocated the use of the industrial 'plan-do-check-act' cycle and other quality management methods and tools, parts of the medical community were well prepared to take on the challenge of self-evaluation for the purpose of facilitating the ongoing improvement of quality of care.
Defining Quality
Since Bartlett's and Codman's solitary efforts, we have come a long way in sharing our quality-related ideas, knowledge and skills, developing sophisticated tools for quality monitoring and improvement, such as quality indicators, adverse events audits, standards- or criterion-based audits, peer review, clinical practice guidelines, accreditation, risk management, meta-analysis, and most of all - evidence-based medicine. We have been conducting massive research efforts, creating quality-promoting professional organizations - governmental, commercial, or nonprofit - at national, regional, and international levels, as well as describing our quality improvement-driven achievements in hundreds of books and thousands of papers published around the world every year.
At the same time, the question remains as to what extent these ongoing efforts and the multitude of books and articles on quality management in healthcare translate into a better understanding of the quality of care concept, or into actual improvements of health outcomes on the national, regional, or global scale.
Indeed, back in 1980, Avedis Donabedian was already concerned that all those quality-driven activities "…have overwhelmed us with a flood of publications that are almost impossible to keep up with, let alone to assess as contributions to some larger design, especially since this muddy torrent of information seems to carry in its roiling rush an indiscriminate jumble of the new and the derivative, the meticulous and the careless, the honest and the manipulative, the well-informed and the unknowing, the wise and the perverse!"13.
If Donabedian had been worried then, what would he say today - 36 years and tens of thousands publications and scores of programs and initiatives later?
Today, we are still at the crossroads when it comes to reconciling and unifying different quality management methods, tools and approaches used in different healthcare systems around the world. There is no consensus as to the very definition of the concept of quality of care. Neither has there been much progress made in defining quality of care since Donabedian pointed out in one of his early works that "the definition of quality may be almost anything anyone wishes it to be, although it is, ordinarily, a reflection of values and goals current in the medical care system and in the larger society of which it is a part."12.
The numerous publications tackling the issue of defining quality of care take a 'pluralistic' approach, acknowledge numerous existing definitions (mostly out of an abundance of respect for various esteemed bodies or individuals who created them) and basically agree that no single definition of quality of care can be formulated14-20.
While it may be a philosophically (and politically) justified approach, for practical reasons, it would be worthwhile to adopt a single working definition of quality of care. In fact, such a definition should be able to help us reconcile the numerous existing definitions, while taking no undue credit for the temporary suspension of the ongoing dispute.
Under such a working definition, the quality of care is the degree to which the services rendered by a healthcare provider are in compliance with four specific criteria: (a) current scientific knowledge, (b) professional ethical standards, (c) applicable law, and (d) principles of fairness and equity. In short, the four criteria are science, ethics, law, and fairness**.
The operative concept here is the degree of compliance because quality of care is a continuum, with a scale ranging anywhere from poor to excellent. The degree of compliance with the four criteria listed in the definition (science, ethics, law, and fairness) indicates the level of quality of care. The criteria of the proposed definition of quality of care can be further described as follows:
(a) Current scientific knowledge
It is undisputed that all aspects of medical care have to be in compliance with evidence-based principles of practice. Moreover, this requirement relates not only to medical knowledge, but also to all other disciplines of human inquiry relevant to healthcare, including e.g. psychology, sociology, economics, architecture, or environmental sciences.
(b) Professional ethical standards
It is also undisputed that physicians, as well as representatives of all other professions involved in the delivery of care, are bound by their respective codes of professional conduct. The level of compliance with the rules of professional conduct indicates the level of quality of care.
(c) Applicable law
All healthcare organizations and individual providers function within specific systems of laws applicable at local, national, and international levels. These include, e.g. health and hospital law, contract law, intellectual property law, environmental law, employment law, and international law, with specific emphasis on civil and human rights.
(d) Principles of fairness and equity
The requirement of compliance with the principles of fairness and equity straddles both the ethical and moral dimension of medical practice, as well as the issue of respect for civil and human rights of individual patients, providers, and entire communities and populations. It also encompasses the issues of equitable social distribution of financial burden and access to care.
While the first component (compliance with current scientific knowledge) lends itself most readily to an objective evaluation, the exact measurement of the three other components may sometimes be less attainable. This does not mean however that it cannot be done, since, as some say, quality is like beauty - it may be difficult to define, but it can be measured.
Quantifying Quality
In the title of his article published in JAMA in September 1988, Donabedian poses a simple question: "The Quality of Care: How it Can be Assessed?"21.
Donabedian anchors the answer to this question in his structure-process-outcome paradigm, which is by now a universally recognized framework for assessing the quality of care in the context of both non-profit and for-profit healthcare organizations.
As far as the tools for measuring quality of care are concerned, the usefulness and wide applicability of quality indicators has been recognized since at least the early 1990s22.
According to the JCAHCO definition, an indicator is "a quantitative measure that can be used to assess and improve the performance of important governance, management, clinical, and support functions that affect patient outcomes."23.
The JCAHCO publication goes on to focus on process and outcome indicators of one specific type, which is the rate-based type of indicators.
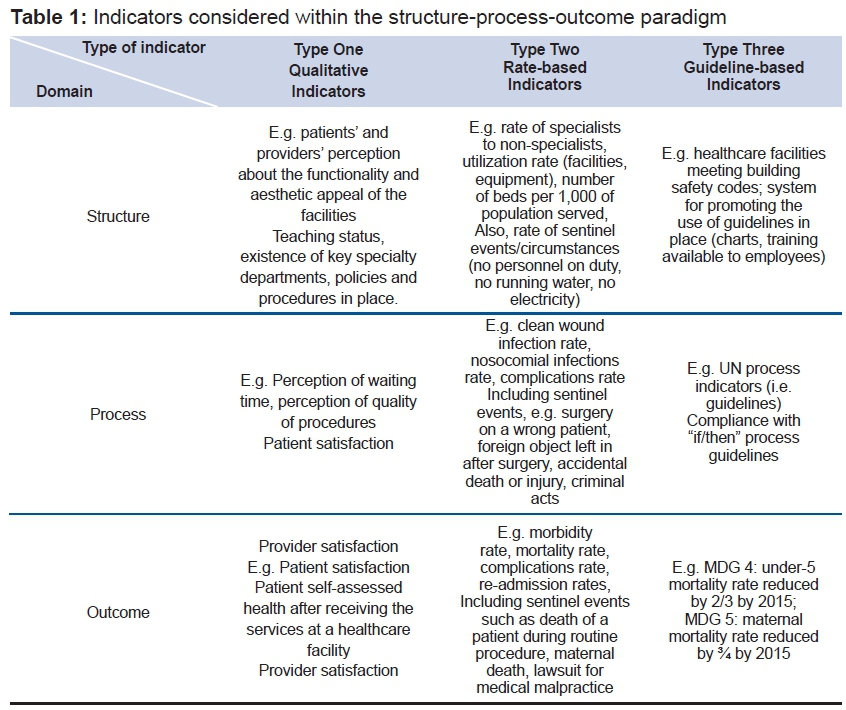
It may be argued that this partial typology can be put in the more comprehensive context of the complete structure-process-outcome paradigm on the one hand, while recognizing two other types of indicators: qualitative indicators and guideline-based indicators. As a result, a pattern of three types of indicators emerges, all considered within the classic structure-process-outcome framework.
- Qualitative indicators are based on qualitative information, which may be provided with or without assigned numeric values (narrative description only or with assigned numeric values, e.g. on a scale 1 to 5 describe the quality of care received, where 1 = bad, and 5 = excellent). The information provided through the qualitative indicators, if based on opinion, is mostly not validated.
- Rate-based indicators are rates, or independent numbers of studied events or characteristics, i.e. variables that lend themselves to quantification. In the case of rate-based indicators, the information may be partially validated (e.g. the numerator is an exact number of specific cases recorded in a study, while the denominator is derived from external demographic data sources regarding the size of a population).
- Guideline-based indicators measure the quality of care by ascertaining the degree of compliance with specific clinical guidelines, e.g. a percentage of patients treated in compliance with specific clinical guidelines. The information obtained through guideline-based indicators is fully validated, i.e. both the numerator (number of patients treated in compliance with guidelines) and the denominator (number of all eligible patients) are exact numbers recorded in the study (Table 1).
It is important to reach a consensus about the hierarchy of the relevant concepts, which can be summarized as follows:
Types of indicators:
- Qualitative - information is obtained by ascertaining patients' or providers' opinion;
- Rate-based - information is obtained by ascertaining the rate of observed events;
- Guideline-based - information is obtained by ascertaining the degree of compliance with specific guidelines, i.e. sets of instructions, recommendations, or algorithms (including clinical pathways) developed at the local, regional, national, or international level by applying evidence-based science.
Standards:
Agreed upon acceptable levels of compliance measured by using any of the indicators within the structure-process-outcome paradigm at the local, regional, national, or international level.
Final consideration
It is necessary to emphasize that quality management is not just one more organizational efficiency tool. It is an empowering philosophy of professionalism based in honesty, transparency, accountability, and respect for people on both sides of the process - the providers and the consumers of products and services.
Quality management is not about coming up with ways to deal with errors and dissatisfied customers. It is about building a system in which there are no errors or dissatisfied customers. In the manufacturing industry it is called the 'zero defects' strategy.
In healthcare such strategy would be attained by ensuring that the services rendered by an organization and individual providers are in compliance with the four specific criteria: science, ethics, law, and fairness.
The measure of quality is the degree to which our services are in compliance with the four criteria. In order to assess the degree of compliance, we use three types of indicators (qualitative, rate-based, and guideline-based) within the structure-process-outcome paradigm.
The concise framework proposed here may prove to be of the utmost practical importance, considering the fact that even a cursory review of the relevant literature on measuring quality of care reveals a multitude of existing frameworks and various classifications of quality of care indicators. This is in addition to a considerable inconsistency of terminology used by different researchers.
A consensus regarding defining and measuring quality may prove helpful in encouraging more effective dialogue among all those concerned with quality of care provided to our patients, communities, and nations in compliance with our universal human values based in science, ethics, law, and principles of fairness and equity.
The importance of our efforts cannot be overestimated. After all, as Tom Peters pointed out in his 1991 book Thriving on Chaos, "what gets measured, gets done."24
It is also envisioned that specifi c tools developed in this study for didactic purposes (a new defi nition of quality of care and a framework for classifying quality indicators) may play a role in encouraging a more effective dialog among all those passionate about the issue of healthcare quality monitoring, assessment, and improvement.
REFERENCES
1.Brocka M, Brocka, B. Quality Management: Implementing the Best Ideas of the Masters. McGraw-Hill; 1992. [ Links ]
2.Lo VHY. The strategic insights of Sun Tzu and quality management. TQM Magazine. 1998; 10(3): 161-8. DOI: http://dx.doi.org/10.1108/09544789810214774 [ Links ]
3.Gabor A. The Man who Discovered Quality. Random House; 1990. [ Links ]
4.Yount L. A-Z of Women in Science and Math: A Biographical Dictionary (Facts on File Library of World). Facts on File; 1999. [ Links ]
5.Temkin O. Soranus' Gynecology. Baltimore: Johns Hopkins University Press; 1956. [ Links ]
6.Dunn PM. Perinatal Lessons from the Past. Leonardo Da Vinci (1452-1519) and reproductive anatomy. Arch Dis Child Fetal Neonatal Ed. 1997;77: F249-51. DOI: http://dx.doi.org/10.1136/fn.77.3.F249 [ Links ]
7. Hogberg U. The decline in maternal mortality in Sweden; the role of community midwifery. Am J Public Health. 2004;94(8):1312-20. [ Links ]
8.Gould JM. Alexander Gordon, puerperal sepsis, and modern theories of infection control - Semmelweis in perspective. Lancet Infec Diseases. 2010;10(4):275-8. DOI: http://dx.doi.org/10.1016/S1473-3099(09)70304-4 [ Links ]
9.Williamson JW. Teaching Quality Assurance and Cost Containment in Health Care (Jossey Bass Higher & Adult Education Series). Jossey-Bass; 1982. [ Links ]
10.Millenson ML. Demanding Medical Excellence. University of Chicago Press; 1997 [ Links ]
11.Luce JM, Bindman AB, Lee PR. A brief history of health care quality assessment and improvement in the United States. West J Med. 1994;160(3):263-8. [ Links ]
12.Donabedian A. Evaluating the quality of medical care. Milbank Q. 1966;44(3):166-206. DOI: http://dx.doi.org/10.2307/3348969 [ Links ]
13.Donabedian A. Explorations in quality assessment and monitoring. V.1. Health Administration Press; 1980. [ Links ]
14.Reerink E. Defining quality of care: mission impossible. Qual Assur Health Care. 1990;2(3-4):197-202. [ Links ]
15.Palmer RH, Donabedian A, Povar GJ. Striving for quality in health care: an inquiry into policy and practice. Health Administration Press; 1991. [ Links ]
16.Campbell SM, Roland MO, Buetow SA. Defining quality of care. Soc Sci Med. 2000;51(11):1611-25. [ Links ]
17.Mainz J. Defining and classifying clinical indicators for quality improvement. Int J Q Health Care. 2003;15(6):523-30. DOI: http://dx.doi.org/10.1093/intqhc/mzg081 [ Links ]
18.Harteloh PPM. The meaning of quality in health care: a conceptual analysis. Health Care Anal. 2003;11(3):259-67. DOI: http://dx.doi.org/10.1023/B:HCAN.0000005497.53458.ef [ Links ]
19.Legido-Quigley H, McKee M, Nolte E, Glinos IA. Assuring the quality of health care in the European Union. A case for action. World Health Organization; 2008. [ Links ]
20.Panzer RJ, Gitomer RS, Greene WH. Increasing demands for quality measurement. JAMA. 2013;310(18):1971-80. DOI: http://dx.doi.org/10.1001/jama.2013.282047 [ Links ]
21.Donabedian A. The quality of care. how can it be assessed? JAMA. 1988;260(12): 1743-8. [ Links ]
22.Klazinga N. Indicators without a cause. Reflections on the development and use of indicators in health care from a public health perspective. Int J Qual Health Care. 2001;13(6):433-8. [ Links ]
23. Joint Commission on Accreditation of Healthcare Organizations. Accreditation Manual for Hospitals. Standars; 1991. [ Links ]
24.Peters T. Thriving on Chaos: handbook for a management revolution. Harper Perennial; 1991. [ Links ]
Manuscript submitted: Mar 21 2016
Accepted for publication Jun 12 2016
Corresponding author: Malgorzata Nabialczyk-Chalupowski - Email: mdphdjd@gmail.com
* In the mid-20 century, the values embedded in the Hippocratic Oath were endorsed and reaffirmed in the Declaration of Geneva adopted by the UN 2 General Assembly in 1948 and amended several times, most recently in 2006. Later, the Declaration of Helsinki adopted in 1964 and revised several times, most recently in 2013, set the standards for medical research ethics. Both documents, while not legally binding instruments under international law, contain ethical principles guiding healthcare professionals worldwide.
** The first letters of the four words form a meaningful acronym SELF, which carries a specific message in the context of quality management culture's commitment to self-examination, self-improvement, and self-fulfillment of individuals, teams, or entire professional communities.


{kind=link}