










Serviços Personalizados
Journal

artigo
 Inglês (pdf)
Inglês (pdf)
 Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
 Curriculum ScienTI
Curriculum ScienTIIndicadores
Compartilhar

 Permalink
PermalinkJournal of Human Growth and Development
versão impressa ISSN 0104-1282versão On-line ISSN 2175-3598
J. Hum. Growth Dev. vol.29 no.3 São Paulo set./dez. 2019
https://doi.org/10.7322/jhgd.v29.9538
ORIGINAL ARTICLE
Impact of the nutrition education Program Nutriamigos® on levels of awareness on healthy eating habits in school-aged children
Suzana Janson FranciscatoI; Guilherme JansonII; Rachel MachadoIII; José Roberto Pereira LaurisIV; Silvana Marques Javarez de AndradeV; Mauro FisbergVI
INutricionista - Especialista em Clínica e Terapêutica Nutricional. Diretora da PEN- Programa de Educação Nutricional Ltda. Instituto PENSI/Hospital Infantil Sabará/Fundação José Luiz Egídio Setúbal - Consolação/SP
IIProfessor Titular. Disciplina de Ortodontia. Departamento de Ortodontia, Odontopediatria e Saúde Coletiva. Faculdade de Odontologia de Bauru - Universidade de São Paulo. Bauru- SP
IIINutricionista, Formada pelo Centro Univ. São Camilo, Especialista em Nutrição Clínica (HC-FMUSP) e Pediatria (EPM/UNIFESP), Mestre em Ciências da Saúde (EPM/UNIFESP). Instituto PENSI/Hospital Infantil Sabará/Fundação José Luiz Egídio Setúbal - Consolação/SP
IVProfessor Titular, Departamento de Odontopediatria, Ortodontia e Saúde Coletiva. Faculdade de Odontologia de Bauru, Universidade de São Paulo. Bauru- SP
VNutricionista, Formada pela Universidade do Sagrado Coração. Instituto PENSI/Hospital Infantil Sabará/Fundação José Luiz Egídio Setúbal - Consolação/SP
VIPediatra e Nutrólogo, Professor Associado do departamento de Pediatria da Escola Paulista de Medicina-UNIFESP e Coordenador do Centro de Dificuldades Alimentares do Instituto Pensi- Fundação José Luiz Setúbal - Hospital Infantil Sabará. Instituto PENSI/Hospital Infantil Sabará/Fundação José Luiz Egídio Setúbal - Consolação/SP
ABSTRACT
INTRODUCTION: With the increase of childhood obesity, early intervention in nutrition education becomes necessary. Therefore, during the school period, the school becomes the best place for implementation of a nutritional education program.
OBJECTIVE: The current study was carried out in a public and in a private school, with the objective of evaluating and comparing the results of the "Nutriamigos®" Program on food and nutrition knowledge of children with different socioeconomic levels, sex, age and Body Mass Index (BMI).
METHODS: Comparative longitudinal study, before and after educational intervention. To evaluate the intervention, a public (school 1) and a private school (school 2) were selected. This was a random, convenience sample comparing students from different social and economic levels, consisting of 242 (school 1) and 99 children (school 2), respectively, totaling 341 children, from 6 to 10 years of age. The Body Mass Index was used to measure nutritional status. Knowledge about food and nutrition was evaluated through a questionnaire, applied before and after intervention. The nutritional intervention consisted of 12 classes of 50 minutes each.
RESULTS: The improvement in knowledge on food and nutrition between the pre and post intervention stages was statistically significant.
CONCLUSION: The "Nutriamigos®" Program reached its goal, proving that it is effective in public and private schools and should not be different for boys or girls, or for children with normal or excessive weight.
Keywords: food and nutrition education, eating behavior, animation, child.
Authors summary
Why was this study done?
The study was conducted with the objective of evaluating and comparing the results of the "Nutriamigos®" Program in the knowledge about food and nutrition of children of different socioeconomic levels, gender, age and Body Mass Index (BMI). The Nutriamigos® Program was developed by author Suzana Janson Franciscato, who playfully presents the universe of food and its importance to health through games, multimedia activities and cartoons.
What did the researchers do and find?
To evaluate the intervention, a public and a private school were selected. Students from different social and economic levels were compared, totaling 341 children, from 6 to 10 years old. To measure nutritional status the Body Mass Index (BMI) was used. Nutrition and dietary knowledge was assessed by means of a knowledge questionnaire applied before and after intervention. The intervention consisted of 12 classes of 50 minutes each. As a result, we had improved knowledge about food and nutrition between the pre and post intervention stages.
What do these findings mean?
These findings mean that the "Nutriamigos®" program has achieved the proposed objective by proving to be effective in public and private schools and should not be differentiated for boys or girls, or for children of normal or overweight.
INTRODUCTION
The increase in childhood obesity is directly related to an unbalanced diet and a sedentary lifestyle1,2 and can lead to chronic diseases, such as hypertension, dyslipidaemia and diabetes3,4.
Official data from the 2013 Food and Nutrition Surveillance System (SISVAN) indicates that in Brazil, overweight accounts for 15% of children in the age range 0-6 years, with males having a higher prevalence than females, at 15.9% and 14.45%, respectively5.
Many factors interfere with eating habits, such as the environment, family, culture and socio-economic status6. Behaviours that are established in childhood can persist into adult life. Consequently, early intervention7 through specific nutritional education programs is required in an attempt to improve dietary knowledge and influence choices, and ultimately, health8-10.
The eating habits of school-aged children are greatly influenced by the school environment, and friends become a reference for the child, whereas pre-schoolers are chiefly influenced by the family environment. The school environment fosters independence, making decisions and evaluating choices, which are necessary and critical life-long skills. Therefore, school becomes the best place for the implementation of a nutritional education program, both because it is a reference environment and because of the opportunity to reach a large number of children11,12.
In 2014, the Pan American Health Organisation (PAHO) of which Brazil is a Member State, launched the "Plan of Action for the prevention of obesity in children and adolescents", with the objective of implementing effective policies in several strategic areas of action, such as promoting healthy eating habits and practicing physical activity in the school environment13. Brazil has been developing important preventive actions, based on the school environment, aimed at the control of childhood obesity through the National School Feeding Program (PNAE), managed by the National Education Fund (FNDE)14.
Several studies found a positive relationship between knowledge and improvement in the intake of fruits, vegetables and milk derivatives after educational intervention15-18, while others did not reach the same results19-21. However, in the US, school education programs are considered effective for the prevention of childhood obesity9,22,23.
According to some authors, low socio-economic status is associated with the ingestion of less healthy foods, such as soft drinks and fast foods, as well with a lower level of knowledge about food and nutrition24,25. It takes 10 to 15 hours of educational intervention to improve knowledge about nutrition, 40 to 50 hours for changes in eating behavior26 and 26 hours of intervention for weight loss in children and adolescents aged over six years, according to the United States Preventive Service Task Force (USPSTF)27.
The "Nutriamigos®"28 nutrition education program is a ludic approach to teaching the universe of food and its importance in health through games, multimedia activities and cartoons. It facilitates learning, attracts attention and provides more effective participation of children. "Nutriamigos®" focuses on all food groups, thereby providing global learning for future improvement in eating habits, whereas other programs are limited to working with fruit and vegetable groups29-31. Furthermore, the teacher's manual is also included, which allows the teacher to easily incorporate the theme into other subjects, including mathematics, science, music and cooking, with diverse dynamics, such as painting, music, collage, crossword puzzles, cut-outs, cooking and vegetable garden, unlike others which only use theoretical classes9 and/or board games23. Additional advantages include free access to the YouTube channel32 and the website33, besides the possibility of using these instruments for several years in different school series, increasing the total number of children benefited without additional investment for schools28.
In Brazil, the "Nutriamigos®" program has been approved by the Education Departments of 20 states and is being used by 3240 public schools, both by nutritionists and teachers. The objective of this study was to evaluate and compare the results of the nutrition education program "Nutriamigos®" in the knowledge about feeding and nutrition of children from different socio-economic levels, and of different sex, age and body mass index (BMI) by applying a knowledge questionnaire before and after the intervention.
METHODS
Study design and population
This comparative (before and after) longitudinal clinical study of an educational intervention was carried out in Bauru, São Paulo, Brazil. For the evaluation of the intervention, this study used a convenience sample of a public school (school 1) and a private school (school 2), randomly comparing students from different social and economic levels, according to the operational possibility of project implementation.
The public school is maintained by the town hall. It has 304 students enrolled in the six- to ten-year age group. This school was chosen because it is located on the outskirts of the city, has not yet had access to nutrition education classes, specifically the "Nutriamigos®" program, and had the request of teachers interested in nutrition education work. Through data provided by the school's management, these students fit into the socio-economic stratum C2 (average monthly family income of R$1,625.00) of the Critério Brasil economic classification34.
The private school is a Brazilian bilingual school that follows the curricular structure stipulated by the Ministry of Education and Culture (MEC). It has 101 students enrolled in the six- to ten-year age group. It was chosen because it is a high socio-economic school, compatible with students of the socio-economic stratum A (average monthly family income of R$20,888.00)34 and is located in a neighbourhood of high-income families. The school has nutritionists who, despite providing some nutritional education classes for children during the year, do not have a planning routine and do not follow a specific program. The topics covered during the sporadic interventions were themes related to commemorative dates of Brazilian folklore, cooking classes, food portions at meal-times and the importance of breakfast.
Participants in the study were children who were authorised by their parents or guardian by signing of the Informed Consent Form (ICF) and who were present at all stages of information collection. The ICF was delivered to all 405 children and was returned by 270 students in school 1 (public) and 101 in school 2 (private), respectively.
Of the 371 children who returned the ICF and had begun the evaluation, twenty-eight were excluded from school 1 (public) and two from school 2 (private) because they were not present at all stages of information gathering, were unable to complete the questionnaires or presented intellectual limitations to understanding the questionnaires or the intervention program (School Inclusion). Therefore, the final sample included 242 and 99 children from the public and private schools, respectively, totalling 341 children.
The study began in August 2013, with nutritional assessment and application of the pre-intervention knowledge questionnaire. The nutritionists responsible for the study applied the nutrition education intervention for 12 consecutive weeks, one class per week, lasting 50 minutes each, and subsequently, evaluation of the knowledge questionnaire was repeated. The school principals were duly informed and consented the study.
Nutritional evaluation
Pre-intervention nutritional assessment was performed. The following children's data were collected:
a) Weight (kg): evaluated using a Filizola scale, calibrated to the approximation of 100 g. The children remained in school uniforms, and their shoes and socks were removed. The results were expressed as the mean of triplicate readings.
b) Height (m): A vertical anthropometer was used to measure the children's body height in the standing position. Measurement was done with the children without shoes, socks and any headgear. Measurements were performed with the children standing erect, arms loose along the trunk, feet joined, buttocks and shoulder blades touching the vertical rod.
All measurements were taken individually in a classroom, according to the school organisation and the teacher responsible for the group of students. The results were delivered in closed envelopes to the teacher in charge and distributed to each student to deliver to their parents or legal guardians.
Weight and height were used to classify nutritional status. Based on these data, BMI was calculated as body mass in kilograms, divided by height in meters, squared (kg/m2). For the classification of nutritional status, the World Health Organisation (WHO) program AnthroPlus (growth curves for children and adolescents aged between five and nineteen years)35 was used. The percentiles (P) classification was applied where BMI<P3 is thinness, P3>BMI<P84 is eutrophic, P85>BMI<P97 is overweight, and BMI>P97 is obese.
The children were separated into two groups: overweight (overweight, obesity and severe obesity) and normal (eutrophic and thinness), according to the WHO criteria described above35.
Questionnaires
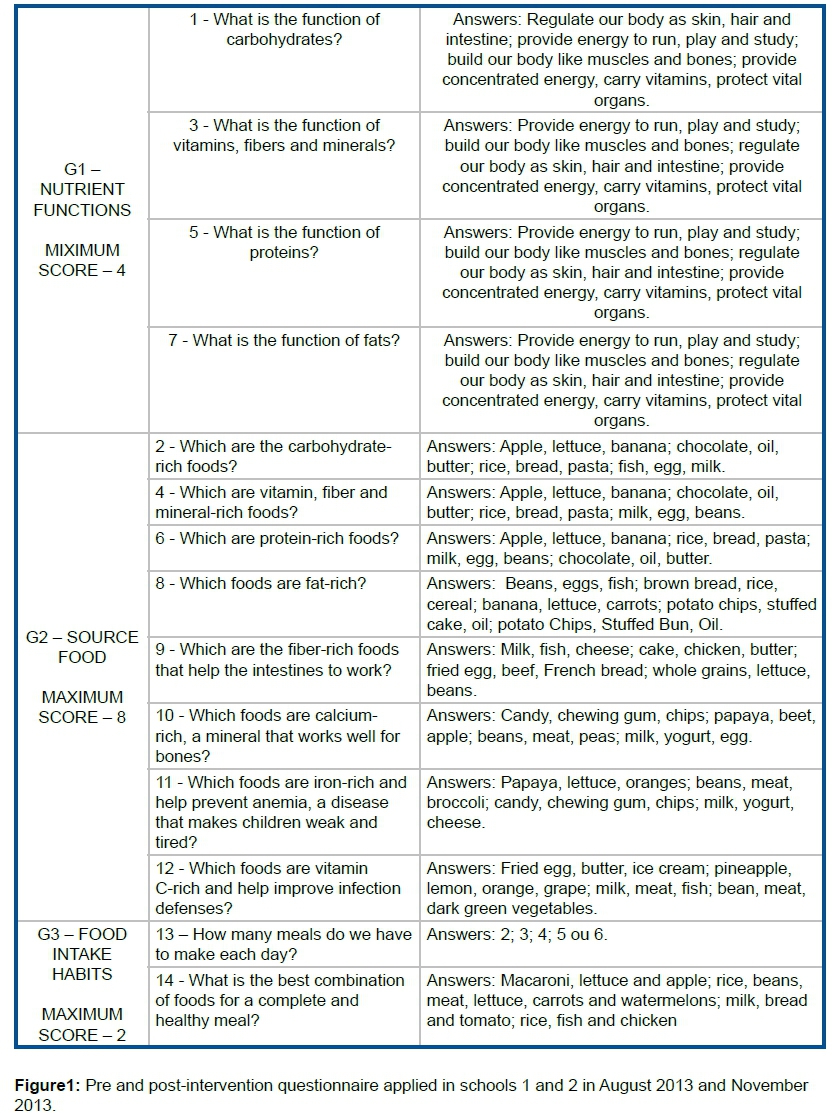
Pre- and post-intervention questionnaires were applied to evaluate knowledge about nutrition and food intake (Figure 1). Two models of original questionnaires were developed for children, based on others already established9,16,36-41. The questionnaires presented 14 questions with multiple choice answers and only one correct answer: one with images for application in children not fully literate in the age group between six and eight years, and another with text only for children aged between nine and ten years, according to the content worked. For children aged six to eight years, illustrations were used in the answers, and the questions were read aloud and explained by the nutritionist to aid understanding, considering these students are in the literacy phase. For the age group of nine to ten years, the questions were all in text and always related to the content given in the educational intervention. The questions were read aloud by the responsible nutritionist, as well as all answer options, but always guiding the child to answer without help from the class teacher and friends (Figure 1).
Each question was worth one (1) point for each correct answer, totalling a maximum of 14 points. Based on the model of other authors16, the questions were grouped into the following topics: Group 1 (G1): nutrient functions (four questions, numbers 1, 3, 5 and 7), Group 2 (G2): food sources (eight questions, numbers 2, 4, 6, 8, 9, 10, 11, 12) and Group 3 (G3): healthy habits (two questions, numbers 13 and 14), with each group having maximum scores of four, eight and two points, respectively. The questions belonging to G1 referred to knowledge about the function of nutrients, leading the child to know the name of the nutrient and its importance in the body. The questions in G2 were about food sources of the mentioned nutrients, and G3 addressed knowledge about healthy eating habits. The questionnaire was applied by the nutritionists responsible for the study to facilitate the understanding of the questions (figure 1).
Nutritional intervention
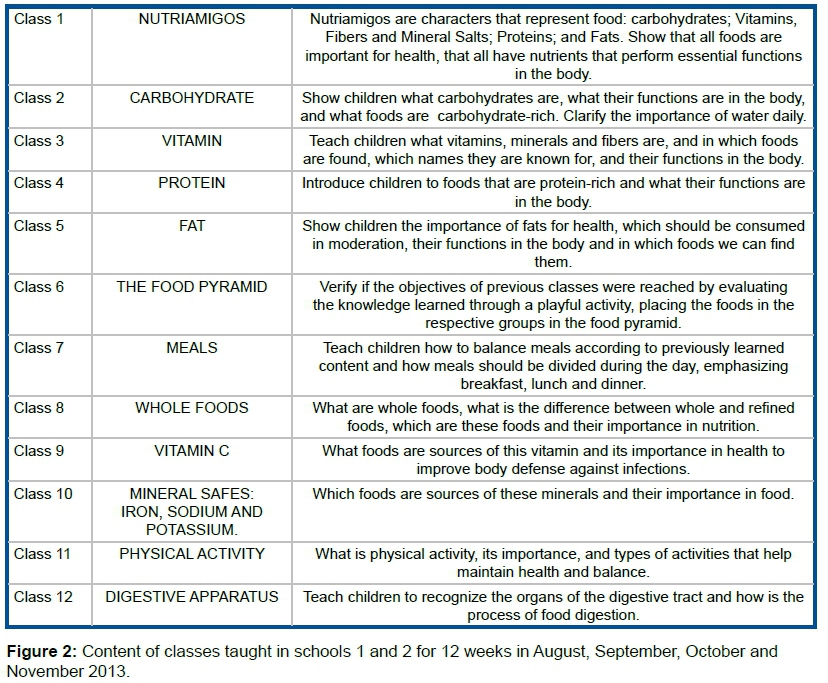
In the present study, the "Nutriamigos®"28 nutrition education program consisted in a classroom application of a DVD content composed of five cartoon episodes of 11 minutes each, with songs and accessible language, in which the main characters represent the nutrients: carbohydrates, vitamins, proteins and fats. In each episode, the importance of a particular group of foods as sources of nutrients and their functions in the organism were emphasised.
In addition to the five episodes in animation, other topics were worked into seven other classes, as follows: food pyramid, meals with emphasis on breakfast, lunch and dinner, whole foods, vitamin C, micronutrients, such as iron, calcium and sodium, importance of physical activity and digestive apparatus, totalling 12 classes. Play materials, including posters, games and paintings, were used, based on the Food Guide for the Brazilian Population of the Ministry of Health42 (Figure 2). Printed pedagogical activities complemented the information and fixed the learning, with each class being completed in 50 minutes. The classes were applied by the nutritionists responsible for the study, with the presence of the responsible teachers of each class of the schools. Classes were included in normal school hours, according to the organisation of the pedagogical coordination of the school (Figure 3).
The acquired knowledge, evaluated by the results in points, questionnaires, and pre- and post-school intervention questions were compared by the Wilcoxon test. For the inter-school comparison of pre- and post-intervention knowledge, the Mann-Whitney test was applied.
All statistical procedures were performed in the SPSS for Windows program (version 17.0; SPSS, Inc., Chicago, IL). In all statistical tests, the significance level of 5% was adopted.
The study was approved by Ethics in Research Committee of the Instituto PENSI - Hospital Infantil Sabará - Fundação José Luiz Egydio Setúbal, in the city of São Paulo, Brazil, case number CAAE: 20205213.1.0000.5567.
RESULTS
Sample characteristics
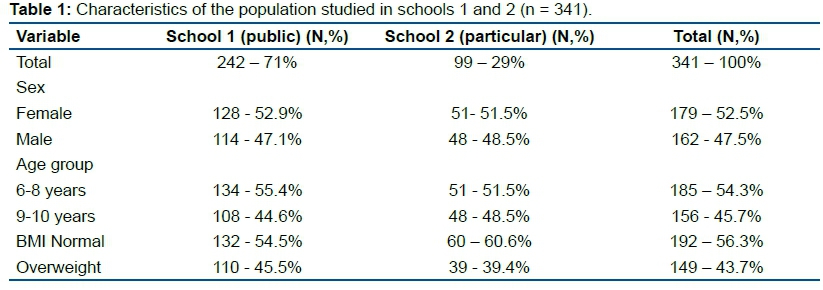
A total of 242 children from the public school (school 1) and 99 from the private school (school 2) participated in the study, totalling 341 children, with 179 females and 162 males (Table 1).
In total, 185 children aged six to eight years and 156 aged nine to ten years were evaluated, representing 54.3% and 45.7% of the sample, respectively. Overweight represented 45.5% of students in school 1 (public) and 39.4% in school 2 (private), as shown in Table 1. All classes planned were completed in both schools.
Questionnaires
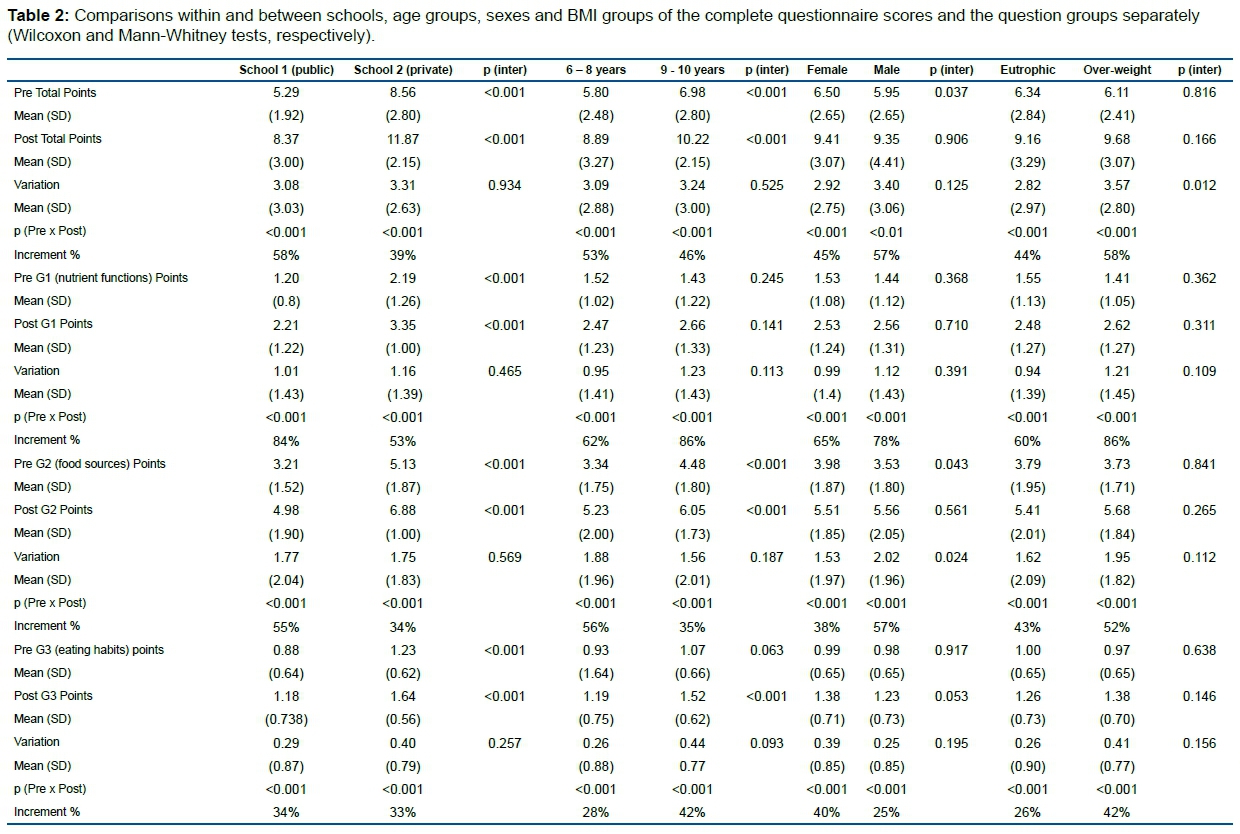
Regarding the complete questionnaire and the groups of questions, knowledge about diet and nutrition improved significantly between the beginning and end of the study in the two schools, different age groups, sexes and in the two BMI groups (Table 2).
Knowledge about feeding and nutrition was significantly higher in school 2 (private) than in school 1 (public) at the beginning and end. However, the percentage of increase in knowledge acquired after intervention was higher in school 1 (public) than in school 2 (private) in all groups, except for G3 (healthy habits), in which both schools had practically the same number of correct answers (Table 2).
The older children presented significantly higher knowledge in the questions of the entire questionnaire and G2 questions (food sources) at pre- and post-intervention, as well as in G3 questions (dietary habits) at post-intervention relative to the younger-aged children (Table 2). However, the percentage of increment in knowledge acquired after the intervention was higher in the youngest of the age groups, in the complete questionnaire and G2 questions (food sources). In G1 (nutrient functions) and G3 (food habits) questions, in which there were no significant differences at the pre-intervention phase, the percentage of increment in knowledge acquired after intervention was higher in the older than in the younger age group.
Females presented a significantly higher knowledge in the questions of the entire questionnaire and G2 questions (food sources) at pre-intervention when compared with the males, while males displayed significantly greater improvement in knowledge of G2 questions (food sources), as shown in Table 2. The percentage of increment in knowledge acquired after intervention was higher in males than in females in the questions of the entire questionnaire and those in G1 (nutrient functions) and G2 (food sources). In G3 questions (eating habits), females showed a superior percentage of acquired knowledge.
There were no significant differences in knowledge about diet and nutrition at the pre- and post-intervention stages among groups with different BMI, but the improvement in post-intervention knowledge in the complete questionnaire was significantly greater in the overweight group (Table 2). In comparison to the other BMI groups, the overweight group exhibited a higher percentage of increase in knowledge acquired after intervention in all groups of questions.
Regarding the complete questionnaire and considering all children, the percentage of correct answers in the pre-intervention was 44.6%, and 67% in the post-intervention, corresponding to a 50% improvement in the acquired knowledge.
DISCUSSION
This study presents the results of the "Nutriamigos®" program as a model of nutritional intervention. The increase in knowledge about food and nutrition was significant for both schools. In school 2 (private), knowledge was higher both pre- and post-intervention, but in school 1 (public), the number of correct answers was higher, except for G3 questions (healthy habits) in which both schools had practically the same number of correct answers.
In the older age group, knowledge was higher at pre-intervention, but the younger age group scored more. However, the difference in the number of hits per age was in the specific knowledge area of G2 (food sources). In other knowledge areas, the age of the children made no difference. Regarding sex, females had better pre-intervention knowledge, while males were more successful post-intervention. For G2 questions (food sources), males had a slight difference in the number of correct answers, whereas, in the other groups of questions, there was no inter-sex difference. Among the groups of different BMIs, there was no difference in the number of correct answers at the pre- and post-intervention, but the overweight group was better in all areas of knowledge evaluated.
The main concern in development of the questionnaires was to make it attractive and easy to complete by the children. In this context, it is considered the best method to obtain information on knowledge and eating habits in schools19.
Receptivity was great in both schools, and the schedule of one lesson per week, for 12 weeks, was completed as planned. The teachers waited for the classes and collaborated, reporting the anxiety and expectancy of the children, who actively participated in the activities. This receptiveness demonstrates that the Cartoon Program was very attractive and caught the attention of the students, as it is a playful and easy-to-use tool43.
In the overall assessment, considering all question groups (G1, G2 and G3) separately, there was a statistically significant improvement in knowledge about diet and nutrition between the pre- and post-intervention stages, demonstrating that the "Nutriamigos®" program reached the proposed goal in schools (Table 2).
The nutritional education intervention lasted for 12 weeks, which is considered sufficient to improve knowledge26, helping to raise awareness about healthier choices44. Some studies showed improved knowledge in a relatively shorter intervention time16,45. Nutritionist-trained pharmacy students applied the Kids Eat Healthy program to 468 elementary students for four weeks, with one class per week, and achieved a significant improvement at post-intervention45. Similarly, another study applied the interactive game "Pizza Please Game" to 1100 children for six weeks, and noticed an improvement in knowledge, in addition to changes in eating habits16.
Several studies were carried out in Brazil involving school-aged children, but unlike the present study, did not evaluate the educational process46 and did not analyse pre- and post-intervention knowledge.
Regarding BMI, children of the private school already started with a superior level of knowledge relative to the public school (Table 2). The socio-economic factor may have contributed to this result, as some studies demonstrated an association of higher social class with better knowledge level and, consequently, a better quality of fruit and vegetable intake10,25. Another contributing factor is that the private school curriculum includes nutritional education classes taught sporadically during the school year, unlike the public school, which had no corresponding classes.
Consequently, as the public school started from a lower level of knowledge, these students showed a greater improvement percentage between the pre- and post-intervention phases in all groups of questions than that seen in the students who already had some knowledge (i.e., private school students; Table 2). As a result, school 1 (public) in the post-intervention equated with the level of school 2 (private) pre-intervention.
Older children had a significantly higher initial knowledge relative to the younger children, in the complete questionnaire and G2 questions (food sources) both pre- and post-intervention, as they learn concepts not only in school but also through the influences of the social environment, friends and the media47-49 (Table 2). This result corroborates the importance of introducing nutritional education in schools from the pre-school age, because habits learned in childhood and adolescence are likely to persist into adulthood44,50. Among the children, the percentage of knowledge acquired in all three themes (G1, G2, G3) was higher in the youngest age category. However, in G1 (nutrient functions) and G3 questions (healthy habits), in which there were no significant differences in initial knowledge between the age categories, the percentage of knowledge acquired was higher in the older age group, probably because of the children's greater maturity, which contributes to assimilate knowledge more easily47-49.
In agreement with other studies25,44,51, females presented significantly higher knowledge than males in the questions of the entire questionnaire and G2 questions (food sources) at pre-intervention (Table 2). Some authors explained this result by the fact that girls are more concerned than boys about body health and appearance48,52.
However, boys had significantly greater improvement in post-intervention knowledge of G2 questions (food sources) compared with the girls. The percentages of knowledge acquired by the boys were also higher in the complete questionnaire and in G2 (food sources) questions, in which the initial knowledge was lower than that of the girls, following the same tendency of the other comparisons. However, in G1 (nutrient functions) and G3 questions (healthy habits), in which the initial knowledge was similar between the sexes, the boys had a higher percentage of knowledge acquired in G1 (nutrient functions), and the girls had a greater percentage of knowledge acquired in G3 (healthy habits). Therefore, it suggests that there is no difference in knowledge acquired between the sexes.
Among the groups of normal weight and overweight children, knowledge about feeding and pre-intervention nutrition was similar (Table 2), although it is important to emphasise that the overweight group presented slightly better knowledge in the complete questionnaire after the intervention. In addition, the percentage of knowledge gained in the overweight group was higher for all groups of questions relative to the children of normal weight. This outcome suggests that the applied educational intervention can be positive in the improvement of the knowledge, leading to healthier food choices, thereby helping in the prevention of childhood obesity23.
Analysing these results, it was observed that, in general, whenever knowledge was significantly lower at the beginning of the intervention, the percentage of knowledge acquired was higher after the intervention (Table 2). This behaviour is logical because when taught the same amount of information, the recipient who has less knowledge will acquire more knowledge than the recipient who initially has more.
A qualitative analysis of student performance in the different sets of questions (G1, G2 and G3) can be done because the number of questions was different for each group. Among the groups of questions, there was a greater number of correct answers in G1 (nutrient functions) after the intervention, which suggests that the program used is more effective for this theme than the others addressed. As the program relies on characters representing the nutrients and their food sources, it implies that children fixate this information more than eating habits. Such insight can serve as information for project improvements for future educational interventions.
According to the American Dietetic Association, the School Nutrition Association and the Society for Nutrition Education, nutritional education in schools is one of the strategies to improve the nutritional status of children. However, there is a need to supplement this education with food and nutrition services, and partnerships between schools, parents and health services related to nutrition, so that effective changes in eating habits occur53.
In general, the results achieved by the intervention program applied in this research infer an improvement in knowledge of food and nutrition, which may lead to better dietary choices in the future. The differential of the "Nutriamigos®" program is that it uses playful elements8 through a method called "edutainment"30 and can be applied by teachers themselves. Thus, it has wide reach28, unlike other programs that must be applied by nutrition students or trained professionals23,39,54.
Limitations and strengths
The present study presented some limitations. Among them, the choice of the private school, which already provided the students with some nutritional education classes during the school year. Although the classes did not follow a specific routine and program, it may have contributed to these students starting with a superior level of knowledge than those from the public school. This factor can be taken into account in an upcoming work opportunity to minimise bias, choosing a private school that does not have these classes or even finding a public school with the same type of educational intervention.
Another limitation was the impossibility of statistically comparing questions among G1 (nutrient functions), G2 (food sources) and G3 (eating habits) because the number of questions differed for each group. Accordingly, a new comparative study to evaluate where children have more or less knowledge base and where they are most accurate will provide additional information to be used in intervention programs.
Among the strengths of the work, is the method used in the "Nutriamigos®" program that mixes entertainment with education, and has playful elements in which the characteristics of the characters refer to the children's imagination, presenting information on nutrients and food that is straightforward and easy to understand. The program is accessible to children aged six to ten years and can be applied by nutrition professionals, as well as by teachers. It is also accompanied by complementary didactic material through games, multimedia activities, cartoons and is free on YouTube, facilitating public access.
CONCLUSION
The "Nutriamigos®" program has reached its goal, proving that it is effective in public and private schools and should not be different between boys or girls, or between children of normal or overweight.
REFERENCES
1.Carlson JA, Crespo NC, Sallis JF, Patterson RE, Elder JP. Dietary-related and physical activity-related predictors of obesity in children: a 2-year prospective study. Child Obes. 2012;8(2):110-5. DOI: http://dx.doi.org/10.1089/chi.2011.0071 [ Links ]
2.American Academy of Pediatrics. Prevention of pediatric overweight and obesity. Pediatrics. 2003 Aug;112(2):424-30. DOI: https://doi.org/10.1542/peds.112.2.424 [ Links ]
3.Ebbeling CB, Pawlak DB, Ludwig DS. Childhood obesity: public-health crisis, common sense cure. Lancet 2002;10;360(9331):473-82. DOI: https://doi.org/10.1016/S0140-6736(02)09678-2 [ Links ]
4.Fleck F. WHO challenges food industry in report on diet and health. BMJ. 2003;326(7388):515. DOI: https://doi.org/10.1136/bmj.326.7388.515 [ Links ]
5.Brasil. Ministério da Saúde. Sistema de vigilância alimentar e nutricional (SISVAN). Módulo gerador de relatórios públicos: estado nutricional dos indivíduos acompanhados por período, fase do ciclo da vida e índice 2014. Brasília: Ministério da Saúde, 2014. [ Links ]
6.Zarnowiecki DM, Parletta N, Dollman J. The role of socio-economic position as a moderator of children's healthy food intake. Br J Nutr. 2014;14;112(5):830-40. DOI: https://doi.org/10.1017/S0007114514001354 [ Links ]
7.Davison KK, Birch LL. Childhood overweight: a contextual model and recommendations for future research. Obes Rev. 2001;2(3):159-71. DOI: https://doi.org/10.1046/j.1467-789x.2001.00036.x [ Links ]
8.Contento IR. Nutrition education: linking research, theory, and practice. Asia Pac J Clin Nutr. 2008;17(Suppl 1):176-9. [ Links ]
9.DeVault N, Kennedy T, Hermann J, Mwavita M, Rask P, Jaworsky A. It's all about kids: preventing overweight in elementary school children in Tulsa, OK. J Am Diet Assoc. 2009;109(4):680-7. DOI: https://doi.org/10.1016/j.jada.2008.12.021 [ Links ]
10.Wardle J, Parmenter K, Waller J. Nutrition knowledge and food intake. Appetite. 2000;34(3): 269-75. DOI: https://doi.org/10.1006/appe.1999.0311 [ Links ]
11.Perez-Rodrigo C, Aranceta J. School-based nutrition education: lessons learned and new perspectives. Public Health Nutr. 2001;4(1A):131-9. DOI: https://doi.org/10.1079/phn2000108 [ Links ]
12.Van Cauwenberghe E, Maes L, Spittaels H, van Lenthe FJ, Brug J, Oppert JM, et al. Effectiveness of school-based interventions in Europe to promote healthy nutrition in children and adolescents: systematic review of published and 'grey' literature. Br J Nutr. 2010;103(6):781-97. DOI: https://doi.org/10.1017/S0007114509993370 [ Links ]
13.Pan American Health Organization (PAHO). World Health Organization (WHO). Plan of action for the prevention of obesityin children and adolescents. Washington: WHO, 2014. [ Links ]
14.Brasil. Ministério da Educação. Fundo Nacional de Desenvolvimento da Educação (FNDE). Programa Nacional de Alimentação Escilar (PNAE). Alimentação escolar. [cited 2018 feb 02]. Availabe from: https://www.fnde.gov.br/index.php/programas/pnae/pnae-sobre-o-programa/pnae-sobre-o-pnae [ Links ]
15.Fahlman MM, Dake JA, McCaughtry N, Martin J. A pilot study to examine the effects of a nutrition intervention on nutrition knowledge, behaviors, and efficacy expectations in middle school children. J Sch Health. 2008;78(4):216-22. DOI: https://doi.org/10.1111/j.1746-1561.2008.00289.x [ Links ]
16.Powers AR, Struempler BJ, Guarino A, Parmer SM. Effects of a nutrition education program on the dietary behavior and nutrition knowledge of second-grade and third-grade students. J Sch Health. 2005;75(4):129-33. https://doi.org/10.1111/j.1746-1561.2005.00010.x [ Links ]
17.Ransley JK, Taylor EF, Radwan Y, Kitchen MS, Greenwood DC, Cade JE. Does nutrition education in primary schools make a difference to children's fruit and vegetable consumption? Public Health Nutr. 2010;13(11):1898-904. DOI: https://doi.org/10.1017/S1368980010000595 [ Links ]
18.Warren JM, Henry CJ, Lightowler HJ, Bradshaw SM, Perwaiz S. Evaluation of a pilot school programme aimed at the prevention of obesity in children. Health Promot Int. 2003;18(4):287-96. DOI: https://doi.org/10.1093/heapro/dag402 [ Links ]
19.Contento IR, Randell JS, Basch CE. Review and analysis of evaluation measures used in nutrition education intervention research. J Nutr Educ Behav. 2002;34(1):2-25. DOI: https://doi.org/10.1016/s1499-4046(06)60220-0 [ Links ]
20.Perez-Lizaur AB, Kaufer-Horwitz M, Plazas M. Environmental and personal correlates of fruit and vegetable consumption in low income, urban Mexican children. J Hum Nutr Diet. 2008;21(1):63-71. DOI: https://doi.org/10.1111/j.1365-277X.2007.00839.x [ Links ]
21.Prelip M, Kinsler J, Thai CL, Erausquin JT, Slusser W. Evaluation of a school-based multicomponent nutrition education program to improve young children's fruit and vegetable consumption. J Nutr Educ Behav. 2012;44(4):310-8. DOI: https://doi.org/10.1016/j.jneb.2011.10.005 [ Links ]
22.Veugelers PJ, Fitzgerald AL. Effectiveness of school programs in preventing childhood obesity: a multilevel comparison. Am J Public Health. 2005;95(3):432-35. DOI: https://doi.org/10.2105/AJPH.2004.045898 [ Links ]
23.Viggiano A, Viggiano E, Di Costanzo A, Viggiano A, Andreozzi E, Romano V, et al. Kaledo, a board game for nutrition education of children and adolescents at school: cluster randomized controlled trial of healthy lifestyle promotion. Eur J Pediatr. 2015;174(2):217-28. DOI: https://doi.org/10.1007/s00431-014-2381-8 [ Links ]
24.Ranjit N, Wilkinson AV, Lytle LM, Evans AE, Saxton D, Hoelscher DM. Socioeconomic inequalities in children's diet: the role of the home food environment. Int J Behav Nutr Phys Act. 2015; 12(Suppl 1):S4. DOI: https://doi.org/10.1186/1479-5868-12-S1-S4 [ Links ]
25.Skardal M, Western IM, Ask AM, Overby NC. Socioeconomic differences in selected dietary habits among Norwegian 13-14 year-olds: a cross-sectional study. Food Nutrit Res. 2014;58. DOI: https://doi.org/10.3402/fnr.v58.23590 [ Links ]
26.Connell DB, Turner RR, Mason EF. Summary of findings of the School Health Education Evaluation: health promotion effectiveness, implementation, and costs. J Sch Health. 1985;55(8):316-21. DOI: https://doi.org/10.1111/j.1746-1561.1985.tb05656.x [ Links ]
27.Preventive Services Task Force. Screening for obesity in children and adolescents: recommendation statement. Am Fam Physician. 2017;96(8):528A-E. [ Links ]
28.Janson G, Franciscato SJ, Fisberg M. Desenvolvimento do programa de educação nutricional "Nutriamigos®" - uma Ferramenta lúdica para ensinar às crianças o valor dos alimentos. [cited 2018 Feb 02. Available from: http://www.nutricaoempauta.com.br/lista_artigo.php?cod=2812 [ Links ]
29.Anderson AS, Porteous LE, Foster E, Higgins C, Stead M, Hetherington M, et al. The impact of a school-based nutrition education intervention on dietary intake and cognitive and attitudinal variables relating to fruits and vegetables. Public Health Nutr. 2005;8(6):650-6. DOI: https://doi.org/10.1079/phn2004721 [ Links ]
30.Baranowski T, Baranowski J, Cullen KW, Marsh T, Islam N, Zakeri I, et al. Squire's Quest! Dietary outcome evaluation of a multimedia game. Am J Prev Med. 2003;24(1):52-61. DOI: https://doi.org/10.1016/S0749-3797(02)00570-6 [ Links ]
31.Rosi A, Scazzina F, Ingrosso L, Morandi A, Del Rio D, Sanna A. The "5 a day" game: a nutritional intervention utilising innovative methodologies with primary school children. Int J Food Sci Nutr. 2015;66(6):713-7. DOI: https://doi.org/10.3109/09637486.2015.1077793 [ Links ]
32.Franciscato SJ. Programa Nutriamigos. [cited 2018 Feb 02]. Available from: https://http://www.youtube.com/channel/UCHOgvbNmDdj4JRZOITgfh1A [ Links ]
33.Franciscato SJ. Programa Nutriamigos. [cited 2018 Feb 02]. Available from: http://www.nutriamigos.com.br [ Links ]
34.Critério de Classificação Econômica Brasil (ABEP). Critério Brasil 2015 e atualização da distribuição de classes para 2016. [cited 2018 Feb 02]. Available from: http://www.abep.org/criterio-brasil [ Links ]
35.World Health Organization (WHO). Growth reference data for 5-19 years. [cited 2018 Feb 02]. Available from: https://www.who.int/growthref/en/ [ Links ]
36.Amaro S, Viggiano A, Di Costanzo A, Madeo I, Baccari ME, Marchitelli E, et al. Kaledo, a new educational board-game, gives nutritional rudiments and encourages healthy eating in children: a pilot cluster randomized trial. Eur J Pediatr. 2006;165(9):630-5. DOI: https://doi.org/10.1007/s00431-006-0153-9 [ Links ]
37.Anderson AS, Bell A, Adamson A, Moynihan P. A questionnaire assessment of nutrition knowledge--validity and reliability issues. Public Health Nutr. 2002;5(3):497-503. DOI: https://doi.org/10.1079/PHNPHN2001307 [ Links ]
38.Caballero B, Clay T, Davis SM, Ethelbah B, Rock BH, Lohman T, et al. Pathways: a school-based, randomized controlled trial for the prevention of obesity in American Indian schoolchildren. Am J Clin Nutr. 2003;78(5):1030-8. DOI: https://doi.org/10.1093/ajcn/78.5.1030 [ Links ]
39.Rosi A, Brighenti F, Finistrella V, Ingrosso L, Monti G, Vanelli M, et al. Giocampus school: a "learning through playing" approach to deliver nutritional education to children. Int J Food Sci Nutr. 2016;67(2):207-15. DOI: https://doi.org/10.3109/09637486.2016.1144720 [ Links ]
40.Stevens J, Cornell CE, Story M, French SA, Levin S, Becenti A, et al. Development of a questionnaire to assess knowledge, attitudes, and behaviors in American Indian children. Am J Clin Nutr. 1999;69(4 Suppl):773S-81. DOI: https://doi.org/10.1093/ajcn/69.4.773S [ Links ]
41.Vereecken C, De Pauw A, Van Cauwenbergh S, Maes L. Development and test-retest reliability of a nutrition knowledge questionnaire for primary-school children. Public Health Nutr. 2012;15(9):1630-8. DOI: https://doi.org/10.1017/S1368980012002959 [ Links ]
42.Brasil. Ministério da Saúde. Secretaria de Assistência à Saúde. Departamento de Atenção Básica. Guia alimentar para a população brasileira: promovendo a alimentação saudável Brasília: Ministério da Saúde, 2006. [ Links ]
43.Banchonhattakit P, Duangsong R, Muangsom N, Kamsong T, Phangwan K. Effectiveness of brain-based learning and animated cartoons for enhancing healthy habits among school children in Khon Kaen, Thailand. Asia Pac J Public Health. 2015;27(2):NP2028-39. DOI: https://doi.org/10.1177/1010539512466425 [ Links ]
44.Tallarini A, Zabeo A, Ferraretto A. Nutritional knowledge in an Italian population of children, pre-adolescents and adolescents. Public Health Nutr. 2014;17(3):708-14. DOI: https://doi.org/10.1017/S1368980013000311 [ Links ]
45.Falter RA, Pignotti-Dumas K, Popish SJ, Petrelli HM, Best MA, Wilkinson JJ. A service learning program in providing nutrition education to children. Am J Pharm Educ. 2011;10;75(5):85. DOI: https://doi.org/10.5688/ajpe75585 [ Links ]
46.Cervato-Mancuso AM, Vincha KRR, Santiago DA. Educação Alimentar e Nutricional como prática de intervenção: reflexão e possibilidades de fortalecimento. Physis. 2016;26(1):225-49. DOI: http://dx.doi.org/10.1590/S0103-73312016000100013 [ Links ]
47.Grosso G, Mistretta A, Turconi G, Cena H, Roggi C, Galvano F. Nutrition knowledge and other determinants of food intake and lifestyle habits in children and young adolescents living in a rural area of Sicily, South Italy. Public Health Nutr. 2013;16(10):1827-36. DOI: http://dx.doi.org/10.1017/S1368980012003965 [ Links ]
48.Pirouznia M. The association between nutrition knowledge and eating behavior in male and female adolescents in the US. Int J Food Sci Nutr. 2001;52(2):127-32. DOI: http://dx.doi.org/10.1080/713671772 [ Links ]
49.Reinehr T, Kersting DM, Chahda C, Wollenhaupt A, Andler W. Nutritional knowledge of obese and nonobese children. J Ped Gastroenterol Nut. 2001;33(3):351. DOI: http://dx.doi.org/10.1097/00005176-200109000-00026 [ Links ]
50.Matheson D, Spranger K, Saxe A. Preschool children's perceptions of food and their food experiences. J Nutr Educ Behav. 2002;34(2):85-92. DOI: http://dx.doi.org/10.1016/s1499-4046(06)60073-0 [ Links ]
51.Sichert-Hellert W, Beghin L, De Henauw S, Grammatikaki E, Hallstrom L, Manios Y, et al. Nutritional knowledge in European adolescents: results from the HELENA (Healthy Lifestyle in Europe by Nutrition in Adolescence) study. Public Health Nutr. 2011;14(12):2083-91. DOI: http://dx.doi.org/10.1017/S1368980011001352 [ Links ]
52.Triches RM, Giugliani ER. Obesity, eating habits and nutritional knowledge among school children. Rev Saude Pública. 2005;39(4):541-7. DOI: http://dx.doi.org/10.1590/s0034-89102005000400004 [ Links ]
53.Briggs M, Fleischhacker S, Mueller CG; American Dietetic Association. School Nutrition Association. Society for Nutrition Education. Position of the American Dietetic Association, School Nutrition Association, and Society for Nutrition Education: comprehensive school nutrition services. J Nutr Educ Behav. 2010;42(6):360-71. DOI: http://dx.doi.org/10.1016/j.jneb.2010.08.007 [ Links ]
54.Gower JR, Moyer-Mileur LJ, Wilkinson RD, Slater H, Jordan KC. Validity and reliability of a nutrition knowledge survey for assessment in elementary school children. J Am Diet Assoc. 2010; 110(3):452-56. DOI: http://dx.doi.org/10.1016/j.jada.2009.11.017 [ Links ]
 Correspondence:
Correspondence:
rhvmachado@gmail.com
Manuscript received: September 2018
Manuscript accepted: August 2019
Version of record online: October 2019


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}