










Serviços Personalizados
Journal

artigo
 Inglês (pdf)
Inglês (pdf)
 Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
Indicadores
Compartilhar

 Permalink
PermalinkJournal of Human Growth and Development
versão impressa ISSN 0104-1282versão On-line ISSN 2175-3598
J. Hum. Growth Dev. vol.26 no.2 São Paulo 2016
https://doi.org/10.7322/jhgd.119298
CASE REPORT
Discal Cyst: a Rare Cause of Neurologic Compression in the Young Adult
André Nunes MachadoI; Rodrigo Junqueira NicolauII; Joice Anaize Tonon do AmaralIV; Renata SalatiniIV; Jiangyi WuV; Luciano Miller Reis RodriguesIII
ISpine Surgeon Fellow ABC Medical School - Brazil
IIOrthopaedic Assistent and Spine Surgeon at Albert Einstein Hospital - Brazil
IIIChief of Spine Surgery Group of ABC Medical School - Brazil
IVOrthopaedic Assistent and Spine Surgeon at Albert Einstein Hospital - Brazil
VPhD student. Department of Surger. School of Medicine, University of São Paulo- Brazil
ABSTRACT
INTRODUCTION: discal cysts are rare pathology. Its clinical presentation can be mistaken for disc herniation, with back pain, radiculopathy and neurological deficit. It is more common in male patients in their fourth life decade. Because they are rare, there is no consensus about the treatment. A great variety of procedures, from medication for the pain to endoscopic or microdiscectomy excision, have been described.
OBJETIVE: Describe a case of discal cyst on the l4-l5 level with compression of l5 right nerve root treated successfully with a minimal invasive procedure. : Case report.
METHODS: Review medical records, pertinent images, interview with the patient and surgical team, intraoperative and histopathological findings. The surgical technique used was minimally invasive.
RESULTS: Magnetic resonance imaging (MRI) demonstrated a cystic lesion imaging at the level of the L4-L5 disc. The cystic mass displaced the thecal sac dorsally compressed the L5 transversing root. The patient was submitted to a minimally invasive microendoscopic technique using a tubular retractor. He recovered completely after the procedure, presenting absence of leg pain and went back to his regular activities 3 weeks after the surgery. Histopathological examination of the cyst revealed thick fibrous connective tissue interspersed with areas of chronic inflammation.
CONCLUSION: Discal cysts are rare intraspinal lesions. They can trigger severe neurological symptoms, and should be differentiated from other forms of epidural cysts and tumors. There are many treatment options that can be chosen from but no consensus. We used a treatment that was less invasive than the ones described in the literature.
Key words: intervertebral disc, minimally invasive surgical procedures, sciatica, back pain, intervertebral disc displacement, radiculopathy.
RESUMO
INTRODUÇÃO: cistos discais são patologia rara. Sua apresentação clínica pode ser confundida com hérnia de disco, com dor nas costas, radiculopatia e déficit neurológico. É mais comum em pacientes do sexo masculino em sua quarta década de vida. Porque eles são raros, não há consenso sobre o tratamento. Uma grande variedade de procedimentos, de medicação para a dor para a endoscopia ou excisão microdiscectomy, têm sido descritas.
OBJETIVO: descrever um caso de cisto discal no nível L4-L5 com compressão da raiz nervosa L5 di-reita tratada com sucesso com um procedimento minimamente invasivo. Desenho do estudo: Relato de caso.
MÉTODO: revisão de registros médicos, imagens pertinentes, entrevista com o paciente e equipe cirúrgica, intra e histopatológicos. A técnica cirúrgica utilizada foi minimamente invasiva. : A ressonância magnética (MRI) demonstrou uma imagiologia lesão cística ao nível do disco L4-L5. A massa cística deslocou o saco tecal dorsal comprimido a transversing raiz L5. O paciente foi submetido a uma técnica microendoscópica minimamente invasiva utilizando um afastador tubular. Ele se recuperou completamente após o procedimento, apresentando ausência de dor nas pernas e voltou às suas atividades regulares 3 semanas após a cirurgia. O exame histopatológico do cisto revela tecido conjuntivo fibroso de espessura intercaladas com áreas de inflamação crónica.
CONCLUSÃO: cistos discais são lesões intra-espinhais raras. Eles podem desencadear os sintomas neurológicos graves, e deve ser diferenciada de outras formas de cistos epidurais e tumores. Há muitas opções de tratamento que podem ser escolhidos a partir de, mas não há consenso. Utilizou-se um tratamento que era menos invasiva do que os descritos na literatura.
Palavras-chave: disco intervertebral, procedimentos cirúrgicos minimamente invasivos, ciática, dor nas costas, o deslocamento do disco intervertebral, radiculopatia.
INTRODUCTION
In the adult population is common rFeports of pain symptoms and musculoskeletal imbalances, and occur predominantly in the lower back, neck and upper limbs1. Discal Cysts are expansive intraspinal extradural lesions, include synovial cysts, Tarlov perineural cysts, extradural arachnoid cysts, dermoid cysts, and neuromas with cystic changes2 which can cause different degrees of neurological compression leading to severe clinical symptoms3.
In the literature, there are few studies addressing this extremely rare pathology4,5. Depending on its location and size in the spinal canal, the lesion can cause symptoms that vary from low back pain, unilateral or bilateral radiculopathy. Discal Cysts can be severe, causing neurological deficits3,6-8. The clinical symptoms of lumbar discal cyst are usually indistinguishable from those of disc herniation and other causes of neurological compression3.
The advance of image techniques and magnetic resonance imaging (MRI) being more accessible worldwide, the diagnosis of these lesions has been facilitated, with more accurate knowledge of their origin and anatomic-clinic correlation9. The intraoperative detection of discal cysts and the confirmation whether a cystic lesion has been totally removed or if it has been entered during surgery, can be done through the intraoperative discography10.
There is no consensus on the treatment choices to address these lesions, because is a rare pathology. Several options and approaches have been described, such as: conservative treatment, percutaneous radiological guided injection, endoscopic resection, microscopic decompression3,11-13, microsurgical discectomy and cyst excision(14) have been described.
The purpose of this case report is to present the outcome of treatment of neurological compression caused by a discal cyst using a minimally invasive decompression technique, and to review the main aspects of this rare pathology.
CASE REPORT
A 27 year old male had a history of low back pain following physical activity that was part of his routine. After simple treatment with analgesics and rest, his back pain symptoms improved. One month after the onset, he started presenting severe right leg pain, which followed mainly L5 dermatome. His physical examination presented with positive straight leg test within 10 degrees, in the right leg. He also had a grade 4 weakness on foot extension, and incapacity to walk in his heels, on the right side. Reflex was bilaterally normal. Even with analgesics and opioids his symptoms got worse. His VAS (visual analog scale) score was 9.
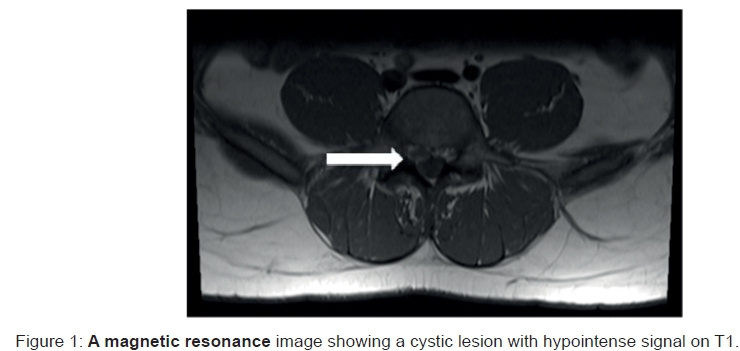
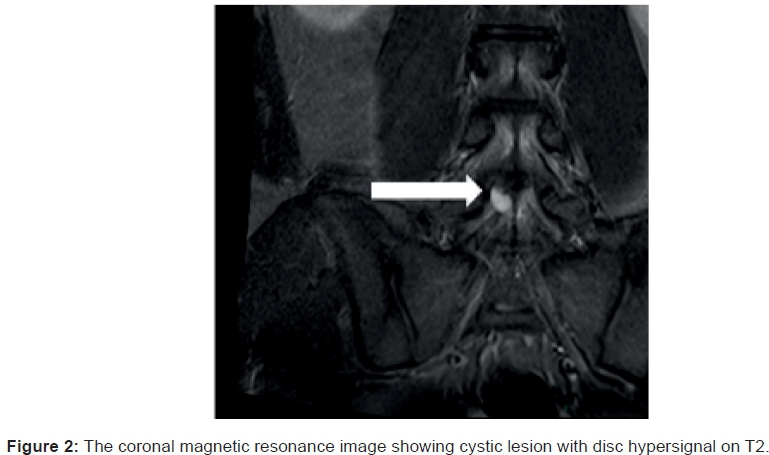
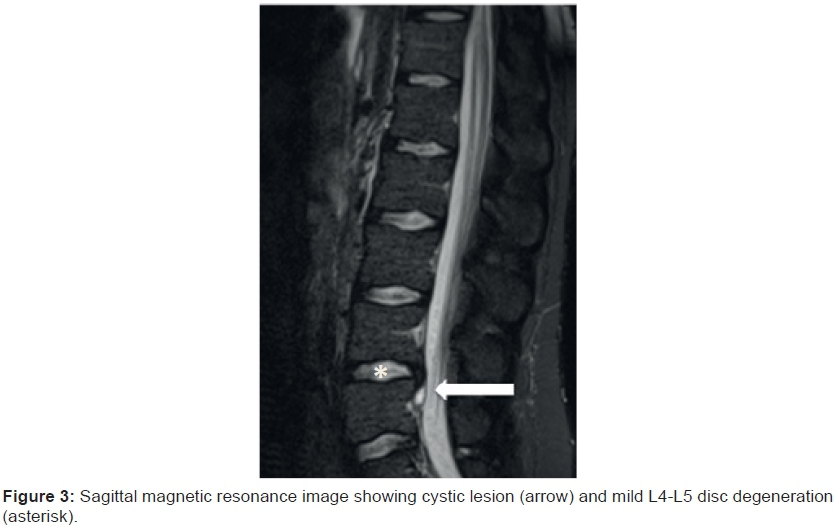
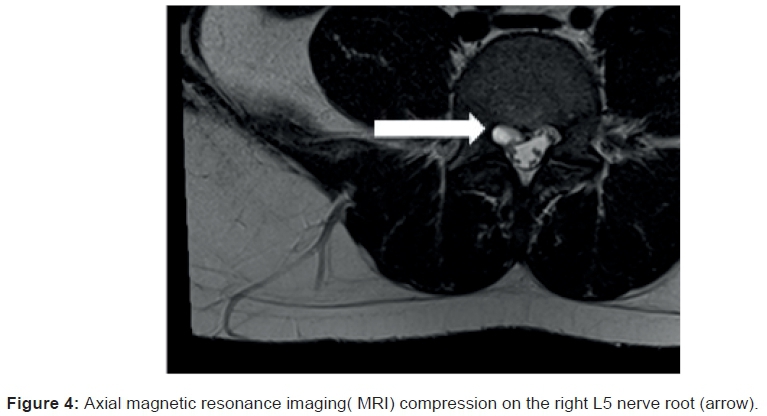
Magnetic resonance imaging (MRI) demonstrated a cystic lesion with low-signal intensity on T1-weighted imaging and high-signal intensity on T2-weighted imaging at the level of the L4-L5 disc (figure 1, 2). The cystic mass, located in the ventral aspect of the extradural space, displaced the thecal sac dorsally. The L4-L5 intervertebral disc appeared to have mild degeneration (figure 3). In the axial view it was located in the center laterally to the right side in the spinal canal, compressing the L5 transversing root (figure 4).
The patient was submitted to a minimally invasive microendoscopic technique using a tubular retractor, after a 2 cm incision. A conservative laminotomy was done, followed by a partial flavectomy. The integrity of the facet joint in the right side was maintained. Once in the epidural space, the L5 nerve root was carefully retracted and a dark blue-colored cyst was identified. The cyst was found mildly attached to both the thecal sac and the posterior longitudinal ligament (PLL). The bloody serous fluid was aspirated from the cyst. The cyst was traced back to its stalk, which communicated with the L4-L5 disc by a central annular tear. The cyst and stalk were excised completely at the base of its connection. Coagulation of the PLL surrounding a round defect was performed. The disc space was not entered.
The patient recovered completely after the procedure, presenting absence of leg pain, only a mild back pain in the surgery region. He was discharged 24 hours after the procedure. He started physiotherapy one week following the procedure and went back to his regular activities 3 weeks later. Within 6 weeks he started jogging.
Histopathological examination of the cyst revealed thick fibrous connective tissue interspersed with areas of chronic inflammation. However, there was no evidence of specific lining cell layers or disc material.
Twelve months after the procedure the patient was completely symptoms free. The new MRI( did not show any signs of recurrence, only keeping the same discopathy in L4/5.
DISCUSSION
Since described in 2001 to Chiba et.al4, the discal cyst has been approached in several forms. From conservative treatment, percutaneous CT-guided puncture and steroid injection, percutaneous endoscopic surgery and microscopic decompression3,11-13. All of these treatment options are described due to the rarity of this disease, lack of studies regarding it and absence of consensus about the best way to deal with this lesion14.
The percent of the cases is bigger in men, ninety percent, with age ranging from 13 to 73 years (mean 33.8, median 31.1), the mean age of the patients with discal cyst is younger than the patients with disk prolapse. Marushima et al.15 point that the simple pre existence of water-containing degenerated disk is sufficient to compose serous fluid of the cysts. The most common cyst locations were L4-L5 in 21 patients (36.8%), followed by L5-S1 in 16 patients (28.1%), L3-L4 in 12 patients (21.1%), L2-L3 in 5 patients (8.8%) and L1-L2 in 3 patients (5.2%).
Two hypotheses for the physiopathology of discal cysts have been proposed. Chiba et al.4 hypothesized that an epidural hematoma is initially formed from hemorrhage of the epidural venous plexus that occurs in the space between the peridural membrane and the vertebral body, and discal cysts form most likely as a consequence of impairment of hematoma resorption. As also, Murata et al.16 studied a case and hypothesis that the haemorrhage of the epidural venous plexus caused by separation of the peridural membrane.
However, this theory does not explain the communicating stalk between the intervertebral disc and the cyst. Recently, focal degeneration was proposed by Kobayashi at al17. He found the presence of residual herniated tissues in the cyst wall. This is a very important finding in the pathogenesis of discal cyst. The rich vascular network in the posterior longitudinal ligament and posterior margin of the vertebral body is thought to play a major role in the spontaneous regression of disc herniation.
Disc herniation developed and during the process of absorption, fibrous tissue with vascuralization covered the migrated disc, with small vessels continuing into the herniated disc material. It appears that monocytes infiltrate the epidural tissue around the migrated herniation, which shows enhancement on MR images, via newly formed infiltrating blood vessels17. The monocytes change into macrophages, which break down, and digest the herniated tissue. The herniated tissue was absorbed by macrophages from the periphery, whereas, the infiltrated vessels connected to the epidural venous plexus.
In this study, electron microscopy suggested that macrophages played an important role in the absorption of herniated tissue and the formation of the discal cyst. Hemorrhage in the cyst wall will make the serous hemorrhagic fluid-filled cystic structure in the absorbed spaces of the prolapsed disc. Simultaneously, fibroblasts in the fibrous tissue covering the herniated disc might have a role in cyst formation, causing the discal cyst to develop18,19.
The histological analysis of the cystshowed the presence of hemorrhagic contents and hemosiderin deposits, which may be found in 30.4% of cases. In addition, myxoid degeneration and apoptotic chondrocytes20 was reported in 24% of cases3.
The clinical feature of discal cyst will depend upon its location and size. In most of the cases described the symptons are indistinguishable from the disc herniation patients. It usually presents as a unilateral radiculopathy accompanied by low back pain3-7. The pain can be severe, and as has happened in this case, with neurologic deficit in the compressed nerve root. One case has been reported presenting neurological intermittent claudication and bilateral radiculopathy signs, mimicking central spinal stenosis symptoms. This case, the discal cyst was occupying the entire spinal canal, and compressing thecal sac and the nerve roots bilaterally.
The MRI is the gold standard image exam to identify this type of lesions. It usually demonstrates spherical extradural masses with low intensities on T1 and high signal intensities on T2-weighted images. However, review of the radiologic findings of the discal cysts demonstrated that these signal intensities may not be the rule. According to a review of cases by Aydin et. al.3, in T1-weighted images, the cyst was hypointense in 68.7% of the cases, isointense in 29%, and hyperintense in 2%. On the other hand, in T2-weighted images, the cyst was hyperintense in 96% of the cases, isointense in 2%, and hypointense in 2%. Post-contrast MRI studies showed rim enhancement in 92% of the cases.
In most of the cases the discal cysts did not cross the midline of the spinal canal, due to the cruciform aspect of the posterior longitudinal ligament2-6. However, there is one case report in which the discal cyst was located in the center of the spinal canal8.
The discal cyst must be differentiated from a variety of other cystic lesions that may develop within the spinal canal, including perineural cyst extradural arachnoid cyst,and synovial cyst of the facet jointas well as extruded disc fragment in the epidural space. Perineural cysts may have the same signal characteristics as nonhemorrhagicdiscal cysts with a thin wall; however, they are multiple and in close relationship with the nerve root21. Extradural arachnoid cyst, showing a bilobed thin-walled cyst, occurs predominantly in younger persons and is located primarily in the thoracic spine usually in the dorsal aspect of the dural sac. Enhancement of an arachnoid cyst is not seen in contrast-enhanced MR images22. Synovial cyst of the facet joint, which frequently occurs, is dorsolateral to or inseparable from the facet joint. It can contain mucinous fluid or blood, has synovial lining cells in its wall23 and has no communication with the intervertebral disc. An extruded disc fragment in the epidural space can occur in the ventro-lateral epidural space just like a discal cyst. MRI shows a nonenhancing disc fragment with surrounding thick granulation tissue24.
Conservative treatment and analgesics administration usually showed slight pain relief. However, some case reports have shown improvement with this approach11. Koga et al.12, described the treatment with a percutaneous CT guided aspiration and steroid injection with improvement. This approach could be a less invasive option, although due to limited results of percutaneous aspiration by a small sample size and short-term follow-up period, careful analysis and follow up with additional cases are required for establishment of a proper therapeutic strategy8,12.
According to the cases reported, 62,5% treated with medical therapies and injections were referred to surgery. These findings show that these lesions are less controllable with conservative treatment modalities, and surgical treatment should be considered as initial management8.
Another promising form of discal cyst treatment is the neural decompression using an endoscopic percutaneous approach. Besides the disadvantage of the steep learning curve, it has been described as a promising option, with complications rates similar to microscopic decompression. During 4 years, 8 cases have been treated using this technique. Recurrence cases have not been reported, and 87,5% of the patients had satisfactory results13. The authors suggest that being outside the disc space and avoiding the disc was the reason of no recurrence3,13. We agree that the disc space should be avoided, to decrease the disc degeneration process. In the case presented only the resection of the discal cyst was performed.
Most of the cases reported have been treated using microscopic decompression and excision of the discal cyst3-8. This technique has been modified to a less invasive technique, due to the improvement of the retractors and better visualisation of the anatomical structures. This approach has the advantages of being more precise to confirm the neural decompression during the procedure, which is most important in cases where an intense sign of neurologic deficit exists. This approach also enables us to find the lesion regardless of its location, and size. Due to thesefeatures this technique was chosen to deal with this patient.
There are certain locations in the spinal canal that can be difficult to identify the discal cyst. Lee et al.9, reported a case that after micro decompression, the patient still presented the previous symptoms. A postoperative MRI showed that the lesion was not removed. The patient was submitted to a new intervention, during which an intraoperative discography was performed. Using fluoroscope the proper location of the lesion was identified and could be removed, reliving the patient's symptoms.
Takeshima et al.25 report one man's case , 39-year-old man presented with an extremely rare discal cyst at the L3-4 level manifesting as a left L4 radiculopathy and his treatment was conservative therapy. After five months of conservative therapy the lesion was improvide. Other research describe a case, 35-year-old man with radiculopathy who presented with a discal cyst and was treated with a routine epidural injection and selective nerve root block26. However, Kim et al.27 studied a 27-old-man presented with left gluteal and leg pain due to a discal cyst at the L5-S1, in this case a percutaneous endoscopic interlaminar was approach appears successful.
In summary, the discal cysts are rare intraspinal lesions. They can trigger severe neurological symptoms, and should be differentiated from other forms of epidural cysts and tumors. There are many treatment options that can be chosen from. One must identify the intensity of the neural compression and use the technique with less morbidity and safer that is most famyliarwith. In this case a microendoscopic technique was performed, avoiding the disc space and confirming the decompression of the neural structures. The patient achieved an excellent result, being able to return to his activities, and showing no signs of recurrence one year after the procedure.
ACNOWLEDGEMENTS
FDA device/drug status: not applicable.
Nothing of value received from a commercial entity related to this research.
REFERFENCES
1. Caetano VC, Ribeiro LC, Cruz DT, Asmus CIRF. Desordens músculo-esqueléticas em adolescentes trabalhadores. Rev Bras Crescimento Desenvolv Hum. 2008;18(3):264-74. DOI: http://dx.doi.org/10.7322/jhgd.19889 [ Links ]
2. Kono K, Nakamura H, Inoue Y, Okamura T, Shakudo M, Yamada R. Intraspinal extradural cysts communicating with adjacent herniated disks: imaging characteristics and possible pathogenesis. Am J Neuroradiol. 1999; 20(7): 1373-7. [ Links ]
3. Aydin S, Abuzayed B, Yildirim H, Bozkus H, Vural H. Discal cysts of the lumbar spine: report of fi ve cases and review of the literature. Eur Spine J. 2010;19(10):1621-6. DOI: http://dx.doi.org/10.1007/s00586-010-1395-9 [ Links ]
4. Chiba K, Toyama Y, Matsumoto M, Maruiwa H, Watanabe M, Nishizawa T. Intraspinal cyst communicating with the intervertebral disc in the lumbar spine: discal cyst. Spine (Phila Pa 1976). 2001;26(19):2112-8. [ Links ]
5. Murata K, Ikenaga M, Tanaka C, Kanoe H, Okuaaira S. Discal cysts of the lumbar spine: a case report. J Orthop Surg (Hong Kong). 2007;15(3):376-9. [ Links ]
6. Hwang JH, Park IS, Kang DH, Jung JM. Discal cyst of the lumbar spine. J Korean Neurosurg Soc. 2008;44(4):262-4. DOI: http://dx.doi.org/10.3340/jkns.2008.44.4.262 [ Links ]
7. Jeong GK, Bendo JA. Lumbar intervertebral disc cyst as a cause of radiculopathy. Spine J. 2003;3(3): 242-6. [ Links ]
8. Hyung-Jun K, Dae-Yong K, Tae-Ho K, Ho-Sang P, Jae-Sung K, Jae-Won J, et al. Lumbar discal cyst causing bilateral radiculopathy. Surg Neurol Int. 2011;2:21. DOI: http://dx.doi.org/10.4103/2152-7806.77026 [ Links ]
9. Lee HK, Lee DH, Choi CG, Kim SJ, Suh DC, Kahng SK et al. Discal cyst of the lumbar spine: MR imaging features. Clin Imaging. 2006;30(5):326-30. DOI: http://dx.doi.org/10.1016/j.clinimag.2006.05.026 [ Links ]
10. Kwon YK, Choi KC, Lee CD, Lee SH. Intraoperative discography for detecting concealed lumbar discal cysts. J Korean Neurosurg Soc. 2013;53(4):255-7. DOI: http://dx.doi.org/10.3340/jkns.2013.53.4.255 [ Links ]
11. Prasad G, Kabir SM, Saifuddin A, Casey AT. Spontaneous resolution of discal cyst around L5 nerve root: case report and review of literature. Br J Neurosurg. 2011;25(6):761-3. DOI: http://dx.doi.org/10.3109/02688697.2011.555020 [ Links ]
12. Koga H, Yone K, Yamamoto T, Komiya S. Percutaneous CT-guided puncture and steroid injection for the treatment of lumbar discal cyst: a case report. Spine (Phila Pa 1976). 2003;28(11):E212-6. DOI: http://dx.doi.org/10.1097/01.BRS.0000067279.53431.6A [ Links ]
13. Ha SW, Ju CL, Kim SW, Lee S, Kim YH, Kim HS. Clinical outcomes of percutaneous endoscopic surgery for lumbar discal cyst. J Korean Neurosurg Soc. 2012;51(4):208-14. DOI: http://dx.doi.org/10.3340/jkns.2012.51.4.208 [ Links ]
14. Lin N, Schirmer CM, Proctor MR. Presentation and progression of a disc cyst in a pediatric patient. J Neurosurg Pediatr. 2011;7(2):209-12. DOI: http://dx.doi.org/10.3171/2010.11.PEDS10227 [ Links ]
15. Marushima A, Uemura K, Sato N, Maruno T, Matsumura A. Osteolytic lumbar discal cyst: case report. Neurol Med Chir (Tokyo). 2008;48(8):363-6. [ Links ]
16. Jha SC, Tonogai I, Higashino K, Sakai T, Takata Y, Goda Y, et al. Postoperative discal cyst: An unusual complication after microendoscopic discectomy in teenagers. Asian J Endosc Surg. 2016;9(1):89-92. DOI: http://dx.doi.org/10.1111/ases.12227 [ Links ]
17. Kobayashi S, Meir A, Kokubo Y, Uchida K, Takeno K, Miyazaki T, et al. Ultrastructural analysis on lumbar discherniation using surgical specimens: Role of neovascularization and macrophages in hernias. Spine (Phila Pa 1976). 2009;34(7):655-62. http://dx.doi.org/10.1097/BRS.0b013e31819c9d5b [ Links ]
18. Kobayashi S, Takeno K, Uchida K, Yayama T, Nakajima H, Miyazaki T, et al. Pathogenesis of the discal cysts communicating with an adjacent herniated disc. Histological and ultrastructual studies of two cases. Joint Bone Spine. 2010;77(2):184-6. DOI: http://dx.doi.org/10.1016/j.jbspin.2009.09.009 [ Links ]
19. Santos FGPL, SouzaI RA, BrottoI MPA, SuguitaI FM, Denise Tokechi Amaral DT, Amaral LLF. Epidural cystic masses associated with interspinous bursitis, synovial and discal cysts. Radiol Bras. 2009;42(2):1373-7. DOI: http://dx.doi.org/10.1590/S0100-39842009000200013 [ Links ]
20. Okada K, Saito H, Nishida J, Miyakoshi N, Takahashi S, Nagasawa H, et al. Discal cyst associated with myxoid change and apoptosis of herniated disc materials: a case report. Ups J Med Sci. 2007;112(1):39-47. [ Links ]
21. Tarlov IM. Perineural cysts of the spinal nerve roots. Arch Neural Psychiatry. 1938;40(6):1067-74. DOI: http://dx.doi.org/10.1001/archneurpsyc.1938.02270120017001 [ Links ]
22. Rohrer DC, Burchiel KJ, Gruber DP. Intraspinal extradural meningeal cyst demonstrating ball-valve mechanism of formation. Case report. J Neurosurg. 1993;78(1):122-5. DOI: http://dx.doi.org/10.3171/jns.1993.78.1.0122 [ Links ]
23. Jackson DE Jr, Atlas SW, Mani JR, Norman D. Intraspinal synovial cysts: MR imaging. Radiology. 1989;170(2):527-30. DOI: http://dx.doi.org/10.1148/radiology.170.2.2911681 [ Links ]
24. Ross JS, Masaryk TJ, Schrader M, Gentili A, Bohlman H, Modic MT. MR imaging of the postoperative lumbar spine: assessment with gadopentetate dimeglumine. AJNR Am J Neuroradiol. 1990;11(4):771-6. [ Links ]
25. Takeshima Y, Takahashi T, Hanakita J, Watanabe M, Kitahama Y, Kuraishi K, et al. Lumbar discal cyst with spontaneous regression and subsequent occurrence of lumbar disc herniation. Neurol Med Chir (Tokyo). 2011;51(11):809-11. [ Links ]
26. Chou D, Smith JS, Chin CT. Spontaneous regression of a discal cyst. Case report. J Neurosurg Spine. 2007;6(1):81-4. DOI: http://dx.doi.org/10.3171/spi.2007.6.1.81 [ Links ]
27. Kim JS, Choi G, Jin SR, Lee SH. Removal of a discal cyst using a percutaneous endoscopic interlaminar approach: a case report. Photomed Laser Surg. 2009;27(2):365-9. [ Links ]
Manuscript submitted: Feb 2 2016
Accepted for publication Feb 29 2016
Corresponding author: E-mail: anm.machado@gmail.com


{kind=link}
{kind=link}
{kind=link}
{kind=link}