










Serviços Personalizados
Journal

artigo
 Inglês (pdf)
Inglês (pdf)
 Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
Indicadores
Compartilhar

 Permalink
PermalinkJournal of Human Growth and Development
versão impressa ISSN 0104-1282versão On-line ISSN 2175-3598
J. Hum. Growth Dev. vol.30 no.1 São Paulo jan./abr. 2020
https://doi.org/10.7322/jhgd.v30.9974
ORIGINAL ARTICLE
Guidelines and practices on feeding children with cerebral palsy
Orientações e práticas na alimentação de crianças com Paralisia Cerebral
Luiza MaggioniI, II, III; Cláudia Marina Tavares de AraújoI
IPrograma de Pós-Graduação em Saúde da Criança e do Adolescente, Universidade Federal de Pernambuco (UFPE) - Recife (PE), Brasil
IIInstituto de Medicina Integrada Professor Fernando Figueira (IMIP) - Recife (PE), Brasil
IIIReal Hospital Português (RHP) - Recife (PE), Brasil
ABSTRACT
INTRODUCTION: Cerebral palsy refers to developmental disorders with direct repercussions on posture control and motricity. Its non-progressive and happens by damage of the brain still in development. Children with Cerebral Palsy (CP) present alterations in the oral functions, which makes feeding difficult and can bring serious health consequences, such as malnutrition and pneumonia. The caregiver plays an essential role of these children's diet, so they need to know the implementation of best practices to provide safe food. Guidelines for food practices and care are essential and need to be satisfactory and effective to avoid complications and reduce stress for the caregiver and child. The speech therapist is the skilled professional in assisting and intervening in children's eating difficulties and in guiding the caregiver. However, the guidance provided is not always incorporated into daily practice, and it is key to know and understand it appropriately
OBJECTIVE: To analyze the quality of the guidelines received and the feeding practices of caregivers of children with cerebral palsy
METHODS: This is an exploratory, cross-sectional study, involving 59 main caregivers of children with CP from 1 to 10 years of age, classified as level IV or V in the Gross Motor Function Classification System (GMFCS), with absent cervical control or compensation and fed orally. Data collection carried out through interviews with questions related to the characterization of the sample, quality of the guidelines received regarding feeding and care. The data were entered, pre-coded and processed by the Epi-info 3.5.4 program, using Fisher's exact test to compare categorical variables
RESULTS: Of the total sample, 52 participants had already received speech-language guidance regarding feeding care. Of these, 76.9% were classified as satisfactory guidelines. The most emphasized aspect is related to posture, while signs of risk of bronchoaspiration were the least oriented.The quality of the guidelines was related to safe food consistency, inadequate utensils and facilitating maneuvers during children's feeding
CONCLUSION: The findings reveal that most of the caregivers receive the feeding guidelines for children with CP , however, there is no periodic and systematic monitoring of what is actually incorporated into the feeding . This may indicate a potential gap between the guidelines received by the caregivers and the effectiveness of their daily practice, especially concerning protective measures of the lower respiratory tract
Keywords: Cerebral Palsy, feeding, caregivers, deglutition disorders, childcare.
Authors summary
Why was this study done?
Children with Cerebral Palsy (CP) present alterations in the oral functions, which makes feeding difficult and it can bring serious health consequences, such as malnutrition and pneumonia. The caregiver plays an essential role of these children's diet, so they need to know how to implement best practices to provide safe feed. Guidelines for a good quality of feeding care are essential and need to be effective and safety to avoid complications and reduce stress for the caregiver and child with CP.
What did the researchers do and find?
It was apply a questionnary to 59 caregivers of children with Cerebral Palsy. , with the purpose of investigating the quality of guidelines received about feeding care of children with cerebral palsy and their practices. Of the total sample, 52 participants had already received guidance from the speech language therapist regarding feeding care. Of these, 76.9% classified the guidelines as satisfactory. The most emphasized aspect is related to posture during meal time , while signs of risk of bronchoaspiration were the least oriented.
What do these findings mean?
Even though most of caregivers received orientation on safe practices in feeding children with CP, exists a need for a periodic and systematic monitoring about what is actually incorporated into the feeding practice . This may suggest a potential gap between the guidelines received by the caregivers and the effectiveness of their daily practice.
INTRODUCTION
Cerebral Palsy (CP) is defined1 as a group of permanent disorders in the development of posture and movement, attributed to non-progressive injury in the early period of brain development. It may present sensory, perception, cognition, communication and behavioral changes that occur both as a result of the primary damage and as a secondary consequence of the limitations that restrict the learning and experiences of perceptual development. Therefore, activities such as walking, eating, swallowing and talking are often compromised1.
Children with CP can develop atypical and compensatory movements during oral functioning, evidenced by the difficulty in coordinating swallowing and breathing, as well as in dissociated oral movements, determining eating disorders, which affect different aspects of the child's life2. The degree of difficulty related to the feeding that children and caregivers experience are mainly determined by the type of paralysis, degree of psychomotor impairment and economic and socio-cultural characteristics3,4.
Usually, a mother assumes the role of feeding her child with CP, saying that it is tiring, unpleasant and stressful for her and the child. This is, probably due to the fact that children are unable to supply their need of feeding in a pleasant, effective and positive way. Therefore, coughing, choking, respiratory instability and regurgitation during feeding are frequent, in addition to the time spent in this activity and the requirement of a specific menu5-7.
On the other hand, when the family is oriented on diagnosis, treatment and prognosis, in addition to the child's potential and therapeutic possibilities, they feel more prepared to make decisions which directly impact the reduction of stress8. Thus, the support of qualified professionals becomes essential, to overcoming difficulties and to improve the quality of life of children and their families4,9. Care for children with CP must be comprehensive, with the active participation of the health care and family members10.
Within the healthcare team, the speech therapist is responsible for assessing the function of feeding, contributing to the diagnosis and etiology of dysphagia, assessing the protective capacity of the respiratory system and indicating alternative ways of eating. Likewise, he/she performs direct and indirect intervention with the patient, in addition to guiding staff and family in relation to better attitudes about feeding11. This professional provides guidance on the ideal shape, temperature and consistency of food, eating utensils, postures and behaviors that facilitate oral supply, in order to promote food safety and, consequently, health and quality of life12,13.
Even though feeding difficulties are frequent in patients with CP and widely well known, it is possible that guidelines focused on feeding are not effectively delivered to mothers and caregivers who build concepts and practices regarding food care and nutrition, based on their own and daily experiences3.
Thus, this study aims to analyze the quality of guidelines received and the feeding practices of caregivers of children with Cerebral Palsy.
METHODS
This is a Cross-sectional exploratory study14, carried out with 59 main caregivers of children with CP from 1 to 10 years old, attended in the pediatric outpatient or nursery at the Hospital das Clínicas of the Federal University of Pernambuco and the Instituto de Medicina Integral Professor Fernando Figueira (IMIP). Inclusion criteria were considered: Care givers of children with compensatory or absent cervical control, being classified through the Gross Motor Function Classification System (GMFCS) at level IV or V and receiving an oral diet (mixed or exclusive). Caregivers of tracheostomized children were excluded.
After, got approval by the IMIP Ethics and Research Committee, under protocol nº 50807815.2.0000.5201, the questionnaire was check in detail before of starting data collection.
Children and caregivers were contacted according the schedule of their medical consultation. After have read and signed the Free and Informed Consent Form (FICF), the questionnaire was filled out. It is noteworthy that the questionnaire was built by the researchers, based on the studies by Araújo15 and Quadro10. It is composed of questions related to the characterization of the sample, to factors related to the quality of the guidance received on feeding and care practice.
The dependent variable "quality of the guidelines" was established through the evaluation of two aspects, namely: the guidelines content and how they were explained. Then, this could be classified as not oriented, satisfactory and unsatisfactory.
- Not oriented: when the caregiver reported not having received guidance related to the care of feeding for a child with CP.
- Satisfactory: when it was answered 50% or more of the aspects of each category below;
- Unsatisfactory: when it was filled in less than 50% of the questions in one of the categories below;
Categories:
How the guidelines were oriented :
• In Individual session;
• Demonstration of how the caregiver should proceed;
• Intervention and adjustment by a speech therapist, when the caregiver fed the child;
• With a minimum frequency of three times in the last semester.
Oriented content:
• Proper posture of the child for feeding;
• Safer food in texture and consistency for the child;
• Ideal eating utensils for children;
• Risk signs for tracheal aspiration.
The independent variables were related to the children characterization (age, sex, type of CP, professional follow-up performed, time and frequency of speech therapy follow-up);and the characterization of caregivers (age, sex, degree of kinship with the child, income and occupation); feeding and care practice (risk signs, meal time, stress, food consistency, posture, eating utensils, facilitating maneuvers, caregiver safety and difficulties when feeding the child).
The "utensil" variable was later categorized as adequate and inadequate. The use of a bottle and/or syringe in the child's diet was considered inappropriate. Other eating utensils were classified as adequate.
The same happened with the "posture" variable. The sitting position with the head aligned was classified as adequate, the others were classified as inadequate.
The data were pre-coded and processed by the Epi-info 3.5.4 program, in WINDOWS mode. Double entry of the data was performed in order to check for possible typing errors. Fisher's exact test was used to compare categorical variables, looking for proportions and inferring associations. Statistical significance was assumed when p <0.05.
RESULTS
All respondents were female, 88.1% (n = 52) of them mothers of the children with CP. Table 1 illustrates the characteristics of caregivers.
The family's financial income consisted predominantly of the financial assistance received by the child.
It is noteworthy that the GMFCS level V was represented by 78.0% (n = 46) of the children, out them 10.2% (n = 6) were on a mixed diet, that is, by gastrostomy and orally (Table 2).
It was registered that 57.6% (n = 34) of the children were undergoing speech therapy at the time of the interview with the care giver.
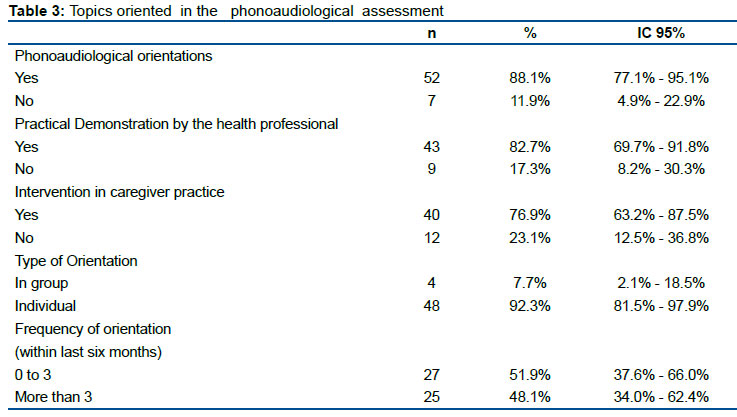
Table 3 shows that 88.1% (n = 52) participants received guidance on care of feeding by a speech therapist. However, about 50.0% of them stated that such guidelines were given less than three times in the last semester.
The aspect, "correct posture at the time of feeding" was the most frequently oriented topic (86.4%). The least one was with reference to signs of bronchoaspiration (64.4%).
Of the 52 caregivers who claimed to have received guidance, 23.1% (n = 12) classified it as unsatisfactory and 76.9% (n = 40) as satisfactory. When speech therapy accompaniment is related to the quality of the guidelines, even without showing a statistically significant difference, it is possible to observe that a lower percentage of caregivers received unsatisfactory guidance.
At least one risk sign for bronchoaspiration (coughing, choking, crying, pinching and/or nauseating reflex) during the feeding was reported in 83.1% (n = 49) of the children. Among these, cough was the most frequent (66.1%). The average duration of a meal was over 30 minutes for 37.3% (n = 22) of the children. In addition, 42.4% (n = 25) referred to the time to feed the child as of stress and/or nervousness.
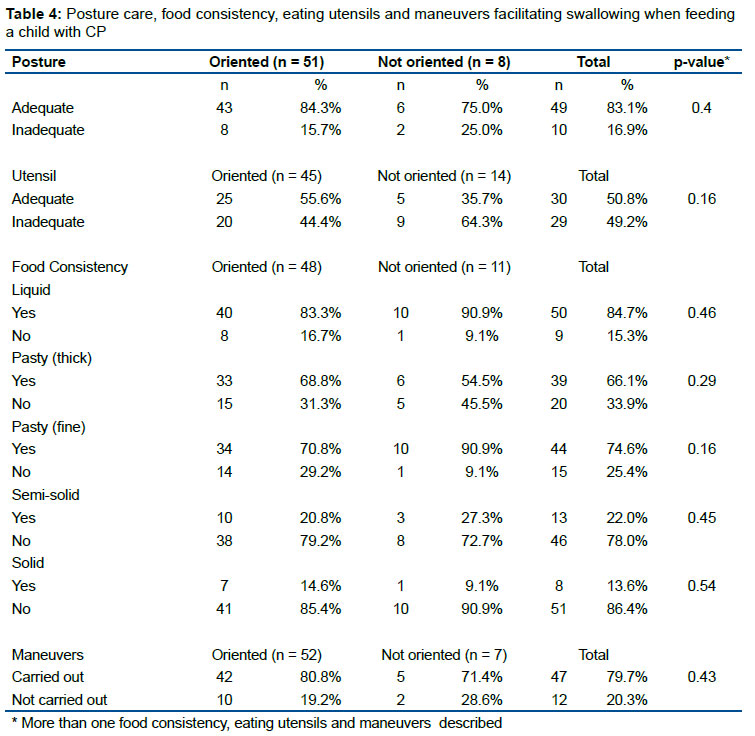
Table 4 indicates the practices of feeding care in relation to the usual posture of children during the meal, food consistency , eating utensils and maneuvers used. It is noteworthy that most children receive a meal while sitting with their heads aligned, defined as adequate posture. Although there is no statistically significant difference, it is registered that 84.3% of the oriented caregivers correctly position the child for food, while such posture is performed by 75.0% of those not oriented.
The most frequent food consistencies in the diet of children with CP were liquid (84.7%) and pasty (liquidized) (74.6%). The offer of liquefied diets was more frequent among non-oriented caregivers, while for those who received guidance, the thick pasty consistency was assumed to be the ideal or most appropriate.
The most used eating utensils were spoon (91.5%) and cup (74.6%). However, it was registered that 49.2% of respondents used inappropriate eating utensils, such as bottles and syringes. Regardless of not being statistically significant, there is a higher percentage of oriented caregivers handling the appropriate eating utensils when compared to non-oriented caregivers.
About 80.0% of the caregivers performed at least some auxiliary maneuver in swallowing, with verbal command being more evident. The practice of these maneuvers was more frequent among caregivers who received orientation on care feeding guidelines.
The relationship between the quality of the guidelines and the practice of care in feeding is illustrated in Table 5. There was no statistically significant difference between caregivers who received satisfactory guidance and those who received unsatisfactory guidance, however it is possible to observe that the first group tends to offer more pasty foods. In addition, the percentage of using appropriate eating utensils and performing auxiliary maneuvers was higher when compared to the group that received unsatisfactory guidance.
Of the participants, 74.6% (n = 44) reported difficulties in feeding the child with CP. Organizing the child's posture was the main difficulty of caregivers (31.8%); then, the acceptance of the diet (18.2%). Food consistency, length of time for feeding, presence of cough and/or choking during feeding, among others, were also cited as major difficulties. The majority of caregivers (84,7%) reported safety concerns during feeding process.
DISCUSSION
Most of the participants were the mothers who care for their children with CP, corroborating Dantas et al.16 who describe caring as a task culturally linked to women. Thus, it is possible to infer that the mother is the main actor in child care, receiving help from her mother and her husband. Despite of this help, almost all participants did not any other labor outside the home, as in the study by Carvalho et al.17, in which 90.0% of caregivers of children with CP did not executive an external professional activity.
This fact is understandable, given that children with CP demand special attention and care. In this way, mothers tend to give up their professional career to meet the needs of their children. This maternal posture was supported by Perez18, who reports the importance of the caregiver being a member of the family, aiming at a more natural, affective, caring performance, with a higher level of tolerance and easier understanding, even non-verbal.
Some socioeconomic aspects were investigated. In general, the population had low income with precarious socioeconomic conditions. Most interrupted their studies in elementary or high school, only 11.9% attended vocational or higher education. These aspects can affect both the frequency of CP and the way children are cared for. In situations of poverty, issues related to difficulties in eating are exacerbated due to limited resources, especially with regard to the purchase of nutritious foods, eating utensils or other materials. In addition to greater difficulty in accessing rehabilitation and health services10.
Children with CP need multidisciplinary monitoring to assist their development9. In this study, 57.6% received speech therapy assistance. Of these, only 17.6% underwent speech therapy two or more times a week. Regardless of the number of weekly visits offered, attendance to treatment is often difficult, mainly due to the reality of public services, in addition to the dependence on transportation, incompatibility of caregiver and child schedules with different treatments and the child's locomotion12.
It is observed in practice, the difficulty in transporting these children, who often live in distant areas of the state and need to travel to other cities for speech therapy and other treatments. In addition, the great demand of patients referred to speech therapy, added to the scarcity of this service in the public network, causes distortions between demand and supply, not being able to serve the entire population that needs speech therapy.
In this study, 88.1% of the participants reported receiving speech therapy guidance regarding feeding care. However, 23.1% of the guidelines were unsatisfactory, due to a failure in the form or content of these recommendations. Adequate speech therapy activities include educational actions aimed at caregivers of dysphagic patients, associated with the therapeutic process.
It should encompass the awareness and training of these caregivers, preparing them to deal with issues related to the child's posture, adequate eating utensils and safe food consistency, in addition to signs of risks for aspiration, importance of cough and compensatory strategies/maneuvers. Such guidelines are crucial from the beginning of rehabilitation and aim to ensure continuity of care and treatment at home10,11.
Silva19 observed the knowledge, attitudes and practices of caregivers of patients with neurogenic dysphagia and found little knowledge regarding the risks of dysphagia, the importance of coughing and care for the food consistency in children with CP, including utensils and a safe posture for feeding.
Carvalho et al.17, in a study with caregivers of children with CP, also reported that knowledge regarding aspects related to feeding difficulties was restricted, 66.6% of the sample were unaware of the definition of aspiration.
Meanwhile, Zapata and Mesa3 in a qualitative study carried out in Colombia, concluded that care with the food and nutrition of children with CP was the mother's own construction through daily experiences, implying that they do not receive professional guidance, a fact that contrast with the finding of our study.
It is noteworthy that 71.2% reported having received guidance on the signs of risk of bronchoaspiration, corroborating studies previously mentioned. Despite this record, this fact is worrying, mainly due to the aggravation and frequency of these events in children with CP. Since in this population, almost all children had some sign of risk for bronchoaspiration, such as coughing, choking, feeling of suffocation, crying or nauseated reflex, in addition to stress at the time of feeding and the prolonged time of this process. .
Arvendson20 states that meals that last more than 30 minutes and the parental stress in the child's diet are warning signs for bronchoaspiration and malnutrition. In this study, 37.3% of the caregivers reported investing more than 30 minutes per meal feeding a child, 42.4% emphasized that it was a time of stress and/or nervousness, suggesting they have need for support and attention from corresponding qualified professionals.
Furthermore, it is known that more than 50% of children with CP have some type of disorder to eat or be fed, with behaviors, reflecting risks to their health, ranging from nutritional aspects to respiratory issues, usually characterized by bronchoaspiration of food and or saliva itself21.
Body posture and alignment are important aspects in the feeding process, being ideal to have the body aligned and the head slightly flexed22,23. However, postural abnormalities are common in children with CP, especially the hyperextension of the neck that promotes airway opening, which impairs the dynamics of swallowing and, mainly, the protection of the lower airways. Properly positioning the child can be a difficult task, but it is essential for safe and effective swallowing24.
The research findings corroborate other studies12,23 which register the importance of the child's posture at the time of feeding in the list of guidelines received.
Another important aspect to be evaluated and guided in the monitoring of neurological children is the consistency of the food offered, which depends on the child's difficulties and potential. Homogeneous soft foods are easier to accept and swallow12, a fact recorded in this study. The liquid and pasty consistencies were the most offered to children. Benfer et al.25 found that 79.2% of parents of children with CP reported difficulty in offering liquid and solid foods, with similarity in the difficulty found with solid foods.
The organoleptic properties of foods are not restricted to consistency and go beyond preference or taste. Respecting the prescribed nutritional aspect, the diet should be offered in the form guided by the speech therapist, according the need for each case. With regard to consistency, the indication is always for the least risk to the child's health. Normally, pasty and thickened liquids, however the diet can vary according to the individual capacity. Therefore, when comparing the food consistency used by oriented and non-oriented caregivers as to the ideal one , there was no significant difference.
From oral motor development, at 12 months of age, the cup and spoon are the eating utensils that should be used for feeding26. When considering the age of the participating children and this reference, the use of a cup and spoon were defined as adequate. Most caregivers (76.3%) reported receiving guidance related to the ideal utensils. However, a large part (49.2%) of them used bottle or syringe in the offer, artifacts harmful to orofacial development, in addition to not offering safety in handling. This can be perceived as a divergence between guidance and practice, probably the caregiver's anxiety to provide adequate nutritional support to her child, made her pass over the utensil that best suited her or even facilitate the feeding process. What is not always what brings greater safety to swallowing.
Maneuvers to facilitate swallowing in children with CP, should be directed to the mother or caregiver23. The performance of at least one of the facilitating maneuvers was exposed by 79.7% of the interviewees. Among these maneuvers, verbal command, a recommended and beneficial resource, was the most widely used , probably because it is something instinctive for those who feed, even without reflect that they received guidance about it. The performance of other maneuvers that are usually guided by a speech therapist, was more present among the caregivers who received guidance on feeding guidelines.
This research also compared the quality of the guidance received in food care with the practice of such care. It is important to note that it is common to find caregivers who feed the children with neurological disorders in an inadequate posture, using not recommended eating utensil and inadequate food consistency, even they have undergone speech therapy or already received orientation on feeding care guidelines.
Regarding the quality of the guidelines, the participants who were satisfactorily oriented, offered more pasty foods and less solid ones. Since pasty foods are highly recommended due to the lower risk of bronchoaspiration. They also showed to use less bottle and syringe, in addition to performing more facilitating maneuvers during feeding.
Such findings allow us to infer that satisfactory guidance that transforms the practice of caregivers, especially in relation to food consistency, eating utensils and feeding maneuvers, should be performed individually and systematically, the therapist demonstrating and observing the care practice, in addition to including important aspects of feeding a CP child such as posture, utensils, food consistency and, risk signs for bronchoaspiration.
Holanda and Andrade27 reported that the most often cited difficulties by mothers in feeding their children with CP consist in achieving the of child's position, acceptance, showing in long-term meals the presence of risk signs for bronchoaspiration, perceived through frequent coughing and choking. Those findings corroborate those found in this study, in which the most cited difficulty was in relation to the child's posture (31.8%), followed by acceptance, food consistency , time spent in meals and presence of coughing/choking during meal time.
A big majority (84.7%) of the sample affirmed feeding their children with safety, compatible with those who received speech therapy guidance regarding care on it (88.1%).
As in other studies, some limitations were also observed during its planning and development. Among the difficulties encountered, the majority of children who met the inclusion criteria were unable to participate in the study, due to the fact that they use an exclusive alternative route of feeding.
Another important aspect is the fact that it is not possible to guarantee the veracity of the data reported by the interviewees. To mitigate potential bias, each question contained in the collection protocol was clarify and explain to participants.
FINAL CONSIDERATIONS
When analyzing the guidelines received by mothers/caregivers and their feeding practices in children with cerebral palsy, it was observed that the aspect related eating utensils was the item least adequated, at same time it was the one with the greatest divergence between knowledge and practice, which may reflect an issue in the guidelines provided.
The guidelines in relation to the most appropriate food consistency , eating utensils, use of maneuvers that facilitate swallowing were very generic, not focused on children with CP. These findings suggest the need of improving the frequency of guidance , doing individually, consistent in its content, demonstrating and observing the practice, in order to increase the chances of implementing the learning to the daily practice correctly.
It is noteworthy that behaviors that reflect risk of bronchoaspiration were one of the aspects least mentioned by the participating mothers/caregivers which is a concern, given the high prevalence of dysphagia in children with cerebral palsy.
The findings reveal that most of the caregivers received the feeding guidelines for children with CP, however, there is no periodic and systematic monitoring of what is actually incorporated into the feeding practice. This may indicate a gap between the guidelines received and the effectiveness of their daily practice, especially concerning protective measures of the lower respiratory tract.
REFERENCES
1.Rosenbaum P, Paneth N, Leviton A, Goldstein M, Bax M, Damiano D, et al. A report: the definition and classification of cerebral palsy. Dev Med Child Neurol. 2007;109:8-14. [ Links ]
2.Arevalo MPG, Calderon MY, Rangel SYA. Participación de la fisioterapia en los procesos de alimentación de niños con parálisis cerebral. Umbral Científico. 2004;(5):83-91. [ Links ]
3.Zapata LFG, Mesa SLR. Alimentar y nutrir a un niño con parálisis cerebral. Una mirada desde las percepciones. Invest Educ Enferm. 2011;29(1):28-39. [ Links ]
4.Rocha PFA, Boehs AE, Silva AMF. Rotinas de cuidados das famílias de crianças com paralisia cerebral. Rev Enferm UFSM. 2015;5(4):650-60. DOI: http://dx.doi.org/10.5902/2179769215685 [ Links ]
5.Sullivan PB, Lambert B, Rose M, Ford-Adams M, Johnson A, Griffiths P. Prevalence and severity of feeding and nutritional problems in children with neurological impairment: Oxford Feeding Study. Dev Med Child Neurol. 2000; 42(10):674-80. DOI: http://doi.org/10.1017/s0012162200001249 [ Links ]
6.Aurélio SR, Genaro KF. Comparative analysis of swallowing patterns between children with cerebral palsy and normal children. Rev Bras Otorrinolaringol. 2002;68(2):167-73. DOI: https://doi.org/10.1590/S0034-72992002000200003 [ Links ]
7.Monteiro CBM, Abreu LC, Valenti VE. Paralisia cerebral: teoria e prática. São Paulo: Plêiade, 2015; p.385-97. [ Links ]
8.Ribeiro MFM, Barbosa MA, Porto CC. Paralisia cerebral e síndrome de Down: nível de conhecimento e informação dos pais. Cienc Saúde Coletiva. 2011;16(4):99-106. DOI: https://doi.org/10.1590/S1413-81232011000400009 [ Links ]
9.Vieira NGB, Mendes NC, Frota LMCP, Frota MA. O cotidiano de mães com crianças portadoras de paralisia cerebral. Rev Bras Promoç Saúde. 2008;21(1):55-60. DOI: http://dx.doi.org/10.5020/177 [ Links ]
10.Milbrath VM, Siqueira HCH. Cuidado da família à criança portadora de paralisia cerebral nos três primeiros anos de vida. Dissertação (Mestrado) - Universidade Federal do Rio Grande. Porto Alegre: 2008. [ Links ]
11.Quadros VAS. Educação em saúde para familiares cuidadores de pacientes disfágicos pós-acidente vascular cerebral. Dissertação (Mestrado) - Universidade Tuiuti do Paraná. Curitiba: 2007. [ Links ]
12.Silvério CC, Henrique CS. Paciente com paralisa cerebral coreoatetóide: evolução clínica pós-intervenção. Rev CEFAC. 2010;12(2):250-6. DOI: https://doi.org/10.1590/S1516-18462010005000007 [ Links ]
13.Goldani HAS, Silveira TR. Disfagia na Infância. In: Jotz GP, Angelis EC, Barros APB. Tratado da deglutição e disfagia: no adulto e na criança. Rio de Janeiro: Revinter, 2010; p.219-29. [ Links ]
14.Zangirolami-Raimundo J, Echeimberg JO, Leone C. Research methodology topics: Cross-sectional studies. J Hum Growth Dev. 2018;28(3):356-60. DOI: http://dx.doi.org/10.7322/jhgd.152198 [ Links ]
15.Araújo BCL. Acurácia do diagnóstico clínico da disfagia em crianças com paralisia cerebral. Dissertação (Mestrado) - Universidade Federal de Pernambuco. Recife: 2012. [ Links ]
16.Dantas MAS, Pontes JF, Assis WD, Collet N. Facilidades e dificuldades da família no cuidado à criança com paralisia cerebral. Rev Gaúcha Enferm. 2012; 33(3):73-80. DOI: https://doi.org/10.1590/S1983-14472012000300010 [ Links ]
17.Carvalho APC, Chiari BM, Gonçalves MIR. Impacto de uma ação educativa na alimentação de crianças neuropatas. CoDAS. 2013;25(5):413-21. DOI: https://doi.org/10.1590/S2317-17822013005000004 [ Links ]
18.Perez ICS, Takayanagui OM. Orientações fonoaudiológicas para cuidadores e/ou familiares de pacientes adultos com demência. Dissertação (Mestrado) - Universidade de São Paulo. Ribeirão Preto: 2011. [ Links ]
19.Silva MAOM, Domingos NAM. Cuidadores de pacientes com disfagia neurogênica: perfil e conhecimentos relacionados à alimentação. Dissertação (Mestrado) - Faculdade de Medicina de São José do Rio Preto. São José do Rio Preto: 2007. [ Links ]
20.Arvedson JC. Feeding children with cerebral palsy and swallowing difficulties. Eur J Clin Nutr. 2013;67(Suppl 2):S9-12. DOI: https://doi.org/10.1038/ejcn.2013.224 [ Links ]
21.Braga WS, Mendes JFR. Avaliação do estado nutricional, terapia nutricional e queixas gastrointestinais em crianças com paralisia cerebral: uma revisão da literatura. Comun Ciênc Saúde. 2013;24(1):27-38. [ Links ]
22.Vianna CIO, Suzuki HS. Paralisia cerebral: análise dos padrões da deglutição antes e após intervenção fonoaudiológica. Rev CEFAC. 2011;13(5):790-800. DOI: https://doi.org/10.1590/S1516-18462011005000057 [ Links ]
23.Díaz AM, Sanmartin CS, Navarro VS. Parálisis cerebral infantil y disfagia. Nuberos Científica. 2010;1(1):62-65. [ Links ]
24.Furkim AM, Behlau MS, Weckx LLM. Avaliação clínica e videofluoroscópica da deglutição em crianças com paralisia cerebral tetraparética espástica. Arq Neuropsiquiatr. 2003;61(3A):611-6. DOI: https://doi.org/10.1590/S0004-282X2003000400016 [ Links ]
25.Benfer KA, Weir KA, Bell KL, Ware RS, Davies PS, Boyd RN. Oropharyngeal dysphagia in preschool children with cerebral palsy: oral phase impairments. Res Dev Disabil. 2014;35(12):3469-81. DOI: https://doi.org/10.1016/j.ridd.2014.08.029 [ Links ]
26.Araújo CMT, Silva GAP. Alimentação complementar e desenvolvimento sensório motor oral. Dissertação (Mestrado) - Universidade Federal de Pernambuco. Recife: 2004. [ Links ]
27.Holanda NMV, Andrade ISN. Dinâmica familiar na alimentação de crianças com paralisia cerebral. Rev Bras Promoç Saúde. 2010;23(1):374-9. [ Links ]
 Correspondence:
Correspondence:
lu_maggioni@hotmail.com
Manuscript received: August 2019
Manuscript accepted: November 2019
Version of record online: March 2020


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}