










Serviços Personalizados
Journal

artigo
 Inglês (pdf)
Inglês (pdf)
 Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
Indicadores
Compartilhar

 Permalink
PermalinkJournal of Human Growth and Development
versão impressa ISSN 0104-1282versão On-line ISSN 2175-3598
J. Hum. Growth Dev. vol.29 no.2 São Paulo maio/ago. 2019
https://doi.org/10.7322/jhgd.v29.9427
ORIGINAL ARTICLE
Cardiac autonomic modulation during different modes of weaning of mechanical ventilation
Marcelle GuerraI; Juliana Zangirolami-RaimundoI; George Jerre Vieira SarmentoIII; Renata SalatiniIV; Pammela de Jesus SilvaV; Rodrigo Daminello RaimundoI
ILaboratório de Delineamento de Estudos e Escrita Científica do Centro Universitário Saúde ABC, Santo André, SP, Brazil
IIFaculdade de Medicina da Universidade de São Paulo, São Paulo, SP, Brazil
IIICoordenador do Serviço de Fisioterapia do Hospital São Luiz/Rede D'or - Unidade Jabaquara, SP, Brazil
IVClínica Cirúrgica, Faculdade de Medicina da USP, São Paulo, SP, Brazil
VUniversidade de São Caetano, São Caetano do Sul, SP, Brazil
ABSTRACT
INTRODUCTION: Heart rate variability (HRV) is a noninvasive method to analyze variations of time intervals between heart beats. HRV is a promising method to analyze autonomic balance quantitatively. During the weaning process of mechanical ventilation, alterations occur in the autonomic activity. Methods to identify increased risk for weaning failure are needed.
OBJECTIVE: To analyze the behavior of cardiac autonomic modulation in different phases of weaning mechanical ventilation.
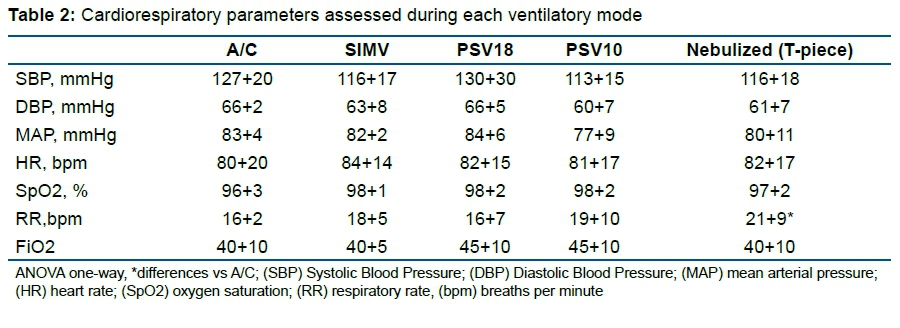
METHODS: Cardiorespiratory parameters (SBP, DBP, MAP, RR, SpO2) of 18 participants were collected and a cardio-frequency meter was placed. The subjects were kept in supine Fowler's position t, ventilating for 10 minutes in the assist-controlled (A/C) ventilation mode the synchronized intermittent mandatory ventilation (SIMV) mode, pressure support ventilation (PSV) 18 and 10, and with nebulization through a T-piece. At the end of all ventilator modes, the pre-specified variables were measured. The HRV parameters were analyzed in the domains of time, frequency and geometric indexes.
RESULTS: There was an increase in the mean rMSSD of the A/C moment of 20.67 ± 19.36ms for the PSV 10 time 29.96 ± 21.26ms (p = 0.027), increase between the SIMV moments of 24.04 ± 18.31ms and PSV 10 to 29.96 ± 21.26ms (p = 0.042), but reduced between PSV 10 and T-Tube moments 21.22 ± 13.84ms (p = 0.035). There was an increase in the LF mean of the SIMV moments 158.46 ± 229.77ms2 and PSV 10 265.50 ± 359.88ms2 for T-tube 408.92 ± 392.77ms2 (p = 0.011 and p = 0.037 respectively). The mean LF showed a decrease between C/A and SIMV moments, respectively, 62.48 ± 17.99nu and 54.29 ± 15.29nu (p = 0.024), increase in SIMV moments 54.29 ± 15.29nu and PSV 10 55.05 ± 23.07nu for TUBE T 65.57 ± 17.08nu (p = 0.049 and p = 0.027 respectively). HF increased between SIMV moments 162.89 ± 231.19ms2 and PSV 10 247.83 ± 288.99ms2 (p = 0.020) and also between SIMV and T-Tube moments 248.28 ± 214.46 ms2 (p = 0.044). There was a reduction in mean HF between PSV 10 times 44.71 ± 22.95nu and T-tube 34.22 ± 17.03nu (p = 0.026
CONCLUSIONS: The present study showed that in comparison with spontaneous breathing, controlled breathing was associated with lower HRV during weaning from mechanical ventilation.
Keywords: autonomic nervous system, heart rate of weaning, ventilatory weaning.
Authors summary
Why was this study done?
- About 50% of intensive care patients require ventilatory support.
- Prolonged time in invasive MV imposes deleterious effects, not only on the respiratory system, but also on other organs of the human body.
- It is estimated that 40% of the total ventilation time is used during the weaning process.
- Markers of Heart Rate Variability (HRV) that may indicate early weaning failure may help in choosing the best strategy, thus minimizing the risks inherent to failure of this process.
What did the researchers do and find?
- Cardiorespiratory parameters of 18 participants were collected and a cardio-frequency meter was placed. The subjects were kept in supine Fowler's position, ventilating for 10 minutes in the assist-controlled (A/C) ventilation mode the synchronized intermittent mandatory ventilation (SIMV) mode, pressure support ventilation (PSV) 18 and 10, and with nebulization through a T-piece.
- At the end of all ventilator modes, the pre-specified variables were measured. The HRV parameters were analyzed in the domains of time, frequency and geometric indexes.
- There was an increase in the mean rMSSD of the A/C moment for the PSV 10, increase between the SIMV moments and PSV 10, but reduced between PSV 10 and T-Tube moments. There was an increase in the LF mean of the SIMV moments and PSV 10 for T-tube. The mean LF showed a decrease between C/A and SIMV moments, respectively, increase in SIMV moments and PSV 10 for TUBE T. HF increased between SIMV moments and PSV 10 and also between SIMV and T-Tube moments. There was a reduction in mean HF between PSV 10 and T-tube.
What do these findings mean?
- In comparison with spontaneous breathing, controlled breathing was associated with lower HRV during weaning from mechanical ventilation.
INTRODUCTION
Invasive mechanical ventilation (MV) is a therapeutic resource used within intensive care units in patients with respiratory failure of varying origin. About 50% of intensive care patients require ventilatory support. However, the time individuals remain in this modality should be minimized1.
Prolonged time in invasive MV imposes deleterious effects, not only on the respiratory system, but also on other organs of the human body. Therefore, withdrawal of MV should be considered as soon as the patient is able to breathe spontaneously2.
Ventilatory weaning represents the transition period from mechanical to spontaneous ventilation. Respiratory work is transferred back from the ventilator to the patient, and this process is considered as a challenging medical problem in clinical practice2. It is estimated that 40% of the total ventilation time is used during the weaning process3. It is important to emphasize that delay or even premature weaning can influence the outcome of the patient: prolonged ventilation, length of stay in intensive care, increased costs, need for longer rehabilitation, and a higher mortality rate2,4.
Ventilator weaning is also associated with changes in autonomic nervous system (ANS) activity. Changes in heart rate variability are expected5-7. The transition from invasive MV to spontaneous breathing is characterized by changes in intrathoracic pressure, which results in increased systolic blood pressure (BP) and heart rate, suggesting an exacerbation of sympathetic activity.
When ventilation is discontinued, more than 25% of patients present respiratory failure requiring return to invasive MV1. Therefore, the use of tools that can assist the professionals involved in predicting success or failure from weaning is extremely valuable.
In this sense, the analysis of heart rate variability (HRV) has been used as a non-invasive tool that reflects the autonomic modulation of the cardiovascular system. The analysis is based on the study of temporal oscillations between heart beats1,2.
It is known that respiratory activity affects cardiovascular regulation. Changes in intrathoracic pressure and pulmonary volumes during MV may induce changes in hemodynamic markers such as preload and afterload of the right and left ventricles and of intrathoracic volume and blood flow. In response, the (ANS) is activated, and this induces changes in ventricular afterload, contractility and heart rate to maintain cardiac output and tissue perfusion. The balance between the two components of autonomic tonus - sympathetic and parasympathetic innervation - can be evaluated by measuring HRV8.
Autonomic dysfunction increases sympathetic activity and reduces parasympathetic activity, which is related to the pathophysiology of some diseases, arrhythmias and increased mortality9.
Several studies2,3,8-14 have evaluated parameters related to cardiovascular interaction and their influence on the weaning process.
Sasaki & Maruyama14 described the behavior of HRV in controlled versus spontaneous breathing. The findings showed that compared to spontaneous breathing, despite similar respiratory rates (RR), controlled respiration was associated with a higher heart rate and a lower high-frequency component (HF), a rate of parasympathetic nerve activity. During controlled breathing, the ratio of low frequency (LF) to HF components (LF/HF), an index of sympathetic nerve activity, increased greatly, while HF decreased and heart rate and BP remained largely unchanged. Thus, controlled breathing, which requires mental concentration, may inhibit parasympathetic nerve activity. During controlled breathing, LF/HF increases because some HF subcomponents are synchronized with respiratory rate and probably move to the LF band15.
The fall in HRV indices has been associated with high mortality in critically ill patients. Shen et al. reported the impact of weaning from MV on HRV. The authors observed a reduction in HRV modulation in patients who failed to transition from the assisted to support or T-piece modality. Also, HRV proved to be a good diagnostic and prognostic predictor in critical illness12.
In this context, markers that may indicate early weaning failure may help in choosing the best strategy, thus minimizing the risks inherent to failure of this process.
With this, the objective of this work was to analyze the behavior of cardiac autonomic modulation in different phases of weaning from mechanical ventilation.
METHODS
Ethical Aspects of Research
The research project was submitted to the Research Ethics Committee of the ABC Medical School and approved (CAAE 27249314.6.0000.0082), opinion number: 638.109 and was applied only after the approval of the Committee and signing the Term of Free and Informed Consent (TCLE) by the legal representative of each research subject.
Type, location and population of the study
A cross-sectional study was carried out in the period from March 2015 to November 2015, in which 18 patients hospitalized at the intensive care unit (ICU) of the Hospital São Luiz - Unidade Jabaquara (HSL) were evaluated during the phase of ventilatory weaning.
Inclusion and exclusion criteria
All patients, both men and women, who were transitioning from mechanical ventilation to spontaneous ventilation in the HSL ICU for tracheal intubation for a further 24 hours or with ventilatory assistance under tracheostomy were considered eligible and authorized to participate in the study by confirming and signing the TCLE by their legal representative.
We excluded patients who did not meet the clinical and physiological criteria for ventilatory weaning, that is, no improvement of the condition caused by the acute event that motivated mechanical ventilation specified as: Partial pressure of oxygen (PaO2) less than 60 mmHg with inspired fraction of oxygen (FiO2) greater than or equal to 0.4 with positive end-expiratory pressure (PEEP) between 5 and 8 cmH20; Low tissue perfusion with vasopressor drug dependence; Patient not able to initiate the respiratory efforts spontaneously (respiratory drive) or no effective cough; Patient could not be awaken to sound stimuli; Maintained pH <7.30; Abnormal values of serum sodium, potassium, calcium or magnesium.
Instruments of data collection
A completed data collection sheet was used at the bedside and from the patient's medical records.
Measurements included SBP and diastolic blood pressure (DBP), mean arterial pressure (MAP), heart rate (HR), respiratory frequency (RF) and peripheral oxygen saturation (SpO2) for monitoring ventilation modes. SpO2 data were collected by viewing the Dixtal® brand DX 2010 multi-parameter monitor and SBP, DBP and MAP data were obtained by a single measurement provided by the same monitor. HR was recorded by the Polar® brand S810i cardio-frequency meter. All patients were ventilated on the Puritan BennettTM 840 device of the Covidien-Medtronic brand.
After filling in the baseline data, the collection belt was placed on the patient's thorax and with the HR receptor (S810i, Polar), previously validated equipment for HR collection, HRV data sampling and analysis was initiated.
The subjects were then placed in the supine Fowler's position (semi-seated at 45 degrees) and remained at rest, ventilating for 10 minutes in the assist-control (A/C) ventilation mode. After 10 minutes the SBP, DBP, MAP, SpO2, and RR (respiratory rate) data were collected. These variables were also collected after all of the maneuvers described next.
Next there was a change to the synchronized intermittent-voluntary (SIMV) mode with a mandatory frequency of 12 to 15 repetitions per minute, PEEP 5cm H2O, remaining for another 10 minutes. .
After the SIMV mode, the patient was placed in pressure-support ventilation (PSV) 18, PEEP 5cm H2O mode for another 10 minutes.
When the patient tolerated, another change was made for PSV 10, PEEP 5 cm H20 for 10 minutes.
To end the protocol, the patient was nebulized through the T-tube for 10 minutes, again with data collection as previously listed.
The data collection was performed from 7:00 am to 9:00 pm, and HRV data collection lasted for minutes in each patient, totaling the attendance-controlled moment, SIMV, PSV 18, PSV 10 and T-tube.
Analysis of Heart Rate Variability
The software Kubios HRV® was used to obtain consecutive RR intervals and subsequent HRV analysis. Only the series with more than 95% of sinus beats were included in the study. For this, a digital filtering, followed by manual, was performed to eliminate premature ectopic beats and artifacts.
The HRV analysis was performed using linear methods, analyzed in the time and frequency domains and through geometric indices16.
In the time domain, the indexes rMSSD, pNN50, and SDNN were used.
The analysis of vagal reentry was performed using the RMSSD, calculated using Kubios HRV analysis software - version 2.0. For this, HR behavior was recorded beat-to-beat throughout the protocol, and before using the R-R series captured for data analysis.
The RMSSD index corresponds to the square root of the sum of the square of the differences between the RR intervals in the record, divided by the number of R-R intervals in a given time minus one R-R interval. For this analysis, we considered the 10 minutes of the period of each ventilatory mode. The pNN50 index is defined as the percentage of successive differences in the R-R interval, whose absolute value exceeds 50 ms and is a sensitive and easily interpretable marker of the activity of the parasympathetic autonomic nervous system. The SDNN represents the standard deviation of the mean of all normal R-R intervals, expressed in ms and reflects the participation of both branches of the ANS17-19.
In order to analyze HRV in the frequency domain, the LF spectral components were used, which is due to the joint action of the vagal and sympathetic components on the heart, with sympathetic predominance. HF corresponds to respiratory modulation and is an indicator of the vagus nerve activity on the heart in normalized units, and the ratio between these components (LF/HF), which reflects the absolute and relative alterations between the sympathetic and parasympathetic components of the ANS, characterizing the sympathovagal balance on the heart20.
For the analysis of the HRV using non-linear methods, the Poincaré chart (components SD1, SD2 and SD1/SD2 ratio)21.
The Poincaré plot allows each R-R interval to be plotted against the previous interval. For the quantitative analysis of the plot, the following indices were calculated: SD1 (instantaneous variability of beat-to-beat variability), SD2 (long-term standard deviation of continuous R-R intervals) and SD1/SD2 ratio22,23
Statistical Analysis
The results were expressed as mean ± standard deviation. The Excel 2013 programs were used for the elaboration of the database and the statistical analyzes were performed by the SPSS software version 13.0 and the Kolmogorov-Smirnov test was applied to verify if there were a normal distribution of the variables and the Levine test to verify the homogeneity of the variances. One-way ANOVA (analysis of variance) was used for all variables. A significance level of 0.05 (5%) was defined for this study, with 95% confidence intervals.
RESULTS
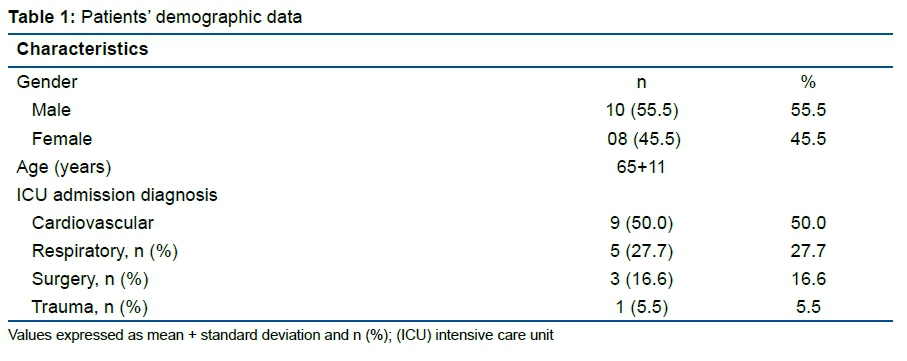
Table 1 presents the demographic data of the study population. Of the 18 patients 10 were male and 8 were female. The age ranged from 54 to 76 years. The studied population was heterogeneous with respect to admission diagnoses in the ICU (Table 1, Table 2 and Table 3).
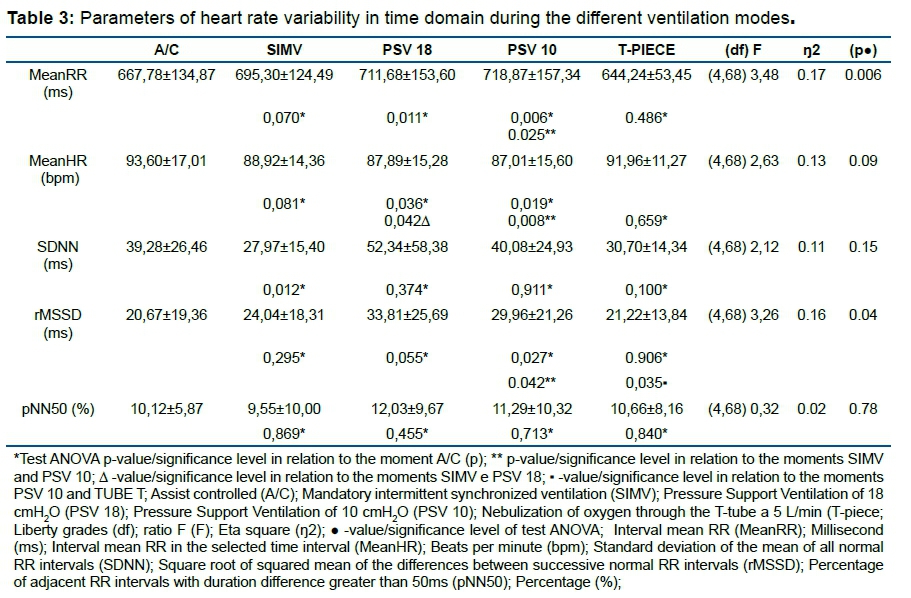
According to the results shown in Table 3, there was an increase in mean R-R interval (MeanRR) at A/C ventilation (667,78±134,87ms) for the moments PSV 18 and PSV 10 (711,68±153,60ms e 718,87±157,34ms, respectively) and increase between the moments SIMV (695,30±124,49ms) and PSV 10 (718,87±157,34ms).
The MeanHR presented decrease from the moment A/C (93,60±17,01bpm) to the moments PSV 18 and PSV 10 (87,89±15,28bpm and 87,01±15,60bpm), decrease between SIMV (88,92±14,36bpm) and PSV 18 and decrease between SIMV and PSV 10. Mean SDNN decreased between the moments A/C (39,28±26,46ms) and SIMV 27,97±15,40ms. There was an increase in the mean rMSSD from the moment A/C of 20,67±19,36ms to the moment PSV 10 29,96±21,26ms, increase between the moments SIMV of 24,04±18,31ms and PSV 10 to 29,96±21,26ms, but reduced between the moments PSV 10 and T-piece 21,22±13,84ms (Table 4).
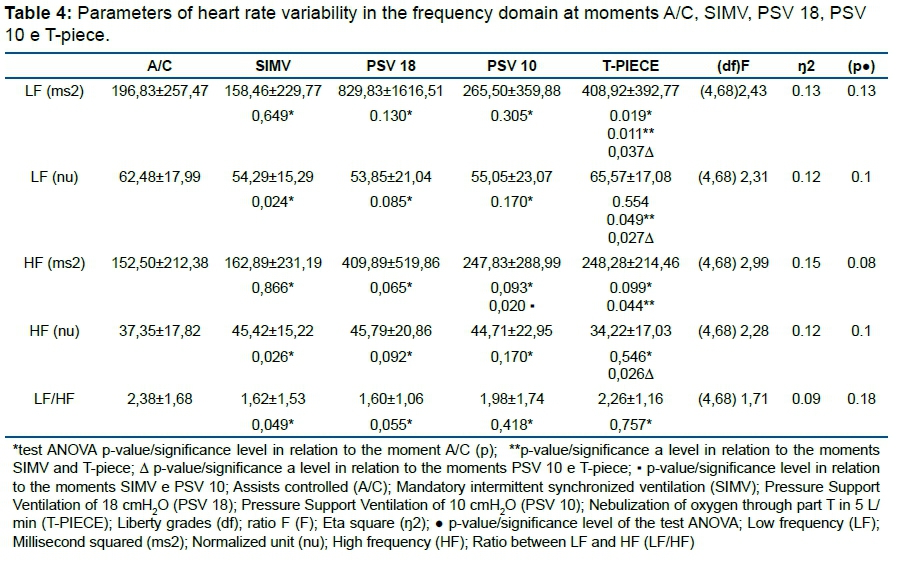
According to the data presented in Table 4, there was an increase in the mean of LF of the moments SIMV 158,46±229,77ms2 and PSV 10 265,50±359,88ms2 to T-piece 408,92±392,77ms2, respectively. The mean for LF presented decrease between the moments A/C and SIMV respectively 62,48±17,99nu and 54,29±15,29nu, increase of the moments SIMV 54,29±15,29nu and PSV 10 55,05±23,07nu to T-piece 65,57±17,08nu respectively. HF increased between the moments SIMV 162,89±231,19ms2 and PSV 10 247,83±288,99ms2 and also between the moments SIMV and T-piece 248,28±214,46ms2. There was a decrease in the mean HF between the moments PSV 10 44,71±22,95nu and T-piece 34,22±17,03nu. The mean of the ratio LF/HF decreased between A/C 2,38±1,68 and SIMV 1,62±1,53 (Table 5).
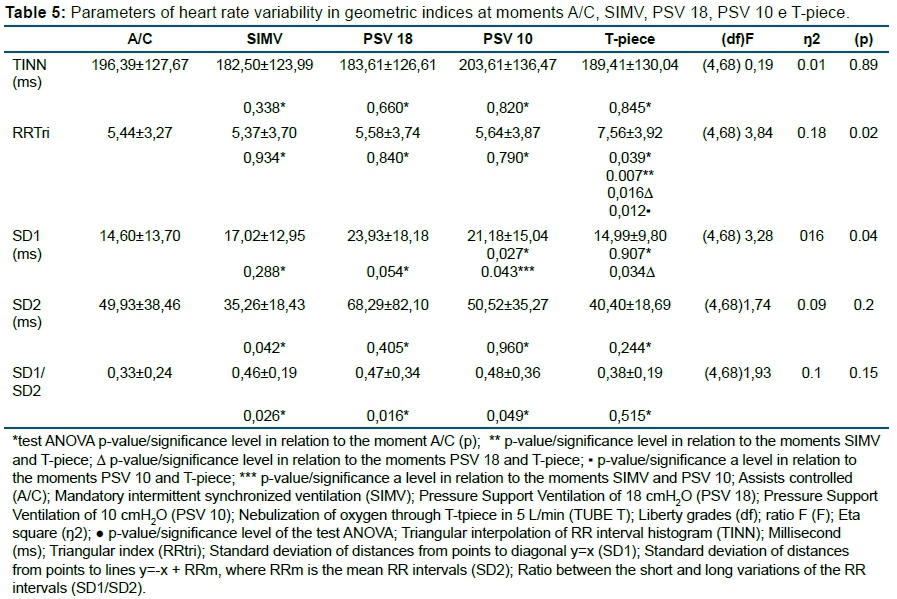
According to the data presented in Table 5, there was an increase of the mean of RRTri of the moments A/C 5,44±3,27, SIMV 5,37±3,70, The mean of SD1 presented increase between the moments SIMV 17,02±12,95ms and PSV 10 21,18±15,04ms and decrease between the moments PSV 18 and T-piece respectively 23,93±18,18ms and 14,99±9,80ms. SD2 showed decrease in the moment A/C 49,93±38,46ms to the moment SIMV 35,26±18,43ms. The mean SD1/SD2 increased from the moment A/C 0,33±0,24 to the moments SIMV 0,46±0,19 and PSV 18 0,47±0,34 and PSV 10 0,48±0,36.
DISCUSSION
The current literature contains several studies24-30 on HRV in different clinical scenarios and environments. However, within the hospital environment, and specifically during the weaning process of mechanical ventilation, the findings are still not well understood.
Weaning from mechanical ventilation for spontaneous breathing is associated with changes in the hemodynamics and in the modulation of the ANS that are reflected in HRV. Cardiac arrhythmias are an important manifestation of hemodynamic changes, but study data on the impact of weaning on HRV is limited30.
This study analyzed the behavior of HRV in different phases of ventilatory weaning to better understand the behavior of the ANS in this process, which could help in assessing clinically important predictive indexes in future research.
In the present study, the LF component (ms2 and nu) increased in the different ventilatory types in relation to the spontaneous respiration through the T-piece (A/C to T-piece; SIMV to T-piece; PSV 10 to T-piece), indicating increased sympathetic modulation.
Tobin et al.11 and Shen et al.10 demonstrated that patients who failed in the weaning process of MV presented higher respiratory rate (RR) and lower tidal volume (TV) during respiration with the T-piece. They observed that weaning failure usually occurs in parallel with a decrease in TV and increased RR due to increased respiratory work; this seems to be the justification for the increase in LF.
Studies have suggested that patients who fail to wean with the T-piece present a greater overload of the inspiratory and expiratory muscles, requiring a greater force to maintain ventilation12.
We also observed an increase of the parasympathetic modulation during the transition from more controlled ventilatory modes (A/C and SIMV) to the spontaneous mode PSV 10 and also during spontaneous breathing through the T-piece.
The study of Shen et al.10 analyzed HRV changes during weaning and found results that showed a decrease in HF in the group that failed in the weaning process. They suggest two reasons for this decrease. The first was that intense sympathoadrenal stimulation during weaning may result in the withdrawal of the activity of the parasympathetic nervous system. The second is that the HF component of the HRV decreases with the increase of the RF and decrease of the CV11. The results differ from the findings in our study, which demonstrated a greater parasympathetic modulation, predicting higher HRV at these stages of weaning.
During the transition from PSV to the T-piece, the HRV components reduced significantly in the group of patients who failed to wean, but not in the success group30.
Although the objective of our study was not to evaluate the success or failure of weaning, we also observed a significant reduction of HF (nu), RMSSD and SD1 components during the transition from PSV 10 to the T-piece.
On the other hand, the components HF, RMSSD, and SD1 increased when there was a transition of the types A/C - SIMV, SIMV - PSV10, SIMV - T-piece (HF); A/C - PSV 10, SIMV -PSV 10 (RMSSD) and A/C - PSV 10, SIMV - PSV 10 (SD1); indicating that these transitions presented greater parasympathetic modulation in the present study.
Our findings corroborate with those of Hammash et al.8 According to the authors, this transition induces changes in hemodynamic markers such as intrathoracic vascular volume, preload and afterload. The ANS responds with increased sympathetic activity, reduction of the parasympathetic activity or a combination of both to maintain adequate cardiac output and tissue oxygenation.
Regarding the global parameters, our findings showed a decrease in the SDNN, LF/HF and SD2 in the transition A/C - SIMV.
Frazier et al.12 analyzed the autonomic tonus in intensive care patients under mechanical ventilation and during weaning through continuous positive airway pressure (CPAP). In agreement with our study, the findings also evidenced a reduction of the HRV identified in the components of the time domain and geometric indices. The decrease in overall HRV was greater in those patients unable to breathe spontaneously during CPAP.
There is evidence that the high positive pressure of mechanical ventilation generates a complex neurohormonal response by altered intrathoracic pressure and changes in cardiopulmonary interaction. Reductions in natriuretic peptide secretion, increased arginine-vasopressin and a significant renin release with consequent elevation in angiotensin 2 and aldosterone lead to increased intravascular and interstitial volume and a hypervolemic state. These changes in neurohormonal homeostasis may contribute to a decrease in overall HRV12.
The reduction of SDNN in the study of Frazier et al.12 was associated with the group of patients who did not have success in weaning.
On the other hand, was observed that the RRTri increased in the transitions of A/C -TUBE T, SIMV - TUBE T, PSV 18 - TUBE T and PSV 10 - TUBE T. There was an increase of the SD1/SD2 and in the transitions A/C - SIMV, A/C - PSV and A/C - PSV 10.
Our findings are in agreement with Huang et al.13 who, in their study with a sample of critically heterogeneous patients, showed different responses during weaning. Thus, changes in some components of HRV are still unknown.
Vitacca et al.29 found that measures of changes in HRV during the weaning process may help clinicians to predict outcomes and, at the end of the analysis, improve outcome and the patients.
The spectral analysis of HRV components, performed at 10-minute intervals during the weaning process, may not have been sufficient to provide additional information.
For the assessment of the prognostic value of changes of HRV indices during ventilator weaning, larger patient populations need to be studied in the future.
CONCLUSION
The present study showed that in comparison with spontaneous breathing, controlled breathing was associated with lower HRV during weaning from mechanical ventilation.
Acknowledgment
This work would not be possible without permission to collect data in the Intensive Care Units of Hospital São Luiz - Jabaquara Unit. We thank the patients' legal guardians for accepting to participate in the study and the professors Luiz Carlos de Abreu and Andrés Ricardo Perez-Riera.
REFERENCES
1.Chiappa AMG, Chiappa GR, Cipriano G Jr, Moraes RS, Ferlin EL, Borghi-Silva A, et al. Spontaneous breathing trial in T-tube negatively impact on autonomic modulation of heart rate compared with pressure support in critically ill patients. Clin Respir J. 2017;11(4):489-495. DOI: http://doi.org/10.1111/crj.12363 [ Links ]
2.Arcentales A, Caminal P, Diaz I, Benito S, Giraldo BF. Classification of patients undergoing weaning from mechanical ventilation using the coherence between heart rate variability and respiratory flow signal. Physiol Meas. 2015;36(7):1439-52. DOI: http://doi.org/10.1088/0967-3334/36/7/1439 [ Links ]
3.Goldwasser R, Farias A, Freitas EE, Saddy F, Amado V, Okamoto V. Desmame e interrupção da ventilação mecânica. J Bras Pneumol. 2007;33(Suppl 2):128-36. DOI: http://dx.doi.org/10.1590/S1806-37132007000800008 [ Links ]
4.Seely AJ, Bravi A, Herry C, Green G, Longtin A, Ramsay T, et al. Do heart and respiratory rate variability improve prediction of extubation outcomes in critically ill patientes? Critical Care. 2014;18(12):R65. DOI: http://doi.org/10.1186/cc13822 [ Links ]
5.Sin DD, Wong E, Mayers I, Lien DC, Feeny D, Cheung H, et al. Effects of nocturnal noninvasive mechanical ventilation on heart rate variability of patients with advanced COPD. Chest. 2007;131(1):156-63. DOI: http://doi.org/10.1378/chest.06-1423 [ Links ]
6.Srivastava S, Chatila W, Amoateng-Adjepong Y, Kanagasegar S, Jacob B, Zarich S, et al. Myocardial ischemia and weaning failure in patients with coronary artery disease: an update. Crit Care Med. 1999;27(10):2109-12. DOI: http://doi.org/10.1097/00003246-199910000-00005 [ Links ]
7.Valipour A, Schneider F, Köessler W, Saliba S, Burghuber OC. Heart rate variability and spontaneous baroreflex sequences in supine healthy volunteers subjected to nasal positive airway pressure. J Appl Physiol. 2005;99(6):2137-43. DOI: http://doi.org/10.1152/japplphysiol.00003.2005 [ Links ]
8.Hammash MH, Moser DK, Frazier SK, Lennie TA, Hardin-Pierce M. Heart Rate Variability as a predictor of cardiac dysrythmias during weaning from mechanical ventilation. Am J Crit Care. 2015;24(2):118-27. DOI: http://doi.org/10.4037/ajcc2015318 [ Links ]
9.Reis MS, Sampaio LM, Lacerda D, Oliveira LV, Pereira GB, Pantoni CB, et al. Acute effects of different levels of continuous positive airway pressure on cardiac autonomic modulation in chronic heart failure and chronic obstructive pulmonary disease. Arch Med Sci. 2010;6(5):719-27. DOI: http://doi.org/10.5114/aoms.2010.17087 [ Links ]
10.Shen HN, Lin LY, Chen KY, Kuo PH, Yu CJ, Wu HD, et al. Changes of heart rate variability during ventilator weaning. Chest. 2003;123(4):1222-8. DOI: http://doi.org/10.1378/chest.123.4.1222 [ Links ]
11.Tobin DD, Menon M, Menon M, Spatta BC, Hodges EV, Perry DG. The intrapsychics of gender: a model of self-socialization. Psychol Rev. 2010 A;117(2):601-22. DOI: http://doi.org/10.1037/a0018936 [ Links ]
12.Frazier SK, Moser DK, Schlanger R, Widener J, Pender L, Stone KS. Autonomic tone in medical intensive care patients receiving mechanical ventilation and during a CPAP weaning trial. Biol Res Nurs. 2008;9(4):301-10. DOI: http://doi.org/10.1177/1099800408314707 [ Links ]
13.Huang CT, Tsai YJ, Lin JW, Ruan SY, Wu HD, Yu CJ. Application of heart rate variability in patients undergoing weaning from mechanical ventilation. Crit Care. 2014;18(1):R21. DOI: http://doi.org/10.1186/cc13705 [ Links ]
14.Sasaki K, Maruyama R. Consciously controlled breathing decreases the high-frequency component of heart rate variability by inhibiting cardiac parasympathetic nerve activity. Tohoku J Exp Med. 2014;233(3):155-63. DOI: http://doi.org/10.1620/tjem.233.155 [ Links ]
15.Task Force of the European Society of Cardiology and the North American Society of Pacing and Electrophysiology.Heart rate variability: standards of measurement, physiological interpretation and clinical use. Circulation. 1996;93(5):1043-65. [ Links ]
16.Pumprla J, Howorka K, Groves D, Chester M, Nolan J. Functional assessment of heart rate variability: physiological basis and practical applications. Int J Cardiol. 2002;84(1):1-14. [ Links ]
17.Vanderlei LCM, Silva RA, Pastre CM, Azevedo FM, Godoy MF. Comparison of polar S810i monitor and the ECG for the analysis of heart rate variability in the time and frequency domains. Braz J Med Bio Res. 2008;41(10):854-9. DOI: http://dx.doi.org/10.1590/S0100-879X2008005000039 [ Links ]
18.Ribeiro JP, Moraes Filho RS. Variabilidade da Frequência cardíaca como instrumento de investigação do sistema nervoso autônomo. Rev Bras Hipertens. 2005;12(1):14-20. [ Links ]
19.Vanderlei LCM, Pastre CM, Hoshi RA, Carvalho TDias, Godoy MF. Noções básicas de variabilidade da frequência cardíaca e sua aplicabilidade clínica. Rev Bras Cir Cardiovasc. 2009;24(2):205-17. DOI: http://dx.doi.org/10.1590/S0102-76382009000200018 [ Links ]
20.Gamelin FX, Berthoin S, Bosquet L. Validity of the Polar S810 Heart Rate Monitor to Measure R-R Intervals at Rest. Med Sci Sports Exerc. 2006;38(5):887-93. DOI: http://doi.org/10.1249/01.mss.0000218135.79476.9c [ Links ]
21.Terathongkum S, Pickler RH. Relationships among heart rate variability, hypertension, and relaxation techniques. J Vasc Nurs. 2004;22(3):78-82. DOI: http://doi.org/10.1016/j.jvn.2004.06.003 [ Links ]
22.Tulppo MP, Mäkikallio TH, Seppänen T, Laukkanen RT, Huikuri HV. Vagal modulation of heart rate during exercise: effects of age and physical fitness. Am J Physiol. 1998;274 (2Pt 2):H424-9. DOI: http://doi.org/10.1152/ajpheart.1998.274.2.H424 [ Links ]
23.Aubert AE, Seps B, Beckers F. Heart rate variability in athletes. Sports Med. 2003;33(12):889-919. DOI: http://doi.org/10.2165/00007256-200333120-00003 [ Links ]
24.Riad FS, Razak E, Saba S, Shalaby A, Nemec J. Recent heart rate history affects QT interval duration in atrial fibrillation. PLoS One. 2017;12(3):e0172962. DOI: http://doi.org/10.1371/journal.pone.0172962 [ Links ]
25.Nagaraj SB, Ramaswamy SM, Biswal S, Boyle EJ, Zhou DW, Mcclain LM, et al. Heart rate variability as a biomarker for sedation depth estimation in ICU patients. Conf Proc IEEE Eng Med Biol Soc. 2016;2016:6397-6400. DOI: http://doi.org/10.1109/EMBC.2016.7592192 [ Links ]
26.Kim CS, Kim MK, Jung HY, Kim MJ. Effects of exercise training intensity on cardiac autonomic regulation in habitual smokers. Ann Noninvasive Electrocardiol. 2017;22(5). DOI: http://doi.org/10.1111/anec.12434 [ Links ]
27.Bisschoff CA, Coetzee B, Esco MR. Relationship between Autonomic Markers of Heart Rate and Subjective Indicators of Recovery Status in Male, Elite Badminton Players. J Sports Sci Med. 2016;15(4):658-69. [ Links ]
28.Guerra M, Pidori Igreja T, Carvalho TD, Valenti VE, Abreu LC, Silva TD, et al. Heart Rate Variability During Weaning Mechanical Ventilation. J Cardiol Ther. 2016; 3(3):519-22. [ Links ]
29.Vitacca M, Scalvini S, Volterrani M, Clini EM, Paneroni M, Giordano A, et al. In COPD patients on prolonged mechanical ventilation heart rate variability during the T-piece trial is better after pressure support plus PEEP: a pilot physiological study. Heart Lung. 2014;43(5):420-6. DOI: http://doi.org/10.1016/j.hrtlng.2014.04.003 [ Links ]
30.Astorino TA, Robergs RA, Ghiasvand F, Marks D, Burns S. Incidence of the oxygen plateau at VO2max during exercise testing to volitional fatigue. J Exerc Physiol. 2000;3(4):1-12. [ Links ]
 Correspondence:
Correspondence:
rodrigo.raimundo@fmabc.br
Manuscript received: December 2018
Manuscript accepted: August 2019
Version of record online: October 2019


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}